


Abstract
Objective To our knowledge, this is the first systematic review to evaluate the available literature on the effects of perioperative serum glucose (SG) on outcomes for patients undergoing spine surgery. This review will add insight into how the perioperative management of SG affects the outcomes of patients undergoing spine surgery.
Methods Three databases were used in this review including Embase, PubMed, and Cochrane Library. The searches were from 2012 to 2022 and included the terms “spine surgery” and “glucose level” to identify studies that demonstrated a correlation between glucose level and postoperative outcomes. Pediatric studies, those that did not specify spine surgical outcomes related to glucose levels, and non-English studies were excluded. The methodological items for nonrandomized studies score was used to assess risk of bias in the included studies.
Results This review included a total of 9 cohort studies, both prospective and retrospective, encompassing a total of 431,156 subjects. Seven of the 9 studies reported an increased overall complication rate among patients with diabetes or with higher SG levels, and 4 studies demonstrated an increased infection rate among this population. Two studies reported an association between decreased SG levels and improved neurological recovery when a deficit was present preoperatively, and 1 of the studies found that this association was statistically significant.
Limitations Limitations of this review include lack of standardization regarding type of surgery, location of the spine, and level of evidence.
Conclusion Most of the current literature suggests that elevated SG levels in patients undergoing spine surgery likely leads to higher complication rates and may lead to increased infection rates, and this review reinforced the current evidence. Additionally, perioperative SG levels may be associated with the extent of neurological recovery after surgery, but further investigation may be warranted.
Clinical Relevance This review adds to the current body of evidence regarding perioperative SG levels and its association with complications.
Level of Evidence 2.
INTRODUCTION
Spine surgery is one of the most common surgical procedures performed in the United States.1 Traumatic injuries, degenerative processes, and other medical conditions lead to numerous cervical, thoracic, and lumbar procedures each year. Pathologies treated range from disc herniations to major deformity correction and stabilization of traumatic injuries. Given this, there has been an observed increase in the number of spine surgeries worldwide. Kobayashi et al reported data from 10 facilities in Japan and showed a 2.4 times increase in spine cases over the past 15 years.2 It is worth mentioning that Japan has a predominant aging population. Norway is another country with an abundant aging population, and Grotle et al reported an increase of 54% in spine surgeries in Norway over a 15-year period.3 The population in the United States is aging as well, and there has been a recent increase in the need for operative intervention for spine pathology.4 A recent analysis by Martin et al reported a 62.3% increase in lumbar fusion surgery in the United States over an 11-year period, with the highest number of procedures performed in people aged 65 years or older.5 Additionally, Deng et al reported an increase greater than 250% for lumbar fusion surgery among patients with degenerative disease over a 12-year period in the United States.6
Given the notable increase in operative spine patients, it may be important to consider factors that can improve surgical outcomes. Diabetes is strongly correlated to obesity, and since obesity and diabetes are increasing among the population at an alarming rate, there may be an increased need for spine surgeries among this population.7,8 Diabetes and uncontrolled glucose levels have been previously reported to negatively affect outcomes in orthopedic surgery.9 Browne et al reviewed a retrospective cohort and reported that patients with diabetes had a statistically significant higher incidence of mortality and infection after lumbar spine surgery.10 Another retrospective study by Chen et al reported that the strongest risk factor for developing infection after lumbar spine surgery was diabetes.11
On the other hand, some literature showed no difference among diabetic patient outcomes after undergoing spine surgery. Of note, these studies analyzed non–insulin-dependent diabetics. Cho et al reported no significant difference in complications after 2 years among non–insulin-dependent diabetic patients and patients without diabetes undergoing lumbar spine surgery.12 However, this study had a small sample size of only 42 patients, which may limit the ability of their results to be generalizable to all surgical patients. Additionally, Dokai et al reported no significantly different major complications among diabetic vs nondiabetic patients undergoing cervical spine surgery for cervical myelopathy.13 The only significant differences between the diabetic patients vs nondiabetic patients in this study were worse recovery of motor and sensory function in the lower extremities in diabetic patients and a negative correlation between recovery rate and preoperative HbA1c. However, the results of this study should be taken cautiously considering its limitations of a small sample size of only 78 patients and its retrospective nature.
In addition to elective spine surgeries, prior literature suggests that abnormal blood glucose levels may significantly worsen outcomes in the acute setting of spinal cord injuries. Furlan et al retrospectively evaluated a cohort of hyperacute traumatic spinal cord injuries and abnormalities in blood glucose among 499 patients.14 Blood glucose levels >140 mg/dL after 7 days of injury were associated with a statistically significant increase in mortality and a decrease in the Functional Independence Measure score within 1 year.
To our knowledge, this is the first systematic review to evaluate the available literature on the effects of diabetes mellitus and abnormalities in glucose levels on outcomes for patients undergoing spine surgery. This systematic review will add significant evidence to the current literature and improve the preoperative and postoperative management of patients undergoing spine surgery.
MATERIALS AND METHODS
This systematic review was designed and conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis protocol and the Cochrane Handbook guidelines.15,16 There was no required institutional board review approval for this systematic review.
Search Strategy
Three databases were used in this systematic review: Embase, PubMed, and Cochrane Library. The searches were from 2012 to 2022 and included the following terms: “spine surgery” and “glucose level”. Initial screening of titles, abstracts, and full-text studies was performed.
Inclusion and Exclusion Criteria
The inclusion criteria were any studies published between 2012 and 2022 that included patients undergoing spine surgery and had a correlation between glucose level and postsurgical outcomes. Pediatric studies, those that did not specify spine surgical outcomes related to glucose levels, and non-English studies were excluded.
Data Collection and Abstraction
The investigators independently evaluated titles, abstracts, and full text from the studies found in the search. The senior author reviewed the available studies and resolved any discussion from the search, inclusion, and exclusion criteria for the studies. The following data were extracted: authors, the title of studies, journal of publication, year of publication, country, level of evidence, number of subjects, number of procedures performed, mean age, number of women and men, visual analog scale (VAS) scores, final follow-up time, control group, surgical procedures, outcomes, and complications.
Statistical Analysis Assessment for Risk of Bias
The methodological items for nonrandomized studies score was used to evaluate the quality of the studies (Table 1).17 All 9 studies adequately reported a clear aim, a prospective collection of data, appropriate end points of the studies, inclusion of consecutive patients, follow-up periods, an adequate statistical analysis, prospective calculations of the study size, and loss of follow-up less than 5% except for the study by Tanashima et al.18 The study by Peng et al was the only one to earn a score of 2 for an unbiased assessment of the study endpoint;the rest of the studies did not report it.19 Four studies reported having control groups.18,20–22 The average score of the studies included in this systematic review was 17.7 with a range from 14 to 22. These scores represent high-quality studies.
MINORS criteria scores by study.
RESULTS
Characteristics of the Systematic Review Search and Studies
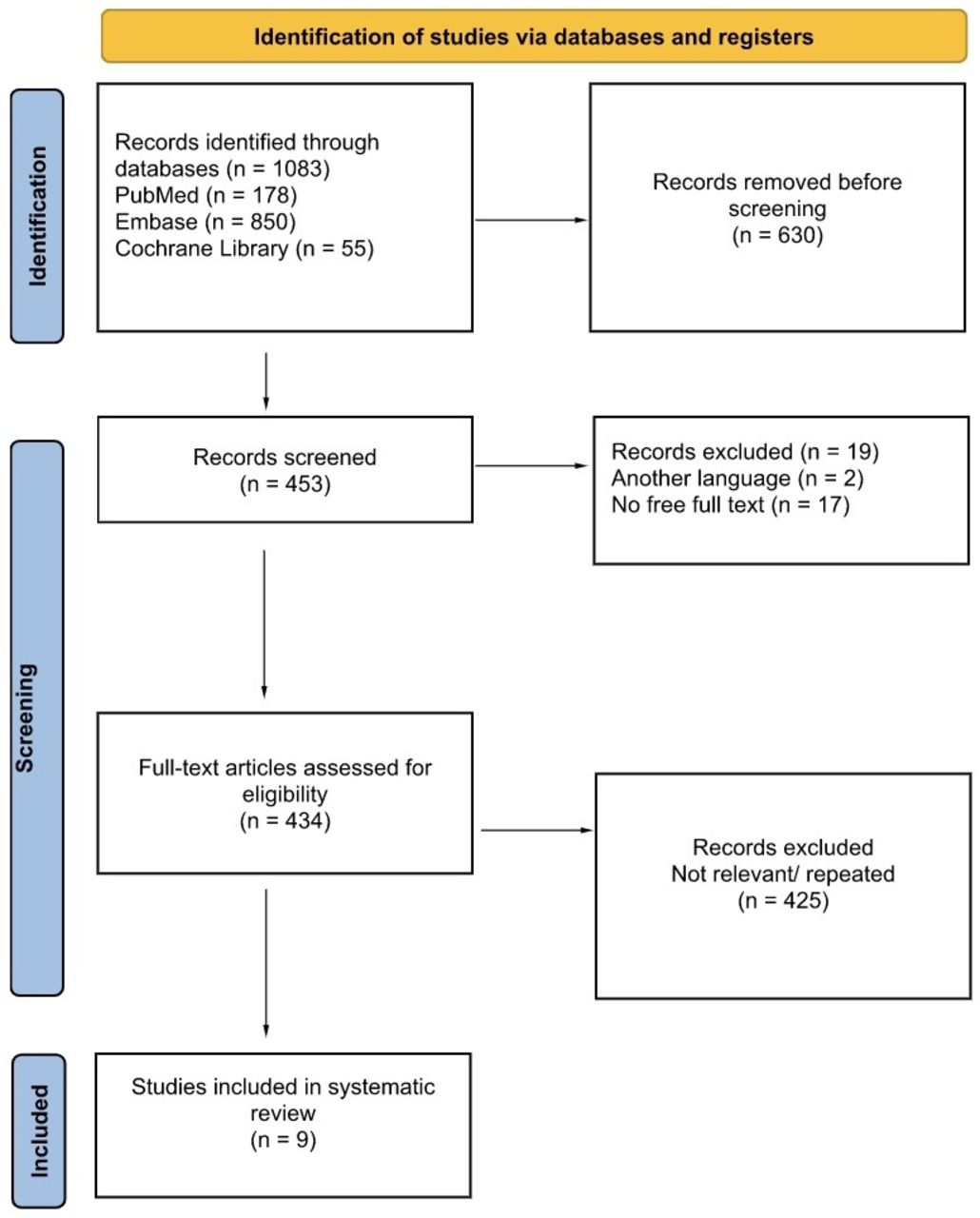
A total of 1083 results were found after the primary databases were searched. PubMed included 178 results, Embase included 850 results, and Cochrane Library included 55 studies. A total of 630 records were removed after adjusting for the selected date range. From the remaining 453 studies, 19 studies were excluded due to non-English language (2) and lack of full-text availability (17). A total of 434 full-text articles were assessed for eligibility, and 425 were excluded due to not meeting the criteria for inclusion or being repeated from other database results. Thus, a total of 9 studies were included in this systematic review, which included a total of 431,156 patients (Figure).
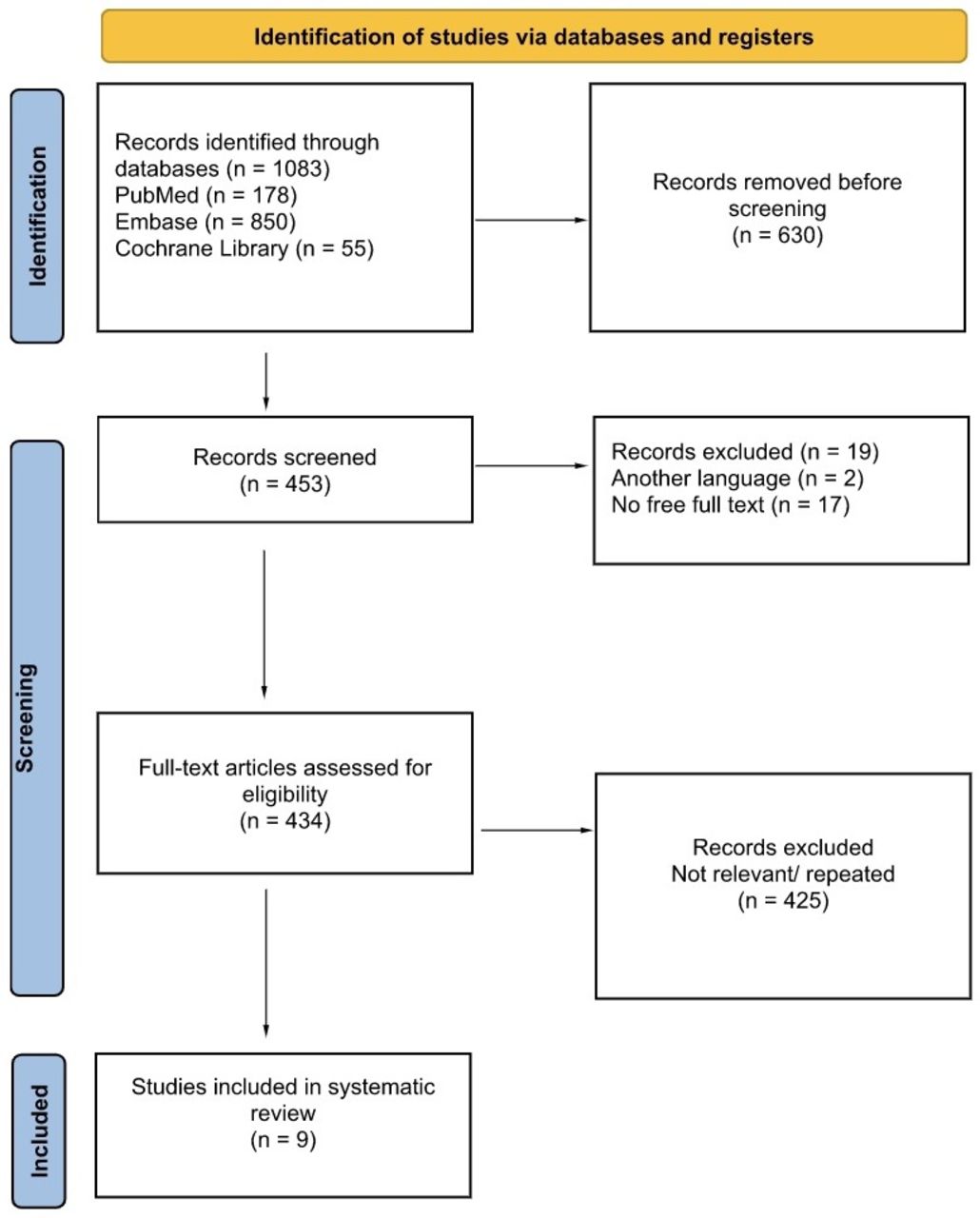
Flow diagram for search strategy and selection criteria.
The 9 studies we analyzed included data from 6 countries, with studies and subjects from the United States being most represented. Of the studies that specified age, the average age ranged from 56.1 to 69.5 years. The percentage of women in these studies ranged from 43% to 65.2%. Five of these studies included lumbar spine surgery, 3 of them included cervical spine surgery, and 1 study included cervical, thoracic, or lumbar spine surgery. Additionally, 5 of these studies were retrospective and 4 were prospective (Table 2).18–26
Demographics and characteristics of the studies.
Postsurgical Outcomes by Study
The retrospective database analysis by Guzman et al came from the Nationwide Inpatient Sample database and included 3 types of procedures: lumbar decompression without fusion, lumbar fusion, and lumbar fusion revision.23 Among all subjects, the group with uncontrolled/controlled diabetes carried a higher risk of having other comorbidities such as congestive heart failure, chronic pulmonary disease, liver disease, neurological disorder, renal disease, obesity, and depression compared with subjects without diabetes. The separation criteria for inclusion into either group was based on ICD-9-CM codes. There was a statistically significantly increased risk of postoperative infection (P < 0.0001), inpatient mortality (P = 0.0001), postsurgical bleeding, and revision rate among patients with diabetes vs patients without diabetes. Among those with diabetes, patients with uncontrolled diabetes had an increased risk of postoperative infection and inpatient mortality compared with those with controlled diabetes. Length of stay (P < 0.0001) was also significantly higher in patients with diabetes (regardless of being controlled) vs patients without diabetes.
The retrospective, single-center analysis by Peng et al reported outcomes of surgical intervention for lumbar stenosis, lumbar disc herniation, lumbar spondylolisthesis, and lumbar vertebral fractures.19 Their patient sample only included patients with diabetes mellitus. Only 37 patients (7.1%) developed a postoperative infection. Their results from a univariate analysis showed the following statistically significant χ 2 test for developing infection: a 10.67 times increased risk (P = 0.01) for patients with preoperative HbA1c > 7.5% compared with those with <7.5%, and an 18.57 times increased risk (P < 0.001) at 3 days postoperatively with a fasting blood glucose level >144 mg/dL (3 days average of all glucose measurements) compared with those with levels <144 mg/dL. There was also an observed 23.79 times increased risk (P < 0.001) at 3 days postoperatively with an average postprandial blood glucose >180 mg/dL compared with those patients with a 3-day postprandial glucose average <180 mg/dL. Their results from the multivariate analysis showed a statistically significant odds ratio of 4.63 for developing infection with a preoperative HbA1c >7.5%, an odds ratio of 5.71 for 3-day postoperative fasting blood glucose >144 mg/dL, and an odds ratio of 7.74 for 3-day postoperative average postprandial blood glucose >180 mg/dL.
The multicenter prospective study by Tanishima et al analyzed laminoplasty and anterior decompression and fusion for cervical spondylotic myelopathy and ossification of the posterior longitudinal ligament.18 They reported no significant differences in postoperative improvement among patients with diabetes vs without diabetes. At 1-year follow-up, the diabetic patients with good control of HbA1c (undefined in the study methods) had a statistically significant (P < 0.01) improvement in upper and lower limb function based on the previously validated Japanese Orthopedic Association Myelopathy Evaluation Questionnaire. However, there was no statistically significant difference when comparing the 2 groups. It is worth mentioning that this study had the lowest number of subjects (61) in this review, consisting of 0.01% of subjects in our study. Another limitation of this study was the high rate of loss to follow-up, with only 61 patients out of the 140 (43.6%) available for 1-year follow-up.
The retrospective review by Hwang et al analyzed single-level posterolateral and posterior interbody fusion surgery.24 They evaluated the relationship between HbA1c and risk of infection and reported that preoperative HbA1c was statistically significantly higher in patients who developed a postoperative infection vs patients who did not develop an infection (HbA1c of 6.78% vs 5.99%, respectively, P = 0.003). A surgical site infection was defined as having a superficial infection within 30 days of surgery or as having a deep infection within 1 year of surgery. The incidence of infection was 26.1%, with 3.3% in deep infections and 22.8% in superficial infections. Six infections resulted from the posterolateral approach, and 18 infections resulted from the posterior interbody fusion. The univariate and multivariate logistic analyses results showed that an HbA1c greater than 6.9% was an independent risk factor for infection with an odds ratio of 4.5 (P = 0.008). Additionally, longer periods of hospitalization were statistically significant, with 45.8 days in the hospital for patients who had a postoperative infection vs 19.3 days for patients who did not (P = 0.003).
The retrospective review by Worley et al analyzed the surgical treatment for patients with cervical spondylotic myelopathy.25 The patient samples included nondiabetic, insulin-independent diabetic, and insulin-dependent diabetic patients. Patients with diabetes were more likely to have cardiac and pulmonary comorbidities and higher body mass index values. A statistically significant increase in pneumonia, unplanned intubation, ventilator for more than 48 hours, bleeding transfusion, and urinary tract infections among patients with diabetes was reported. Longer hospital stays were found among patients with diabetes (P < 0.001). The only statistically significant difference found among diabetic patients was an increased incidence of wound complications (P < 0.001) for insulin-dependent patients vs for noninsulin-dependent patients (2.1% vs 0.3%, respectively, P = 0.045).
The prospective cohort study by Langlois et al analyzed surgeries of the cervical, thoracic, and lumbar levels of the spine.26 They evaluated levels of glucose among nondiabetic patients and found a 29.3% incidence of postoperative complications within 3 months. There were statistically significantly higher glucose levels during the first 3 days of surgery when compared with preoperative values. On postoperative day 2, the average blood glucose level for patients who needed surgical revision was 140.4 ± 16.2 mg/dL, which was significantly higher than that of patients who did not need a revision (blood glucose level: 120.6 ± 21.6 mg/dL; P = 0.04). Factors that may have been associated with this increase in glucose included age, smoking status, instrumentation, operative time, blood loss, and need for a transfusion.
The retrospective cohort study by Khan et al analyzed open posterior lumbar fusion for degenerative spondylolisthesis.20 They compared outcomes between diabetic vs nondiabetic patients. The only reported statistically significant difference among these groups was higher discharge rates to facilities for diabetic patients (P = 0.018). Radiological measures showed a statistically significantly higher pelvic incidence-lumbar lordosis difference for patients with diabetes. There were no statistically significant differences among the groups regarding postoperative complications, VAS scores, reoperation, or length of hospital stay.
The prospective study by Moazzeni et al analyzed lumbar fusion for patients with canal stenosis, disc herniation, and degenerative spondylolisthesis.22 They evaluated surgical outcome differences among diabetic vs nondiabetic patients. Fusion status was assessed by lumbar computed tomography scan and anteroposterior and lateral x-rays images 1-year postoperatively. They reported a statistically significant increase in fusion rate in nondiabetic patients at 78% vs in diabetic patients at 53% after 1-year (P = 0.02). Additionally, at the last follow-up, statistical significance was observed to be higher in diabetic patients for both Oswestry Disability Index (ODI) scores (average score in diabetic patients was 52 vs average score in nondiabetic patients was 41.3 [P < 0.001]), and for postoperative bleeding (P = 0.006). VAS scores were significantly higher preoperatively in diabetic patients (P = 0.07); however, the postoperative scores were not. Among diabetic patients, insulin-dependent diabetics had statistically significantly higher HbA1c, preoperative ODI, and 6-month postoperative ODI.
The prospective cohort study by Machino et al analyzed cervical double door laminoplasty in patients with cervical spondylotic myelopathy.21 They evaluated both diabetic and nondiabetic patients and compared their outcomes after 1 year postoperatively. The diabetic patients were classified as having a previous diagnosis or having fasting blood glucose >126 mg/dL. All patients were confirmed with an HbA1c test before meeting criteria for the diabetic group. It was reported that the recovery rates of lower extremity motor function (P = 0.047), upper extremity sensory function (P = 0.006), and urinary bladder function (P = 0.035) were significantly lower in diabetic patients. It was also reported that all patients had well-controlled glucose levels during the perioperative period. The study did not report differences among patients with a history of diabetes vs those who were recently diagnosed and did not report whether patients’ glucose levels were monitored during the 1-year follow-up period. There was no significant difference among recovery rates for upper extremity motor function, lower extremity sensory function, and trunk sensory function. The preoperative and postoperative results of the 10-second step test were significantly lower in the diabetic group (P < 0.001). Machino et al did not report on the rate of infection. There was no significant difference between the 2 patient groups regarding operative time, blood loss, postoperative cervical alignment, or range of motion.
The overall number of postoperative complications per study is shown in Table 3. All comparisons were based on diabetic subjects vs nondiabetic subjects, or among patients with higher levels of glucose vs those with normal levels of glucose. Only statistically significant differences were reported. The studies by Machino et al, Moazzeni et al, and Tanishima et al did not report specific differences on the values for glucose levels or HbA1c.18,21,22 Guzman et al reported on controlled diabetic patients, uncontrolled diabetic patients, and nondiabetic patients; however, this study did not include specific blood glucose or HbA1c values.23 Worley et al reported on diabetic patients stratified based on whether their diabetes was insulin or non–insulin dependent, but no specific glucose values were noted in this study.25 Khan et al reported an average HbA1c of 7.2% (range 5.1–10.7) for diabetic patients in their study.20 Langlois et al reported on nondiabetic patients and found that, on postoperative day 2, the average glucose level for patients who needed surgical revision was 140.4 ± 16.2 mg/dL, which was significantly higher than that of patients who did not need a revision, with an average blood glucose level of 120.6 ± 21.6 mg/dL (P = 0.04).26 Peng et al reported that values of postprandial glucose >180 mg/dL, postoperative fasting glucose >144 mg/dL, and/or HbA1c >7.5 were associated with a higher rate of infection.19 Hwang et al reported that preoperative HbA1c was higher for patients who developed a postoperative infection (6.78%) vs those who did not develop an infection (5.99%; P = 0.003). Additionally, they found that an HbA1c >6.9% was associated with a significant increase in surgical site infection (P = 0.001).12
Complications per study.
DISCUSSION
The goal of this systematic review was to evaluate and analyze the current available literature on the outcomes of diabetes and abnormalities in blood glucose levels for patients undergoing spine surgery. During our search, we were unable to find any other meta-analysis or systematic review on this specific topic. Spine surgery is one of the most frequently performed orthopedic surgeries in the United States. The literature also demonstrates a considerable increase in the number of patients worldwide undergoing spine surgery in recent years, particularly in countries with a large aging population.2,3,5,6
This systematic review included 9 studies that consisted of both prospective and retrospective studies. There were no randomized controlled trials included. Among the included studies were 4 studies that reported an increase in the rate of infection among patients with diabetes or higher levels of glucose.19,23–25 There were 2 studies that reported no significant difference in the rate of infection among patients with diabetes vs patients without diabetes.20,22 Three studies did not report information regarding infection.18,21,26 The 4 studies that included a statistically significantly higher rate of infection included a total of 429,569 subjects, which represented 99.6% of the patients included in this systematic review.19,23–25 There was only 1 study that reported a mortality risk, which was statistically significantly higher in patients with diabetes compared with that of patients without diabetes.23 This study was a database analysis that included 98.1% of patients in this review.
Overall, 7 of the 9 studies included in this review reported a statistically significantly higher complication rate among patients with diabetes or abnormalities in blood glucose levels compared with that of patients with normal blood glucose levels. Tanishima et al did not report an increase in postoperative complications among diabetic patients, but they included only 61 subjects and had only 1-year postoperative follow-up data for 43.6% of patients analyzed.18 Machino et al reported on operative time and blood loss values but did not investigate complications such as infection.21
An interesting finding from this review came from the study by Machino et al that analyzed cervical spondylotic myelopathy patients, demonstrating a delayed neurological recovery rate in diabetic patients or in patients who had uncontrolled postoperative blood glucose.21 This phenomenon was not found to be well studied during our literature review. It appears that there is currently very limited data regarding outcomes of neurological recovery in the surgically managed spinal trauma patient population or in patients with cervical spondylotic myelopathy. Tanishima et al investigated neurological recovery in patients with the same diagnosis and showed a trend toward improved recovery with better serum glucose (SG) control, but they did not find a statistically significant difference.18 From the data found in this review regarding higher rates of wound infections and medical complications in diabetic patients, one may expect similarly worsened outcomes for neurologic recovery, but this topic may require further exploration. It may also be worth researching whether more rigorous blood glucose control plays a role in neurological recovery after a traumatic spinal cord injury that is managed operatively. Given that patients who sustain traumatic spine injuries that meet indications for operative intervention are often polytrauma patients, it would be advantageous to understand whether we can significantly improve their overall outcomes, recovery, and mortality by tightly controlling blood glucose levels.
One limitation of this review was the lack of reporting on the use of intrawound antibiotic powder that is becoming common practice. How this plays a role in the reduction of infection for patients with better perioperative glucose control also remains to be seen. A recent study by Ushirozako et al included more than 1200 patients and found a decrease in the number of surgical site infections in both superficial and deep tissue in the vancomycin group vs the control group, but this was not statistically significant.27 However, when Ushirozako et al used baseline and surgical data of propensity score–matched patients, they found a statistically significant decrease in the occurrence of infection by half for the vancomycin group (P = 0.041). Additionally, a meta-analysis by Tailaiti et al included 27 studies with more than 17,000 subjects and reported that vancomycin significantly reduced the incidence of surgical site infection for those undergoing internal fixation of the spine (P = 0.01).28 Although patients with diabetes and abnormalities in blood glucose were included in these studies, there were no specifications made regarding the ability of vancomycin to improve outcomes based on the severity of their disease/blood glucose levels.
Another limitation of this review is the lack of standardization of the included studies regarding type of surgery, location of the spine, whether trauma patients were included, and level of evidence, as these factors can significantly alter results. Also, there is potential for human error in the reported SG levels because humans were responsible for performing the test and appropriately documenting this information. Additionally, we were unable to account for the possibility of patients receiving steroids, which are known to impact neurological deficits, pain control, control of dysphagia symptoms, and SG levels, in the perioperative period.
CONCLUSION
This systematic review will add to the current body of evidence regarding perioperative SG levels and their association with postoperative complications and infections. Most of the current literature suggests that elevated SG levels in patients undergoing spine surgery may lead to postoperative infections, and this review reinforced the current evidence. In addition, perioperative SG levels may be associated with the extent of neurological recovery after spine surgery when a deficit is present preoperatively, but further investigation may be warranted.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Gregory Grabowski reports payment/honoraria from DePuy Synthes (AO Faculty Honoraria); support for attending the AO Foundation meeting; and a leadership/fiduciary role for the Southern Orthopedic Society (board member). The remaining authors have nothing to report.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.