


Abstract
Background Idiopathic spinal cord herniation (ISCH) is a rare condition and its pathogenesis remains unclear. The purpose of this case report is to present an ISCH case with dorsal subarachnoid septum suggesting the pathogenesis of ISCH being adhesions from preexisting inflammation.
Methods Single case report.
Results A 60-year-old woman presented with Brown-Séquard syndrome below the level of T6. Magnetic resonance imaging revealed the thoracic spinal cord was displaced ventrally, and the dorsal subarachnoid space was enlarged and had a septum between the spinal cord and dura mater. Intraoperatively, the dorsal dura mater was seen to be adherent and the subarachnoid septum was identified after durotomy. The inner layer defect of the duplicated dura mater was found in the ventral dura mater, through which the spinal cord had herniated. After releasing the septum, the adhesions around the dura mater, and the hiatus, the spinal cord was reduced.
Conclusions The present case indicates that adhesions around the dura mater can be the pathogenesis of ISCH.
Introduction
Wortzman et al1 reported the first case of idiopathic spinal cord herniation (ISCH) in 1974. In the years since magnetic resonance imaging (MRI) came into widespread use, the concept of ISCH has been gradually appreciated, and the number of reported cases has increased since 1990. This herniation exclusively occurs in the thoracic spine, typically T4-T7,2 causing progressive myelopathy. Diagnosis is based on ventral displacement of the spinal cord observed on MRI and CT myelography.
Aizawa et al3 classified this condition into three types depending on the abnormality of the ventral portion of the dura mater, but the pathogenesis of ISCH has yet to be established. Both congenital and acquired mechanisms have been postulated for development of the lesion.2 An adhesions secondary to inflammation of the dura mater is one candidate. Here we report a case of ISCH with a dorsal subarachnoid septum suggesting preexisting inflammation as the pathogenesis.
Case report
History and examination
A 60-year-old active woman presented with a loss of temperature and pinprick sensation in her left leg, a loss of tactile sensation and muscle weakness of the right lower leg at the age of 45. She had no history of spinal surgery, spinal puncture, or trauma. Her symptoms slowly progressed, and on presentation the gait was spastic, especially on the right side. Neurological examination revealed Brown-Séquard syndrome below the level of T6. Position and vibration sensations were preserved bilaterally. Hyperreflexia and ankle clonus were observed of the right leg. Muscle strength was reduced to 4/5 (moves joint against gravity and resistance but no normal strength) on the right and normal on the left. Vesicorectal functions were preserved. Peripheral blood tests, biochemical tests, chest X-ray and urinalysis revealed no abnormalities.
Radiological findings
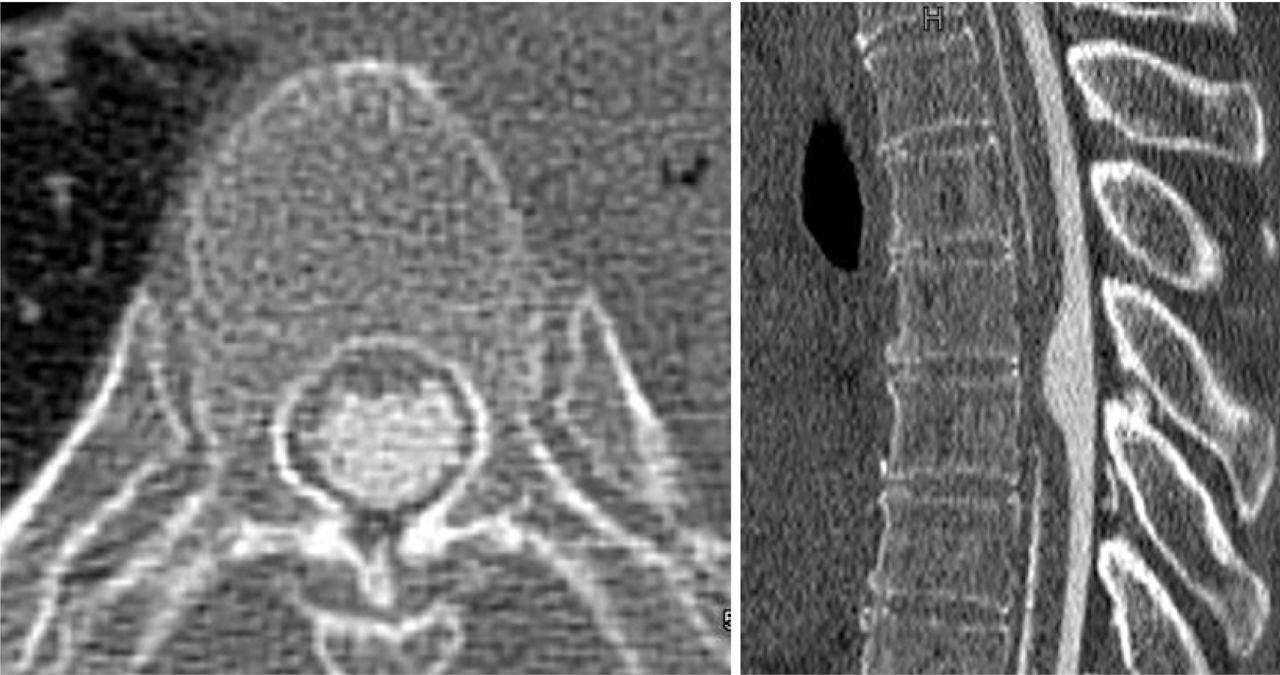
MRI showed the thoracic spinal cord displaced ventrally to the right, an enlarged dorsal subarachnoid space, and a midline septum between the dura mater and spinal cord at T5–T6 disc level (Figure 1). The midline septum separated dorsal subarachnoid space at the level, but not cranial nor caudal levels. Spinal cord was flattened, and high T2 signal intensity was not detected. Ventral spinal cord deviation was limited at T5–T6 disc level. Scalloping of the vertebral body4 and erosion of the dura mater by a herniated and calcified disc5 were not seen. CT myelography showed the compressed spinal cord ventrally as well as no pooling and extravasation of contrast medium ventral to the spinal cord. As for dorsal side of spinal cord, it also showed an uninterrupted flow of contrast material and no filling defect (Figure 2). A nuclear trail sign, a feature suggestive of a path of herniation of the nucleus pulposus, was not present. The septum seen on MRI could not be distinguished with contrast medium on CT myelography.
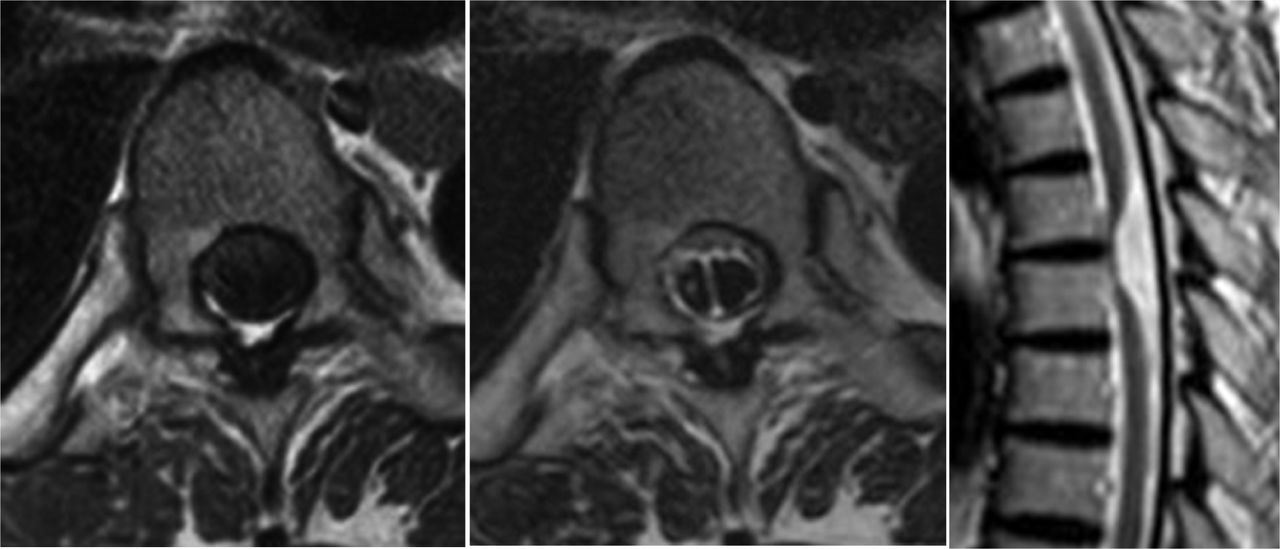
Axial T1, T2-weighted MRI (left, center) shows significant right ventral shift of the spinal cord and a dorsal midline subarachnoid septum at T5–T6 disc level. The midline septum is observed only at this level. Sagittal T2-weighted MRI (right) shows ventral displacement of the spinal cord at T5–T6 disc level. Focal ventral kinking and adhesion of the spinal cord is apparent with an enlarged dorsal subarachnoid space.

Axial CT myelography at the same level as the MRI axial image (Figure 1) shows no pooling of contrast medium ventrally to the spinal cord, an uninterrupted flow of contrast material and no filling defect.
Operative findings
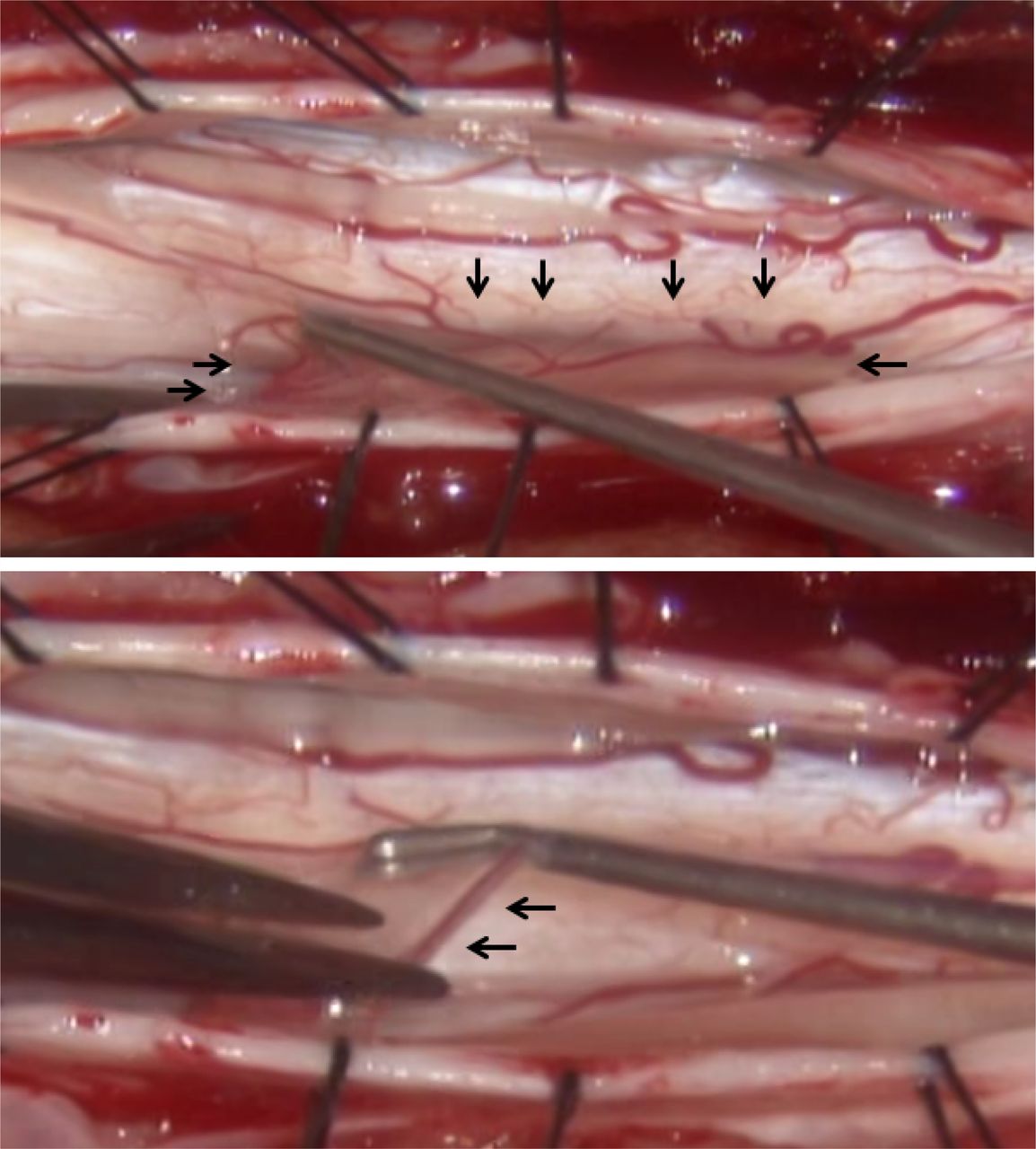
Laminectomy and right-sided partial pediculotomy of the T5 and T6 vertebrae was performed, and adhesion of the dura mater was found. Ultrasonography revealed the septum in the dorsal subarachnoid space, and a ventral spinal cord herniation and the dorsal subarachnoid septum were identified after durotomy. The septum was a muddy, thin, shiny whitish membrane containing small vessels, and was 15 mm in cephalocaudal length. It connected the dorsal dura mater to the dorsal surface of the spinal cord (Figure 3), it is not a normal arachnoid trabeculation which is usually seen in the thoracic spine. Cerebrospinal fluid (CSF) flowed freely around the septum.
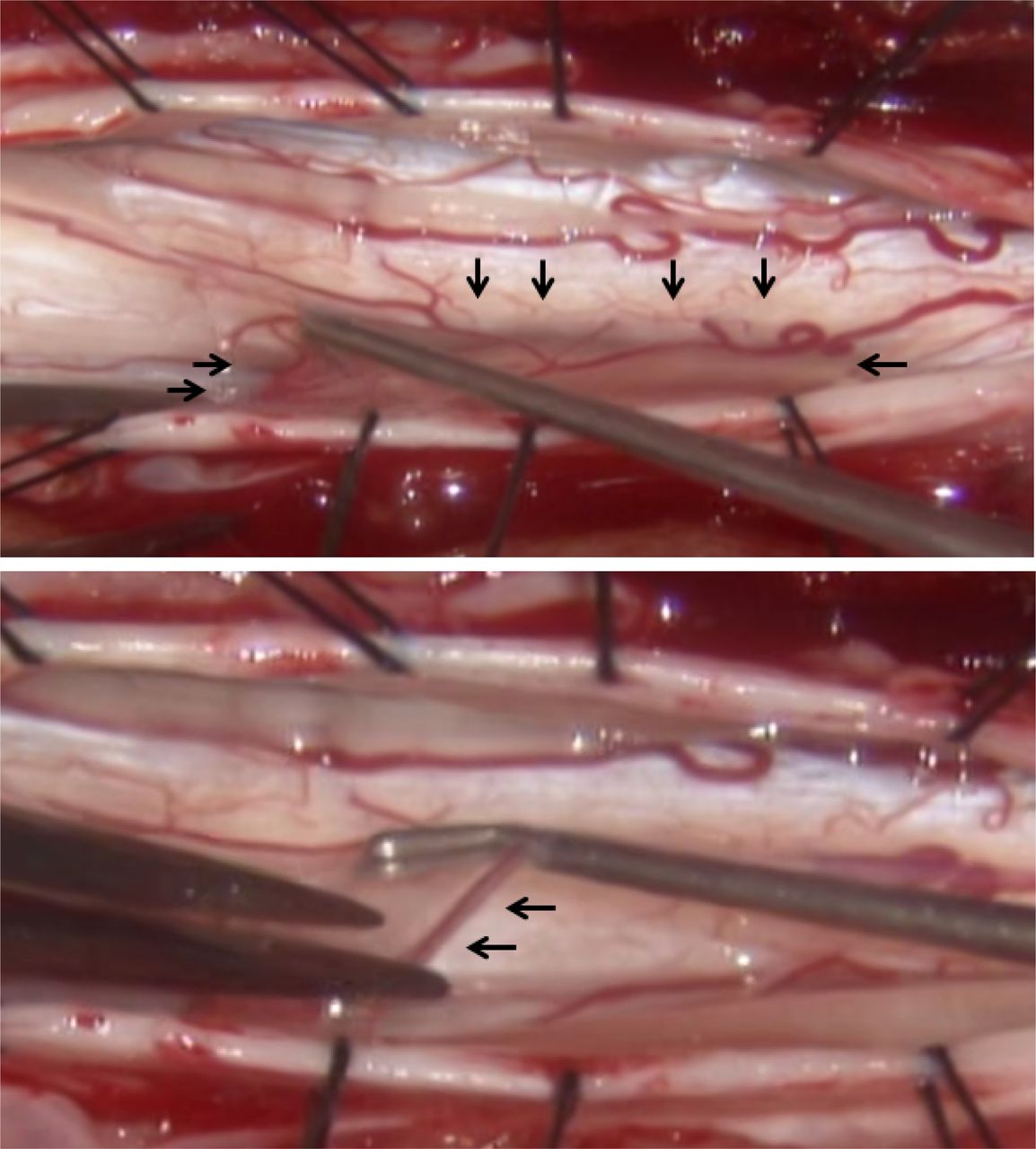
Intraoperative photographs. The upper photograph shows the dorsal subarachnoid septum (arrows). Right side is cranial. The lower photograph indicates the vessels in the septum (arrows).
After removal of the septum, the spinal cord was not reduced into the normal position. The dentate ligament was divided, the defect of the inner layer of the ventral dura mater was found, through which the spinal cord had herniated. Incarceration of the spinal cord in the hernia orifice was not observed. The herniated hiatus was enlarged by a 15 mm cephalocaudal incision and the spinal cord was carefully untethered without significant traction. Through the defect, another glossy white layer of dura mater, which was presumed to be the outer layer of the duplicated dura mater, was observed. With ultrasonography, we confirmed that CSF flowed freely in the ventral arachnoid space and the spinal cord had reduced.
Postoperative course
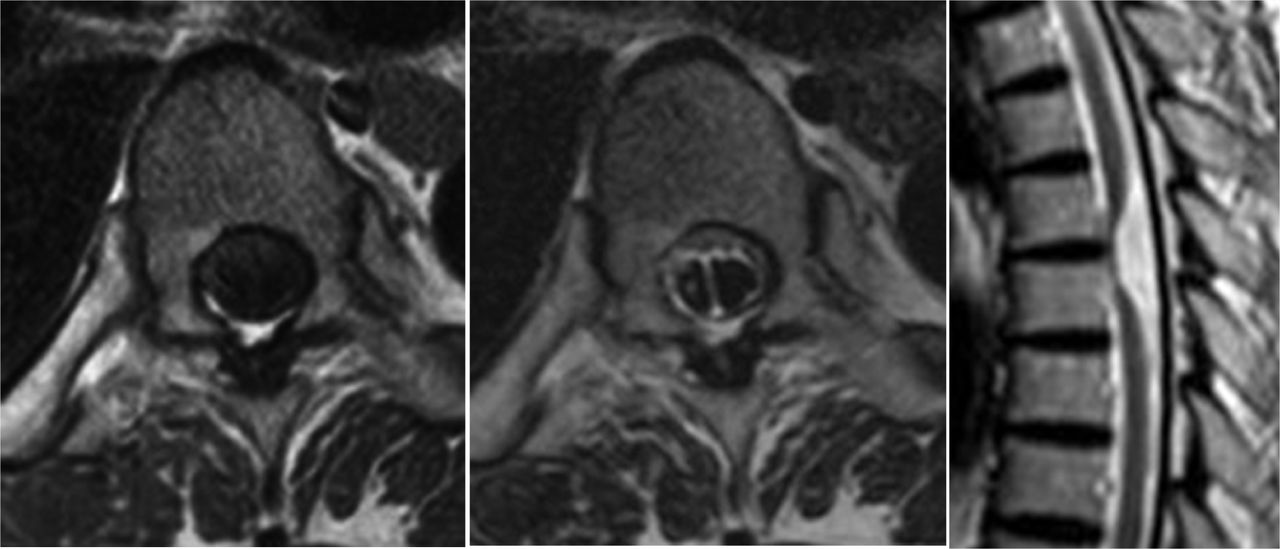
By 2 postoperative weeks, the patient had recovered muscle power and some sensation, with a slight lessening of spasticity. A half year later, the spinal cord remained reduced on postoperative MRI (Figure 4). Atrophy and high signal changes within the spinal cord were not observed. At 2 years follow up, the patient had no recurrence of symptoms, no instability and no back pain.

Axial T1, T2-weighted MRI (left, center), sagittal T2-weighted MRI (right). The focal mildly high T2 intensity in the cord (arrows) was believed to be due to regional edema, gliosis or postoperative effects.
Discussion
ISCH typically occurs in middle-aged adults with a female preponderance. A slowly progressive Brown-Séquard syndrome at upper thoracic spine is the most common clinical presentation. All considered, it seems more likely that ISCH is a pathological condition acquired in adulthood. An inflammation and degenerative process with slow erosion of the dura mater would seem consistent with the age of presentation and the location of lesion.
The proposed pathogenesis of ISCH is initiated by minor or unrecognized trauma and inflammation including mechanical stress, which means CSF pulsation, physiological anterior movement of spinal cord secondary to cardiac pulsations and respiratory movements, and the biomechanical impact of flexion and extension movements at thoracic spine, although active inflammation may not be present in the inner layer of dura mater.6 The thoracic spine, where spinal cord is anteriorly located and the change in spinal fluid flow occurs,7 has limited mobility, physiologic kyphosis at this level, which may lead to ventral adhesion of the pia mater once inflammation develops around the dura mater. Dorsally thickened arachnoid mater has also been reported by many authors and this adhesion seems to be secondary to inflammation of the dura mater.8 Prada et al. reported that histology of thick, fibrotic, inflammatory tissue surrounding the herniated cord demonstrated a chronic dural inflammatory process.9 Therefore, it may be that the inflammatory reactions causing adhesion of the arachnoid mater occur in the early pathogenesis of ISCH and then ventral adhesion of the spinal cord occurs.10 Together with cardiorespiratory-associated CSF pulsations, this event may cause continuous spinal cord friction and erosion of the dura mater, which could lead to the formation of the dural defect with progressive herniation of the spinal cord.11 Unfortunately for this case, we could not perform histologic examination of the septum and the inner layer of duplicated dura mater because it was too thin to capture without destructing the original form. Several authors reported that histologic examinations demonstrated that the inner layer of duplicated dura mater consisted of fibrous connective tissue without inflammatory cellular infiltration.3
One important lesion in the differential diagnosis of this condition is compressive dorsal arachnoid cyst12 which is the most common erroneous radiological diagnosis in patients with ISCH. Our case showed no filling defect by CT myelography, which was confirmed during surgery.
In our case, we speculate that circumferential adhesion had occurred early in disease pathogenesis, the dorsal adhesion was released by pulsations of CSF, the spinal cord was tethered ventrally, a part of the adhesion remained which became the dorsal subarachnoid septum, and the ventral adhesion caused ISCH. The definitive diagnoses can be made only with intraoperative findings.11 In case of a suspected dorsal subarachnoid septum, the surgeon should proceed to thoroughly inspect the ventral portion of spinal cord and dura mater.
Conclusion
Idiopathic spinal cord herniation is rare, but is an increasingly recognized cause of progressive and potentially curable thoracic myelopathy. The present case indicates that adhesions around the dura mater can be the pathogenesis of ISCH.
Disclosures
The authors declare no financial disclosures.
- Copyright © 2014 ISASS - International Society for the Advancement of Spine Surgery
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.