


Abstract
Background Lumbar spinal stenosis (LSS) is prevalent among octogenarians, causing significant pain and disability. Surgical intervention is often required because of the ineffectiveness of conservative treatments. This study investigates the efficacy and safety of biportal endoscopic decompressive laminectomy (BED) in octogenarians with severe LSS, evaluating its potential as a minimally invasive surgical option.
Methods This retrospective study included 107 patients aged 80 years or older who underwent BED for LSS between March 2017 and December 2022. Data were collected from electronic medical records, including demographic information, clinical outcomes, and surgical details. Patients with fractures, infectious spondylitis, herniated discs, and follow-up less than 12 months were excluded. Clinical outcomes were assessed using the visual analog scale, Oswestry Disability Index, European Quality of Life-5 Dimensions, and painDETECT at baseline and at 3, 6, and 12 months after surgery.
Results The mean age of the 107 patients was 84.1 years, with 59% being women. Significant improvements were observed in visual analog scale scores for lower back and lower extremities pain, Oswestry Disability Index, European Quality of Life-5 Dimensions, and painDETECT scores, indicating reduced pain, decreased disability, and enhanced quality of life. There were no significant differences in outcomes between patients aged 80 to 84 and those 85 or older. Surgery-related outcomes such as operation time, blood loss, and complications were similar in both age groups.
Conclusions BED is a safe and effective treatment for LSS in octogenarians, providing significant pain relief and functional improvement. This minimally invasive technique is also viable for patients older than 85 years, without increased risk of complications, supporting its broader indications in managing LSS in the elderly.
Clinical Relevance This study highlights the efficacy and safety of BED for LSS in octogenarians, demonstrating its potential to improve quality of life and function with low risks, making it a feasible option for elderly patients.
Level of Evidence 4.
Introduction
Lumbar spinal stenosis (LSS) is significantly more prevalent in geriatric patients aged 80 years or older. The degenerative changes in the spine frequently result in substantial pain and disability for these patients.1 Surgical intervention is often necessary to decompress the spinal canal, as conservative treatments, including physical therapy, medication, and injections, are often insufficient to provide adequate relief.2–4 Despite the inherent risks associated with their advanced age and comorbidities, decompressive laminectomy with fusion surgery provides significant pain relief and functional improvement in geriatric patients.5 Nevertheless, carrying out complex procedures such as interbody fusion in geriatric patients is difficult due to the existence of other medical histories, such as osteoporosis, cardiovascular diseases, and other systemic comorbidities. These factors exacerbate the likelihood of perioperative complications and prolong the recovery process.6
Minimally invasive techniques, particularly endoscopic decompression surgeries, have been increasingly adopted in recent years and have demonstrated good clinical results.7 These procedures provide substantial advantages over conventional microscopic laminectomy, such as shorter hospital stays, faster recovery periods, and reduced surgical damage.2,8,9 Endoscopic decompression has been demonstrated to yield comparable results to conventional open microscopic procedures, particularly in elderly patients.10 Recently, biportal endoscopic decompressive laminectomy (BED) has emerged as a minimally invasive surgical technique for treating LSS.11–14 A BED technique for LSS resulted in favorable clinical outcomes, reduced pain, and shorter hospital stays.15 Additionally, different minimally invasive decompressive surgeries for lumbar central stenosis were compared, including biportal endoscopy, uniportal endoscopy, and microsurgery, demonstrating the efficacy of biportal endoscopic approaches.16
This investigation aims to assess the efficacy and safety of BED in patients aged 80 and older, determining its feasibility as a favored surgical option for LSS. This research looks at the potential to improve the quality of life (QOL) for geriatric patients with LSS by investigating minimally invasive spine surgery techniques that address the specific challenges of advanced age.
Materials and Methods
Study Design and Patient Demographics
The design and protocol of this retrospective case series study were approved by the institutional review board at our hospital (B-2309-853-103). This study is a retrospective analysis of patients aged 80 years or older who underwent BED for LSS. The study was conducted at our institution from March 2017 to December 2022. The data were collected from electronic medical records and included patients’ demographic information, clinical outcomes, and surgical details.
We included patients who underwent BED for LSS aged 80 years or older. All patients had severe central canal stenosis classified as Schizas grades C or D. The exclusion criteria were as follow: fractures (n = 14), infectious spondylitis (n = 16), herniated intervertebral disc (n = 1), tethered cord syndrome (n = 1), thoracic myelopathy (n = 9), and less than 12-month follow-up or incomplete medical records during follow-up (n = 21).
After applying the exclusion criteria, 107 patients were included in the final analysis. The detailed demographic data and clinical outcomes of these patients were analyzed to assess the efficacy and safety of BED in this elderly population.
Surgical Procedures
The biportal endoscopic laminectomy technique is similar to microscopic decompressive laminectomy, with the main difference being the use of 2 portals.14 The surgery is performed with the patient in the prone position under general anesthesia. Using this procedure, enough working space is created for both the endoscope viewing portal and the working portal for the spinal instruments. The portals are located 0.5 and 1 cm lateral to the spinous process and are made under C-arm guidance. For a left-sided decompressive laminectomy, which is recommended for right-hand dominant surgeons, the working portal is located at the lower margin of the lamina with a 1-cm incision, while the viewing portal is positioned vertically 1 cm proximal to the working portal with a 7-mm incision. After making the skin incisions, the paraspinal muscles are detached from the lamina using a narrow Cobb elevator to create adequate working space. A 4-mm, 30° endoscope is inserted through the viewing portal under saline irrigation, maintained at a pressure of 30 to 40 mm Hg. Various instruments such as bipolar radiofrequency cautery, burr, Kerrison punch, and pituitary forceps are inserted through the working portal. Muscle and soft tissue debris are cleared using a shaver and bipolar radiofrequency cautery.
The laminectomy technique then proceeds similarly to microscopic laminectomy. A high-speed match-head burr is used to resect the ipsilateral lamina and spinous process base, creating space for instrument movement. An ipsilateral partial laminectomy is performed to facilitate ligamentum flavum (LF) detachment.
The ipsilateral lateral margin of the LF is identified with a Penfield dissector while resecting the hypertrophic facet joint medial margin. The LF is then split from the laminar undersurface to the lower laminar upper border and then removed by Kerrison punch or pituitary forceps. Using a dissector, the LF is detached from the contralateral lamina’s undersurface. After removing the contralateral LF, the lateral margin of the dural sac and traversing root pathway are inspected to confirm sufficient decompression. This procedure is repeated at each affected level (Figure 1).

Biportal endoscopic decompressive laminectomy in a 92-year-old woman. (A) Magnetic resonance image (MRI) showing severe central canal stenosis at the L4–L5 and L5–S1 level and moderate central canal stenosis at the L3–L4 level. (B) Postoperative MRI showed fully decompressed dura after surgery.
Outcome Assessment
Patient demographics, including body mass index, Charlson Comorbidity Index, and American Society of Anesthesiologists score, were recorded. Additionally, surgical details, such as the operated lumbar levels, operation time, blood loss, postoperative drainage, and length of hospital stay, were collected.
Patient-reported outcome measures were evaluated at 4 time points: preoperative (baseline), and at 3, 6, and 12 months postsurgery. Clinical assessments included the visual analog scale (VAS) for low back pain and radiating pain in the lower extremities, the Oswestry Disability Index (ODI),17 the European Quality of Life-5 Dimensions (EQ-5D) score,18 and the painDETECT questionnaire.19
The VAS pain score was used to measure the intensity of low back pain and radiating pain in the lower extremities. The VAS pain score ranges from 0 (no pain) to 10 (severe pain), with higher scores indicating greater pain intensity. The ODI score was employed to assess the level of disability in daily activities due to low back pain. It provides a subjective percentage score, with higher scores reflecting greater disability. The ODI is a widely used tool for measuring the functional status of patients with spinal disorders. The EQ-5D score was utilized to evaluate the QOL of the patients. This measure includes 5 dimensions of health: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D index score is converted to a value ranging from −0.066 to 1.000, with 1 indicating the best possible QOL. The painDETECT questionnaire was used to assess the presence and severity of neuropathic pain in the lower extremities. It consists of 9 questions, with a total score ranging from −1 to 38 points. A score below 12 suggests that neuropathic pain is unlikely, whereas a score above 19 indicates a high likelihood (>90%) of neuropathic pain.
To evaluate clinical outcomes during follow-up, we analyzed serial changes in patient-reported outcome measures from the preoperative period to the final follow-up at 12 months postsurgery. The primary outcomes were the changes in these scores over time and the comparison of these changes between the 2 age groups (80–84 years [Group 1] vs 85 years and older [Group 2]).
Surgery-related outcomes, including total postoperative drainage (mL), operation duration (minutes), postoperative hospital stay (days), and intra- and postoperative complications, were thoroughly analyzed. Total postoperative drainage was quantified as the amount collected in the Hemovac (Zimmer Biomet, Warsaw, IN, USA) drain system up to the second postoperative day. Operation duration was documented from the time of skin incision to skin closure, as recorded in the anesthesia log.
Statistical Analysis
Descriptive statistics were used to summarize the demographic and clinical characteristics of the study population. Continuous variables were reported as means and SDs, while categorical variables were reported as frequencies and percentages. The study population was divided into 2 groups based on age. Group 1 included patients aged 80–84 years, and Group 2 included patients aged 85 years or older. Statistical comparisons between the 2 age groups were conducted to determine whether there were significant differences in baseline characteristics and outcomes. For continuous variables, independent samples t tests were used to compare means between the 2 groups. For categorical variables, χ 2 tests were used to compare proportions. To assess the impact of decompressive laminectomy on clinical outcomes, we analyzed changes in clinical outcomes over time. To account for the repeated measures within individuals and to analyze the effect of time and age group on clinical outcomes, we used Generalized Estimating Equations (GEE) with an exchangeable working correlation structure and Gaussian family. The GEE models included the main effects of time and age group as well as their interaction terms to assess whether the change in clinical outcomes over time differed by age group. Stata/MP 17.1 (StataCorp LLC, College Station, Texas, USA) was used for all analyses. All statistical tests were 2-tailed, and results were considered statistically significant if P < 0.05.
Results
Demographic Characteristics
The demographic and clinical characteristics of the study population are summarized in Table 1. A total of 107 patients aged 80 years or older who underwent decompressive laminectomy for spinal stenosis were included in the study. The mean age of the patients was 84.1 years. The majority of the patients were women (59%). The mean body mass index was 24.5, and the mean American Society of Anesthesiologists score was 2.41. The mean Charlson Comorbidity Index score was 0.98. The most common levels of surgery were L3 to L4 and L4 to L5.
Demographic and clinical patient data.
Group Comparison Based on Age
The study population was divided into 2 groups based on age: Group 1 (aged 80–84 years) and Group 2 (aged 85 years or older). The demographic characteristics of the 2 groups are compared in Table 2. Statistical comparisons between the 2 age groups revealed no significant differences in most baseline characteristics.
Clinical characteristics according to age.
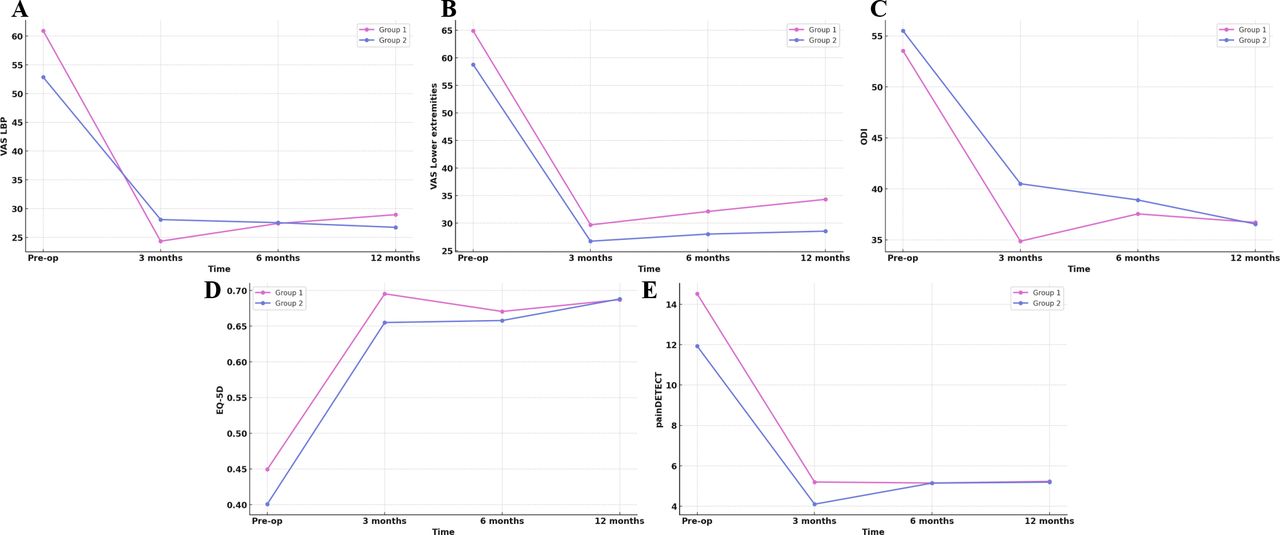
The results of the GEE analysis indicated that time had a statistically significant effect on all clinical outcomes, demonstrating significant changes in scores from baseline to follow-up periods. However, age group did not show a statistically significant effect on any of the clinical outcomes, suggesting that the improvements in clinical outcomes over time were similar across both age groups (Figure 2).

(A and B) Changes in mean VAS score for low back and lower extremities radiating pain, ranging from 0 (no pain) to 10 (worst pain). (C) Changes in mean ODI score, ranging from 0 (no disability) to 100 (high disability). (D) Changes in mean EQ-5D value, ranging from 0 (worst quality of life) to 1.000 (best quality of life). (E) Changes in mean painDETECT score, ranging from −1 (neuropathic pain less likely) to 38 (neuropathic pain most likely). VAS, visual analog scale; ODI, Oswestry Disability Index; EQ-5D, European Quality of Life-5 Dimensions.
The complications and surgery-related outcomes for biportal endoscopic laminectomy were compared between Group 1 and Group 2 as summarized in Table 3. The mean operation time, hospital stay, blood loss, and postoperative drainage were slightly longer and higher in Group 2 compared with Group 1, but the difference was not statistically significant. All complications, such as incidental durotomy, hematoma, surgical site infection, revision surgery due to recurrent symptoms, delirium, and pneumonia, were not significantly different. Furthermore, no major complications, such as surgery-related death, deep vein thrombosis, pulmonary embolism, stroke, cardiovascular event, and neurological injury, were observed.
Clinical and surgery-related outcomes for biportal endoscopy laminectomy during 12-month follow-up.
Discussion
This study evaluated the outcomes of BED in elderly patients aged 80 years or older with LSS. Our findings indicate significant improvements in patient’s symptoms without major complications. These improvements were also observed across both age groups (80–84 years and 85 years or older), with no significant differences between 2 groups. While most existing research has primarily focused on patients younger than 80 years, our study sought to investigate whether the benefits of minimally invasive surgery, such as biportal endoscopic techniques, could also be observed in super-aged individuals. The results suggest that biportal endoscopic surgery may offer meaningful benefits even in patients older than 80 years, including those older than 85, without an apparent increase in risk. These findings contribute to the ongoing discussion about the suitability of minimally invasive approaches in managing spinal stenosis in the elderly, particularly in those of advanced age.
Managing LSS in patients aged 80 years or older presents several challenges. While surgery is recommended for patients unresponsive to conservative treatments, symptomatic spinal stenosis is being recognized more frequently in older individuals who may not be suitable candidates for surgery due to their physical status.20 However, surgical treatment for LSS in carefully selected elderly patients has been shown to provide good results with acceptable morbidity.21 Advanced age is associated with a higher prevalence of comorbidities, reduced physiological reserve, and increased surgical risks.22 These factors complicate the perioperative management and postoperative recovery in this population. Although fusion surgery is an option for spinal stenosis, it has significant risks and may not be acceptable for many senior individuals due to extended recovery periods, increased risk for complications, and higher demands on their overall health.23 Given the complexities and risks associated with fusion surgery in the elderly, decompressive laminectomy is frequently preferred for patients older than 80 years.24 The decision between decompression alone and fusion surgery remains a topic of debate, with studies suggesting that decompressive laminectomy alone can yield favorable outcomes in elderly patients with advanced age or poor general condition.23
Previous studies have reported favorable outcomes with laminectomy in this age group, demonstrating its efficacy in relieving symptoms and improving function.25 Less invasive approaches such as unilateral microsurgical procedures have been increasingly utilized for decompression in elderly patients with LSS.24,26,27 These findings highlight the importance of considering laminectomy as a viable option for managing LSS in the elderly, emphasizing its role in improving symptoms and functional outcomes in this population. Full-endoscopic decompression procedures have been highlighted as advantageous due to their small incisions and rapid recovery, making them a viable alternative for treating LSS, especially in elderly patients with comorbidities.28 Additionally, endoscopic spine surgery under local anesthesia has been suggested as an effective option for elderly patients with poor general health, further supporting the utilization of endoscopic techniques in this population.29 However, the use of biportal endoscopic techniques has not been extensively studied in this population.
The emergence of novel techniques such as biportal endoscopic unilateral laminectomy for bilateral decompression has provided minimally invasive options for spinal stenosis treatment, emphasizing the importance of less invasive approaches in managing this condition.3,14 In our study, we performed biportal endoscopic laminectomy on a cohort of elderly patients, including those aged 80 years or older. Our results demonstrate that this minimally invasive technique provides significant symptom relief and functional improvement in high-risk elderly patients. Furthermore, the extremely advanced old age (≥85 years) was comparable to those in the 80- to 84-year age group, suggesting that even the oldest patients can benefit significantly from this procedure. The lack of significant differences in results between the 2 groups indicates that age alone should not discourage consideration of this minimally invasive surgical alternative for older patients with spinal stenosis. Notably, even among the oldest patients, biportal endoscopic laminectomy resulted in positive clinical outcomes, suggesting its safety and efficacy in this challenging patient population.
In our study, the incidence of dura tears was 14%, which is higher than the rates reported in the existing literature. This discrepancy is likely due to the inclusion of only elderly patients. It is plausible that the incidence of dura tears is higher in elderly patients because the dura mater is thinner in this age group compared with younger populations. Additionally, adhesions to the dura and LF may be more severe in cases of severe stenosis. Despite the higher incidence, the management of these tears was conducted in accordance with established protocols from previous studies, and all patients were treated successfully without any further complications.30
Limitations
This study has several limitations. First, its retrospective design may introduce selection bias, and the lack of a control group (younger than 80 years) limits the ability to compare outcomes with other surgical techniques. Second, the relatively small sample size and single-center nature of the study may affect the generalizability of the results. Additionally, making surgical treatment decisions for patients older than 80 years is challenging due to the high risk of complications, and surgery was only considered for those with severe spinal stenosis. This made it difficult to gather a large number of cases. Third, while follow-up was conducted for up to 12 months after surgery, longer-term outcomes were not assessed. Future studies should include larger cohorts, multiple centers, and extended follow-up periods to validate these findings.
Conclusion
BED is a safe and effective treatment for LSS in patients aged 80 years or older. This technique offers significant improvements in pain, function, and QOL, even among the oldest patients. These findings support the use of minimally invasive endoscopic techniques in managing spinal stenosis in the elderly, providing a viable alternative to more invasive surgical options.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.