


Abstract
Background Three-dimensional (3D) navigation has become routinely used in spine surgery, allowing more accurate and safe procedures. However, radiation exposure related to the use of imaging is an unresolved issue, and information about it is relatively scarce. The “as low as reasonably achievable” (ALARA) principle aims to reduce the radiation exposure for the patients as low as possible. The objective of this study was to compare the effective dose related to the use of the O-arm in standard settings with adapted features for dose reduction during percutaneous cementoplasty.
Methods From March 2021 to October 2022, all consecutive patients who underwent navigated percutaneous cementoplasty with the use of the O-arm were prospectively included. Demographic, operative, irradiation, and radiological data were collected. The main outcome was the effective dose (E) in millisievert (mSv). Secondary outcomes were the absolute risk of cancer (AR) in percent equivalent to a whole-body exposition, operative time, and radiological results according to Garnier. In group A, patients were operated on with standard settings of the O-arm, whereas in group B, navigation on the field of view, collimation, and low-dose settings were used.
Results A total of 70 patients were included in the study: 43 in group A and 27 in group B. Also, 109 vertebrae were operated: 59 in group A and 50 in group B. Mean E was significantly higher in group A than in group B (9.94 and 4.34 mSv, respectively; P < 0.01). The 3D-related E followed the same trend (7.82 and 3.97 mSv, respectively), as did 2-dimensional–related E (2.12 and 0.37 mSv, respectively; P < 0.01). Average AR was also significantly higher in group A than in group B (5.10–4% and 2.10–4% respectively; P < 0.01). Operative time was similar in both groups, but the rate of satisfactory radiological results was higher in group A than in group B (95% and 84%, respectively; P = 0.11), and we found similar rates of cement leakage (22% and 24%, respectively; P = 0.71).
Conclusions The application of settings of the O-arm in accordance with the ALARA principle helped to significantly reduce the radiation exposure and should be routinely used for O-arm-assisted cementoplasty procedures.
Clinical Relevance This study details technical aspects and settings that may help users of the O-arm to decrease radiation exposure to patients and surgeons alike, especially in cementoplasty procedures, as well as in other procedures performed under O-arm guidance.
Level of Evidence 2.
Introduction
Vertebral compression fractures are common conditions, mostly related to high-energy accidents in young people and bone fragility in the elderly.1 According to the degree of compression, gold standard treatment is cementoplasty, such as vertebroplasty or vertebral augmentation (balloon kyphoplasty,2,3 SpineJack,4 or stentoplasty5).
Three-dimensional (3D) navigation has become routinely used in spine surgery,6 allowing more accurate and safe procedures.7 However, radiation exposure related to the use of imaging is an unresolved issue,8 and information about it is relatively scarce. The “as low as reasonably achievable” (ALARA) principle9 aims to reduce as low as possible the radiation exposure for the patient.10,11 Effective dose allows to estimate the radiation exposure and also the radiation-induced cancer risk8 related to the imaging using radiations. In our institution, we are used to perform cementoplasty under O-arm navigation (Medtronic, Minneapolis, MN, USA).12,13
A previous study found a mean effective dose of 11.33 mSv during percutaneous cementoplasty using the O-arm in standard mode.12 This result was almost 3 times the 1-year natural irradiation received by people in Switzerland14 and 10 times the dose obtained with another imaging device named Surgivisio12 during similar procedures. Decreasing the dose in accordance with the ALARA principle9 appeared to be mandatory. The O-arm allows some features and settings such as low-definition scan, 2-dimensional (2D) field of view (FOV) navigation, and imaging collimation, leading to a potential reduction of radiation exposure.13,15
The objective of the study was to compare the effective dose related to the use of the O-arm in standard mode with the use of the O-arm with adapted features for dose reduction in percutaneous navigated cementoplasty.
Methods
Inclusion/Exclusion Criteria
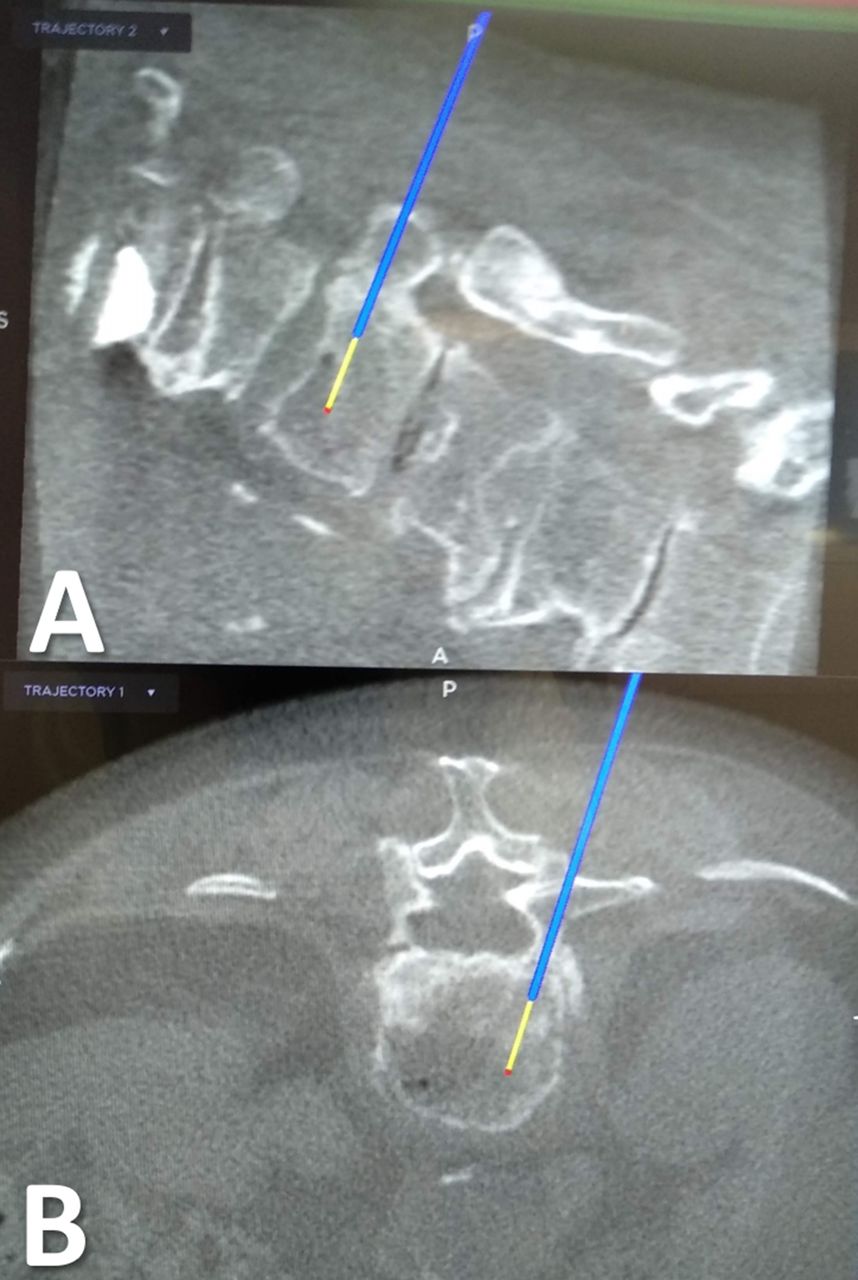
All consecutive patients who underwent navigated percutaneous cementoplasty (Figure 1) on 1 or several vertebral levels for vertebral compression fracture from March 2021 to October 2022 were enrolled in the study. Inclusion criteria were: (1) adult patients aged more than 18 years and (2) patients who underwent percutaneous cementoplasty with the use of the O-arm imaging system coupled with navigation. Exclusion criteria were (1) lack of information to calculate the radiation exposure; (2) vulnerable patients such as children, pregnant women, and patients unable to give consent; and (3) refusal to participate or lack of consent.
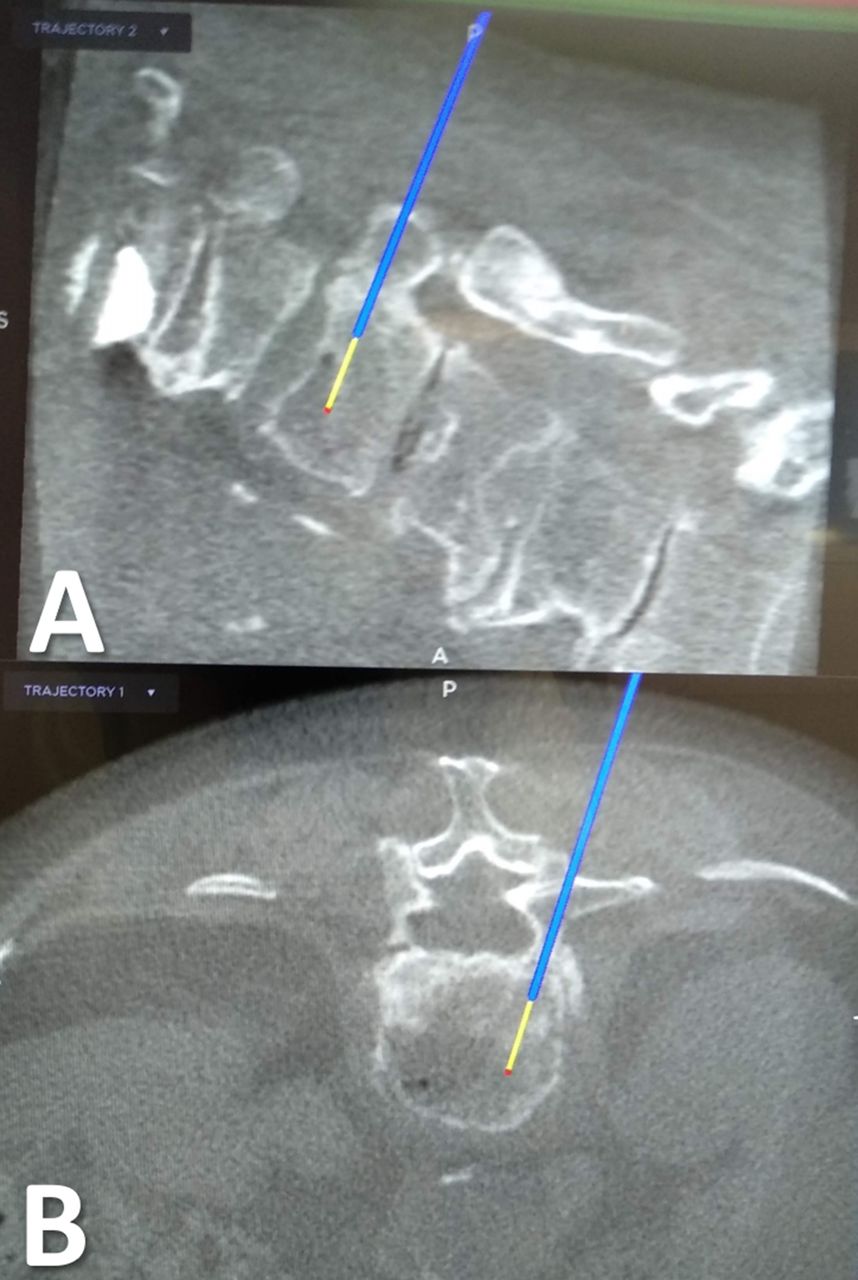
Intraoperative views of the 3D navigation on O-arm with the trajectory of the navigated Jamshidi needle. (A) Sagittal plane. (B) Axial plane.
Study Design
Study design was prospective.
Ethical Statement
The study was performed in accordance with the Ethical Commission of the Vaud canton which allowed the research protocol (Nr. 2021–00298). All patients signed a written consent for participation in the study.
Interventions
All patients were operated on in prone position, under general anesthesia, and after antibiotic prophylaxis. O-arm 2D and 3D acquisitions could be performed under patient apnea, and the images transmitted to the Stealth navigation (Medtronic, Minneapolis, MN, USA) as a standard technique.12 Then, a percutaneous cannulated navigated Jamshidi needle could be introduced inside the pedicle of the fractured vertebra, and cementoplasty performed under 2D imaging. The surgeon and other personnel carried a lead apron and a thyroid shield for radiation protection. According to a loss of height of the operated vertebra more than 20% and a local kyphosis more than 10°, balloon kyphoplasty was performed (Kyphon, Medtronic, Minneapolis, MN, USA) and then polymethyl methacrylate cement was injected in the vertebral body. In other cases, for both groups, polymethyl methacrylate cement was injected alone for standard vertebroplasty. X’Pede cement was used (Medtronic, Minneapolis, MN, USA).
Data Collection
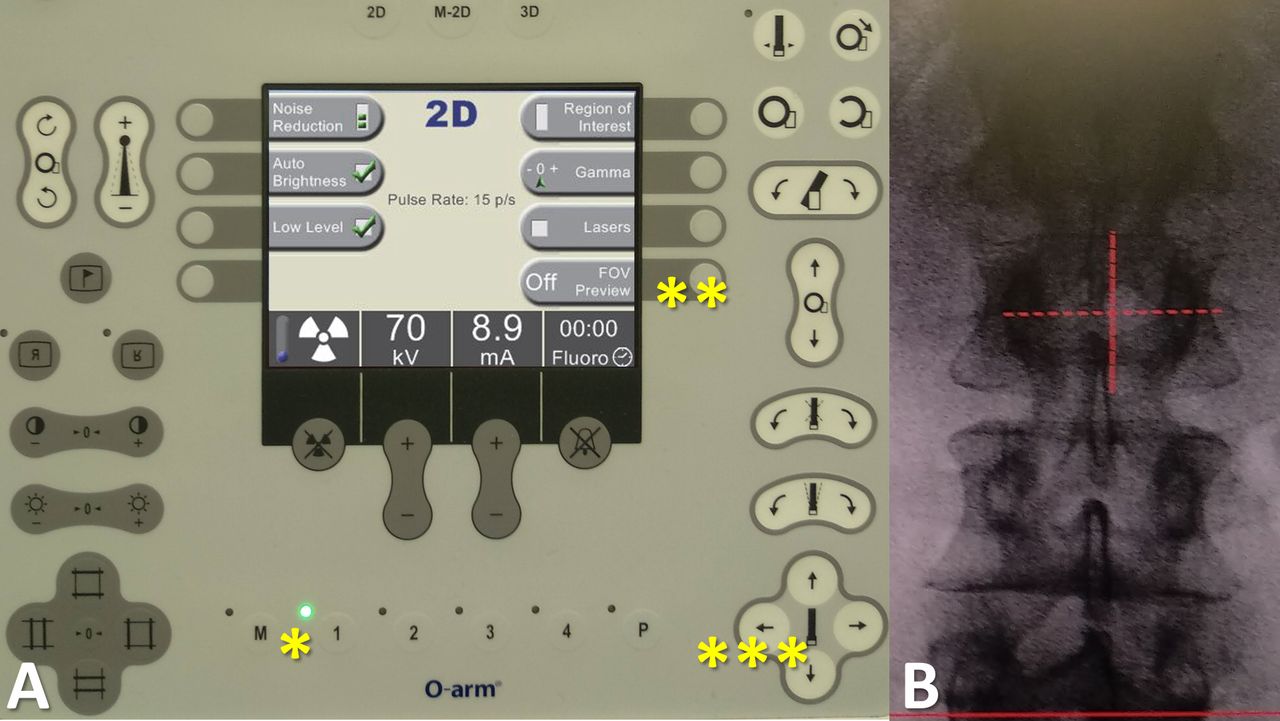
Group A was defined as patients for whom the standard settings of the O-arm were used as currently performed for many years in our institution. Group B was defined as patients for whom the O-arm was used with standard 3D protocol but low-dose 2D imaging, collimation, and navigation through an FOV of 20 cm (Figure 2). The FOV navigation principle was obtained with the memorization of the first 2D acquisition and of the O-arm position, allowing the surgeon to navigate on the imaging without performing any new acquisition. This process helped the surgeon to center the images on the targeted vertebra and to use collimation as well (Figure 3). O-arm settings in the groups are summarized in Table 1.
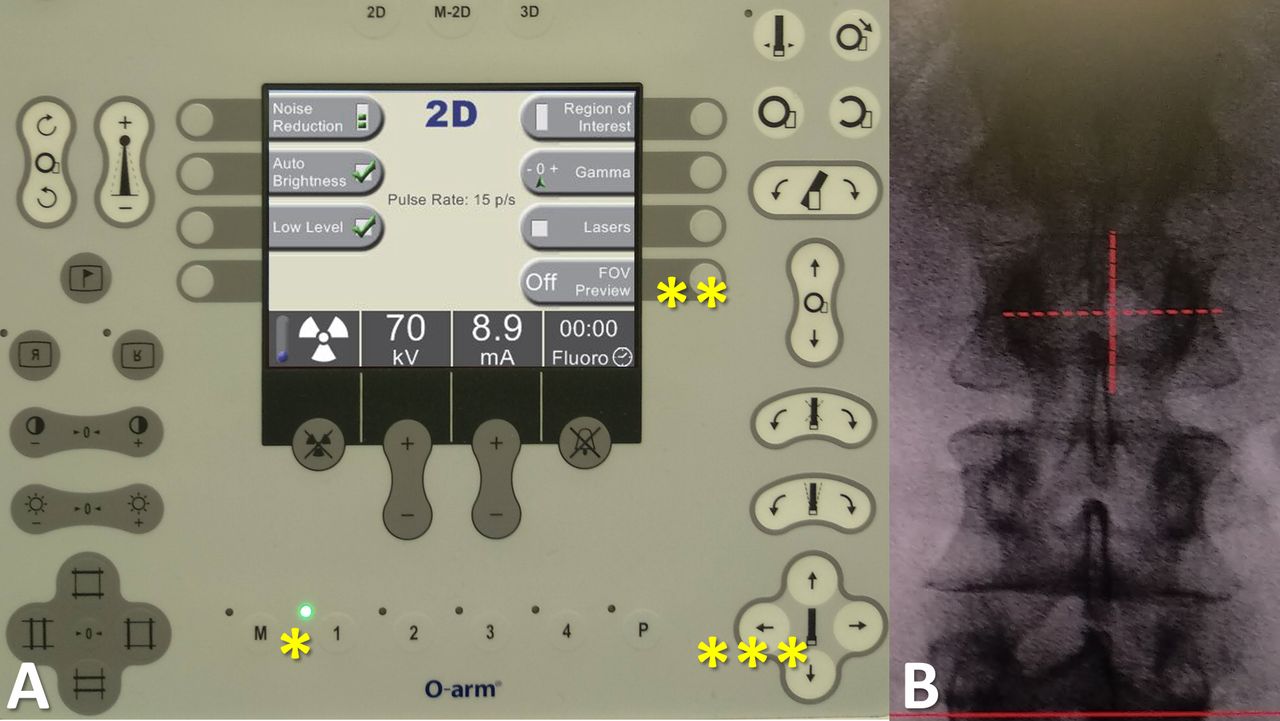
View of the control panel for settings of imaging acquisition. (A) First, an anteroposterior view can be taken. Then, the image and the O-arm position (*) are recorded. Second, the radiological technician can activate the navigation on the images by pressing the "FOV (field of view) Preview" button (**). Third, the radiological technician can navigate on the screen, using the position arrows of the control panel (***), especially in order to center the view on the fractured vertebra. (B) Finally, the lateral view is obtained and the height of the region of interest can be reached without another acquisition. Thus, a 3-dimensional navigated scan can be performed.
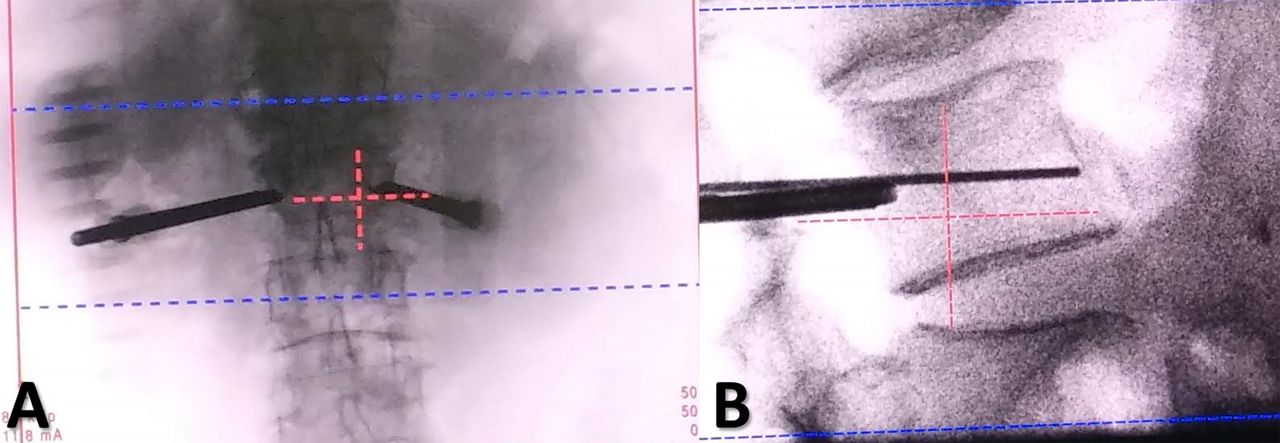
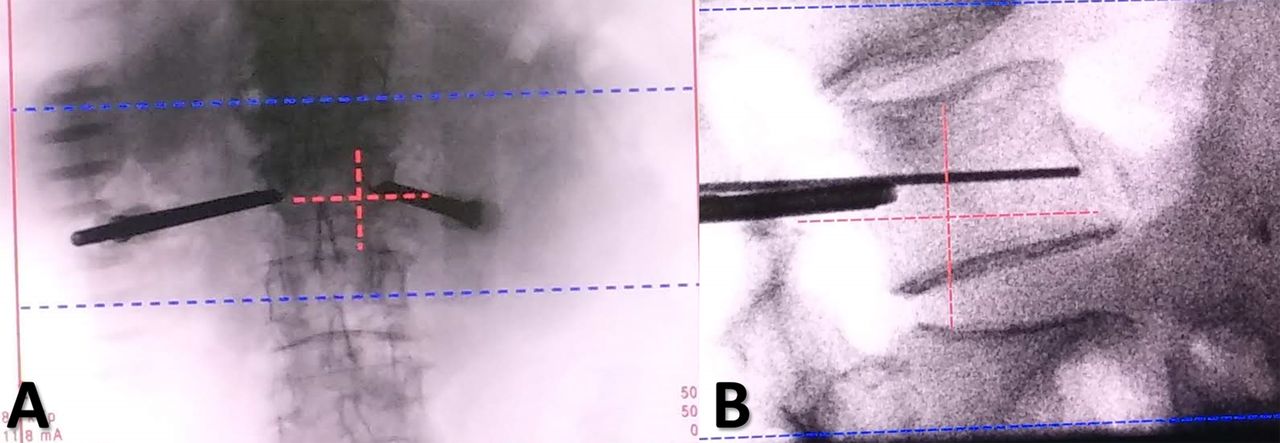
Intraoperative views of a cementoplasty procedure using the field of view (FOV) preview. (A) Anteroposterior view after placement of navigated Jamshidi needles in the fractured vertebra. (B) Lateral view. The region of interest may be reached with the FOV principle, allowing the fractured vertebra to be at the center of the image. Collimation can then be applied and also a zoom on the screen, to follow the cementoplasty procedure, and to decrease radiation exposure.
O-arm settings for 2D and 3D procedures.
Demographic data were collected, such as age, gender, height in centimeters (cm), and weight in kilograms (kg). Operative time in minutes (min) from incision to closure was also recorded. Surgeon level was recorded, considering “senior” as a surgeon with more than 3 years of experience in spine surgery and “junior” as a surgeon with 3 or fewer years of experience.
Radiation exposure was studied by recording the dose length product (DLP) in milligray·centimeter (mGy·cm) related to 3D irradiation and the dose area product (DAP) in milligray·square centimeter (mGy·cm2) related to 2D, and were used to calculate the effective dose E in millisievert (mSv). E is the sum of irradiation related to 3D and 2D, as follows: E3D = DLP × k, with k as the conversion factor related to the irradiated region: k = 0.015 and 0.014 mSv/mGy·cm for the lumbar and thoracic regions, respectively.16 E2D was calculated with the conversion factor w according to the European Commission as follows: w = 0.26 and 0.19 mSv/Gy·cm2 for the lumbar and the thoracic regions, respectively,16 E2D = DAP × w. Absolute risk (AR) of radiation-induced cancer equivalent to a whole-body acquisition in % was also calculated, using the formula AR = 5%/Sv.8 Image quality subjectively assessed by the surgeon was collected and considered to be sufficient or insufficient. Cement amount in cubic centimeter (cc) was recorded, and the volume by level calculated. Complications, especially cement leakage with its direction, were also recorded.
Outcomes
The main outcome was the overall E. E per operated level and E related to 2D and 3D were also compared as secondary outcomes. Other secondary outcomes were AR, operative time, amount of injected cement overall and by level, imaging duration, radiologic result according to the Garnier classification,17 cement leakage according to Lador18 et al, and other complications. In particular, satisfactory radiological results were defined as Z3, Y3, and X3, whereas other results were mild or poor and considered to be not satisfactory.12,17
Statistical Methods
Statistical analysis was performed with the R software version 3.1.3.19 Mean differences of numerical variables were compared using the Student t test. Correlation of Pearson and analysis of variance were used for association studies. A threshold of P ≤ 0.05 was defined as statistically significant. The number needed to treat was calculated for a 1-mSv difference, a common SD of 5 mSv, an alpha risk of 5%, and a power of 90%. Calculation found a minimal number of 19 patients mandatory in each group.
Results
Demographic Data
A total of 70 patients were included in the study: 43 in group A and 27 in group B. Also, 109 vertebral levels were cemented, including 59 in group A and 50 in group B. The 2 groups were similar in terms of gender, body mass index, number of operated levels, and Magerl classification, but age was significantly higher in group A than in group B (P = 0.02) (Table 2).
Patient demographics and surgery data.
Operative Data
Operative time was similar in both groups, with 34.6 minutes for group A vs 41.9 minutes for group B (P = 0.13). The number of unipedicular approaches was 25 (42%) in group A vs 26 (52%) in group B (P = 0.04). Surgeon level was comparable between the groups (P = 0.29). Cement injection volumes were similar in both groups, with a mean of 6.8 cc in group A vs 8.2 cc in group B (P = 0.13). Similarly, the volume by level was 4.9 cc in group A and 5.3 cc in group B (P = 0.30). Operative data are detailed in Table 2.
Radiological Results
Radiological results according to the Garnier classification (Table 3) showed a better rate of satisfactory results in group A than in group, with 95% and 84%, respectively. Cement leakage rate was 22% and 24% for groups A and B respectively (P = 0.62), and no complication occurred for both groups (Table 3).
Garnier classification of vertebral filling and cement leakage.
Radiation Exposure
Imaging duration was slightly higher in group A than in group B, with 23.67 and 17.82 seconds, respectively (P = 0.06), but the imaging duration by level was significantly higher in group A than in group B, with 18.56 and 12.93, respectively (P = 0.02). The number of 3D acquisitions per patient was similar in both groups (1.5 and 1.4, respectively; P = 0.72). E was significantly higher in group A than in group B, with 9.94 vs 4.34 mSv, respectively (P < 0.01). E per operated level was also significantly higher in group A than in group B, with a mean of 7.65 and 2.97 mSv, respectively (P < 0.01). E2D showed an average of 2.12 mSv in group A and 0.37 mSv in group B, with a significant difference (P < 0.01). E3D was also lower in group B, with a mean of 7.82 vs 3.97 mSv in groups A and B, respectively (P < 0.01). AR followed the same trend as E, with an average 5.10−4% for group A and 2.10−4% for group B (P < 0.01). Detailed irradiation data are summarized in Table 4.
Radiation exposure data comparison in the 2 groups.
Correlation Study
Correlation study in group A found a strong association between E and age, imaging duration, and surgeon level (P < 0.01). Similarly, group B had a strong association between E and operative time (P = 0.01), E2D and imaging duration (P < 0.01). However, there was no association in group B between E and age (P = 0.13) and E and imaging duration (P = 0.06). For both groups, there was a strong association between E2D and imaging duration as well as between surgeon level and operative time (P < 0.01). E2D and surgeon level were strongly associated only in group A (P < 0.01). E and operative time were strongly associated only in group B (P = 0.01). Correlation study of the whole series only found a strong association between E or E2D and imaging duration (P < 0.01 for both). The results of the complete correlation study are given in Table 5.
Correlation study: E, E2D, and surgeon level with other outcomes.
Image Quality
Image quality assessment (Table 6) found 100% of acceptable results in 3D in both groups and similar results in 2D in both groups without a significant difference (P > 0.99).
Subjective image quality assessment.
Discussion
The most important finding in this study was the significant radiation exposure reduction, thanks to the application of the ALARA principle for percutaneous cementoplasty using the O-arm imaging device. Both overall E and E related to 2D and 3D imaging were reduced without significant loss of image quality and radiological results.
The first prospective series about O-arm kyphoplasty was performed by Schils on 16 cases.20 He reported an operative time of 41 minutes (which was similar to group B), a fluoroscopy time of 3.2 minutes, and a fluoroscopy time per level of 2.4 minutes, almost 10 times higher than our results in both groups. The same author published about 54 cases21 and found an operative time of 38 minutes, which was close to our results, a fluoroscopy time of 3.1 minutes, and a fluoroscopy time per level of 2.5 minutes, almost 10 times higher than our results in both groups as well. This may be explained by the learning curve, considering the study at the beginning of Schils’ experience in O-arm cementoplasty.
Significant reduction of 2D imaging duration per level in group B may be explained by the use of navigation on images, which allowed more accurate placement of the O-arm without performing new acquisition in this aim, the cross was centered on the targeted vertebra by the radiology technician using the O-arm direction commands. On the contrary, in group A, the surgeon was compelled to reach the position of the targeted vertebra with additional acquisitions, leading to higher imaging duration for each level and higher radiation exposure accordingly. Collimation used in group B also helped to reduce the field of irradiation and then the overall 2D dose.22
Significant reduction of 3D irradiation was only explained by the systematic choice of standard or low-dose protocols and to draw attention on other parameters according to the patients’ body mass index. Rousseau et al published a dosimetric study comparing radiation exposure generated by the O-arm at the lowest irradiation mode in comparison with the Surgivisio device.15 They found a mean E3D of 2.41 mSv, a third lower than the results of group B, and an average E2D of 1.54 mSv, respectively, close to the results of group A, but almost 7 times higher than the results in group B. Collimation was the explanation of such difference.
Wojdyn et al published radiation exposure of 29 patients (44 vertebrae) operated on for percutaneous navigated vertebroplasty under O-arm23 and found a mean DAP of 9120 mGy·cm2, for thoracic vertebrae: 5281.4 mGy·cm2, 47.73% of cases and for lumbar vertebrae: 6680.6 mGy·cm2, 52.28% of cases. The calculation of effective dose using the conversion factors16 found a mean E2D of 1.39 mSv, among them 1.00 mSv for thoracic vertebrae and 1.74 mSv for lumbar vertebrae. These results were inferior to those of group A but almost 3.5 times higher than those of group B.
As not all facilities throughout the world have an O-arm device available, radiation exposure related to 2D fluoroscopic device use for 1-level percutaneous vertebroplasty was also compared. Boszcyk et al published a study about 60 percutaneous kyphoplasty procedures24 under fluoroscopic guidance and found a mean effective dose of 4.28 mSv, which was similar to the results of group B. Li et al published a comparison series about 1-fluoroscopic vs 2-fluoroscopic devices,25 using dosimeters for effective dose measurement. The mean radiation dose to the patient was 1.97 mSv for the 1-fluoroscopic technique group, less than half of group B results, and 0.95 mSv for the 2-fluoroscopic technique group. The mean radiation dose to the surgeon, which can be assimilated to E2D of the current series, was 0.27 mSv for the 1-fluoroscopic technique group and 0.25 mSv for the 2-fluoroscopic technique group, which were similar to the results of group B. The operative time was significantly different between groups: 47.15 minutes for the 1-fluoroscopic technique group vs 36.62 minutes for the 2-fluoroscopic technique group, which was comparable with groups B and A, respectively. So, the authors recommended using 2 fluoroscopic devices to decrease radiation exposure and operative time. Wojdyn et al23 compared O-arm with C-arm for percutaneous vertebroplasty. They found for the C-arm use a mean DAP of 16677 mGy·cm2 for thoracic vertebrae (leading to an E2D of 3.17 mSv16) and for lumbar vertebrae a mean DAP of 14202 mGy·cm2 (leading to an E2D of 3.69 mSv16). These results are 50% higher than in group A and almost 10-fold higher than in group B.
Cumulative natural irradiation in Switzerland during a year is estimated to be 4.30 mSv,14 which is similar to the results of group B but less than half of group A.
Similar rates of cement leakage in the groups may indicate that the decrease of image quality in 2D in group B did not affect accuracy and safety of the procedure, especially in consideration of the similar rates of kyphoplasties. This observation can be put in perspective that there was no correlation between surgeon level and radiation exposure or even operative time. This point illustrates the ergonomics of 3D navigation to help standardize the cementoplasty procedure for junior surgeons.
The current study has several limitations. First, the sample of patients was short, although the number needed to treat was reached for both groups. Second, the accuracy of effective dose calculation may have been altered because it represents an estimation, obtained with standard conversion factors,16 considering the use of PCXMC software26–28 which is a more accurate calculation through a Monte Carlo simulation.8 Collimation used in group B avoided the ability to estimate the radiation exposure as it was impossible to know the exact dimensions of the irradiation field required in PCXMC for dose calculation. However, we opted for the use of conversion factors because a previous study on irradiations with the O-arm found no significant differences between E2D calculated with the conversion factors and with PCXMC.12 For comparative purposes, the calculation was performed similarly in both groups.
Conclusion
The application of settings of the O-arm in accordance with the ALARA principle allowed a significant reduction of radiation exposure for both patients and surgeons. Image quality was also decreased but did not compromise the radiological results. Using the low-dose settings, navigation on the FOV and collimation should be always performed for percutaneous cementoplasty under O-arm for dose reduction.
Footnotes
Funding This study was supported by the Swiss Personalized Health Network (2018DRI13 to Thomas J. Wolfensberger).
Disclosures Duccio Boscherini discloses that he was on the speakers bureau for Medtronic, a company involved in the manufacture of a device examined in this study, and he still remains a non-remunerated consultant. He was also on the speakers bureau for the Johnson & Johnson Company and received consulting fees. The remaining authors have nothing to disclose.
Ethics Approval The procedures followed were in accordance with the ethical standards of the responsible committees on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. The ethical commission on human research of the Vaud canton approved the research protocol (No. 2021-00298).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.