


Abstract
Background The anteriorly displaced type II odontoid fracture is treated either conservatively by halo-vest brace immobilization or surgically by posterior atlantoaxial fusion. Anterior odontoid screw fixation is not advised for this pattern of odontoid fracture because of the difficult trajectory for screw insertion despite its advantage of salvaging the upper cervical spine rotatory range of movement. This article presents a new transoral manipulation technique for reduction of anteriorly displaced type II odontoid fracture and review of the literature.
Methods A 24-year-old man presented 2 weeks after a motor vehicle accident with anteriorly displaced type II odontoid fracture. Intraoperatively, after unsuccessful attempts to reduce the anteriorly displaced type II odontoid fracture, complete reduction of the odontoid process and proper screw placement were achieved by direct transoral manipulation with an army-navy hand retractor. Additional manual pressure on the spinous process of the cervical spine at the same time has resulted in better reduction. The patient was followed up neurologically and radiologically to assess the reduction and healing of the odontoid fracture.
Results Postoperatively, the patient was neurologically intact, and his computed tomography cervical spine scan showed proper placement of the odontoid screw with adequate reduction of the odontoid process. At the 3-month follow-up, the patient was neurologically intact and had painless full range of cervical spine movement, and his computed tomography cervical spine scan showed a well-healed odontoid fracture.
Conclusions Direct transoral manipulation with an army-navy hand retractor can be used to assist in reducing the anteriorly displaced type II odontoid fracture during anterior odontoid screw fixation.
Fractures of the odontoid process comprise 18% to 20% of cervical injuries, of which 65% to 74% are type II fractures.1 Management of type II odontoid fractures includes either conservative halo-vest immobilization, which has a higher rate of nonunion because of the disruption of the odontoid process vascular supply, or surgical treatment, which is more preferred in acute cases.2, 3 Posterior C1-2 wiring and bone fusion comprise a common surgical technique, but they require external support until the completion of the bone fusion and yield a fusion rate of about 74%.4
Posterior C1-2 transarticular or transpedicular screwing is an alternative surgical technique, which provides a more rigid fixation The demerit of the posterior fixation procedures is the elimination of the normal C1-2 rotatory motion (which accounts for >50% of all cervical spine rotatory movements), as well as the reduction of cervical spine flexion-extension by 10%.5
Anterior odontoid screw fixation was presented by Bohler6 in 1982. In this technique, C2 is the only vertebra to be involved in the surgical procedure. This fact singles out anterior odontoid screw fixation as a more physiological technique in comparison with posterior fixation techniques. In addition, it provides immediate spinal stability, rapid patient mobilization, and minimal postoperative pain, and it preserves the normal axial rotation between C1-2 that is needed especially in a young person with high-demand activities. Moreover, the anterior screw fixation technique has a fusion rate of approximately 90%.4, 7
Contraindications to the anterior odontoid screw fixation technique include a short neck and barrel-shaped chest, which are unfavorable for the screw's trajectory; atlantal transverse ligament disruption; fracture nonunion; and irreducible displaced odontoid fracture.8
This article presents a new transoral manipulation technique for reduction of an anteriorly displaced type II odontoid fracture during anterior odontoid screw fixation.
Methods
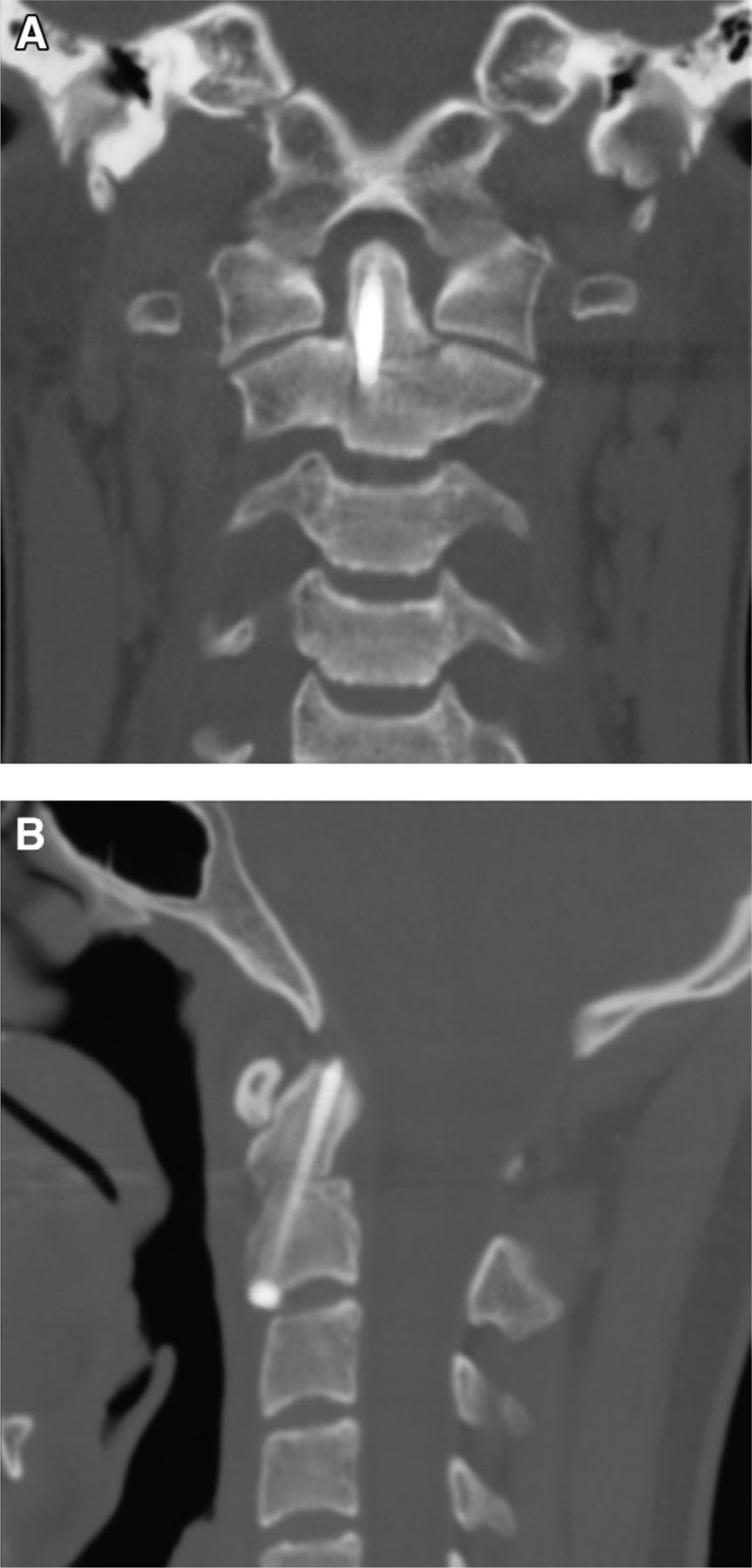
A 24-year-old male patient presented with type II odontoid fracture, due to a motor vehicle accident 2 weeks earlier. He had severe neck pain on admission without neurologic deficits. A computed tomography (CT) scan of his cervical spine showed a type II anteriorly displaced (6.2 mm) odontoid fracture (Fig. 1).
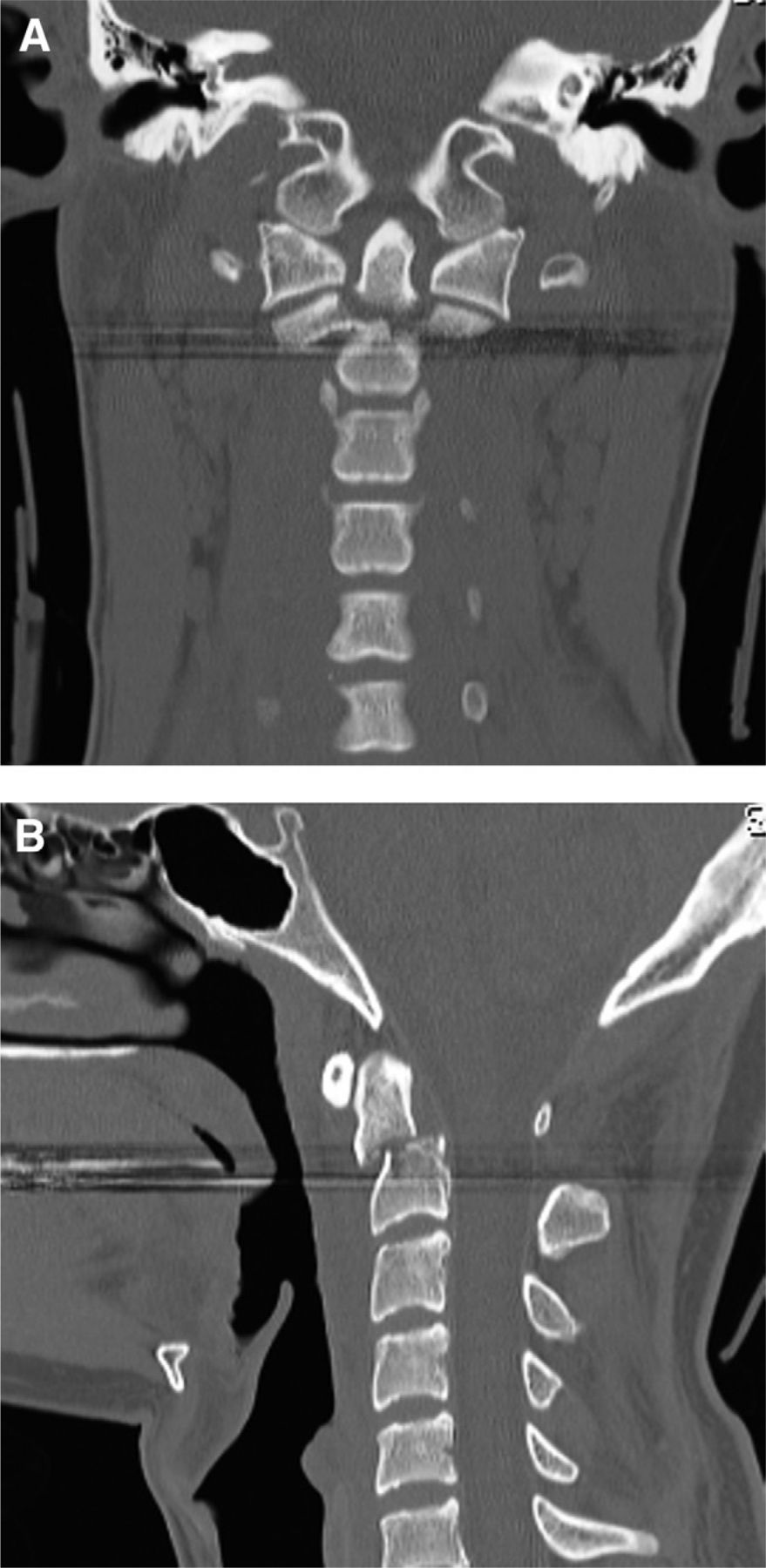
Preoperative CT cervical spine scans. (A) The coronal CT scan showed a type II odontoid fracture. (B) The sagittal CT scan showed an anteriorly displaced odontoid process (6.2 mm).
The surgical options were discussed with the patient, and we decided to perform the anterior odontoid screw fixation procedure to treat the unstable odontoid fracture.
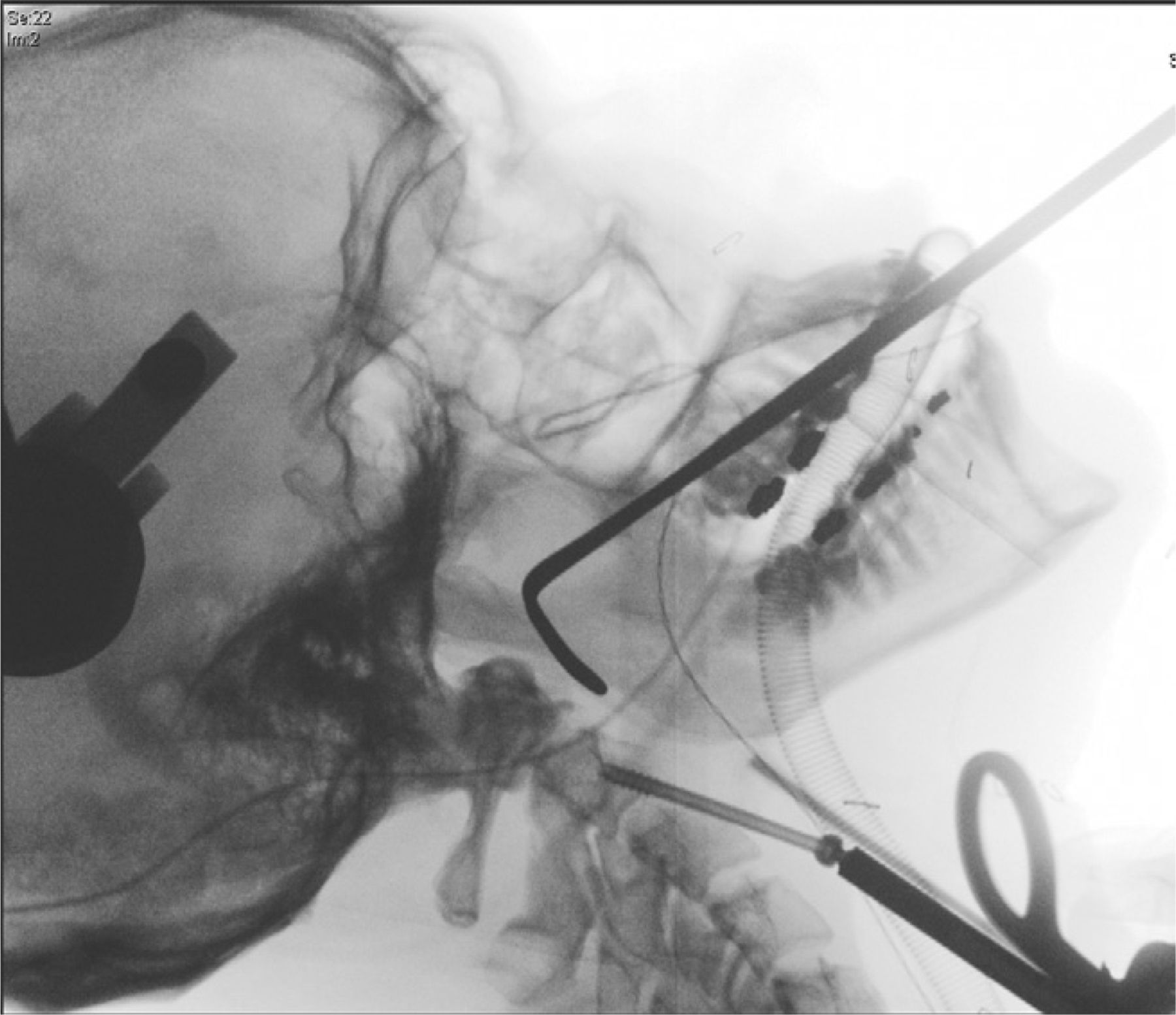
With the patient under general anesthesia by use of Fiberoptic intubation with somatosensory evoked potential and electromyography monitoring, a Mayfield 3-pin head holder was applied to secure the head. A radiolucent mouth block was used to keep the mouth open to provide an anteroposterior view of the odontoid process. A bi-planar fluoroscope was brought into position, and closed reduction under fluoroscopic guidance was attempted by use of combinations of distraction with flexion or extension without success. After the standard exposure for odontoid screw placement had been performed, the anteriorly displaced odontoid fracture remained misaligned. At that point, under lateral fluoroscopic imaging, the blade of an army-navy hand retractor (25 mm) was introduced into the oropharynx, with exertion of continuous pressure directly applied over the posterior pharyngeal wall and anterior to the arch of the atlas, resulting in nearly anatomic reduction of the displaced odontoid fracture. Additional pressure on the spinous process of the cervical spine in the back of the neck at the same time has resulted in better reduction. While pressure was applied on the odontoid process, the guidewire passed through the C2 body, crossing the fracture site, followed by insertion of a lag, partially threaded cannulated odontoid screw (4.0 × 36 mm). The surgeon was ready to remove the guidewire once the reduction was achieved and the odontoid screw passed the fracture site to avoid guidewire breakage (Fig. 2). The screw appeared to be holding satisfactorily when the neck was gently placed through a range of flexion and extension under fluoroscopy.
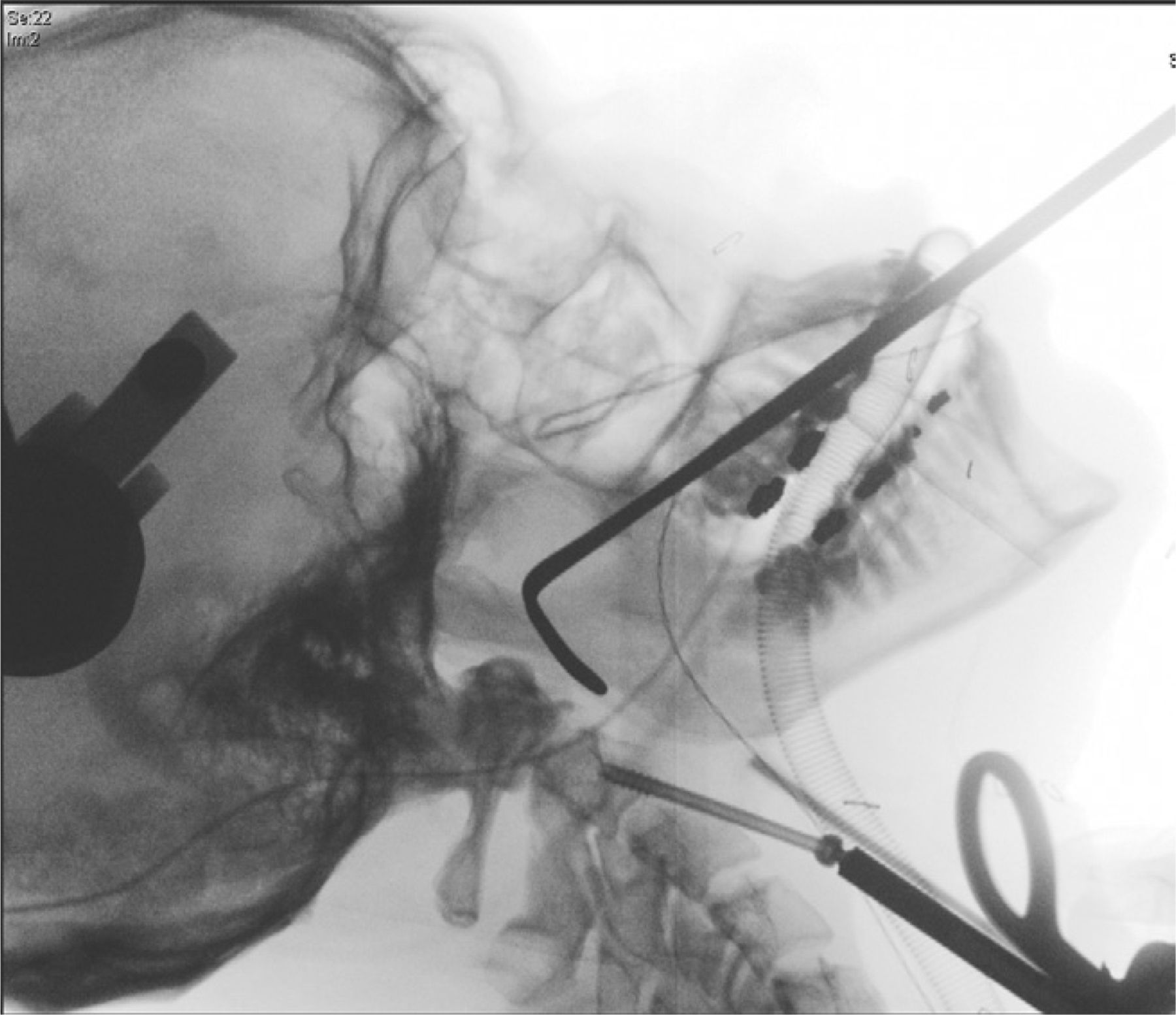
An intraoperative fluoroscopic image showed the transoral position of the army-navy hand retractor reducing the anteriorly displaced odontoid fracture during screw placement.
Results
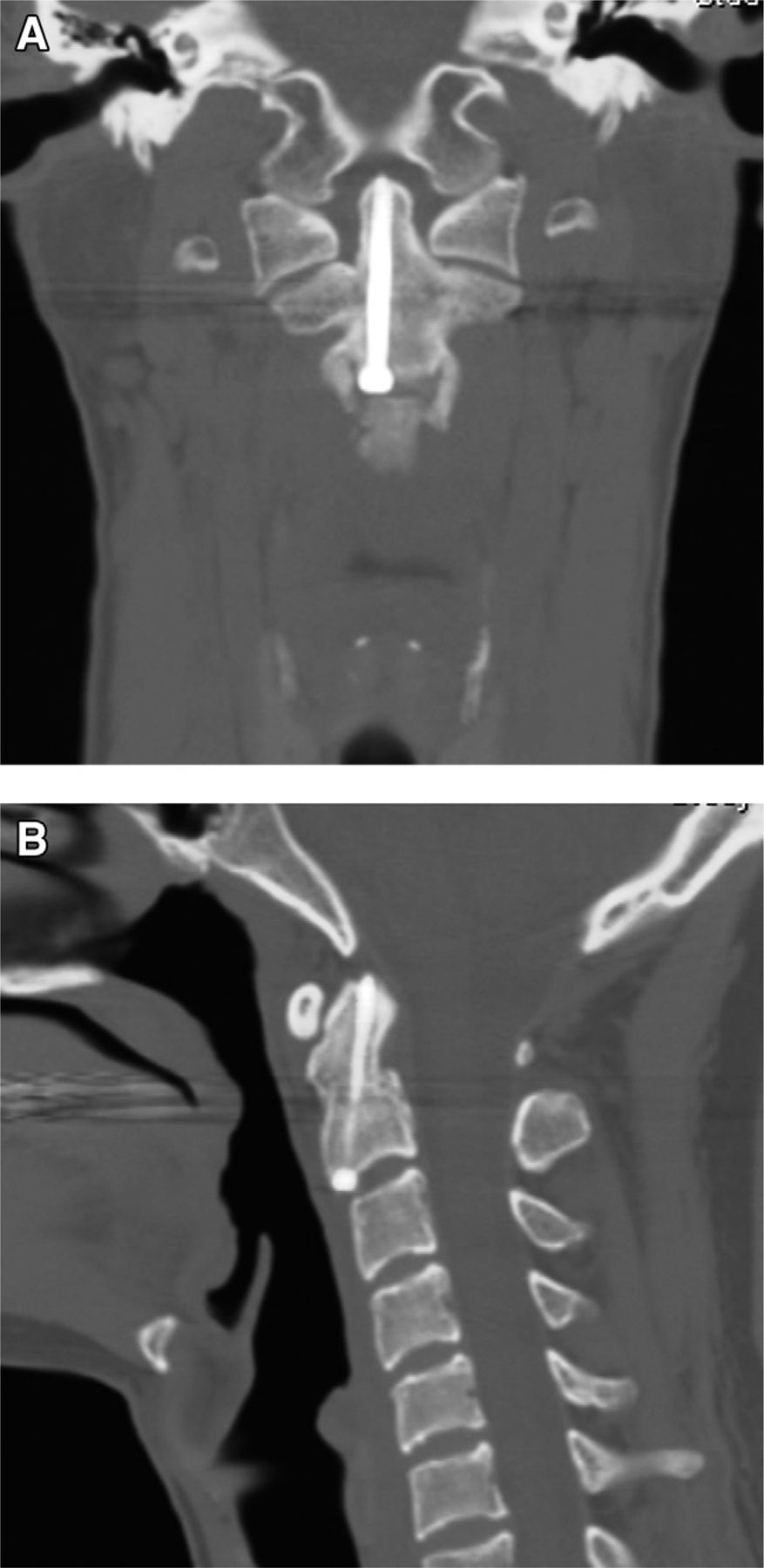
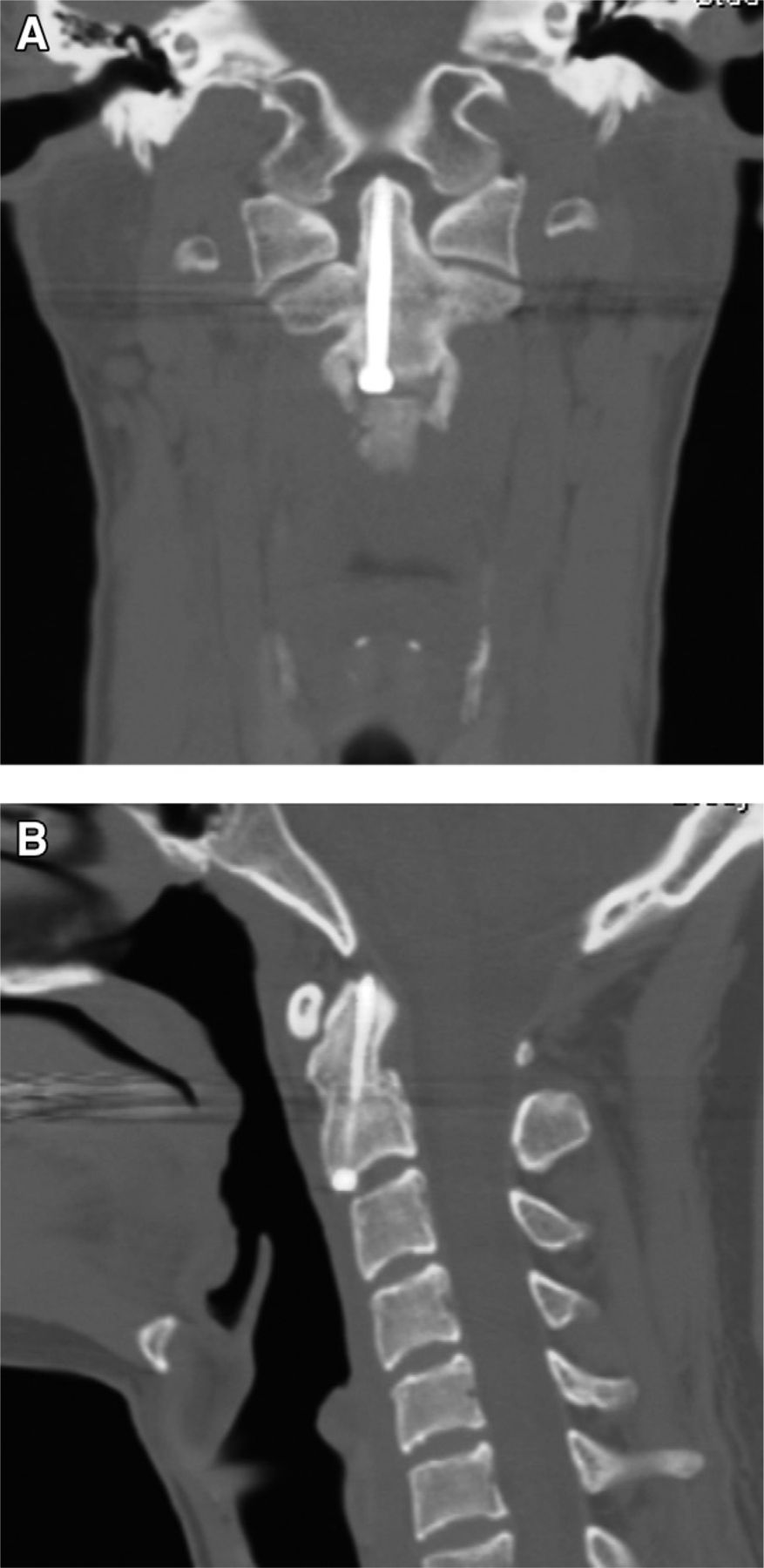
The patient's postoperative course was uneventful with no neurologic deficits or dysphagia from the oropharyngeal manipulation. The CT cervical spine scan showed proper placement of the odontoid screw into the body of C2 with adequate reduction (2.3 mm) of the odontoid process (Fig. 3).

Early postoperative CT cervical spine scans. (A) The coronal CT scan showed proper placement of the odontoid screw. (B) The sagittal CT scan showed adequate reduction of the displaced odontoid process (2.3 mm).
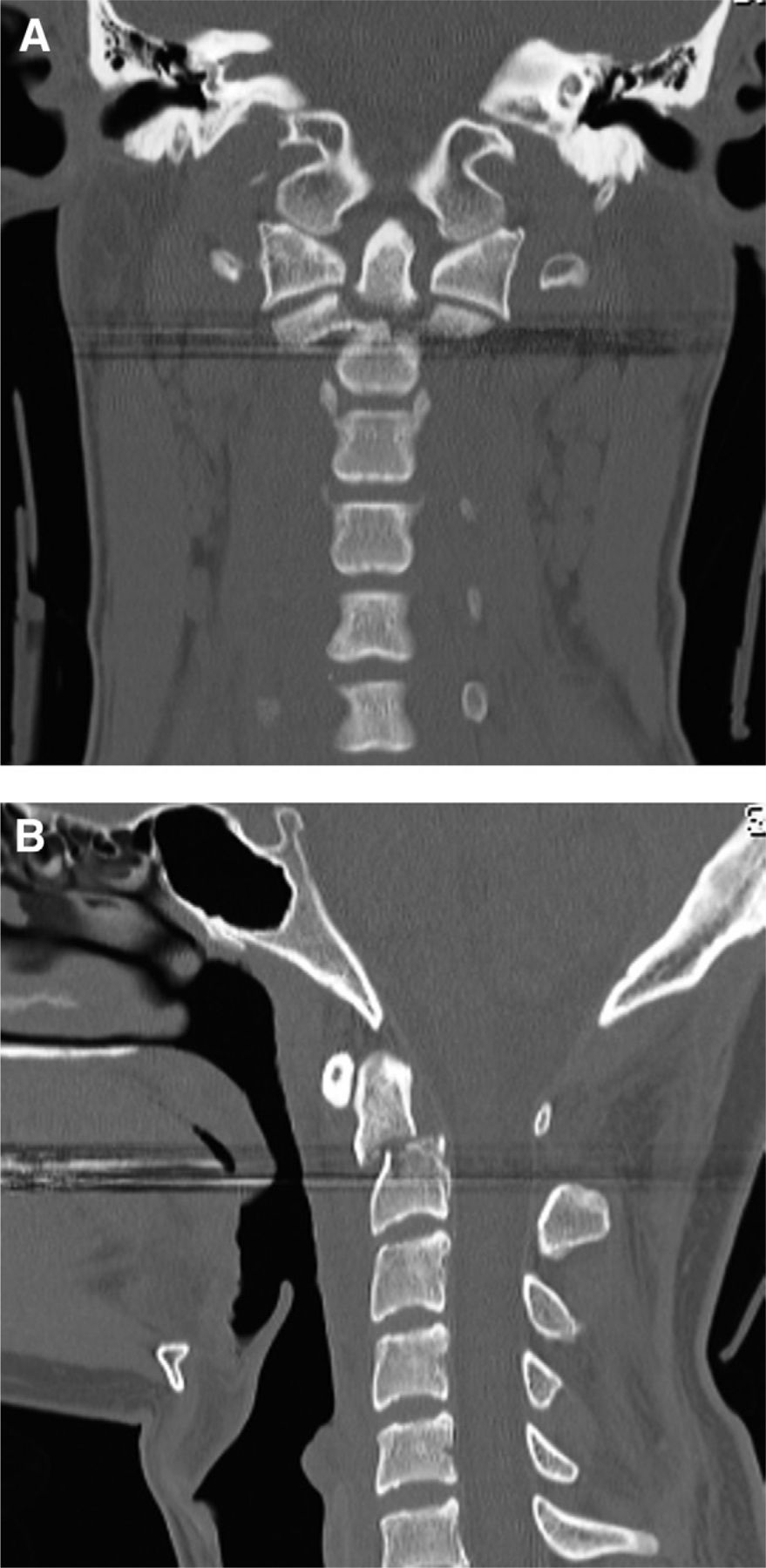
At the 3-month follow-up, the patient is neurologically intact and has full range of cervical spine movement without pain, and the CT cervical spine scan showed a well-healed odontoid fracture (Fig. 4).
CT cervical spine scans at 3 months postoperatively. (A) The coronal CT scan showed the well-healed odontoid fracture. (B) The sagittal CT scan showed proper screw placement and bony fusion.
Discussion
Anatomic reduction of the fractured odontoid process is imperative before one attempts the anterior odontoid screw fixation technique because the inability to achieve proper reduction of the anteriorly displaced odontoid process makes the surgery more challenging given the difficult trajectory for screw insertion.
With regard to the management of the irreducible anteriorly displaced odontoid fracture, the posterior stabilization of the C1-2 complex with transarticular screws with sublaminar wiring appears to be the recommended surgical treatment option.7 In the presented case, the age of the patient made us choose the anterior odontoid screw fixation procedure with transoral manipulation.
Extreme cervical manipulation to reduce the anteriorly displaced odontoid fracture would not be recommended, because it is not reduced completely by positioning. Additional manipulation through direct oropharyngeal anterior pressure on the anteriorly displaced odontoid process can be effective in completing the reduction.
The placement of 2 odontoid screws is more challenging with no biomechanical advantage as compared with 1-screw odontoid fixation. Sasso et al9 found no significant difference when they compared the use of 1 screw versus 2 screws for stabilization of the odontoid process under loading to failure. Graziano et al10 also found no difference between 1 screw and 2 screws in bending and torsional stiffness of the instrumented odontoid process.
There are different transoral manipulation techniques for reduction of displaced type II odontoid fractures described in the literature (Table 1). Elias et al11 reported that transoral digital manipulation could reduce the anteriorly displaced type II odontoid fracture to aid in screw fixation. Piedra et al12 used the same technique of closed transoral digital reduction of locked-type II odontoid fracture with posterior cervical manipulation. However, the transoral digital technique carries the hazards of radiation exposure and inaccurate fluoroscopic visualization.
Transoral manipulation techniques for reduction of displaced type II odontoid fractures in literature
Ben-Galim and Reitman13 reported that using a padded laryngoscope blade for transoral manipulation of anteriorly displaced type II odontoid fracture may provide better fluoroscopic visualization and radiation exposure avoidance. However, oropharyngeal wall trauma and improper handling during the manipulation may occur.
In the presented technique, the use of an army-navy hand retractor has clear advantages including minimal radiation exposure, good fluoroscopic visualization, less trauma to the oropharyngeal wall, and proper handling with better force control in reducing the anteriorly displaced type II odontoid fracture. Additional pressure on the cervical spinous process in the back of the neck has resulted in better reduction.
Conclusions
We found that direct transoral manipulation with an army-navy hand retractor can be used to assist in reducing the anteriorly displaced type II odontoid fracture during anterior odontoid screw fixation.
- © 2012 ISASS - International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}