


Abstract
Background Lumbar interbody fusion with screw fixation is a standard treatment for lumbar degenerative diseases. While full-endoscopic lumbar interbody fusion is minimally invasive, it utilizes smaller cages compared with the oblique lateral interbody fusion (OLIF) technique, which offers superior biomechanical support. To merge full-endoscopic lumbar interbody fusion minimal invasiveness with OLIF’s advantages, we developed a novel instrument, the Single Beak Adjustable Cage Glider, to facilitate OLIF cage insertion via the full-endoscopic trans-Kambin triangle approach. This note and case report introduce this alternative solution.
Case Presentation In a case of L4 to L5 spondylolisthesis, we performed fluoroscopy-guided uniportal facet-preserving trans-Kambin endoscopic fusion surgery. We initially installed percutaneous pedicle screws and rods to correct the anterolisthesis, then established the endoscopic trans-Kambin approach. After releasing the disc-endplate junction, the nerve root was mobilized and protected by the beak of the cage glider. The disc space was cleared, and a 22 × 40 × 12 mm interbody device was inserted through the cage glider under fluoroscopic guidance. The integrity of the exiting nerve root was confirmed with an endoscope.
Results Postoperatively, the patient experienced significant improvements in both low back pain and bilateral lower limb numbness. Muscle strength in both lower limbs returned to baseline, and the patient was able to walk independently without assistive devices. Follow-up radiographs and computed tomography scans showed a well-reduced regional lordotic angle, and the axial computed tomography view confirmed adequate decompression of the spinal canal while preserving the facet joints.
Conclusions The Single Beak Adjustable Cage Glider enables precise positioning of the OLIF cage through the Kambin triangle lumbar interbody fusion approach, avoiding nerve root injury and preserving facet joints. This technique reduces surgical trauma and maintains spine biomechanics, potentially improving patient outcomes.
Clinical Relevance This technique potentially reduces the cage subsidence rate.
Level of Evidence 5.
- degenerative spinal disease
- endoscopic fusion surgery
- novel spine technique
- full-endoscopic-KLIF
- reverse oblique lateral interbody fusion
Introduction
Lumbar interbody fusion combined with screw fixation is the criterion standard treatment for various lumbar degenerative diseases, such as spondylolisthesis, spinal stenosis, disc herniation, and degenerative scoliosis.1,2 This procedure can be performed via the anterior, direct lateral, oblique, or posterior approach, each offering distinct benefits and risks.1 Recently, advancements in full-endoscopic spine surgery have gained popularity due to their potential benefits of minimal invasiveness.3 With the introduction of large working cannula systems, both single-portal and biportal endoscopic systems are widely utilized in full-endoscopic lumbar interbody fusion (FE-LIF).3 FE-LIF can be performed in 2 ways: full-endoscopic transforaminal lumbar interbody fusion (TLIF) and full-endoscopic Kambin’s triangle lumbar interbody fusion (KLIF).4 Although there are slight differences in the positioning of the intervertebral cage between the 2 approaches, the cage used in FE-LIF has a smaller cross-sectional area compared with those used in the oblique lateral interbody fusion (OLIF) approach.5,6
To the best of our knowledge, current literature demonstrates that the OLIF construct, which provides a larger cross-sectional area, offers better biomechanical performance and more successful restoration of disc height, foraminal height, and lumbar lordotic angle.2,6,7 Therefore, to combine the benefits of minimal invasiveness associated with FE-LIF with the superior structural advantages of the oblique lateral cage insertion technique, we designed a novel instrument, the Single Beak Adjustable Cage Glider, to facilitate the insertion of the OLIF cage via the full-endoscopic trans-Kambin triangle approach. This technical note, along with a case report, illustrates the application of this method, providing an alternative solution for lumbar degenerative diseases.
Surgical Technique
Case Presentation
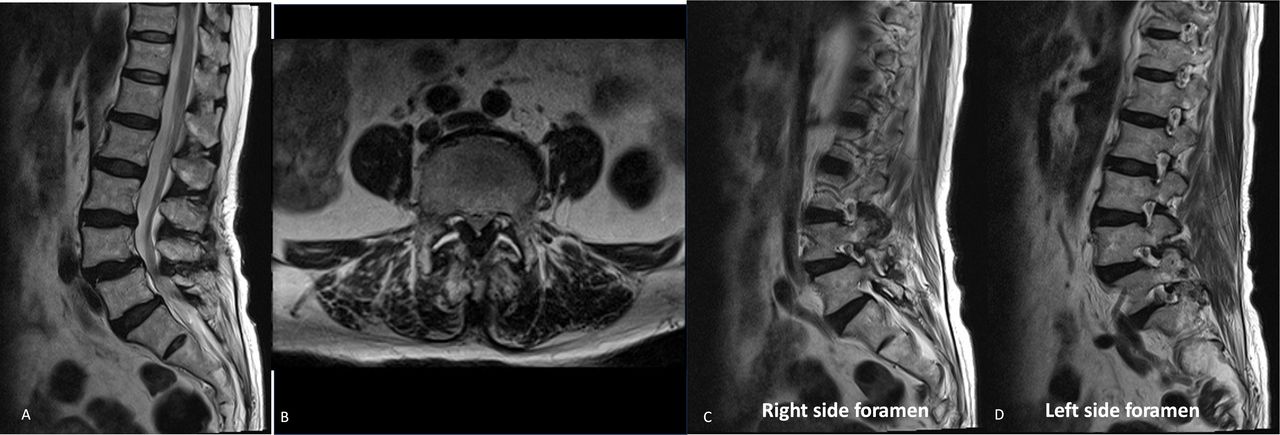
A 79-year-old woman presented with a 1-year history of progressive low back pain. She also reported bilateral lower limb weakness and numbness in the lower legs, with more severe symptoms on the right side. Although she could walk independently with a walker, she was barely able to tolerate long distances. Upon examination, muscle strength in the right lower limb was graded as 3 out of 5 points and in the left lower limb as 4 out of 5 points. Plain films of the lumbar spine revealed spondylolisthesis at L4 on L5 with Meyerding classification grade II (Figure 1). Magnetic resonance imaging indicated spondylolisthesis at L4 on L5 with minimal erosion, severe central stenosis, and bilateral foraminal narrowing. Ligamentum flavum hypertrophy and facet fluid sign were also observed (Figure 2). Bone mineral density, assessed by dual-energy x-ray absorptiometry, revealed a T-score of −3.0 at the lumbar spine and −3.4 at the femoral neck. She underwent a uniportal facet-preserving trans-Kambin endoscopic fusion surgery at L4 to L5.

X-ray images of the lumbar spine in anterior/posterior (A/P) (A), lateral flexion (B), and extension (C) views were taken for this 79-year-old woman who presented with progressive low back pain, as well as bilateral lower limb weakness and numbness over the years. There is evidence of reduced intervertebral disc spaces and spondylolisthesis at L4 on L5 with a Meyerding classification grade of II.

Preoperative magnetic resonance imaging. (A) A sagittal T2 image shows severe compression of the dural sac at the L4/L5 level. (B) An axial T2 image demonstrates severe compression of the dural sac at the L4/L5 level, with ligamentum flavum hypertrophy and bilateral facet fluid sign. (C) A sagittal T2 image reveals severe right-sided foraminal stenosis at the L4/L5 level. (D) A sagittal T2 image shows the left-sided foramen without stenosis.
The Single Beak Adjustable Cage Glider
The Single Beak Adjustable Cage Glider (shown in Figure 3) consists of a cylindrical body with a tapered, beak-like tip that plays a crucial role in protecting the exiting nerve root during surgery. This tip gently guides and keeps the nerve root away from the operative area while the interbody cage is being placed, minimizing the risk of nerve injury.

The Single Beak Adjustable Cage Glider features a cylindrical body with a tapered, beak-shaped tip. This tip delicately directs and maintains the nerve root away from the surgical site while positioning the interbody cage, thereby reducing the risk of nerve injury.
The tool is equipped with 2 adjustable knobs that enhance its versatility. The first knob, located at the base of the cylinder, allows for precise depth adjustment, enabling the instrument to glide smoothly into the correct position. The second knob is designed to adjust the width of the canal, giving the surgeon the ability to fine-tune the tool’s fit within the surgical site. This dual-adjustment capability ensures that the tool can adapt to varying anatomical conditions, providing both precision and safety during the procedure. The perpendicular extension at the base of the tool adds stability, allowing for controlled manipulation while protecting surrounding tissues and nerve roots.
Operation Technique
Under general anesthesia, the patient was positioned prone with all pressure points carefully padded. Fluoroscopic guidance was used to confirm correct positioning on the surgical table. After aseptic preparation and draping, small incisions were made to insert 4 percutaneous pedicle screws (5.5 mm diameter and 45 mm length) into the L4 and L5 vertebrae. The pedicle screws were augmented with cement due to osteoporosis. Prebent rods of appropriate lengths were placed on both sides. Once the screw-rod system was assembled, the L5 set screws on both sides were fully tightened, while the L4 set screws were initially left loose to allow controlled movement.
The anterolisthesis was partially reduced by gradually connecting and fastening the L4 set screws to the rods, aligning the displaced vertebra. The segment was then distracted using the extender, and the L4 set screws were further tightened to maintain the correction and ensure spinal stability (Figure 4A). At this stage, the Meyerding grade improved from grade II to I. To allow for controlled movement between the L4 pedicle screws and rods during subsequent steps, the L4 set screws were not fully tightened at this point.

Intraoperative fluoroscopic images and views of the full endoscopic Kambin’s triangle lumbar interbody fusion approach. (A) Pedicle screw fixation and rod placement were performed first to restore sagittal alignment and facilitate indirect decompression of the spinal canal. (B) An intraoperative fluoroscopic image shows the advancement of the Single Beak Adjustable Cage Glider into the disc space after cannula removal. (C and D) Intraoperative fluoroscopic images demonstrate the placement of the cage trial and the oblique lateral interbody fusion (OLIF) cage. (E) Direct visualization of the OLIF cage via the endoscope. (F, G, and H) The integrity of the exiting nerve root is confirmed after the removal of the cage glider. (I and J) Intraoperative fluoroscopic images display the final position of the screw-rod construct and cage placement. (K) Photograph of the patient’s surgical wounds.
Under fluoroscopic guidance, a guide wire was inserted, with its tip docking on the superior articular process of the caudal vertebra on the right side. Serial dilators were then introduced sequentially to reach the surface of the superior articular process. Finally, the 4.7 mm-wide cannula of the full endoscope was advanced to the disc level. At this point, the exiting L4 nerve root was identified in its anatomical location.
Discectomy was performed to access the disc space. A guide wire was inserted into the disc space, followed by the removal of the endoscope. Sequential dilators were then introduced into the disc space. After removing the cannula, the Single Beak Adjustable Cage Glider was advanced into the disc space (Figure 4B). Initially, the beak was docked on the endplate of the caudal vertebra and subsequently rotated ventrally and cranially to keep the nerve root outside the path of insertion during cage placement. The intended width of the inserted cage was 22 mm, and the ideal prepared disc space distance was 25 mm. To enlarge the size of the discectomy portal for cage insertion, the disc-endplate junction—the junction between the annular ring and the superior endplate of the caudal vertebra—was released from dorsal to ventral using the beak of the cage glider and cautery. The exiting nerve root was mobilized and protected by the beak during the release of the disc-endplate junction. After adequate release, a disc rongeur, disc shaver, and curette were used to clear the disc space and prepare the disc endplate. The interbody device (CLYDESDALE Spinal System, PEEK cage with Tantalum markers, length 40 mm, width 22 mm, and height 12 mm) was filled with demineralized bone matrix and inserted through the cage glider under fluoroscopic guidance (Figure 4C, D and E). This facilitated the complete reduction of the vertebrae and ensured proper alignment and stability.
The integrity of the exiting nerve root was confirmed using the endoscope (Figure 4F, G and H). After applying a compression force to the pedicle screws, both L4 set screws were fully tightened to complete the surgical procedure. The final positioning of the screw-rod system and the interbody cage was verified under fluoroscopic guidance to ensure proper alignment and stability (Figure 4I and J).
A hemovac drain was placed subcutaneously, and all skin incisions were closed (Figure 4K). The total operating time was 4 hours, and the estimated blood loss was approximately 50 mL.
Results
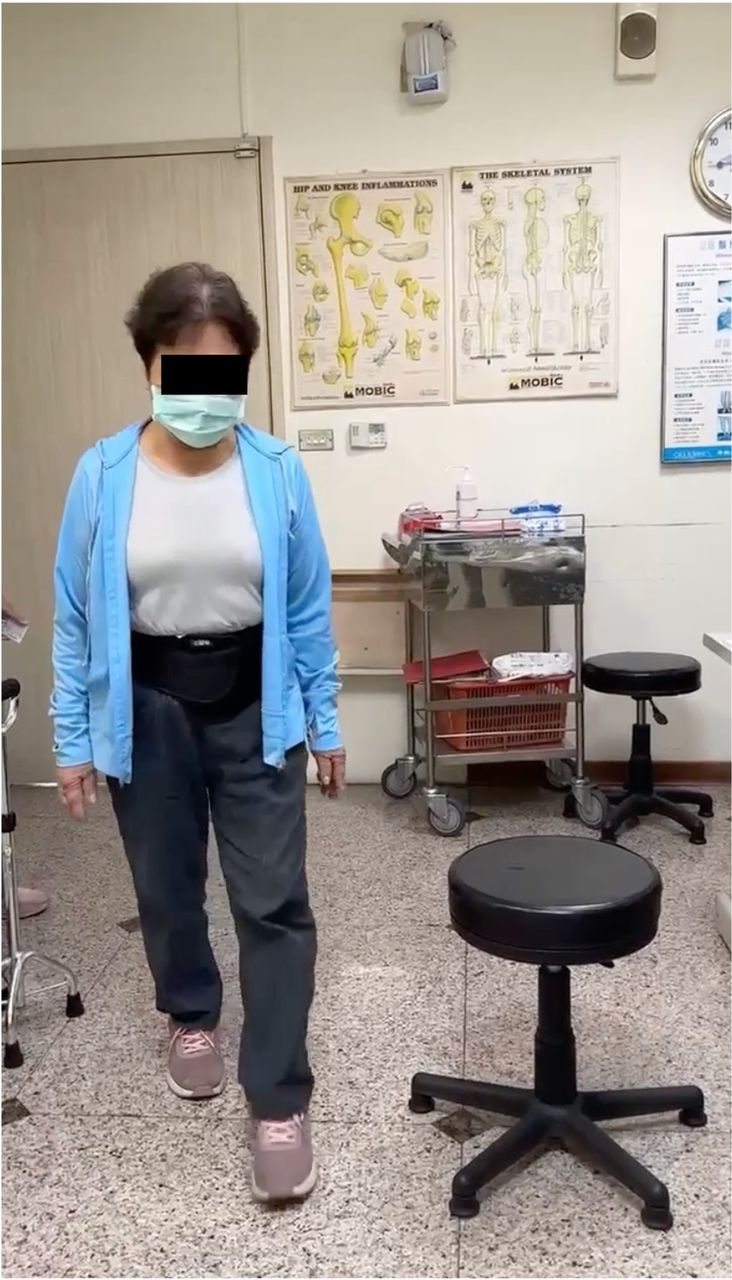
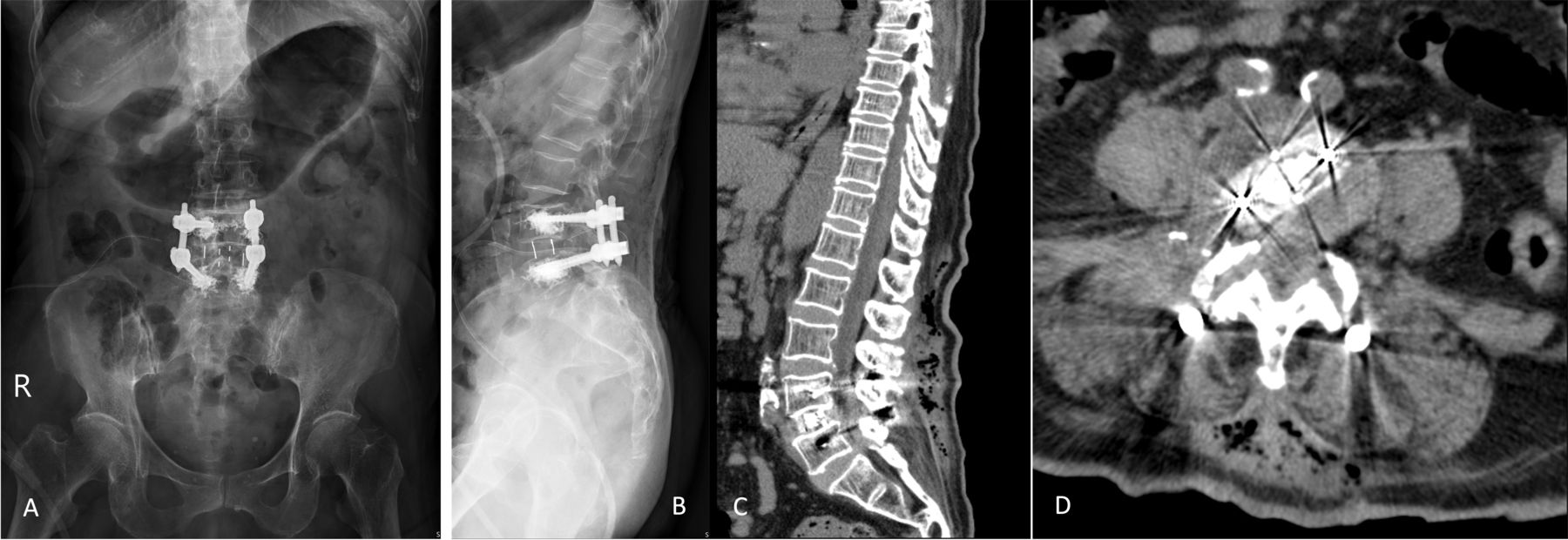
After the operation, the patient was instructed to wear a lumbosacral corset for 3 months. On the first postoperative day, a physical examination showed significant improvement in both low back pain and bilateral lower limb numbness. Muscle strength in the right lower limb was 4/5, as was the muscle strength in the left lower limb, which improved massively on postoperative day 2. The patient was able to walk with the assistance of a walker, though at a slow pace and with limited distance. A postoperative lateral radiograph revealed a reduction in anterospondylolisthesis and restored disc height at L4/L5. The patient was successfully discharged on the second day after surgery and participated in a postoperative rehabilitation program for 2 weeks. The surgical wounds healed without complications, and the patient experienced complete resolution of low back pain and lower limb numbness. Bilateral lower limb muscle strength returned to baseline, and the patient was able to walk independently without the need for assistive devices (Figure 5). Follow-up radiographs indicated intact screws with no signs of breakage and maintained sagittal plane alignment (Figure 6A and B). Computed tomography scans in the sagittal view revealed a well-reduced regional lordotic angle, indicating successful correction of the deformity (Figure 6C and D). Furthermore, the axial view of the computed tomography scan confirmed adequate decompression of the spinal canal without sacrificing the facet joints.

At the 2-week follow-up, the patient demonstrated independent ambulation without the use of assistive devices.

Postoperative anteroposterior (A) and lateral (B) radiographs show restoration of the sagittal alignment and the height of the L4/L5 disc. Postoperative computed tomography images demonstrate restoration of sagittal alignment and disc height in the sagittal view (C) and illustrate the cage insertion trajectory in the axial view (D), which reflects the reverse trajectory of the oblique lateral interbody fusion cage insertion.
Discussion
In this study, we present a surgical technique for reverse insertion of the OLIF cage using a full-endoscopic trans-Kambin approach, aided by the novel Single Beak Adjustable Cage Glider. This technique offers an alternative to the traditional OLIF approach, combining the minimal invasiveness of full-endoscopic surgery with the stability and enhanced deformity correction provided by larger cage insertion.
For lumbar degenerative diseases, the primary surgical objectives include reducing spondylolisthesis, restoring lumbar stability, re-establishing disc and foraminal height, and decompressing the spinal canal to relieve pain and promote neurological recovery. However, in lumbar interbody fusion surgery, cage subsidence is the most common and serious complication, potentially leading to the failure of reduction, indirect decompression, and even nonunion.8,9 To address this, many studies have advocated for the OLIF approach, which allows for the use of a larger cage that enhances stability, improves fusion rates, and restores natural disc height to correct sagittal imbalance. On the other hand, full-endoscopic KLIF has gained popularity in recent years due to its inherent minimal invasiveness, offering several advantages over traditional open procedures and even other minimally invasive approaches like OLIF or TLIF.10 However, according to the literature, the cage used in the KLIF approach is the same as the one used in the TLIF approach, which is typically smaller than the cage used in the OLIF approach.5 With the help of an adjustable cage glider, the exiting nerve root is protected and kept out of the operative zone without the need for direct visualization. Through the release of the disc-endplate junction, the space created by the release and discectomy is large enough to accommodate the insertion of an OLIF cage without sacrificing facet joints. Additionally, the diameter of the cage glider can be adjusted during the discectomy process to accommodate the larger OLIF cage.
Based on current literature, there are 2 main approaches regarding the order of pedicle screw and cage insertion in lumbar interbody fusion procedures. In FE-LIF, many surgeons prefer inserting the cage before final pedicle screw fixation to achieve proper indirect decompression and allow for optimal cage positioning before final screw tightening. However, in the full-endoscopic-KLIF technique described by Ishihama et al, the pedicle screws are inserted first.10 This approach allows for the potential reduction of listhesis and provides a frame of reference for the subsequent steps. In our experience, inserting the OLIF cage at one-third of the disc space can be challenging for patients with spondylolisthesis due to malalignment. Additionally, the reduction of spondylolisthesis may not be as effective when the cage is inserted first, as the tightly inserted interbody cage can impede proper alignment. Therefore, we have chosen to follow the surgical steps outlined by Ishihama et al,10 who prioritized pedicle screw insertion before cage placement.
With the advancement of OLIF surgery, various internal fixation instruments have been incorporated to increase the rigidity of the construct.11 In a biomechanical finite element analysis, Cai et al compared the biomechanical differences in OLIF when augmented by different instrumentations.12 They found that OLIF augmented with bilateral pedicle screws fixation retained the greatest ability to maintain lumbar stability, resist cage subsidence, and preserve disc height. The technique described in our study achieves this construct entirely in a prone position without the need to switch the patient’s position, potentially reducing operative time and decreasing blood loss due to less surgical wound exposure. Additionally, cage insertion can be performed from either the right or left side, which is an advantage over the traditional OLIF approach that is typically performed from the left side due to vascular anatomy.13
It is crucial to recognize the limitations of our report. First, it includes only a single patient with L4 on L5 spondylolisthesis, highlighting the need for additional research and practice to fully assess the safety and efficacy of this technique. Second, our approach necessitates the retraction of the exiting nerve root to release the disc-endplate junction, thereby allowing for an adequate discectomy and sufficient space for cage insertion. According to a study by Gerling et al, longer nerve root retraction times were associated with the onset of radiculitis and worse pain outcomes, averaging 13.8 minutes.14 In contrast, our surgical procedure required a retraction time of less than 2 minutes to perform the disc-endplate junction release, which is even shorter than the times reported for their group with favorable outcomes. However, further studies are necessary to validate the safety of this brief retraction time. Third, intraoperative neuromonitoring was not employed during this surgery; instead, we assessed nerve integrity through direct visualization. The patient experienced complete resolution of low back pain and lower limb numbness following the procedure. Intraoperative neuromonitoring, by providing real-time functional feedback on the nervous system, can offer reassurance to surgeons and help mitigate the risk of neural injury. Therefore, its use is recommended when the necessary equipment is available.
Conclusion
By using a specially designed instrument, the Single Beak Adjustable Cage Glider, the OLIF cage can be precisely positioned through the KLIF approach without injuring the exiting nerve root or sacrificing facet joints. This method not only minimizes the surgical footprint and associated trauma but also preserves the biomechanical integrity of the spine, potentially leading to improved patient outcomes.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the present article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.