


Abstract
Background Cervical laminoplasty (CLP) and posterior cervical laminectomy and fusion (CLF) are well-established surgical procedures used in the treatment of cervical spondylotic myelopathy (CSM). In situations of clinical equipoise, an influential factor in procedural decision making could be the economic effect of the chosen procedure. The object of this study is to compare and analyze the total hospital costs and charges pertaining to patients undergoing CLP or CLF for the treatment of CSM.
Methods We performed a retrospective review of 81 consecutive patients from a single institution; 55 patients were treated with CLP and 26 with CLF. CLP was performed via the double-door allograft technique that does not require implants, whereas laminectomy fusion procedures included metallic instrumentation. We analyzed 10,682 individual costs (HC) and charges (HCh) for all patients, as obtained from hospital accounting data. The Current Procedural Terminology codes were used to estimate the physicians’ fees as such fees are not accounted for via hospital billing records. Total cost (TC) therefore equaled the sum of the hospital cost and the estimated physicians’ fees.
Results The mean length of stay was 3.7 days for CLP and 5.9 days for CLF (P < .01). There were no significant differences between the groups with respect to age, gender, previous surgical history, and medical insurance. The TC mean was $17,734 for CLP and $37,413 for CLF (P < .01). Mean HCh for CLP was 42% of that for CLF, and therefore the mean charge for CLF was 238% of that for CLP (P < .01). Mean HC was $15,426 for CLP and $32,125 for CLF (P < .01); the main contributor was implant cost (mean $2582).
Conclusions Our study demonstrates that, in clinically similar populations, CLP results in reduced length of stay, TC, and hospital charges. In CSM cases requiring posterior decompression, we demonstrate CLP to be a less costly procedure. However, in the presence of neck pain, kyphotic deformity, or gross instability, this procedure may not be sufficient and posterior CLF may be required.
Introduction
Cervical spondylosis is a common disorder that results from degeneration of intervertebral discs and hypertrophic ossification of discoligamentous structures within the cervical spine. Resultant cervical spinal stenosis may cause cervical spondylotic radiculopathy (CSR) and cervical spondylotic myelopathy (CSM). Additional pathologies, such as a herniated nucleus pulposus and ossification of the posterior longitudinal ligament (OPLL), may contribute to the development of axial neck pain, CSR, and CSM. Recently, guidelines have been published regarding the natural history, predictive prognostic features, surgical indications for cervical radiculomyelopathy, and means for assessing functional outcomes.1–5 Significant controversy remains concerning the most appropriate means of operative management.
Posterior cervical procedures, such as cervical laminectomy (CL), cervical laminectomy and fusion (CLF), and cervical laminoplasty (CLP), have been advocated for patients with multisegmental disease (>2 segments).4, 6, 7 CLP has the additional caveat of requiring preserved lordotic cervical alignment.8–10 There have been no large, multicentered, prospective, randomized, controlled trials comparing CLF with CLP and the existing literature is limited to retrospective case series and cohort analyses.11–13 There have been several studies that demonstrate the relative merits of these 2 procedures and their superiority over simple CL.6, 7, 14–18 There are well-described situations in which one procedure may be preferred over the other based on clinicoradiographic features; however, in situations of clinical equipoise, the question of relative cost may be significant. There is essentially no existing literature on the relative cost of CLF in comparison with CLP.
There is a growing concern over the escalating cost of health care, and the relative cost of procedures may ultimately become a component of a surgical decision-making algorithm. This is certainly the case in clinical scenarios where both laminoplasty and laminectomy and fusion are deemed to be appropriate treatments. In such scenarios, the advantages and disadvantages of each procedure must be compared to determine the best course of action, and cost may become a relevant issue to both patients and providers. Direct care cost has been defined in the literature as the cost directly associated with intervention (ie, cost of perioperative inpatient management).19 This excludes both the utilization of outpatient healthcare resources and consideration of lost or gained economic productivity (or return to work potential). Our hypothesis is that CLP has an obvious cost advantage over CLF due to the lack of surgical implants, even if open-door spacer implants are utilized. However, a detailed account of the contributing factors has never been demonstrated. The aim of this study is to analyze the relative direct and indirect (housekeeping etc. are “indirect costs,” which are different from outpatient and long-term resource consumption) care costs associated with 2 surgical techniques for subjects with symptomatic cervical disease, CLP and CLF.
Methods
Patient population
The institutional review board approved this study before collection of any data. A retrospective chart review was performed at a single institution between 2006 and 2009 for subjects treated for CSM, OPLL, and multilevel CSR. Subjects were treated according to the surgeon's preference, via either variable length CLF (C2-T1 inclusive) or CLP (C2-T1 inclusive). CLF was performed using typical lateral mass screw and rod constructs with C7 and T1 pedicle screw fixation in individual cases; CLP was performed using the “double-door” or “French-door” technique, utilizing cadaveric allograft bone struts with suture fixation.8, 10, 17 There was no direct involvement with industry in this study, and therefore no consideration was given to companies providing supportive grants. The double-door technique utilizes cadaveric allograft and suture only, whereas the laminectomy and fusion procedures were completed with metallic implants from a single vendor with no known discount other than the negotiated rate for the institution. No laminoplasty spacers were employed preferentially.
Subject demographic and surgical data were obtained for each individual subject. This included subject's age, gender, length of stay (LOS), surgical technique, revision cases, number of levels decompressed/fused, and method of payment as non-Medicare versus Medicare. A matched subanalysis, focused on patients undergoing C3-7 level decompression, including demographics and the overall cost analysis, was also performed.
Financial data
Individual subject costs, charges, and payment values were obtained from the hospital financial records with regard to all itemized costs for direct care. These costs included, but were not limited to, operating room materials and supplies (ORMS), transfusions, time in the operating room, laboratory results, physical therapy, and inpatient housekeeping. To these costs were added the costs of the physicians’ labor (physician cost); physician costs were based on Medicare reimbursement schedules and were comprised of the procedure-specific Medicare reimbursement rates for surgeon, neuromonitoring, and anesthesiologist fees. The Current Procedural Terminology (CPT) codes used for calculating physician fees were taken from the Current Procedural Terminology 2009 Professional Edition, and the Manhattan health referral region adjustment factor was applied to all the fees.20 This information is kept confidential by institutional policy, as billing rates are shared between insurance and medical device companies, and publication of such information could represent a breach of such a contract with providers.
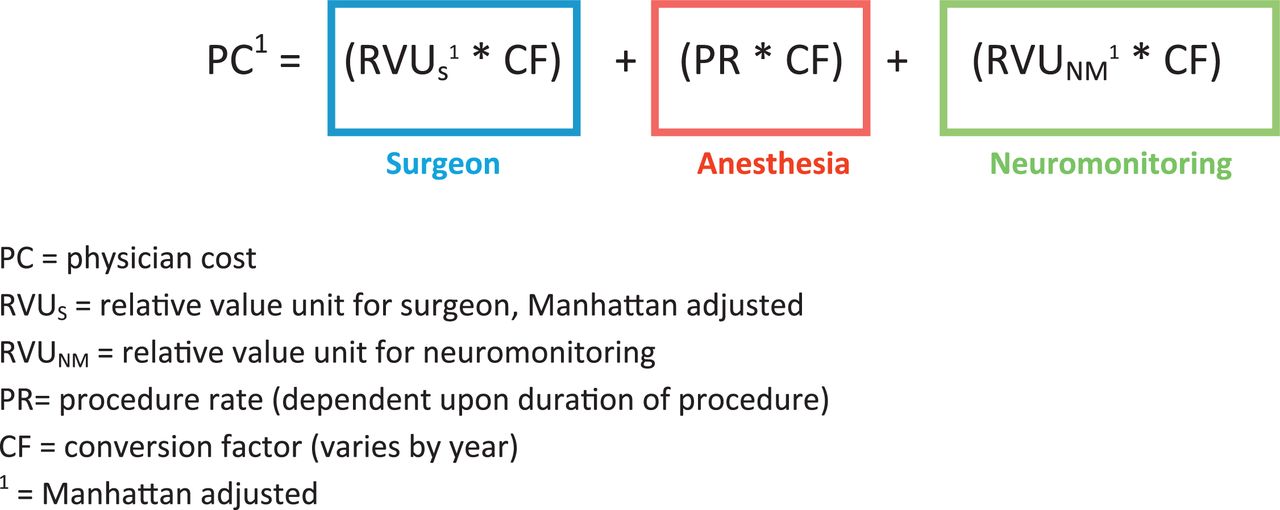
Physician cost was calculated using the formula described and illustrated later in the article, which accounts for relative value units (RVUs) for both the surgeon and neuromonitoring, as well as the anesthesia rate per procedure (PR). The RVUs are location-specific factors and represent the labor and supply elements required to provide a service. The physician-specific RVU we used were based on CPT codes and comprised of work, practice expense, and malpractice expense values. Each of these individual values is dependent upon geographic location; for our study, these values were adjusted for Manhattan rates. Physician-specific RVUs were multiplied by standard conversion factors (CFs) to calculate the corresponding dollar amount, which represented the Medicare payment to the physician. These CFs vary depending upon the service provided; for our study, we were interested in surgeon-, anesthesia-, and neuromonitoring-specific CF. The anesthesia PR was determined by the formula PR = (X/15) + 13, where X is a constant dependent upon procedure. For CLP, this constant is 120; for CLF, it is 180.
Therefore, we calculated the Manhattan-adjusted physician cost for each procedure as the sum of the geographically adjusted costs for the surgeon, anesthesia, and neuromonitoring. Surgeon cost was represented by RVU for surgeon multiplied by the surgeon-specific CF; anesthesia cost was represented by the anesthesia procedure rate multiplied by the anesthesia-specific CF; and neuromonitoring cost was equal to RVU for neuromonitoring multiplied by the neuromonitoring-specific CF (Fig. 1). The CPT codes for CLP included 63051 for surgeon cost, as well as 95920, 95925, and 95926 for neuromonitoring. The CPT codes for CLF included 63015, 22842, 22600, and 22614 for surgeon cost, as well as 95920, 95925, and 95926 for neuromonitoring. This adjustment in cost for the Manhattan region is limited to physician reimbursement and plays no more than a small role in absolute dollar quantities. However, it should be noted that the Manhattan health referral region commands an increased adjustment for both procedures, as Manhattan is considered to be an expensive practice region.

Breakdown of physician cost calculation (Medicare reimbursement formula).
Total cost, charge, and payment analyses between both groups were performed. Cost has been defined as the value (US dollars [USD]) of resources and supplies consumed in the provision of a service or product. Charge is defined as the assigned price from the provider institution based on the value of the given service or product, with consideration for additional resource expenditure; payment has been defined as the reimbursement received by an institution for the provision of a given service or product.
As charge and payment financial data pertaining to implants and hospital billing records are confidential under institutional policy, values for each procedure are reported as relative units (eg, charge CLP/charge CLF). By way of example, the relative charge unit for CLP patients was determined by dividing the mean total charge for CLP by the mean total charge of CLF. Subsequently, a mean relative charge was reported, with the corresponding P-value representing the statistical comparison of the original USD values. This was also performed to establish relative payments. Detailed and itemized cost comparisons for operating room–related costs (ORRC) and perioperative-related costs (PORC) were then performed based on hospital billing records. Each type of cost, ORRC, or PORC is broken down into several categories of goods and services, and all figures are reported in USD. Under the ORRC analysis, ORMS refer to the cost of grafts, implants, operating room instruments, and operating room materials. This analysis excludes any confidential information regarding suppliers of equipment, resources, or services. Comparison analysis within each group between non-Medicare- and Medicare-insured patients consisted of total cost (USD), charge (relative units), and payment (relative units). Likewise, comparison analysis of procedures within patient insurance type also consisted of total cost (USD), charge (relative), and payment (relative).
Statistical methods
Descriptive statistics, including means and standard deviations, were calculated for demographic, operative, and financial data (SPSS v.17, Chicago, Illinois). Nominal variables were analyzed using contingency tables and the Fisher's exact test was reported. A Student's t test was used for quantitative variables and the level of significance was set at P < .05.
Results
Demographics
In our study there were 2 populations, CLP (n = 55) and CLF (n = 26) (Table 1). The 2 groups were comparable in age, gender, rate of prior cervical operations, and method of payment (private insurance vs Medicare). The CLP subjects had a significantly shorter LOS following surgery at 3.7 ± 2.2 days when compared with 5.9 ± 3.2 in the CLF subjects (P < .01). This finding came despite the fact that the CLP subjects had significantly more levels decompressed with 6.0 ± 1.0 compared with 4.7 ± 0.6 in the CLF subjects (P < .01).
Demographics of cohorts
Cost, charge, and payment data
After the financial records were obtained and processed, we identified statistically significant reductions in cost when CLP was performed for cervical spondylosis in comparison with CLF (Table 2). Hospital cost for CLP averaged $15,426 ± $4939, whereas CLF averaged $32,125 ± $10,112 (P < .01). Hospital charges for CLP averaged 0.42 ± 0.13 times the cost of CLF, which means that CLF was 2.38 ± 1.07 times the cost of CLP (P < .01). Hospital payment received for CLP was 0.48 ± 0.18 the payment received for CLF; CLF was 2.07 ± 1.34 times the cost of CLP (P < .01). A more intuitive way of reporting these values may be to state, eg, that the payment received by the hospital for CLP was 48% ± 15% the payment of CLF, whereas payment received by the hospital for CLF, therefore, represented 208% ± 66% of the payment for CLP. Physician cost was $2977 versus $6132 ± $253 (P < .01) in CLP and CLF, respectively (these values are based on CPT 2009 adjusted for Manhattan). Most notably, the mean total cost for CLP was $17,734 ± $4939; the total cost of CLF was $37,413 ± $10,167 (P < .01).
Total cost by cohort
This was true despite significantly greater spinal segments being decompressed in the CLP subjects versus the CLF subjects. If we perform a subanalysis comparing just subjects with C3-7 decompressions, we find that LOS, hospital cost, charge, and payment received remain statistically significant (Table 3). Physician cost (including surgeon, anesthesia, and neuromonitoring) and total cost reduction utilizing CLP also remain statistically significant (P < .01).
C3-7 subanalysis
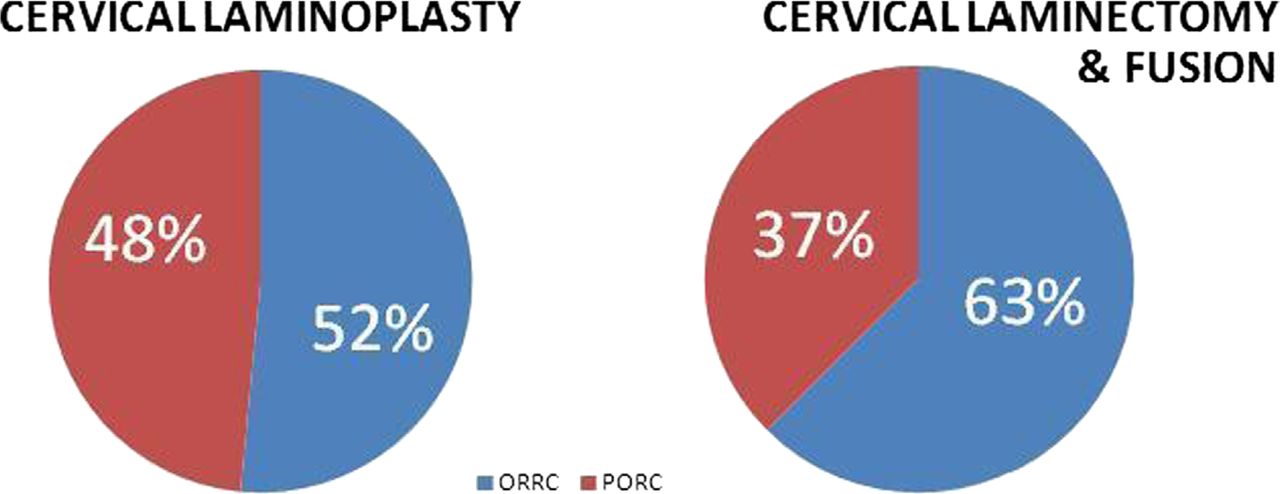
When cost is broken down into ORRC and PORC, we identify significant contributors to the relative cost of CLP versus CLF. First looking at ORRC (Table 4), we identify 4 statistically significant factors. ORMS, which included the cost of the graft, implants, operating room instruments, and operating room materials, were significantly more costly for CLF than for CLP; the average cost of ORMS was $15,212 ± $10,988 for CLF and $3085 ± $1677 for CLP (P < .00). CLF is also significantly more costly in imaging ($699 ± $466 vs $290 ± $336; P < .01), neuromonitoring ($1030 ± $524 vs $1419 ± $853; P = .04), and operating room ($1836 ± $870 vs $2820 ± $1554; P < .01). When reviewing PORC (Table 5), we identify 5 statistically significant factors in favor of CLP. These include housekeeping ($1686 ± $1299 vs $2692 ± $1643; P < .01), materials (297 ± 765 vs 860 ± 887; P < .01), medications (189 ± 157 vs $504 ± $546; P < .01), physical therapy ($287 ± $221 vs $630 ± $561; P < .01), and room expenses ($4738 ± $2434 vs $7148 ± $3730; P < .01). The most notable discrepancies are the ORMS cost under ORRC and room expenses under PORC. Overall, the distribution of costs for CLP is 52% ORRC and 48% PORC, and in the CLF population, this distribution is 63% ORRC and 37% PORC (Fig. 2). It should be reiterated that the overall cost for CLP was lower in comparison with the overall cost for CLF, and that these percentages are calculated from significantly different total costs.
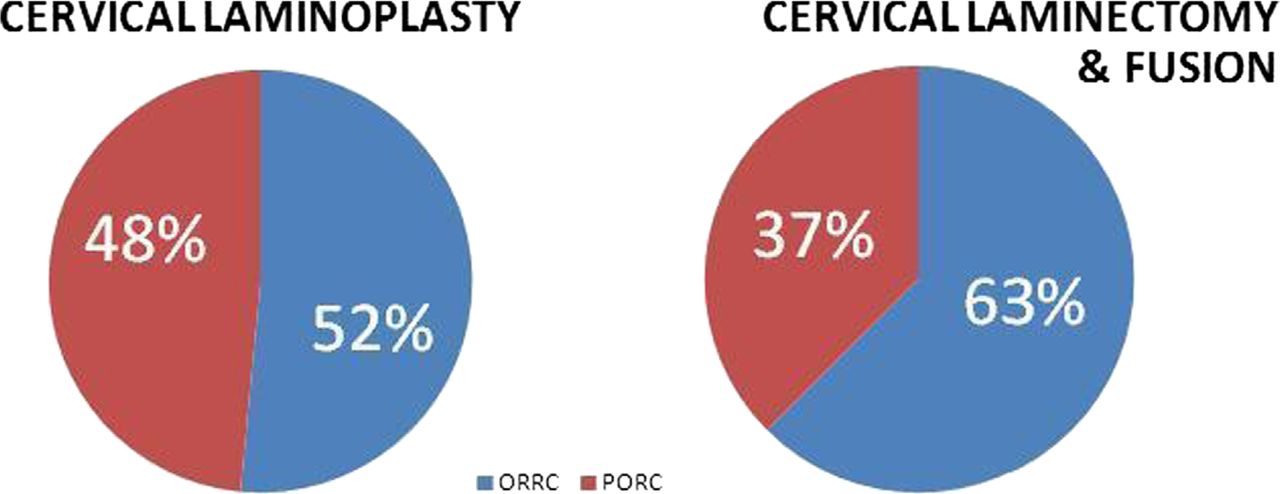
Distribution of costs per procedure.
Operating room–related costs
Perioperative-related costs
Non-Medicare insurance versus Medicare
The results described earlier were also apparent when patients were categorized by insurance type (Medicare vs non-Medicare) before comparison (Table 6). Amongst non-Medicare patients, the mean hospital cost of CLF ($33,336 ± $9720) was significantly greater than that of CLP ($14,762 ± $5093) (P < .01). Likewise, hospital charges for CLF were 1.48 ± 0.95 times the charges for CLP (P < .01), and hospital payments received were 1.54 ± 1.13 times the payments received for CLP (P < .01). These findings were comparable to procedural comparisons of patients covered by Medicare only; CLF was more costly for the hospital (mean cost $30,474 ± $10,870) than CLP ($16,284 ± $4700) (P < .01), it generated 1.39 ± 0.88 times the hospital charges of CLP (P < .01) and resulted in 1.08 ± 0.59 times the payments received for CLP (P < .01).
Total cost by procedure, within insurance type
When CLP and CLF subjects were broken down separately by payer (non-Medicare insurance and Medicare), we did not find many significant differences within the 2 populations (Table 7). Within CLP, there were 31 non-Medicare insurance subjects and 24 Medicare subjects. When comparing cost ($14,762 ± $5093 for non-Medicare insurance versus $16,284 ± $4700 for Medicare), there was no difference between insurance types (P = .3). The charge for non-Medicare CLP patients was 94% ± 81% of the charge for Medicare patients, therefore, the charge for Medicare patients was 107% ± 123% the charge for non-Medicare patients, and the difference between the procedures was not significant (P = .5). The hospital payment received was also insignificantly different between the groups, as non-Medicare patients averaged payments of 118% ± 93% that of Medicare patient payments, and Medicare payments averaged 85% ± 107% the non-Medicare payments (P = .1). Therefore, we did not find any statistically significant difference in cost, charge, or payment received for subjects covered by private insurance versus those covered by Medicare.
Total cost by insurance type, within procedure
Likewise, in the CLF population, of 15 non-Medicare-insured and 11 Medicare subjects, the cost ($33,336 ± $9720 for non-Medicare insurance versus $30,474 ± $10,870 for Medicare, P = .5) was not significantly different. The charge between insurance types was also not significantly different, as non-Medicare patients averaged charges of 118% ± 81% of the average for Medicare patients, whereas Medicare patients averaged charges 85% ± 123% of the average for non-Medicare patients (P = .4). Once again, comparisons were not statistically significant in comparing those subjects covered by non-Medicare insurance versus Medicare. Both procedures demonstrated marginal gains under private insurance (CLF > CLP), although both procedures report marginal losses under Medicare (CLF > CLP).
Discussion
The best management of CSM or CSR in the context of cervical spinal stenosis, herniated nucleus pulposus, and OPLL remains an arena of intense clinical debate. Expert consensus essentially remains that individual patient factors are of the utmost importance in devising the most appropriate management strategy. There are several procedures available in the arsenal of posterior approaches to the cervical spine, including CLF and CLP. In clinical situations where more than one type of procedure could be deemed appropriate, patients and caregivers are forced to weigh multiple factors to determine the best treatment option. Factors that guide decision-making between these procedures include the patient's cervical alignment, axial neck pain, multisegmental (>2 levels) spondylosis, the presence of OPLL, the extent of cervical cord compression, other patient factors (eg, comorbidities and age), and the surgeon's own preferences.6, 15, 21, 22
CLP has been deemed the more appropriate procedure in cases of preserved lordosis, no segmental instability, and minimal neck pain. It has been associated with neurologic recovery rates from 41%–81%, based on Nurick grading and Japanese Orthopedic Association outcomes,23–25 though several authors have noted differing recovery based on age, with older patients showing lesser degrees of recovery.24, 26 Despite being considered a motion-preserving procedure, CLP has been demonstrated to reduce ROM in the range of 8°–34°.17, 27, 28
In contrast, CLF has been the procedure of choice when patients present with kyphotic deformity, gross instability, and neck pain. CLF can be recommended for the treatment of CSM and OPLL and should be considered equivalent to CL and CLP with regard to functional improvement.29 The neurologic stabilization and recovery rates range from 51%–97%, based on Nurick and Japanese Orthopedic Association outcomes,7, 30 though early studies demonstrating effective neurologic outcome with CLF had high complication rates that included kyphosis and pseudarthrosis when using onlay bone graft techniques.30, 31 However, a more recent series, with better rates of neurologic recovery when utilizing lateral mass fixation techniques, demonstrated lower rates of complication.7, 32
Therefore, institutional practice is such that cervical laminoplasty is reserved for patients with CSM who have limited axial neck pain and maintenance of neutral or lordotic cervical alignment. Laminectomy and fusion is employed when there is significant axial neck pain, kyphotic deformity, dynamic hypermobility, or instability. However, it is not uncommon for a patient to lack definitive symptoms that would clearly indicate which procedure, CLP or CLF, is preferable; in such situations of clinical equipoise, the importance of defining clinical superiority between these 2 procedures is overshadowed by the individual patient factors and surgeon's preferences that influence the decision-making algorithm of the surgeon. The existing comparative literature between CL, CLP, and CLF, however is surprisingly scarce. Several authors have demonstrated equivalent rates of postoperative neurologic recovery and improvement in CLF and CLP,12, 33–35 though CLP is suspected to result in reduced ROM,36 and there have been conflicting reports of which procedure is more advantageous with respect to the rate of postoperative kyphosis.33, 35–37 A 2001 independent matched-cohort analysis of CLF versus CLP concluded that CLP may be the preferable procedure owing to reduced complication rates and improved functional outcomes.11 However, a more recent study has suggested that both procedures offer effective and comparable functional outcomes, and that a RCT would be necessary to determine the superiority of either modality.29 An additional factor that deserves attention, and which previously has not been considered, is the relative economic cost of these techniques.
We have chosen to evaluate the 2 most common posterior cervical techniques from a simplified economic perspective. Assessment of their total costs and relative charges and hospital payments based on institutional data is illustrative of differences in the perioperative setting. Overall, our results demonstrate that CLP carries a lower cost, presents a reduced relative charge to payers and results in a lower relative payment to the institution. This is largely a result of direct ORMS costs from an ORRC perspective and increased LOS from PORC perspective. In the evaluation of this type of data, there are several interested parties including the patient, the providers (physician and hospital), the payers (subjects, Medicare, and private insurers), and policy makers (Government and society). Overall, CLP is the superior procedure from a direct and indirect short-term care cost perspective if reduced cost is the goal (Table 2).
The institution incurs significantly lower short-term care costs in providing CLP in comparison with CLF. The major ORRC factors involved are the surgical implants. It is relevant to note, however, that the cost of CLP can be increased incrementally by the utilization of an “open-door technique” employing customized implantable spacing devices and plates.8, 10 Likewise, the overall cost of CLF may be reduced through the judicious inclusion of levels in the fusion construct and the number of implantable screws and rods. These factors may be considered in the context of overall patient outcome, which obviously must not be sacrificed. Within PORC, the room expense is the largest factor, which is certainly a consequence of increased LOS. In reality, it is likely that all of the statistically increased PORCs demonstrated are a product of increased LOS. This makes reductions in LOS an important target from an economic perspective, in addition to the clinical benefits of reduced hospital admission periods.
Despite the similarity in complexity between CLP and CLF, the payment received by the hospital is also significantly less for CLP; this finding was true regardless of the patient's insurance type, which demonstrates that hospital payment rates in this population are not necessarily driven by characteristics of the payer. Providers may, therefore, find themselves in situations where economic factors could potentially influence decision making. In an era with continued interest in reducing healthcare cost, payers and policy makers are likely to choose a less costly procedure in situations of clinical equipoise; in the setting of CSM, that procedure appears to be CLP.
This is, perhaps, the most controversial aspect of this type of cost-analysis information. As providers, spine surgeons utilize existing literature, clinical training and experience, and access to advanced technology to deliver the best possible care for patients. The additional factor of cost should remain secondary, but must still be considered. An undesirable scenario is one in which payers and policy makers utilize cost as rationale to cover one procedure without truly understanding the clinical nuances of the decision, therefore, the importance of defining clinical outcomes to associate with cost data could not be more apparent. Prospective collection of general and disease-specific health-related quality-of-life outcome scores related to the management of CSM, as well as outpatient healthcare resource utilization and gained or lost patient economic productivity, will be crucial information to consider moving forward.
Conclusion
We demonstrate that, in clinically similar populations, cervical laminoplasty results in a shorter LOS and reduced costs, charges, and payment. In clinical scenarios requiring posterior decompression and procedural equipoise, we recommend spine surgeons to consider performing a cervical laminoplasty. In the presence of neck pain, kyphotic deformity, or gross instability, this procedure may not be sufficient and CLF may be required. Long-term follow-up with consistent reporting of general health and disease-specific outcome measures is essential to study the economics of CSM more effectively. Additionally, monitoring economic factors including non–short-term care healthcare resource utilization and loss or gain of productivity will remain a challenge that must be met with accurate data collection and consistent modeling of cost-utility research.
Footnotes
Support for this study was obtained through departmental funding within an academic institution. Drs. Bendo and Goldstein maintain relationships within the medical industry for the advancement of the field; their full financial disclosures are listed below.
Bendo, John A.: Consulting, Synthes Spine.
Goldstein, Jeffrey A.: Private Investments, K2M; Physician Fellowship Partners, Spinecore; Consulting, Synthes Spine, NuVasive, Medtronic, K2M; Speaking or Teaching Arrangements or both, Synthes Spine; Trips/Travel, Synthes Spine (Financial, Reimbursement for travel to teach); Scientific Advisory Board, Pearl Diver; Research Support—Staff or Materials or both, Axiomed (paid directly to institution/employer); Fellowship Support, Medtronic (paid directly to institution/employer), Synthes Spine (paid directly to institution/employer).
- © 2013 ISASS - The International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.