


Abstract
Background Multiple techniques and implants can be used in ACDF, the newest of which are integrated cage and screw constructs. These devices may be beneficial over anterior plate constructs due to a negligible anterior profile that may reduce dysphagia. The goal of this study is to review the early radiographical and clinical results associated with a low profile integrated intervertebral cage in one- and two-level anterior column fusions.
Methods Fusion rates, incidence of hardware failure and deformity correction were assessed through 1 year. Patientreported scores, including VAS for neck pain, and improvements in axial neck pain and neurologic deficit from the preoperative baseline were quantified at 3, 6 and 12 months post-operatively. The incidence of dysphagia was recorded.
Results Lordosis and disc space height at the operated levels increased an average of 4.5° and 3.3mm after device placement (p<0.001). Sagittal plane correction was maintained at 1 year. VAS improved from an average of 5.1 preoperatively to 3.1 immediately postoperatively and was maintained at 12 months. At 3 months, patient-reported improvements in axial neck pain and neurologic deficit were 85% and 93%, respectively. Reported improvements were sustained for both parameters at 12 months (77% and 86%, respectively). Fusion was noted in 93% of the operated levels. There were two documented cases of dysphagia that lasted more than 5 weeks, both following two level ACDFs with the test device (3.5% rate of chronic dysphagia).
Conclusions The low profile integrated device improved lordosis at the operated level that was maintained at 1 year. Fusion rates with the new device are consistent with ACDF using anterior plating. In combination with improvements in pain and a minimal rate of dysphagia, study findings support the use of integrated interbody spacers for use in one- and two-level ACDF procedures.
Level of Evidence Level IV, Case Series.
- Anterior cervical discectomy and fusion
- integrated interbody spacer
- radiographic fusion
- clinical outcomes
Introduction
Cervical degenerative disc disease is a very common problem. Related neurological symptoms include radiculopathy and myelopathy, which can arise from trauma, activities that increase stress on the cervical spine and the normal process of aging. Symptoms are routinely initially treated with conservative measures ranging from physical therapy, chiropractic treatment, oral pain or anti-inflammatory medications, and epidural steroid injection. When these less invasive measures fail to satisfactorily relieve symptoms, surgical intervention is warranted. Surgical options include cervical total disc replacement, posterior foraminotomy, anterior partial discectomy and foraminotomy, anterior cervical discectomy and fusion (ACDF), and posterior decompression with or without fusion.
Clinical literature indicates single-level ACDF fusion rates ranging from 83%-97% using autografts and 82%-94% using allografts with concomitant relief of arm and neck pain.1, 2 The technique for ACDF was simultaneously and independently reported by Cloward as well as Smith and Robinson in 1958. Since that time the technique has evolved and includes several options for implants including disc spacers made of autograft or allograft bone, porous metal, polyether ether ketone (PEEK) and anterior plates and screws. The addition of anterior plates and screws was first reported by Orozio in 1970.
Benefits of anterior plates and screws include improved biomechanical fixation, higher fusion rates and decreased need for cervical collars after surgery.1, 2 Resultantly, the use of anterior plates and screws in ACDF is common practice today. Potential drawbacks of plating include the anterior profile of the plate, which may be related to chronic dysphagia after surgery.3–5 There is also the added risk of plate migration that may result in catastrophic esophageal perforation.6 Additionally, studies have reported increased adjacent level ossification when the plate is within 5mm of the disc above or below the operative level.7 Park et al. reported adjacent level ossification in 67% of the levels above the surgical level when the plate was <5mm from the superior disc and only 24% when >5mm away. In the level below, ossification was seen in 45% versus 5% when the plate was within 5mm or farther than 5mm, respectively.7
Recently new implants have been designed for ACDF to address some of the issues with anterior plates and screws. These implants are commonly described as zero or no profile integrated cage and screw implants. They sit just dorsal to the anterior cortex of the cervical vertebral body, completely contained within the intervertebral disc space. Potential benefits of this implant include decreased dysphagia, lower risk of migration, and lower incidence of adjacent segment degeneration.
As clinical data regarding the utility of these devices are sparse in the literature, the purpose of this study was to evaluate the early (12 months) clinical and radiographic results of ACDF performed with a zero anterior profile cage and integrated three screw implant.
Materials & Methods
A retrospective review of all one- and two-level ACDFs was performed from 2010 to 2013 on all patients who received the test implant. All procedures were performed by two fellowship-trained spine surgeons at a single institution using a standard Smith Robinson anterior approach to the cervical spine. All patients had at least 12 months follow-up. Inclusion criteria for the study were cervical pathology suitable for treatment with ACDF, age greater than 18 years old, and 1-2 diseased cervical levels. Exclusion criteria included need for posterior fixation, greater than 2 affected levels, and history of dysphagia prior to surgery. Fifty-seven patients (36 females; 21 males) with 73 operated levels met our inclusion criteria and were followed clinically and radiographically for 12 months.
The test implant was a PEEK interbody cage with 6 degrees of lordosis and three integrated screws (STALIF C, Centinel Spine, West Chester, PA). Implants were available in two styles, one with a domed superior surface, and one with a flat superior surface. Each implant had three screws. The midline screw is designed to be directed superiorly, and the inferior screws are meant to be directed inferiorly and converge in the midline. Implant sizes ranged from 5.5-9.5mm in height in tapered versions, with the domed versions adding 1.44mm of height at the dome peak. The PEEK cage has an open void in the center that was filled with bone graft and/or substitute. Osteocel (Nuvasive, San Diego, CA) and local autograft bone were used in 22 patients while 27 patients received Grafton DBM Gel (BioHorizons, Birmingham, AL) and allograft cancellous bone chips. DBX putty (DepuySynthes, Westchester, PA) and allograft cancellous bone chips were used in 5 patients. Local autograft and allograft cancellous bone chips were used in 3 patients.
Change in lordosis and intervertebral disc height at the operated levels was evaluated immediately postoperatively and at 1 year (lordosis only). Fusion status, VAS for neck pain, NDI, patient-reported improvement in neck pain and neurologic symptoms, and incidence of dysphagia were evaluated at 3 months, 6 months and 12 months postoperatively.
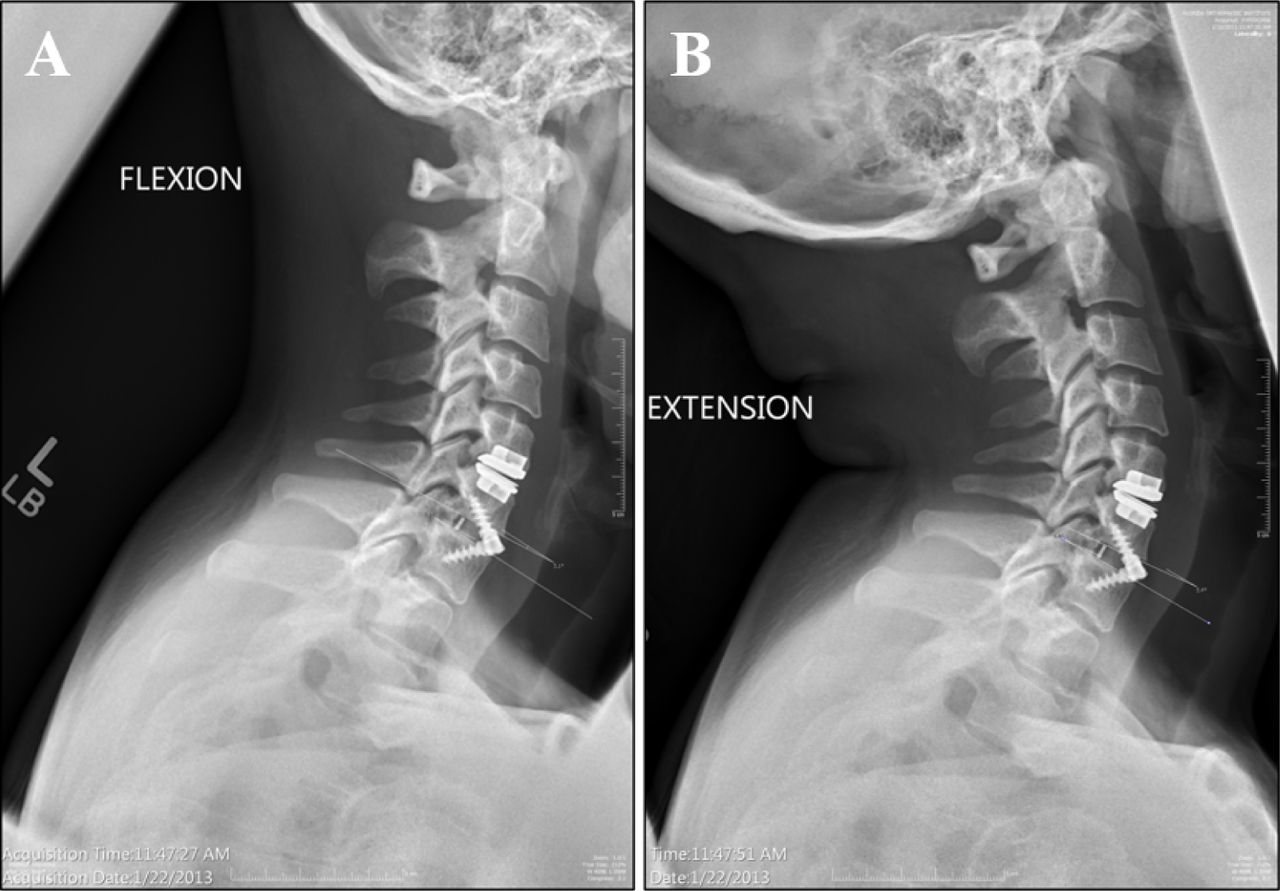
Radiologic outcomes were measured using plain lateral radiographs of the cervical spine taken at each postoperative visit from immediately after surgery until 12 months. Radiographs were taken using a standardized protocol in which the radiology technician instructed the patient to stand perfectly straight and as close to the detector as possible. The only exceptions to plain radiographic analysis were the cases where CT was available to determine fusion status. Disc height was measured on preoperative and immediate postoperative radiographs and determined by measuring the distance from the posterior inferior aspect of the superior vertebral body to the posterior superior corner of the inferior vertebral body. This location was used versus the anterior disc height as it was felt this would give a better measurement of the increase in vertical neural foramen height and therefore indirect decompression of the foramen. Radiographic images were calibrated for disc height measurement using a calibration scale placed in the x-ray field at the level of the detector. Lordosis was determined at the operative level by measuring the angle between the superior endplate of the superior vertebral body and the inferior endplate of the inferior vertebral body. The combination of disc height and lordosis at the operative level was additionally used to determine the incidence of implant subsidence after surgery. Fusion status was determined one of two ways. If a CT of the cervical spine was available that showed a solid fusion, this study was used. If no CT was available, flexion/extension xrays were used to monitor for motion at the operative level (Figure 1). A level was deemed to be fused if a difference of 2° or less of intervertebral motion at the operated level was measured between the full flexion and full extension radiographs. This motion threshold has been utilized in prior literature assessing fusion after ACDF in the cervical spine.8–11 All imaging studies were evaluated by a board certified musculoskeletal radiologist blinded to the purpose of the study.
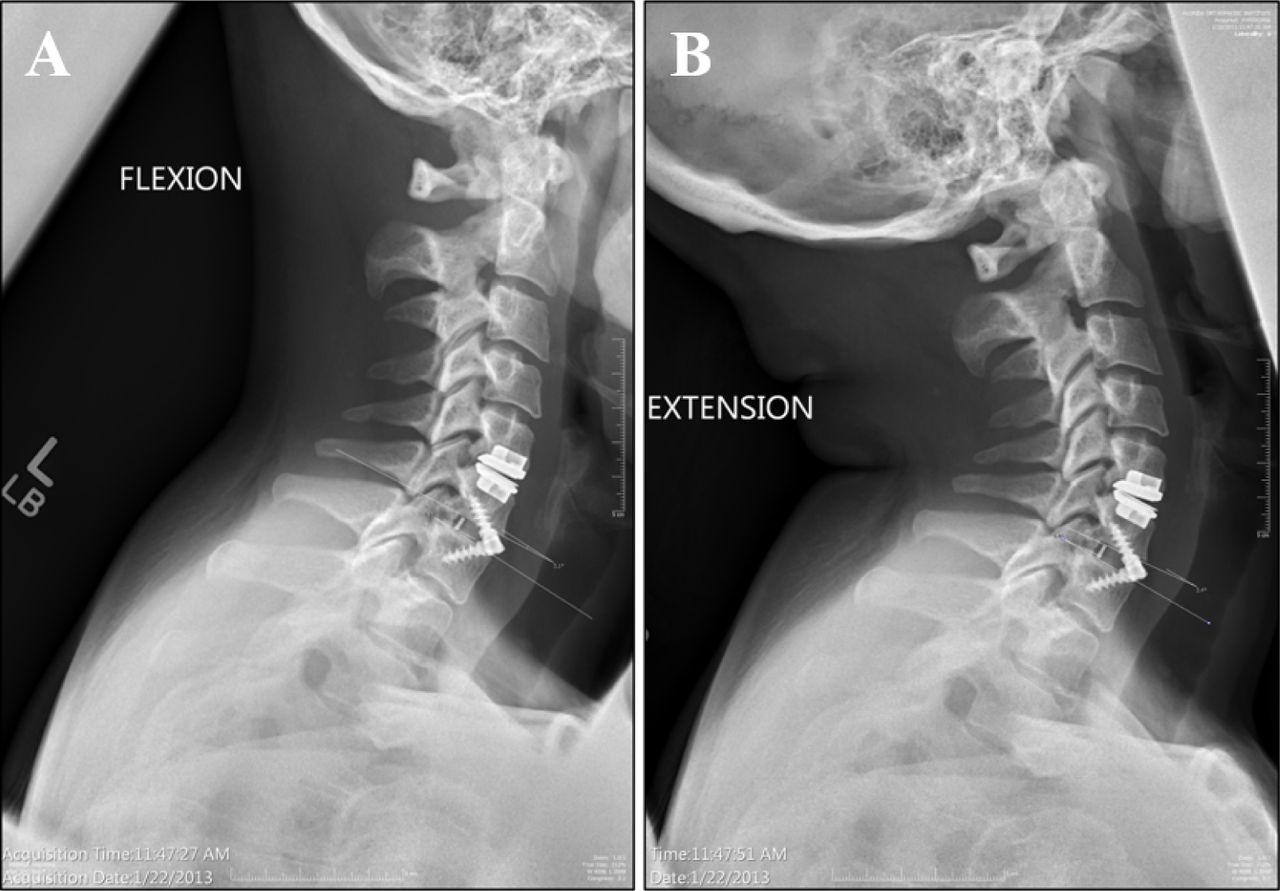
Lateral flexion (A) and extension (B) radiographs of the cervical spine with the test device implanted at C6-C7. The operated level was noted as being fused if intervertebral motion of less than 2° between full flexion and full extension was measured on the x-rays.
Patient-reported outcomes included improvement in axial neck and arm pain, and the presence or absence of dysphagia. VAS and NDI score were obtained at each clinical visit. Change in disc height from the pre-operative baseline to the immediate postoperative was compared with a paired t-test (SPSS, v22, IMB, Armonk, NY). Change in lordosis at the operated level over 12 months as well as improvements in clinical measures were determined with a repeated measures analysis of variance (RM-ANOVA) with Bonferroni correction. Significance was set at α = 0.05.
Results
Of the 73 operated levels, 41 were single-level ACDFs and 16 were two-level ACDFs (Figure 2). The majority of single-level ACDFs were performed at the C5-C6 level (Table 1). Of the 16 two-level ACDFs, the most frequent was implantation at C5-C6 and C6-C7. Operative time was 110 minutes (±42), and blood loss was 89cc (±45). The most frequent implant used was the tapered 6.5 mm interbody cage (47% of all cases) (Table 2). Domed interbody cages were used in two operated C5/C6 levels (3%) in two patients due to endplate concavity. The most commonly used screws were 15mm (57%) and 16mm (35%) in length. We documented one hardware failure in our patient cohort, manifested as breakage of a single screw, which did not require any further treatment. The patient was asymptomatic, and the radiographic correction obtained from surgery was maintained at the last visit.

Pre-operative radiographs of patients undergoing two-level (A) and one-level (E) ACDF with the test device. Immediate postoperative AP and lateral images (B,C) and (F,G) and lateral radiograph of the two-level (D) and one-level (H) fusions taken one year after the surgery.
Frequency of 1-Level ACDFs with the test device.
Summary of interbody device sizes implanted.
Forty-two patients (age 29-73) with 57 out of a total of 73 operated levels had appropriate imaging available to evaluate fusion status. Of the 57 operated levels, 54 were found to be solidly fused resulting in a fusion rate of 93% (Table 3). The 4 operated levels that did not fuse were in two patients that underwent two-level ACDFs. Lordosis was significantly improved immediately postoperatively compared to baseline films an average of 4.5 degrees (p<0.001) (Table 4). Lordosis was maintained at one year postoperatively at 4.5 degrees. Intervertebral disc height also significantly increased on average 3.3mm from 4.3 ± 1.4 mm pre-operatively to an average of 7.6 ± 1.2 mm after surgery (p<0.001). No evidence of cage subsidence was noted radiographically.
Summary of graft material used and associated fusion rates.
Postoperative increase in lordotic angle on a per level basis.
Thirty patients had complete outcomes data at the one year time point. VAS for neck pain improved from an average of 5.1 (range 2-10) preoperatively to 3.1 (range 0-9) immediately postoperatively (p<0.001) and was maintained at 3.3 (range 0-9) at 12 months. NDI decreased from 39.8 (range 16-94) at the pre-operative baseline to 28.0 (range 12-82) (p = 0.053) at 3 months and was maintained at 25.0 (range 10-82) at 1 year. At 3 months, patient-reported improvements in axial neck pain and neurologic deficit were 85% and 93%, respectively. Reported improvements were sustained for both parameters at 12 months (77% and 86%, respectively). Twenty patients did not have complete clinical outcome scores at 1 year, representing a 35% lost to follow-up rate.
Fourteen patients (25%) reported dysphagia at some point postoperatively. Ten cases resolved in 2 weeks, and 2 cases resolved in 5 weeks. The remaining 2 patients continued to have some dysphagia at the one year mark, both of which were 2-level ACDFs. The rate of chronic dysphagia was 3.5% in our patient cohort surgically treated with the integrated interbody devices.
Discussion
Stand-alone cage and screw implants for ACDF are a relatively new class of devices used for surgical treatment of cervical spine pathology. Stein et al.12 evaluated the same test implant used in our clinical study against locked anterior plate fixation at a single level in human cadaveric spines and concluded that the integrated screw and cage implant conferred nearly equivalent acute biomechanical stability to traditional plating (within 1° of motion in all loading modes). Similar biomechanical findings were recently reported by the same group over two contiguous cervical spine levels.13 These and other similar studies14 provide biomechanical evidence supporting the use of integrated spacers as an alternative to rigid anterior plating for ACDF procedures.
Studies on the short- and medium-term clinical efficacy associated with the use of these devices are beginning to emerge due to their relatively recent introduction in the cervical spine implant market. Barbagallo et al.15 reported on 85 patients with 4 year follow up using a zero profile stand-alone cage and screw implant. SF-36 and NDI showed a statistically significant improvement (p < 0.01) and mean arm pain VAS score decreased from 79 to 41. X-rays and CT demonstrated, respectively, a 94.5% and a 92% fusion rate. Three patients complained of moderate and two of mild transient dysphagia (15.5%). No device-related complications occurred and no fractures were reported. They found the zero profile device to be safe and effective, even on multilevel cases. This series has the longest follow up to date.15
Hofstetter and coworkers16 compared the incidence of dysphagia in ACDF with an anterior plate versus a stand-alone cage and screw construct. They looked at 70 patients total, 35 with an anterior plate and 35 with a zero profile stand-alone cage and screw implant. Radiographs showed increased prevertebral swelling in the anterior plate group out to six months. There were also 7 patients in the anterior plate group that complained of dysphagia compared to only one in the zero profile group.16 In the current study, we only had 2 patients with dysphagia that lasted more than 5 weeks, and both patients were two level ACDFs. This gave us a chronic dysphagia rate of 3.5%, which compares favorably with dysphagia rates in other studies evaluating these new interbody devices. 17–22 Yue et al.22 reported a chronic dysphagia rate of approximately 35% in patients who underwent ACDF using an anterior plate with a 5-11 year follow up. Riley et al.19 reported a dysphagia rate of approximately 11% and 24% at 2 years after surgery in one- and two-level plated constructs, respectively. Similar to our findings, Li et al.17 demonstrated a trend towards decreased incidence of dysphagia with a zero profile implant versus an anterior plate. They looked at 46 patient's prospectively, 23 in the zero profile group and 23 in the anterior plate group. At all time points, the control group with the anterior plate reported more dysphagia than the test group with the zero-profile implant. At one year postoperatively, 4 patients in the control group reported mild dysphagia compared to no reported dysphagia in the test group.
We noted only a single instance of hardware failure in our study cohort, which manifested as breakage of a single screw. The patient was asymptomatic at the index level, no further treatment was deemed necessary and the operated level went on to radiographic fusion. Migration of hardware is of particular concern with anterior cervical plates as the consequences of prominent anterior hardware can be severe, and range from dysphagia to esophageal perforation as described in other studies.3–6 Further, at one year we identified no instances of subsidence of the integrated interbody spacer. Our finding is in agreement with those of Scholz et al.23 who also reported early radiographic outcomes with a similar test device. Certainly, longer follow up is necessary to confirm our findings at 12 months.
Our fusion rate in this study was 93%, consistent with published ACDF fusion rates. Kaiser et al.1 reported single- and two-level ACDF fusion rates with an anterior plate and cortical allograft of 96% and 91%, respectively. Song et al.24 compared the fusion rates of ACDF with anterior plate and cage versus cage only. They found a fusion rate of 97.5% in the plated group versus 78.9% in the cage only group. Again, our fusion rate in this study was similar to the rates found for constructs using anterior plates. Barbagallo et al.15 tested a similar zero profile cage and screw implant and reported a 92% fusion rate on CT.
Our patient satisfaction rates with symptom improvement and improvement in VAS scores were also similar to established success rates in ACDF of approximately 90% or better.7, 16 Patients reported improvements in neck and arm pain of 77% and 86%, respectively, one year out from surgery. Zero profile stand-alone cage and screw implants perform comparably to cage and anterior plate constructs in terms of fusion and patient rated factors such as symptom relief. 15, 17
Our study has several limitations. Firstly, the radiographic measurements were performed by a single observer and thus we have no measure of inter-rater reliability. However, prior work by our group in a study of similar scope indicates that such radiographic measurements can be performed with a high degree of correlation between observers (intraclass correlation (ICC) = 0.986).25 Secondly, we acknowledge the potential for linear distance measurement error (i.e. disc height). We attempted to minimize this error by utilizing a standard imaging protocol, but, nonetheless, we acknowledge that slight deviations in patient positioning as well as parallax may affect the measurements. Thirdly, this was a retrospective study and we acknowledge a moderate lost to follow up rate with 20 patients lacking complete clinical outcomes data at 1 year post-operatively and only 42 patients having radiographical data to assess fusion. In an attempt to minimize our lost to follow-up rate, we made multiple attempts (x3) over a three month period to contact all patients with incomplete data.
Finally, this is a relatively small patient cohort that demonstrates similar fusion rates and clinical improvements to patients historically treated with rigid anterior plating. However, our cohort size is similar to previously published work describing the clinical efficacy of this new class of cervical fusion implants. Future studies should include prospective analysis with more patients and comparative cohorts to truly define the clinical utility of these implants.
In conclusion, the low profile integrated device studied here improved cervical spine sagittal balance at the operated level and the correction was maintained at 1 year. Reported fusion rates with the new device are consistent with ACDF using anterior plating. In combination with patient-reported improvements in pain and a minimal rate of dysphagia, study findings support the use of integrated interbody spacers for use in one- and two-level ACDF procedures.
Disclosures
Antonio Castellvi was a consultant for Centinel. The other authors declare no relevant financial disclosures.
- Copyright © 2015 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
References
In this issue




{kind=link}
{kind=link}