


Abstract
Background Approved treatment modalities for the surgical management of lumbar spinal stenosis encompass a variety of direct and indirect methods of decompression, though all have varying degrees of limitations and morbidity which potentially limit the efficacy and durability of the treatment. The coflex® interlaminar stabilization implant (Paradigm Spine, New York, NY), examined under a United States Food and Drug Administration (US FDA) Investigational Device Exemption (IDE) clinical trial, is shown to have durable outcomes when compared to posterolateral fusion in the setting of post-decompression stabilization for stenotic patients. Other clinical and radiographic parameters, more indicative of durability, were also evaluated. The data collected from these parameters were used to expand the FDA composite clinical success (CCS) endpoint; thus, creating a more stringent Therapeutic Sustainability Endpoint (TSE). The TSE allows more precise calculation of the durability of interlaminar stabilization (ILS) when compared to the fusion control group.
Methods A retrospective analysis of data generated from a prospective, randomized, level-1 trial that was conducted at 21 US sites was carried out. Three hundred forty-four per-protocol subjects were enrolled and randomized to ILS or fusion after decompression for lumbar stenosis with up to grade 1 degenerative spondylolisthesis. Clinical, safety, and radiographic data were collected and analyzed in both groups. Four-year outcomes were assessed, and the TSE was calculated for both cohorts. The clinical and radiographic factors thought to be associated with therapeutic sustainability were added to the CCS endpoints which were used for premarket approval (PMA).
Results Success rate, comprised of no second intervention and an ODI improvement of ≥ 15 points, was 57.6% of ILS and 46.7% of fusion patients (p = 0.095). Adding lack of fusion in the ILS cohort and successful fusion in the fusion cohort showed a CCS of 42.7% and 33.3%, respectively. Finally, adding adjacent level success to both cohorts and maintenance of foraminal height in the coflex cohort showed a CCS of 36.6% and 25.6%, respectively. With additional follow-up to five years in the U.S. PMA study, these trends are expected to continue to show the superior therapeutic sustainability of ILS compared to posterolateral fusion after decompression for spinal stenosis.
Conclusion There are clear differences in both therapeutic sustainability and intended clinical effect of ILS compared to posterolateral fusion with pedicle screw fixation after decompression for spinal stenosis. There are CCS differences between coflex and fusion cohorts noted at four years post-op similar to the trends revealed in the two year data used for PMA approval. When therapeutic sustainability outcomes are added to the CCS, ILS is proven to be a sustainable treatment for stabilization of the vertebral motion segment after decompression for lumbar spinal stenosis.
Introduction
Decompressive laminectomy for symptomatic pseudo-claudication of spinal stenosis has been the mainstay of surgical treatment for progressive degenerative neurocompressive disease.1 Internal fixation after decompression has been utilized primarily to stabilize an already unstable spinal segment or one which will be rendered unstable by the decompression itself. However, stenotic patients with high Visual Analog Scale (VAS) back pain scores pre-operatively are at risk for continued back-pain following decompression surgery alone.2 This is most likely secondary to a combination of facet disease and other mechanical degenerative changes. While the need for stabilization in the latter group of patients has not been definitively determined, it is well accepted that these patients may benefit from post-decompression instrumentation. Stabilization, as with posterolateral fusion with pedicle screw fixation, can help relieve mechanical back pain and reduce the potential for recurring stenosis at the treated level. However, fusion has been shown to have unfavorable long-term side effects, including pseudarthrosis,3 loss of fixation,4 and adjacent segment disease.5 Thus, therapeutic sustainability of fusion may wane over time.
Direct surgical decompression via laminoforaminotomy is a reliable and straightforward method of relieving the leg pain and claudication associated with lumbar stenosis. While decompression of stenosis is typically successful in relieving the symptoms of neural compression, it often does little to address the mechanical back pain and progressive degenerative disease which is commonly associated with the stenotic disease state. Facet degeneration, in particular, can lead to persistent or worsened back pain, and the foraminal height is at risk of decreasing over time.6 Similar to fusion, the therapeutic sustainability of decompression alone may wane over time, as well.
The FDA-approved coflex interlaminar stabilization (ILS) implant provides a less-invasive, motion preserving stabilization option for the stenotic patient after direct decompression to relieve back pain and preserve foraminal height.7 coflex is a U-shaped titanium device which is implanted deep within the inter-laminar space, providing neutral stabilization while maintaining normal spinal kinematics. The device allows for compression in extension while permitting normal flexion. This permits maintenance of sagittal balance and lordosis, as well as rotational and translational motion. Additionally, by mechanically offloading of the facets, it helps with relief of back pain and maintenance of foraminal eight over time. Through its mechanism of action, the clinical intent is to bolster the therapeutic sustainability of the procedure, and offer a clinically superior alternative in this select patient population.
Previously published literature shows that ILS has significantly shorter operative and hospitalization time than pedicle based fusion procedures, with less blood loss.7 The device is approved for use in patients with one- or two-level lumbar stenosis and up to a Grade 1 spondylolisthesis.8 It was examined under an investigational device exemption (IDE) beginning in 2006, and approved under premarket approval (PMA) in the USA in October, 2012.
The purpose of this paper is to describe the clinical, safety, and radiographic results of the ILS clinical study in comparison to a control group consisting of posterolateral fusion with autologous bone graft at four years post-op. Effectiveness comparisons between ILS and fusion cohorts were based on composite clinical success (CCS) endpoints from the FDA trial and a therapeutic sustainability endpoint (TSE) determined by combining CCS endpoints with factors hypothesized to be associated with longer-term durability and sustainability. CCS was achieved in either cohort if the following criteria were met: ODI improvement of at least 15 points achieved at 24 months post-op, no secondary surgeries, no post-operative lumbar epidural steroid injections, and no device related complications. To determine TSE, additional factors analyzed and combined with CCS included index-level motion preservation in the ILS group, decrease in index-level motion in the fusion group, unaltered kinematics at the adjacent level for either group, and maintenance of foraminal height in the ILS group.
Materials and Methods
Since prior reports described the IDE study design in detail,7, 8 only a brief summary follows: randomization was 2:1, resulting in 230 and 114 patients receiving ILS and fusion during the enrollment period from 2006 through 2010 at 21 participating US sites. Main inclusion criteria were: radiographic confirmation of moderate to severe stenosis, age range from 40-80; ODI score ≥ 40 (out of 100), VAS for back pain of ≥ 50mm (out of 100mm), failing ≥ 6 months of conservative care including ≥ 1 epidural steroid injection, no prior decompression surgery, up to a Grade 1 stable spondylolisthesis, and a willingness to consent to participation. Main exclusion criteria were: osteopenia or osteoporosis, prior fusion, laminectomy or interspinous process device (IPD) implantation, and more than two levels needing treatment. Patient reported outcomes (PROs) administered were the Oswestry Disability Index (ODI), back pain and leg pain VAS, and the Zurich Claudication Questionnaire (ZCQ). Safety was assessed via adverse event reporting and then adjudicated by a Clinical Events Committee through month 24.9 Extensive quantitative and qualitative radiographic evaluations were carried out by a core lab. After removal, revision, or replacement of the study device, or after the first lumbar steroid injection, clinical measurements (ODI, VAS, ZCQ) were not included in the analysis data sets to avoid confounding the interpretation and to allow unambiguous reading of mean improvements as expected changes among patients not requiring a secondary intervention.
In this paper, we compare device groups using conventional CCS endpoints and then assessed a Therapeutic Sustainability Endpoint (TSE) at four years from the initial surgery. TSE extends the CCS end-point to include factors suggestive of durability that are associated with longer term maintenance of outcomes and treatment success, including segmental motion preservation, preservation of foraminal height, and maintenance of adjacent level kinematics.
Independent radiographic analysis (Medical Metrics, Inc., Houston, TX, USA) determined a number of quantitative and qualitative changes from baseline through four years post-op in both the investigational and the control cohorts using methods with demonstrated validity and reliability. These analyses included assessment of segmental rotation (degrees) and translation (in millimeters and percentage) at the treated level(s) and at the adjacent levels. Since the majority of procedures were performed at L4-L5, results for only the level above the implant are reported to avoid accounting for differences associated with L5-S1 levels.
Success of fusion at the treated level was defined as radiographic evidence of “bony bridging” and < 2° rotation from flexion to extension. Bony bridging was defined as a continuous connection of bone from the superior vertebra to the inferior vertebra between the superior and inferior portions of the implant. A definition for lack of fusion success for ILS patients was defined as no bridging bone and ≥ 2° rotation. Maintenance of foraminal height, assessed by x-ray and CT Scans and for the ILS cohort only, required that the month 48 foraminal height be no more than 2 mm less than baseline, where the minimum foraminal height was taken for two-level procedures. Qualitative radiography analysis of device condition was also performed.
Results
Patient Accounting
Consistent with prior reports and with results used to support US regulatory approval,7 analyses were conducted on the Per Protocol (PP) set that excluded 15 of 230 (6.5%) and 7 of 114 (6.1%) patients randomized to ILS and fusion, respectively. This resulted in final sample sizes of 215 ILS and 107 fusion patients. Reasons for exclusion included receiving a two-level decompression but only one-level device implantation, significant violations of inclusion or exclusion criteria including spondylolisthesis beyond Grade 1, and other operative violations for which no waiver was granted. The percentages of patients evaluable for the Month 48 evaluation are high (ILS 184/215, 86.4%; fusion 90/107,85.7%), enhancing generalizability of study results. As previously reported, there were no significant baseline differences in pain, function, or demographic factors between device groups.
Reoperations at the index level and steroid injections at any lumbar
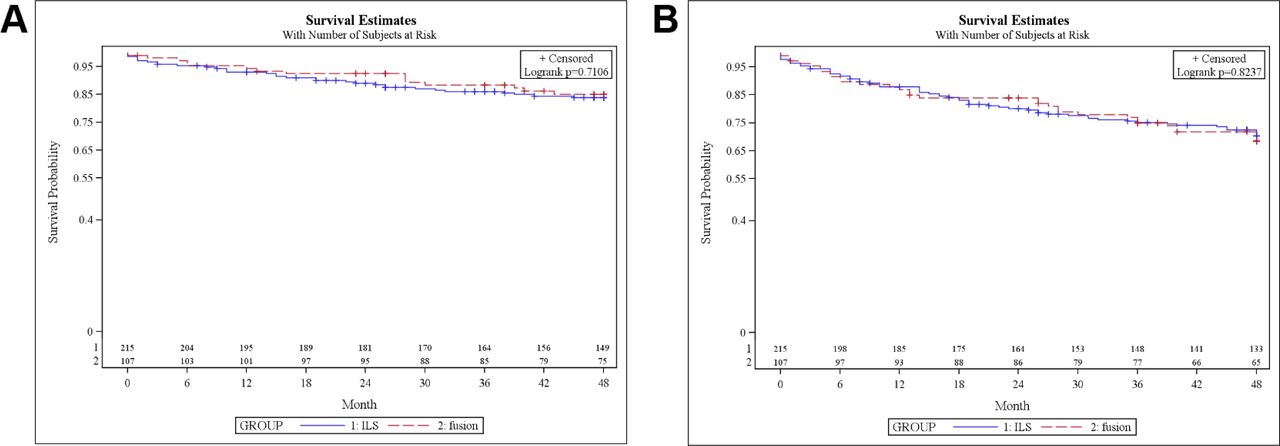
The 48 month cumulative rates of index level second surgeries were 16.1% (SE = 2.6%; 35/215) and 14.9% (3.6%; 15/107) for ILS and fusion, respectively. Kaplan-Meier survival curves comparing times from index surgery to any reoperation, revision, removal or supplemental fixation did not significantly differ between device groups (Figure 1A, logrank p = 0.71). Further analyses revealed that reoperations during the earlier post-op time-period for patients implanted with ILS included a number of index-level post-operative seroma or hematoma, performance of an irrigation and debridement, treatment of dehiscence, and repair of a durotomy that required surgical treatment to resolve. An analogous analysis was performed for the times from index surgery to treatment failure defined as second surgery at the treated level or a steroid injection at any lumbar level, whichever came first. The Kaplan-Meier estimate of the cumulative percentages of patients requiring secondary intervention by Month 48 also did not significantly differ between ILS and fusion (Figure 1B, p = 0.82).
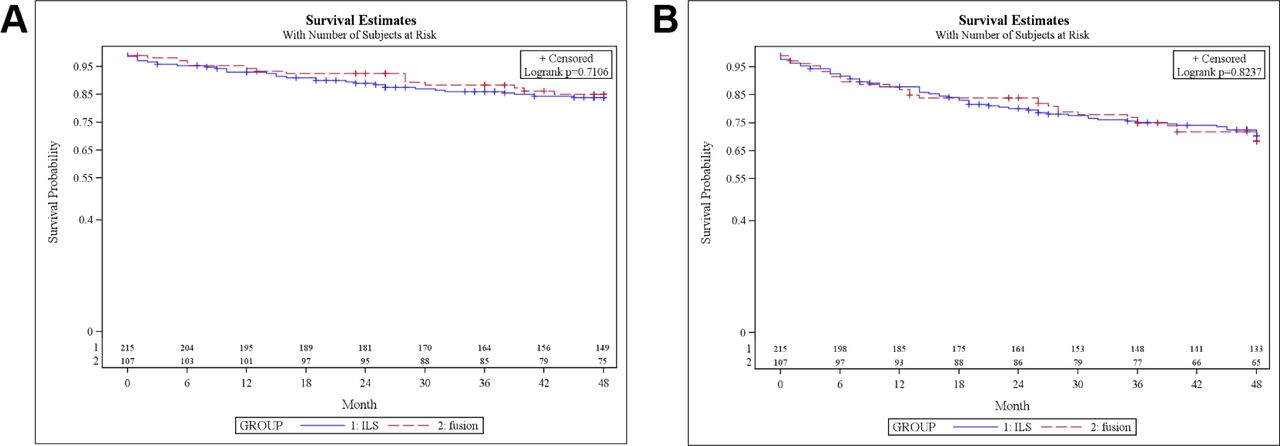
Kaplan-Meier survival curves by device group. A) Distributions of times from index surgery to first reoperation, revision, removal or supplemental fixation at a treated level. B) Distributions of times from index surgery to reoperation at a treated level or steroid injection at any lumbar level.
Patient Reported Outcomes
A clinically significant improvement in ODI was defined to be an improvement of at least 15 points out of 100. Among patients with no index level re-operations or lumbar steroid injections, 86.2% (106/123) of ILS and 72.4% (42/58) of fusion subjects had a clinically significant improvement in ODI scores (p = 0.038). The corresponding mean (SD) improvements were 35.8 (18.8) and 32.0 (24.1), respectively, for ILS and fusion. An improvement of at least 20 mm was used to define clinically significant improvements for VAS scores. Using this threshold, 82.3% (102/124) of ILS subjects and 80.4% (45/56) of fusion subjects achieving clinically meaningful improvement in back pain (p = 0.84), with mean improvements of 52.7 mm (SD = 29.1) and 53.4 (SD = 29.5) mm in the ILS group and fusion groups, respectively. Improvement in leg pain was evaluated by a summary measure that was based on changes in the maximum score (worse) leg. 80.0% (100/125) receiving the ILS and 83.9% (47/56) undergoing fusion experienced a clinically meaningful improvement in leg pain (p = 0.68). Mean improvements in VAS (worse) leg pain were 52.9 (SD = 32.5) and 56.6 (SD = 29.3) for ILS and fusion, respectively. Similar analyses were performed for the ZCQ. A 0.5 improvement in ZCQ symptom severity and physical symptoms was defined as clinically significant. For Symptom Severity, 81.6% (102/125) of ILS and 81.0% (47/58) of fusion achieved a clinically meaningful improvement (p > 0.99) with mean improvements of 1.5 (SD = 1.0) and 1.4 (SD = 0.9) for ILS and fusion, respectively. 81.6% (116/141) of ILS subjects and 74.1% (43/58) of fusion subjects achieved clinically meaningful improvement on the Physical Function ZCQ subscale (p = 0.25) with mean improvements of 1.1 (SD = 0.7) for ILS and 1.1 (SD = 0.8) for fusion.
Overall clinical success at month 48
An overall responder analysis was performed using a composite clinical success (CCS) endpoint. To achieve month 48 CCS the patient must have been free from a reoperation for treatment failure at the index level, have receiving no lumbar epidural injection, and experience a clinically meaningful improvement in pain and function as reflected in at least a 15 point improvement in ODI. The percentages of patients that achieved composite clinical success at month 48 were 57.6% (106/184) and 46.7% (42/90) for ILS and fusion, respectively (p = 0.095). The difference in month 48 success rates is 10.9% in favor of ILS. A 95% confidence interval (CI) for this difference is (-1.6% to 23.5%). Using non-informative priors, the Bayesian posterior probability of non-inferiority (δ = -0.10) of ILS relative to fusion at month 48 is larger than 0.999 confirming the previously established finding of non-inferiority at Month 24. The Bayesian posterior probability that the ILS is superior to fusion based on this endpoint is 0.956.
Radiographic factors
The baseline and month 48 values for rotation, translation (% endplate width) are summarized. There was no statistically significant difference between device groups at baseline in either rotation (p = 0.28) or translation % (p = 0.86). For the ILS group, there was a small but statistically significant mean reduction in rotation from baseline to month 48 at the treated level (-0.64 deg SD = 4.02, paired t-test p = 0.037). In contrast, the mean reduction in the fusion group at the treated level was much larger -2.89° deg (SD = 3.30) and highly clinically significant (p < 0.0001). Similarly, the mean change in translation at the treated levels was not significantly different from zero among patients implanted with ILS (-0.13%, SD = 3.05, p = 0.565). In contrast, the mean change in translation for the fusion group was -1.88% (SD = 2.69), p < 0.0001. The device group differences in mean changes from baseline to month 48 were highly statistically significant for both rotation and translation percentage (p < 0.0001).
These analyses were repeated for the level above the treated level. The mean change in rotation from baseline to month 48 was 0.12° (SD = 3.63) was not statistically significant (p = 0.70) for patients implanted with the ILS. In contrast, among fusion patients, the mean increase in rotation was statistically significant (p = 0.014) above the level of the fusion with mean (SD) equal to 1.42° (SD = 4.53). The device group difference in mean rotation changes above the treated level from baseline to month 48 was statistically significant (pooled t-test p = 0.032).
Further, Figure 2 compares the empirical distribution functions for changes in rotation from baseline to month 48. This graph provides the proportions of patients in both groups (on the y-axis) with values of rotational changes no larger than the values specified on the x-axis. 1 minus this proportion is the proportion of patients exceeding any specified value on the x-axis. For example, if an increase of 3 degrees rotation was considered a clinically significant increase, then the figure shows that 19.4% of patients receiving the ILS compared to 35.4% of patients undergoing fusion (p = 0.015) experienced the magnitude of rotation increases at level above their index level(s).

Empirical cumulative distribution functions for ILS and fusion for changes from baseline to month 48 in adjacent level (above) rotation (degrees).
Other, more qualitative radiographic analyses, showed that in the ILS cohort approximately 39.2% of 181 treated levels had some evidence of heterotopic ossification but only 1 patient exhibited bony bridging in a treated level at month 48. Among 89 levels in the fusion cohort, 76.4% (69/89) demonstrated clear bony bridging and 3 (3.4%) were indeterminate. In 18 levels, there was no evidence of bony bridging.
Among ILS levels the mean foraminal height at the index level(s) was 17.77 ± 2.67 mm at baseline and 17.34 ± 2.81 mm at month 48. For two level procedures, the minimum foraminal height was determined across index level. Minimum foraminal height at month 48 was within 2 mm of pre-operative baseline in 98.4% of patients. This assessment was not carried out for the fusion control cohort.
Analysis of Clinical Composite Success including Therapeutic Sustainability Endpoint (TSE)
The radiographic factors hypothesized to be associated with therapeutic sustainability and described in the previous section were combined with the composite clinical success (CCS) endpoints summarized above which utilized ODI improvements as the PRO. Table 1 summarizes these results in an incremental fashion. The criterion for treated level success for fusion was defined as bridging bone (at all treated levels) and a (maximum) rotation from flexion to extension that was less than 2°. Conversely, treated level success for ILS was defined as no bridging bone (at any level) and rotation of at least 2°.
Composite Clinical Success Summary of Incremental CCS Analyses at Month 48 Including Indicators of Treatment Sustainability.
When “treated level success” is added to the CCS, the success rates change from 65.6% vs. 54.8% to 46.4% vs. 32.3% (difference = 14.2%, 95% CI 2.4% to 26.0%). When adjacent level instability is added to the CCS using ODI the success rates become 58.0% vs. 38.7% (difference = 19.2%, 95% CI 7.2% to 31.3%). When both treated level fusion success and adjacent level instability success are both added to CCS the CCS rates become 39.3% vs. 22.6% (difference = 16.7%, 95% CI 5.8% to 27.6%). Finally, maintenance of foraminal height in ILS was added to the CCS, including both treated level and adjacent level success, the success rates become 35.7% vs. 22.6% (difference= 14.2%, 95% CI 3.5% to 24.9%).
Adverse events
Through 48 months, adverse events rates were similar in both cohorts, although the incidence of events that were deemed ‘definitely or probably related to the implant’ occurred in 14.9% (32/215) ILS patients and in 20.6% (22/107) of fusion patients (p = 0.21). Events that were classified as ‘severe’ occurred in 8.8% of the ILS population and 15.0% of the fusion population (p = 0.13).
Discussion
The coflex IDE clinical trial is the only level 1 study examining longer-term outcomes of interlaminar stabilization after direct surgical decompression for lumbar spinal stenosis. Demonstrating the durability of positive outcomes is essential for validation of the appropriateness of ILS as a treatment option. Durability is demonstrated in this study through the lack of increased revision surgeries or epidural steroid injections in ILS patients compared to fusion in the setting of stabilization after decompression. Additionally, maintained improvements in key PROs including ODI and VAS scores, in addition to lack of any increase in severe device-related adverse events, are further evidence of the therapeutic sustainability and durability of ILS. At month 48 post-op, more patients in the ILS cohort experienced clinically meaningful improvements on ODI, VAS back pain, and ZCQ physical function and symptom severity score than in the fusion control cohort. The percentages of patients achieving meaningful improvements in VAS (worse) leg pain were essentially the same between device groups. Durability of coflex is also supported by the 48 month maintenance of index level motion and foraminal height, as well as the absence of increased motion at the adjacent level. Lumbar fusion is a widely accepted treatment option for relief of mechanical low back pain in the stenotic patient. This study's findings of similar improvements in back pain, if not slightly better, can be accomplished by the offloading of facets achieved with ILS in comparison to fusion after decompression. This confirms that the mechanical effect of ILS offloading of the degenerated facets results in clinical improvement outcomes that are similar to a fusion. VAS Leg improvement was similar in both cohorts, as well. The need for stabilization after decompression is validated, and this data supports superiority of ILS over fusion in the studied patient population.
Adjacent level degeneration after spinal fusion has been well documented, and may lead to the need for subsequent therapies and surgical interventions. This is widely considered to be a main drawback of spinal fusion procedures. More recently, surgical treatments for spinal stenosis have been geared towards the stabilization via preservation of spinal segmental motion in an effort to reduce the development of adjacent level disease. Angular and translational motion data confirms the expected maintenance of index level motion in the ILS cohort and elimination of motion in the fusion cohort. At the level above the implant, angular motion increased significantly in the fusion cohort by a mean of 1.42°. In contrast, neither adjacent level rotational motion nor index level rotational motion where affected by ILS. This data provides Level 1 evidence that spinal fusion results in hypermobility at adjacent levels, while ILS preserves it.
The main limitation for this study is duration of follow-up limited to 48 months at this time. The radiographic indicators of long-term therapeutic sustainability utilized in this study are supported by the literature and further validation through extended follow-up will be of benefit.
Conclusion
This study demonstrates that coflex interlaminar stabilization is associated with improved clinical, safety, and radiographic outcomes at 48 months post-op when compared to fusion in the studied patient population. When considering factors hypothesized to be associated with longer-term therapeutic sustainability and durability, ILS is again superior to fusion.
In a recent publication, Ong et al. has demonstrated that ILS has comparable but slightly better utilities relative to fusion with substantially lower cost over a five-year period with average cost savings of $11,681.10 This led Ong et al. to conclude the ILS after decompression for lumbar spinal stenosis was ‘dominant’ to fusion when considering clinical outcome equivalency, and possibly superiority, in the setting of substantially lower overall costs. These findings are extended in this study by incorporating factors associated with therapeutic sustainability and durability favor ILS over fusion at 36 months post-op, suggesting that the clinical improvements and cost savings advantage of ILS relative to fusion is likely to persist. Considering clinical, radiographic, and comparative effectiveness data generated by this Level 1 study, coflex is proven to be a safe alternative to traditional stabilization with pedicle based fixation at 48 months, and has provided quicker return to function and higher quality of outcomes in the this same timeframe.
Disclosures
Hyun Bae has received research support for clinical trials from Paradigm Spine. Carl Lauryssen is on the scientific advisory board and possesses stock in Paradigm Spine, receives royalties from DePuy, Medtronic, Amedica and owns stock in Spinal Kinetics and SpinalMotion. Scott Leary is a consultant for and owns stock in Paradigm Spine. Greg Maislin is Principal Biostatistician of Biomedical Statistical Consulting (BSC), Wynnewood, PA and was Study Statistician for subject clinical trial. BSC receives compensation for these services and for statistical programming and reporting services provided by BSC staff. Michael Musacchio, Jr. is a consultant and physician educator for Paradigm Spine, though received nothing in relation to this publication.
- Copyright © 2015 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.