


ABSTRACT
Background: Synovial cysts are commonly associated with instability. Whether to fuse patients is a matter of controversy. Simple resection may offer favorable clinical outcomes but may come at the expense of recurrence rate. We describe our experience with the minimally invasive management of these lesions using microsurgical dissection through a tubular retractor system.
Materials: A retrospective cohort study of symptomatic patients with synovial cysts treated by a minimally invasive tubular approach from 2001 to 2018 was performed. We evaluated variables such as preexisting spinal pathology, previous surgery, radiological findings, comorbidities, and secondary surgery requiring fusion. We used the visual analog scale (VAS), the Oswestry disability index (ODI), and the Macnab scale for clinical evaluation.
Results: There were 35 patients with a mean age of 63 years. The mean duration of symptoms before surgery was 195 weeks. Axial pain was present in 77.1% of cases; radiculopathy was the main symptom in 94.3% of cases. The most frequent site was L4-L5 (62.8%). Presenting comorbidities were lumbar stenosis (28.6% of patients), spondylolisthesis (8.6%), and facet hypertrophy (31.4%). Mean surgical time was 143 minutes (range, 55–360 minutes). The mean hospital stay was 2 days, ranging from 1 to 5 days. No complications were encountered as a consequence of the surgical procedure. All patients showed neurophysiological improvement after surgical intervention. A total of 34 patients (97.14%) showed clinical improvement at the end of follow-up, averaging 17 months and ranging from 1 to 60 months, 28 patients (80%) had good to excellent Macnab outcomes, 6 patients (17.14%) were rated as fair, and 1 (2.86%) patient had a poor Macnab outcome. Radicular VAS significantly changed (P < .05) from a preoperative mean of 8.23 ± 1.24 to a postoperative mean of 2.23 ± 1.94. ODI significantly decreased (P < .05) from a preoperative of mean of 41.02 ± 12.56 to a postoperative of mean of 11.82 ± 10.56. We performed fusion at initial surgery in 37.1% of cases; however, 3 more patients required secondary fusion at follow-up.
Conclusion: Our series corroborates the prior literature with a low incidence of synovial cysts in the cervical spine and none in the thoracic spine. The present work shows the efficacy of minimally invasive surgery in the treatment of these lesions. Synovial cysts were associated with instability, ultimately requiring fusion in the majority of patients. The authors' study includes a large patient series with minimally invasive microsurgical decompression performed through a tubular retractor to date.
Level of Evidence: 3.
- minimal invasive spine surgery
- synovial cyst
- instability
- lumbar and cervical spine
- tubular approach
- fusion
- posterior approach
INTRODUCTION
Synovial cysts cause radiculopathy of the exiting nerve root by compressive foraminal stenosis, rarely causing axial pain at initial presentation.1–3 Their most frequent localization is at the facet joints of L4-L5.1,2,4–7 They are rarely encountered in the cervical or thoracic spine.1,2 Synovial cysts are frequently associated with vertebral instability and other degenerative spinal diseases.1,3,6,8,9 Surgical management is considered the treatment of choice5,9–12 due to a lower recurrence rate and more significant improvement of neurological symptoms than conservative or interventional treatments, such as surgical drainage or intralesional steroid injection.5,9,11,13 Current research focuses on the use of minimally invasive surgery as an alternative to conventional open surgery, with lower risks and similar outcomes.13–16 Some authors perform contralateral approaches, advocating better exposure and lower postoperative instability risk due to limited articular bone resection and direct view of the lesion.15–18 Whether to perform a facet joint resection during a spinal fusion or a simple decompression is controversial.11,14,19,20 However, evidence suggests that fused patients have lower recurrences4,6,7,10,12,16,19–25 and, in some cases, better clinical results with decreased postoperative pain.5,25 Consequently, the debate on the optimal treatment strategy for patients with symptomatic synovial cysts continues. We present our 10-year experience in minimally invasive management of these lesions by a tubular approach.
MATERIAL AND METHODS
Study Design and Patients
We performed a retrospective cohort study of 35 patients with symptomatic synovial cysts of the lumbar and cervical spine treated by a single surgeon with a minimally invasive tubular microsurgical approach between December 2001 and May 2018.
Inclusion and Exclusion Criteria
Only patients who underwent spinal surgery because of symptomatic synovial facet cysts and other associated degenerative spine conditions responsive to decompression and confirmed by magnetic resonance imaging or computed tomography were selected for this study. Therefore, the presence of spondylolisthesis or stenosis in the central or lateral spinal canal was not a contraindication to including patients in this analysis. Patients with unmanageable radicular pain unresponsive to a minimum of 12 weeks of medical and interventional conservative care with a positive Lasègue's tension sign and minimal low back pain were included. However, patients with other concomitant conditions that could impair the authors' ability to determine clinical improvements with surgical treatment of synovial cysts were excluded. For example, a concurrent diagnosis of infection, tumor or metastatic disease, recent spinal fracture, coronal or sagittal plane deformity above 30°, behavioral abnormalities, dependence on pain killers, or any electrodiagnostic evidence of chronic demyelination or denervation in the dermatomes innervated by the affected surgical nerve roots prompted exclusion from the study.
Preoperative Work-Up and Clinical Decision-Making
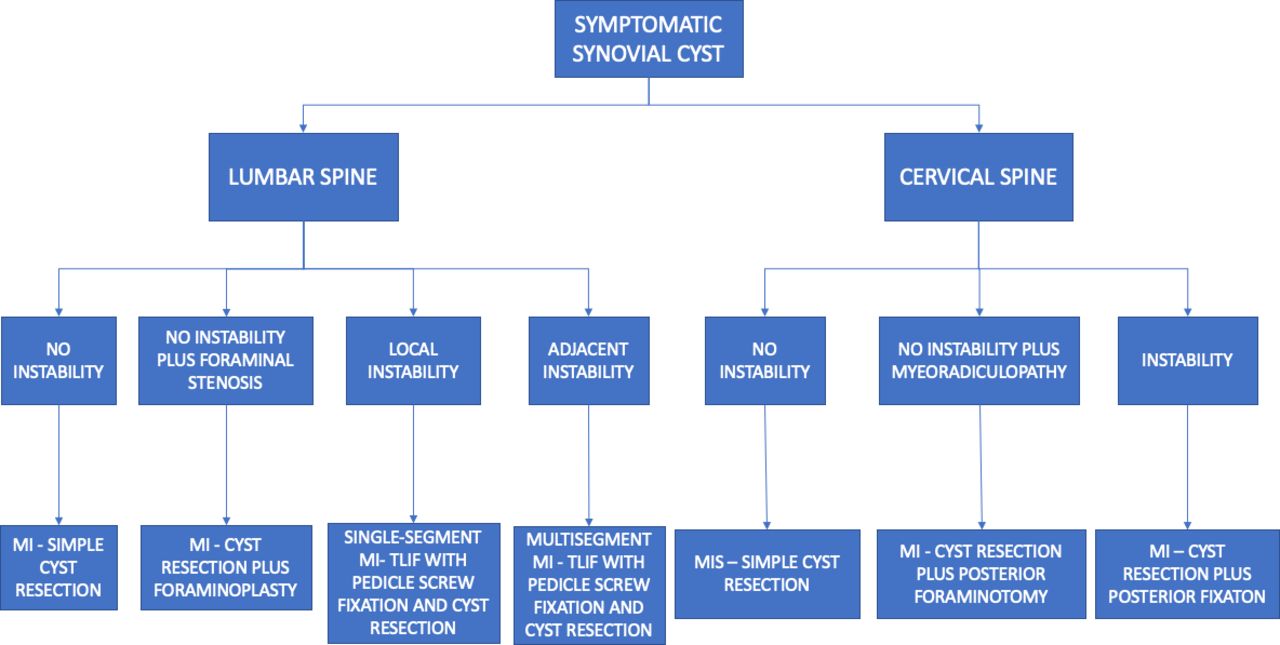
All of our patients were evaluated preoperatively with a thorough physical examination, standing and dynamic x-rays of the region of interest, and magnetic resonance imaging or computed tomography. Additionally, neurophysiologic studies were performed to support clinical decision-making in patients with equivocal findings. Diagnostic facet and selective nerve root blocks were also used. Bone densitometry was performed for patients over 50 years old who were scheduled for fusion. The surgical technique choice was made according to the patient's clinical presentation, synovial cyst location, and the presence of instability. A simple resection of the lumbar cyst was performed in patients without associated instability or other painful spinal pathologies. Minimally invasive transforaminal lumbar interbody fusion (MI-TLIF) was the procedure of choice in patients with spondylolisthesis or instability of the facet joint, as demonstrated by diastasis of the joint space and thickening of the ligamentum flavum.4,10,11,14,16,21,26 For cervical spine cysts, a simple resection was performed in the absence of instability. In patients with cervical radiculopathy in addition to neck pain, we performed a foraminotomy as needed. Patients with concomitant instability at the surgical level should be treated with a simultaneous fusion procedure.19,27,28 The authors' decision-making algorithm is summarized in Figure 1.
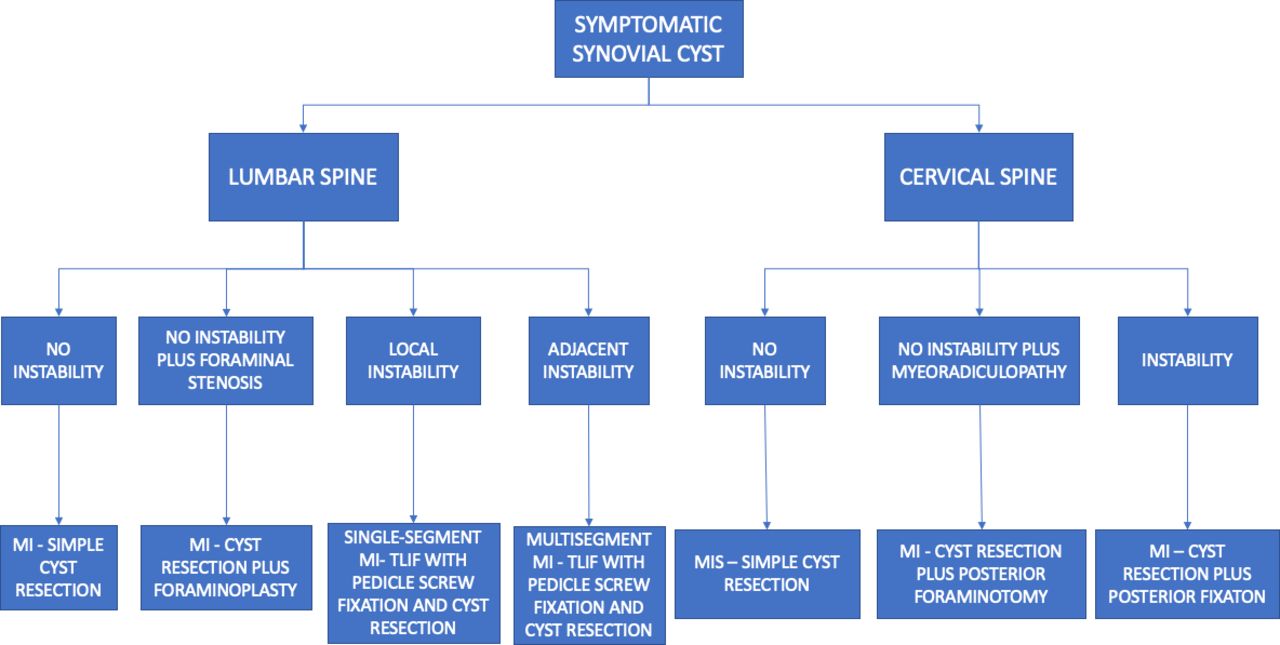
Decision-making algorithm.
Positioning, Anesthesia, and Surgical Approach
Patients were placed in a prone position, and surgery was performed under total intravenous anesthesia without neuromuscular blockade to permit intraoperative multimodal neurophysiologic monitoring in all patients.29–33 After fluoroscopic identification of the lumbar surgical level, a paramedian incision was made approximately 5 mm from the midline. A muscle-splitting dissection technique was used to facilitate tubular retractor placement in the posterior lumbar spine. Serial dilation was used. Throughout the operation, bipolar electrocautery was used to shrink the synovial tissue and control bleeding, after which a multilayer wound closure was performed. The patient was placed in a prone position with a Mayfield head holder, with the head in capital flexion and the cervical spine in extension (military position) for the cervical procedures.
Surgical Techniques
Simple Lumbar Synovial Cyst Resection
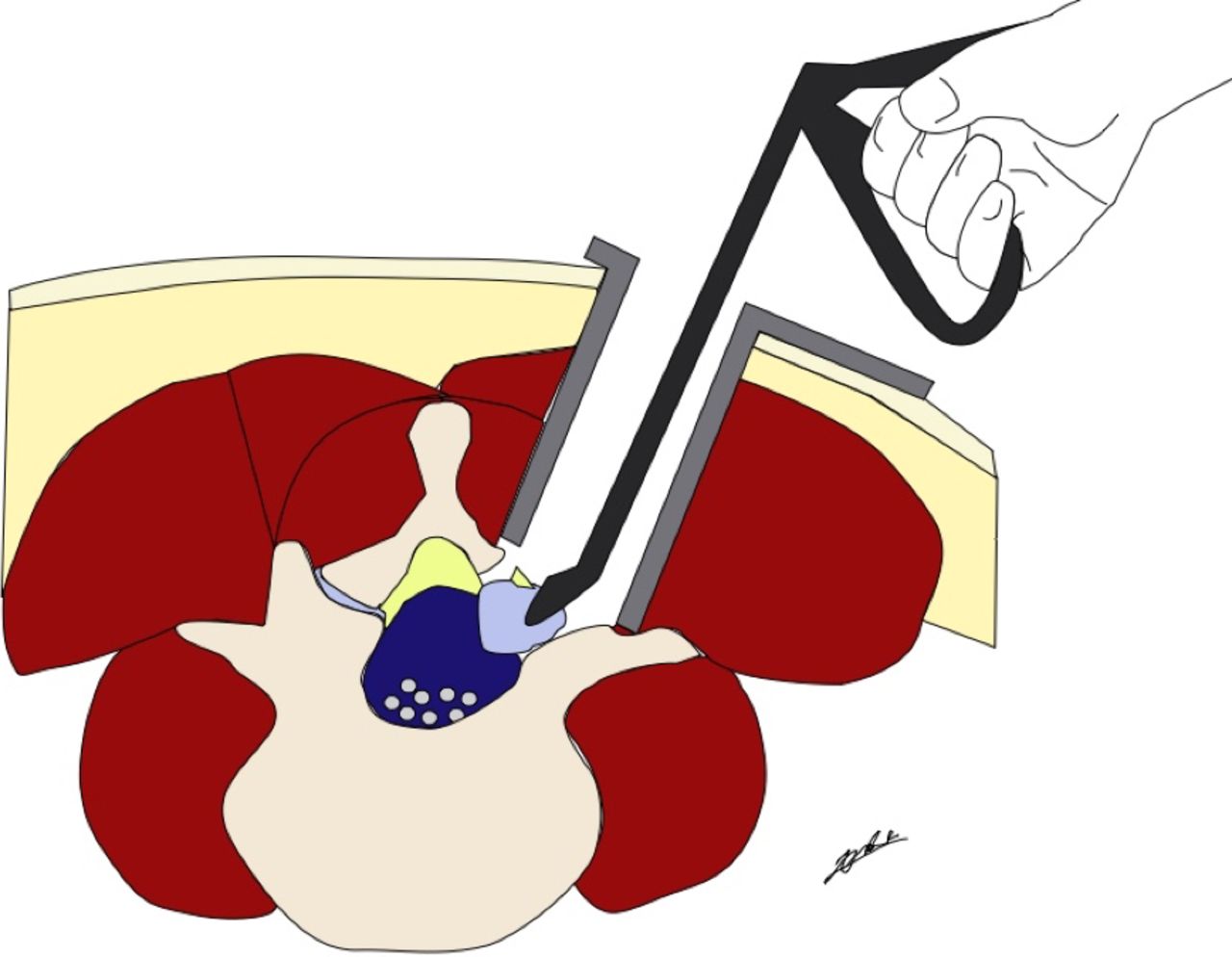
Patients without lumbar instability and no other symptomatic compressive pathology underwent simple resection of the synovial cyst via an interlaminar approach. Typically, a 14-mm tube was sufficient to permit the surgeon to perform the operation. Depending on the cyst's relation to the lamina, we chose the rostral or the caudal lamina to gain access to the cyst with a high-speed drill. Most synovial cysts required minimal laminar resection. At times, partial resection of the pars interarticularis was needed to remove huge synovial cysts. In these cases, the authors often first aspirated the cyst before commencing the decompression with drills and rongeurs. The authors emphasized limiting the medial facet resection to less than 50% to avoid iatrogenic instability. Typically, the decompression was begun medially with partial resection of the ligamentum flavum to accomplish a clear view of the dural sac. Rarely, adhesions of the synovial cyst tissue to the dura could not be safely dissected. To avoid cerebrospinal fistula leakage, a sharp dissection of adherent cyst tissues was occasionally required, leaving some synovial membrane on the dura. Figures 2 and 3 demonstrate the surgical technique.
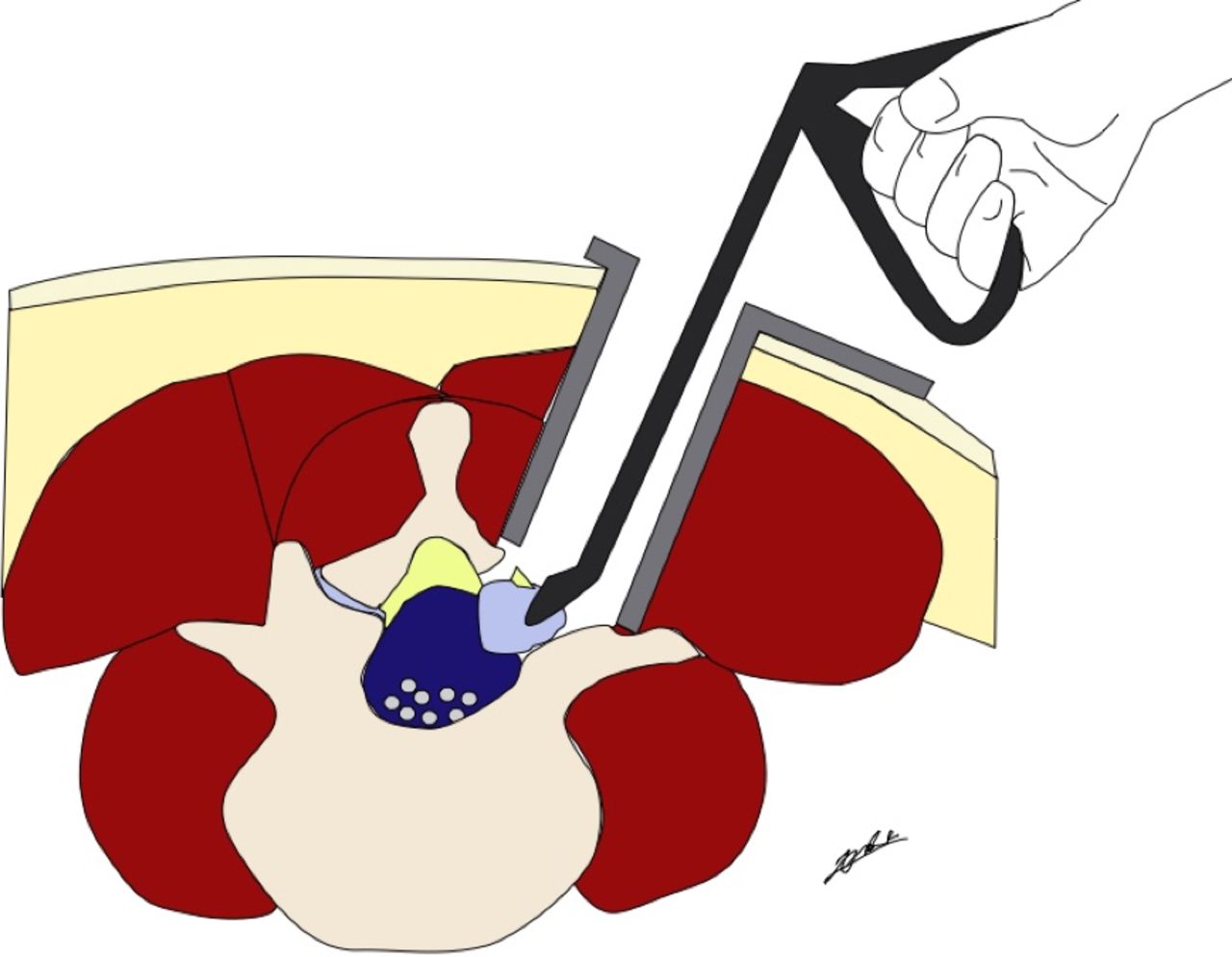
Schematic drawing of simple lumbar synovial cyst resection.
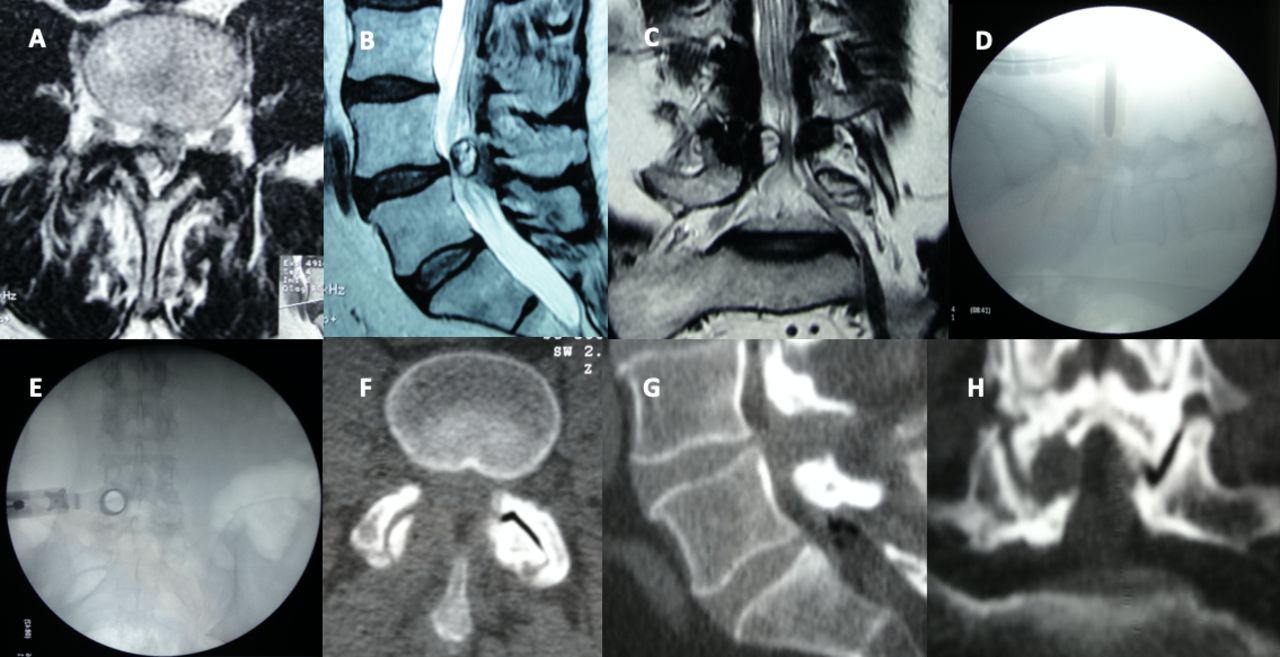
An illustrative case demonstrating an L4-L5 right synovial cyst resection (A). Axial (B), sagittal (C), and coronal T2-weighted magnetic resonance imaging images show a synovial cyst causing lumbar spinal stenosis. Intraoperative lateral (D) and anterior-posterior fluoroscopic views show the tubular retractor positioned right above the facet-laminar junction. Postoperative axial (F), sagittal (G), and coronal (H) computed tomography scans demonstrate laminotomy and validate the cyst resection.
Lumbar Foraminoplasty
For selected cases with radiculopathy in addition to low back pain and foraminal stenosis at the level of the synovial cyst and no local instability, a foraminoplasty was additionally performed to allow for simple resection in the same segment. Once the synovial cyst had been removed, we proceeded to perform an undercutting of the adjacent facet joint junction using an ultrasonic bone aspiration device with careful attention to resect no more than 50% of the facet joint. Thorough surgical decompression of the foramen with resection of the tip of the inferior articular process is of the utmost importance in these cases as the resolution of clinical symptoms may be otherwise incomplete.
MI-TLIF
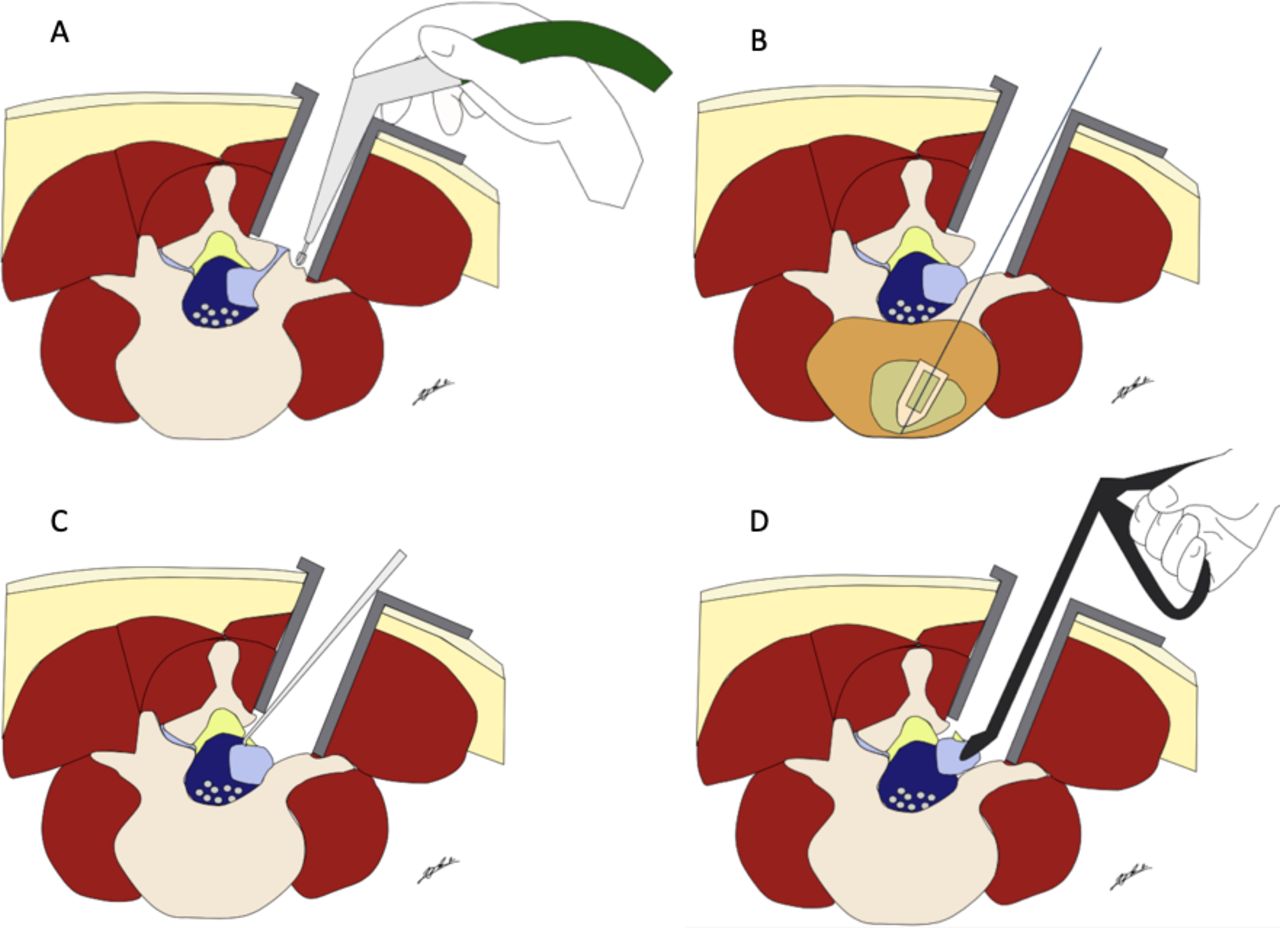
Patients with Meyerding grade I or higher underwent MI-TLIF using a senior author's modified technique described herein. The skin incision was placed 2 cm lateral to the lateral interpedicular line, as verified on the intraoperative fluoroscopic posterior-anterior view. The surgical level was confirmed in the lateral projection. A surgical access corridor was created, exploiting the intermuscular plane between the longissimus and iliocostalis, easily identified by digital palpation. A 20-mm tubular retractor was placed on top of the facet joint complex to best facilitate the insertion of an interbody cage. The decompression was begun from lateral to medial using a high-speed drill. The authors' preference was to leave a thin portion of the most medial part of the superior articular process and the inferior articular process intact to avoid dural tears. Once the intervertebral disc was exposed, a bayonetted knife was used for the annulotomy, and a port cannula was positioned in the intervertebral space through the tubular access retractor to facilitate the discectomy and endplate preparation done with the use of disc rongeurs and endplate dissectors. Bone graft was harvested locally, mixed with a demineralized bone matrix, and abundantly placed into the disc space through the cannula and within the polyetheretherketone interbody fusion cage. The latter was inserted over a Kirschner wire. The authors aimed to position a single interbody fusion cage into the anterior third in the lateral projection and across the midline in the posterior-anterior projection. After completing the interbody fusion with cage insertion, we completed the decompression by removing the remaining medial portion of the inferior articular process and superior articular process, ligamentum flavum, and the cyst. The MI-TLIF was then concluded with the placement of percutaneous pedicle screws. Briefly, a Jamshidi needle was used to cannulate the surgical pedicles under posterior-anterior and lateral fluoroscopic control, and the cannulated screws were inserted via a Kirschner wire. The screws-rod construct was completed by securing a rod with set screws under slight compression that was intentionally chosen 5 mm longer than the distance measured between the screws. Figures 4 and 5 demonstrate the surgical technique.
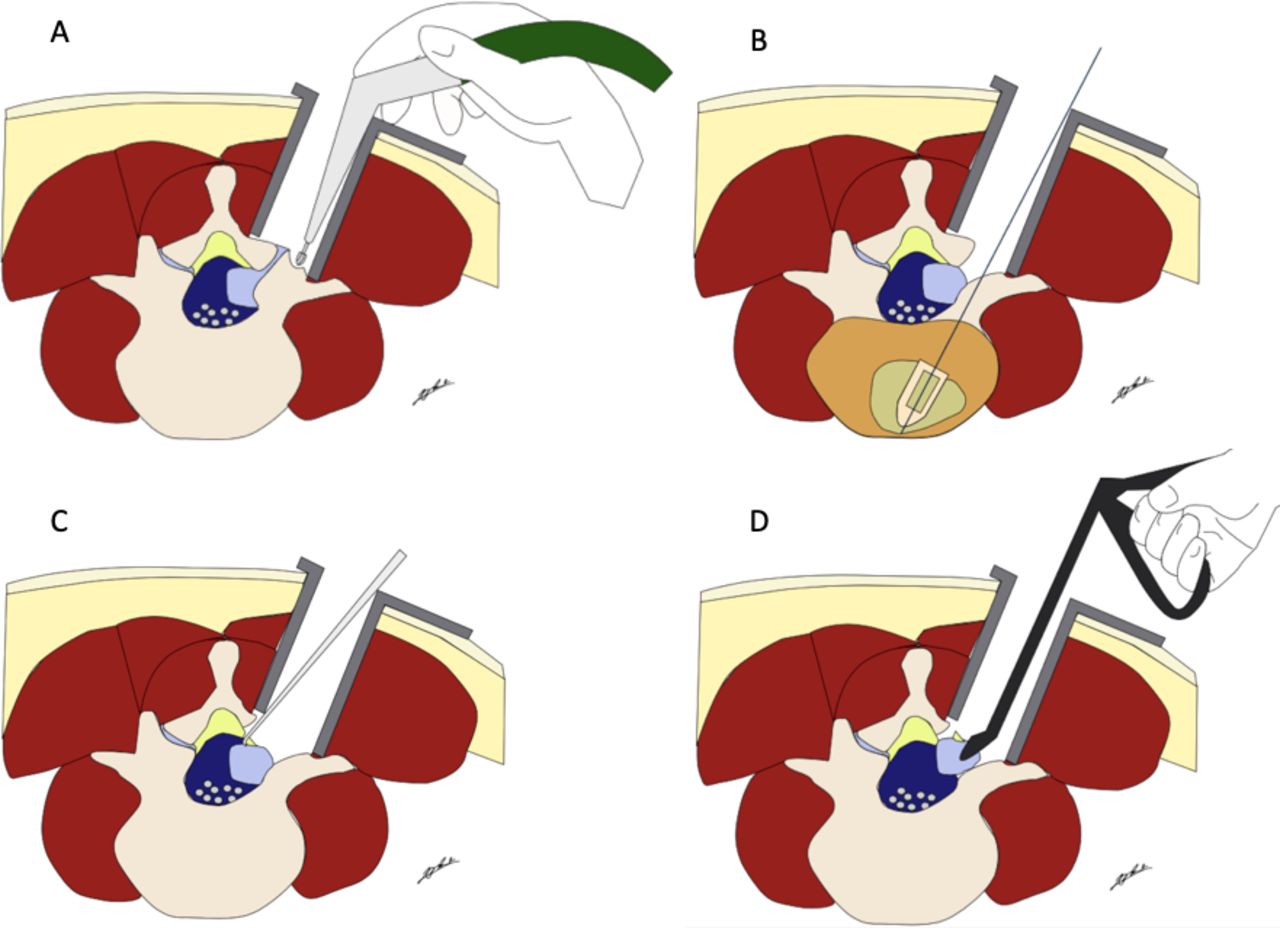
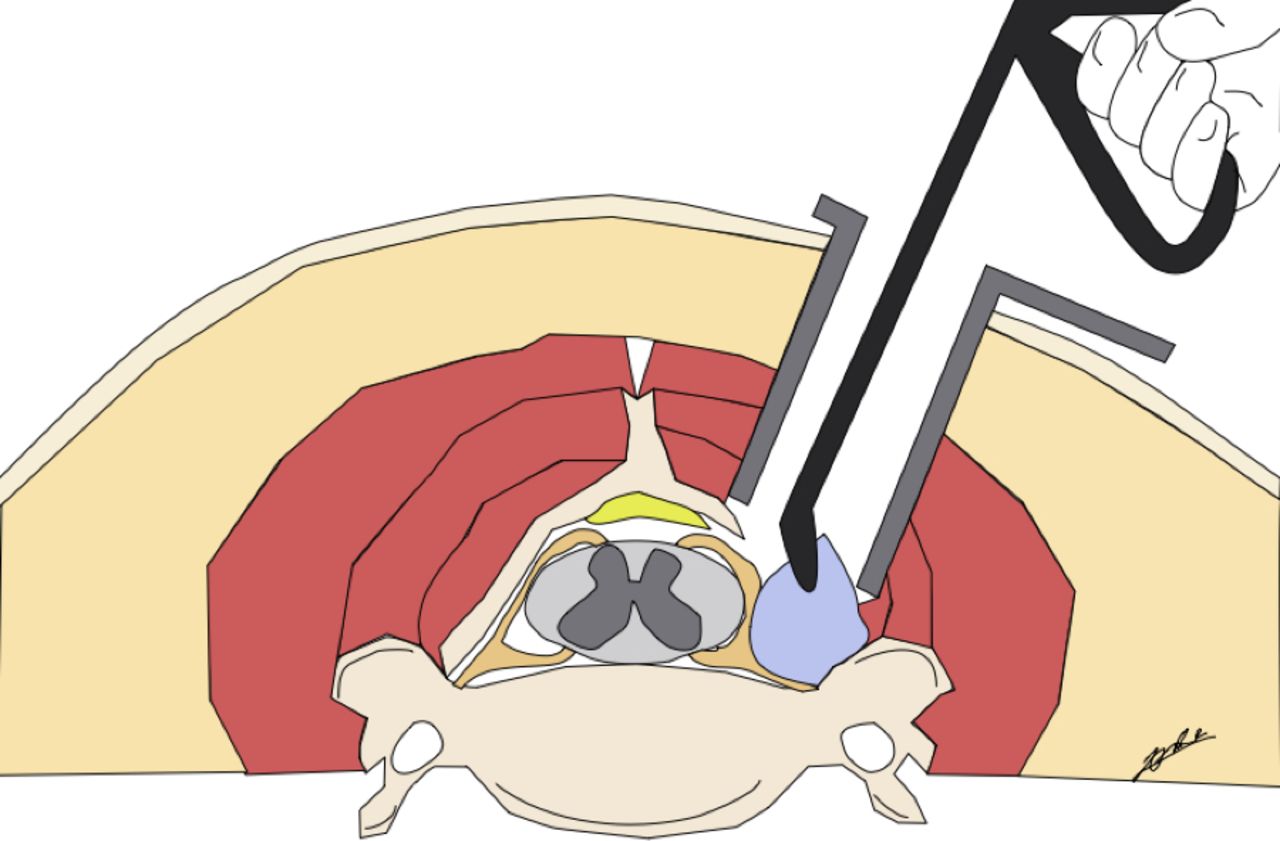
Schematic synovial cyst resection and transforaminal lumbar interbody fusion. (A) Lateral facetectomy by high-speed drill. (B) Bullet cage inserted by aid of Kirschner wire once the synovial cyst has been completely removed and the thecal sac decompressed. (C) Medial ligamentum flavum incision for medial to lateral dissection from underlying normal dura to synovial cyst capsule. (D) Synovial cyst resection with overlying ligamentum flavum.

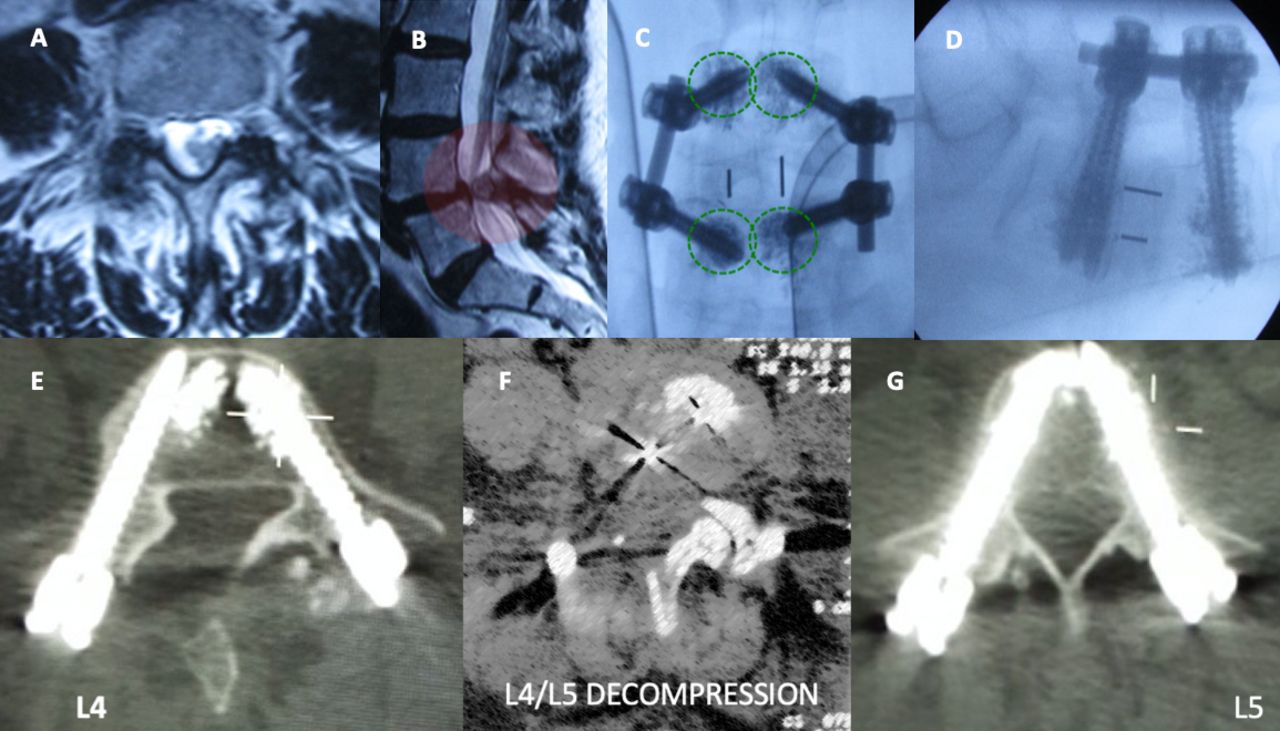
An illustrative transforaminal lumbar interbody fusion (TLIF) case shows axial (A) and sagittal (B) magnetic resonance imaging scans demonstrating a huge right synovial cyst at the L4-L5 level. Anterior-posterior (C) and lateral (D) intraoperative fluoroscopic views illustrating TLIF and transpedicular screw fixation augmented with bone cement because of osteopenia evident on the preoperative bone density scan. The postoperative axial computed tomography scan images (E–G) validate the L4-level cyst resection, adequate position of the interbody fusion cage, and the L4 and L5 pedicle screws without breaches.
Simple Cervical Synovial Cyst Resection
This procedure was done in patients without instability or associated cervical compressive pathologies. The skin incision was marked over the surgical level by the aid of fluoroscopy. On the true anterior-posterior projection, the skin was marked 2 cm lateral from the midline. The lateral view was used to confirm the procedure's cervical level requiring decompression properly. We performed a muscle-splitting dissection technique through the muscle bundles in each layer in the direction of its fibers until the laminofacet junction was reached. Then, we inserted the cylindrical dilators above the facet junction using fluoroscopy to place a tubular retractor. Often, a 14-mm tube was sufficient to resect synovial cysts. Depending on the relation of the cyst to the laminae, we chose the upper or the lower lamina for high-speed drilling. The decompression commenced from the most medial aspect of the ligamentum flavum and proceeded laterally, dissecting the plane between the dural sac and the cyst's sac. Complete cyst resection and extirpation may be facilitated by a combination of bipolar electrocautery and mechanical traction with rongeurs and disc clamps. Careful hemostasis was confirmed before closing the soft tissues by a multilayer technique. Figure 6 demonstrates the surgical procedure.
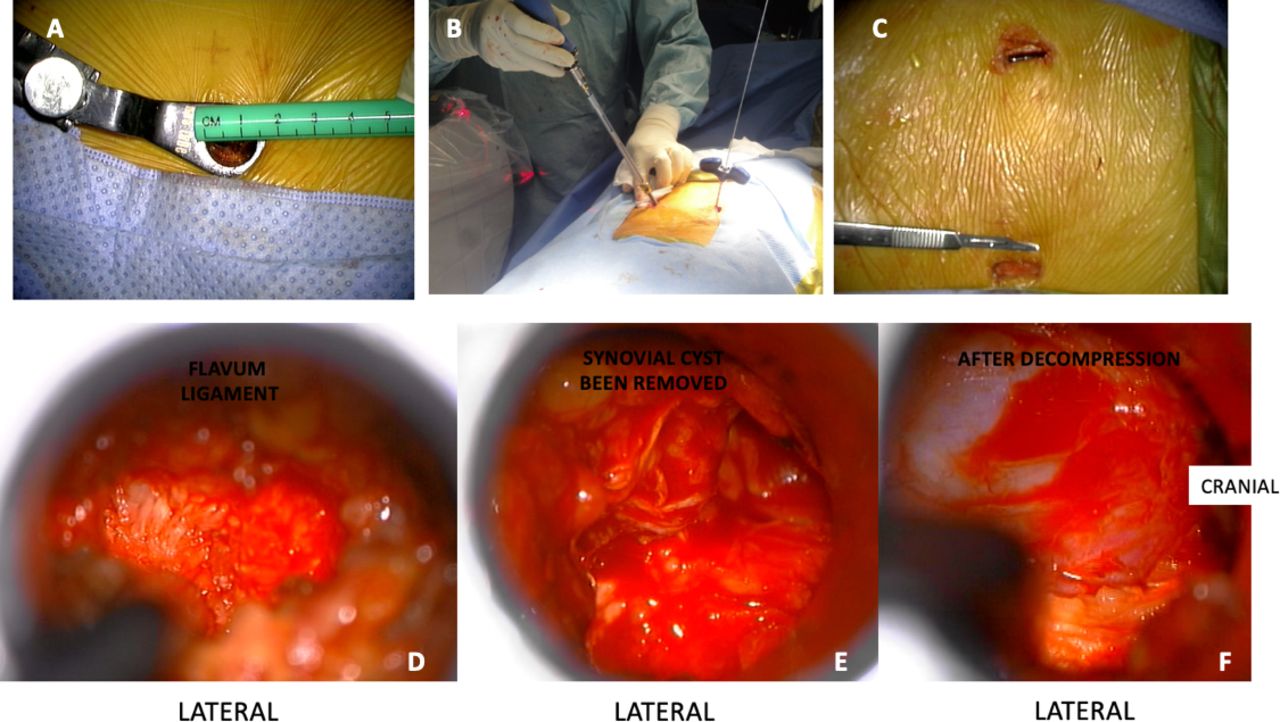
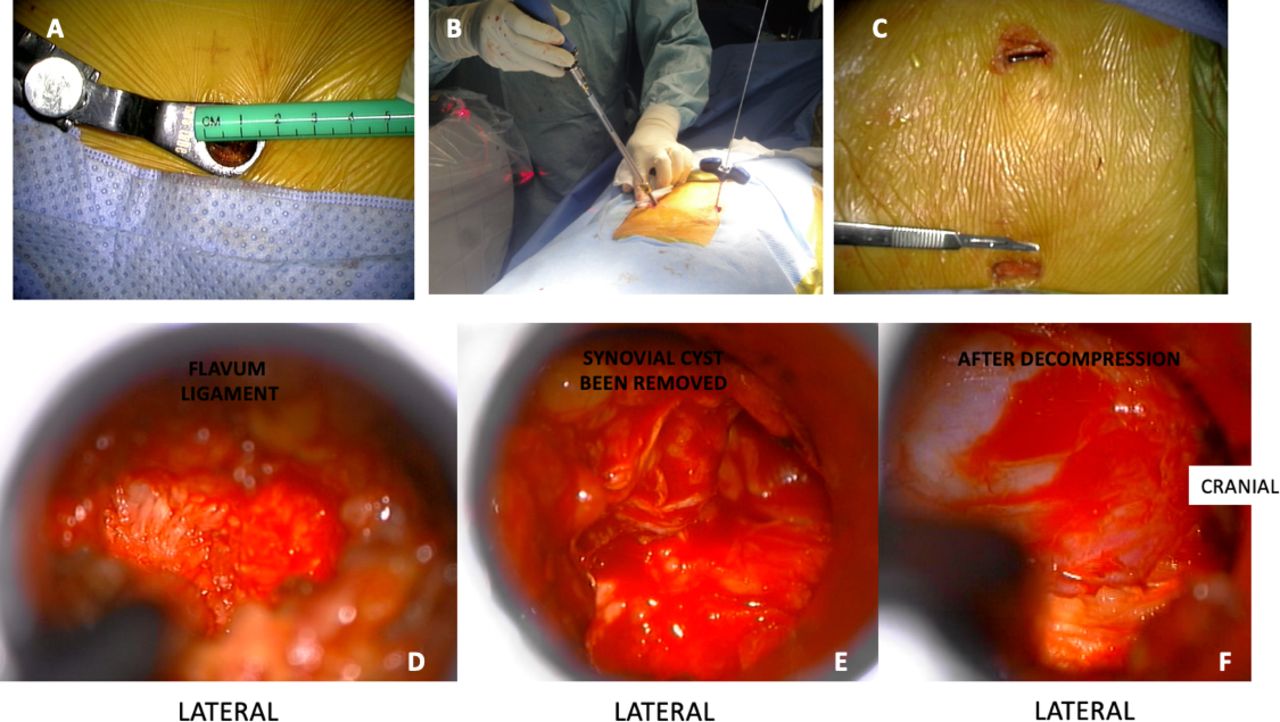
Continuation of the same illustrative case shown in Figure 5. A 14-mm tube was placed for right-sided transforaminal lumbar interbody fusion and synovial cyst resection (A). Bilateral transpedicular screw fixation after transforaminal interbody fusion and cyst resection was performed (B). Bilateral skin incisions (right side at the bottom, left side at the top) were made (C). The ligamentum flavum was identified (D), and the synovial cyst (at the top) was noted to be adherent to it (E). The decompressed dural sac was visualized after completion of the cyst resection (F).
Cervical Foraminotomy
In patients where the synovial cysts cause both neck pain and radiculopathy due to associated foraminal stenosis, a posterior foraminotomy was performed in addition to the cyst resection (Figure 7). Once the cyst had been thoroughly dissected, we proceeded to identify the exiting nerve root under the laminofacet junction. A standard keyhole foraminotomy was performed with attention to resecting less than 50% of the overlying facet joint. The authors also used an ultrasonic bone aspiration device to avoid excessive friction-induced heating of the underlying nerve root and its dorsal root ganglion.

Schematic of simple cervical synovial cyst resection.
Demographic Data and Outcome Measures
We collected the following data from the patients' charts: age, sex, body mass index, time to presenting symptoms, preexisting spinal pathology, previous surgery, radiological findings (level, side, and presence of instability by dynamic lumbar plain films), comorbidities, type of surgery, and follow-up, including patients requiring secondary fusion. Initially, a blinded researcher reviewed the patients' charts retrospectively. The data were entered into a Microsoft Excel spreadsheet. Primary clinical outcome measures were reductions in the visual analog scales (VAS)34 for leg, ranging from no pain (0) to worst pain (10), and the Oswestry disability index (ODI). The ODI is a 10-item composite instrument assessing pain intensity, personal care, and function, including walking, lifting, personal care, sitting, standing, sleeping, social interaction, and traveling35,36 Postoperatively, patients were scheduled to be seen in follow-up for reevaluation at 6 weeks and then at 3, 12, and 24 months. These lumbar primary clinical outcome tools recorded preoperatively and at final follow-up were used for the authors' statistical analysis. This analysis was only performed on patients with lumbar spine synovial cysts since there were only 2 patients suffering from synovial cysts of the cervical spine.
Statistical Analysis
To minimize selection and hindsight bias, this unidentified patient database was transferred to Statistical Package for Social Sciences version 26. Descriptive statistics (mean and standard deviation) and cross-tabulation statistics were computed for two-by-two tables. The Pearson χ2 and the likelihood ratio χ2 tests were used as statistical measures of association between confounding demographic and clinical factors, complications, and clinical outcome measures. The confidence intervals for the likelihood ratios were calculated using the “log method” according to Liberati and Altman et al.37
RESULTS
From December 2001 to May 2018, 35 patients were operated using a minimally invasive tubular approach and included 26 (74.3%) females and 9 (25.7%) males, with a mean age of 63 years (47-80 range) and a mean time to symptom presentation of 195 weeks, ranging from 4 to 728 weeks.
Thirty-three patients had lumbar cysts, and 2 had facet cysts of the cervical spine. Five patients (14.3%) had prior spine surgery, 3 in the lumbar (8.6%) spine and 2 (5.7%) in the cervical spine. No previous surgery was performed at the level of the symptomatic synovial cyst; however, a lumbar case was associated with a synovial cyst in the adjacent segment. Radiculopathy was the main symptom in 33 patients (94.3%), low back or neck pain was the main symptom in a total of 27 patients (77.1%), and as few as 10 patients (28.6%) had decreased sensitivity and up to 24 patients (68.6%) had some degree of paresis. Table 1 summarizes demographic and preoperative data. The most frequently affected segment was L4-L5 in 22 cases (62.8%). Left-sided pathology was seen in 17 (48.57%) patients, and the same was observed for right-sided pathology, with just 1 patient having bilateral compromise (2.86%). Magnetic resonance imaging findings more frequently encountered were fluid-filled facets instead of facet degeneration in up to 88.57% of our patients (31 patients). Concurrent spondylolisthesis was found in 17 patients representing 48.6% (Meyerding grade I), severe facet degeneration (Grogan III and IV) in 11 cases (31.4%), and 10 patients (28.6%) with associated lumbar stenosis (Table 2).
Demographic and preoperative data.
Summary of clinical series.
Single-level surgery was performed in 23 (65.7%) cases, while 12 patients (34.3%) required multiple-level surgery. An average of 1.4 surgical procedures per patient were done. Simple resection of the synovial cyst was the surgical procedure in 14 patients (40.0%). The two cervical patients underwent simple resection of the cyst in 1 patient and with additional foraminotomy in the other patient. In comparison, a MI-TLIF and transpedicular fixation was required in 13 patients (37.1%). In the remaining 8 patients (22.9%), a foraminotomy (7 patients) with foraminoplasty (1 patient) was performed to manage their symptoms adequately. Adjacent segment pathology developed (radiological findings) in 8 patients (22.9%), and 3 patients (8.57%) ultimately required late fusion, contributing to a final fusion rate of 45.7% (16 cases). Mean surgical time was 143 minutes (range, 55–360 minutes). The mean hospital stay was 2 days, ranging from 1 to 5 days. No complications were encountered as a consequence of the surgical procedure. All patients showed neurophysiological improvement after surgical intervention. A total of 34 patients (97.14%) showed clinical improvement at the end of follow-up, averaging 17 months and ranging from 1 to 60 months, 28 patients (80%) had good to excellent Macnab outcomes, 6 patients (17.14%) were rated as fair, and 1 (2.86%) patient had a poor Macnab outcome. Radicular VAS scores significantly changed (P < .05) from a preoperative mean of 8.23 (range, 6–10) to a postoperative mean of 2.23 (range, 0–9). ODI significantly decreased (P < .05) from a preoperative mean of 41.02 (range, 14–60) to a postoperative mean of 11.82 (range, 0–54). Table 3 summarizes the relevant postoperative clinical data. These VAS leg score and ODI reductions were statistically significant (Tables 4 and 5). The case with poor outcomes developed a recurrence in the same surgical site, and another patient developed a de novo synovial cyst in the contralateral segment.
Postoperative clinical outcomes.
Paired sample t test of preoperative and postoperative VAS leg and ODI scores.
Paired differences of preoperative and postoperative VAS leg and ODI scores.
DISCUSSION
Our clinical series compares favorably to reported series in the current literature. Radiculopathy was the main symptom followed by axial pain. Nevertheless, muscle weakness showed a higher incidence rate (68.6% compared with 32–40% reported rate).3,10,21 In the present series, we observed similar mean age and a slightly higher rate of female predominance (74.3%) than more extensive series (50–67%).13,25,38
Birch et al13 reported a history of prior surgery in 2.5% of cases compared with our incidence rate of 14.3%. Due to a high percentage of comorbidities, including spondylolisthesis, severe facet degeneration, and lumbar stenosis, many of our patients required an extended surgical procedure and early fusion with MI-TLIF and supplemental posterior transpedicular fixation. The authors agree with prior reports in that the natural history of synovial facet cysts is likely related to the progression of instability of the involved lumbar spinal motion segment, as was seen in the 8 patients (22.9%) requiring primary fusion and in the 3 patients (8.57%) ultimately requiring late fusion, contributing to a final fusion rate of 45.7% (16 cases).38 Our findings of higher rates of subsequent adjacent segment pathology (22.9%) and symptomatic disease (8.57%) are corroborated by many prior reports.1,8,10,11,13,25
Our series includes one case of a de novo synovial cyst generation at the contralateral side of initial resection, advocating a clear role in instability development to synovial cyst pathology. The most frequent site of the synovial cyst was L4-L5, as in most series. Our initial fusion rate was 37.14% (13 patients); however, 48.6% of patients had preexisting spondylolisthesis in an otherwise asymptomatic and initially unrelated segment. Therefore, 3 more patients ultimately required secondary fusion, increasing the final fusion rate to 45.71%.
The main limitation of the current study is its single-surgeon and single-center nature. Therefore, favorable outcomes could have been artificially inflated by using our reproducible surgical protocol since all of our team members had already mastered the learning curve. Our favorable clinical results may not be reproducible to this extent by surgeons with less clinical support or training. Another limitation is the retrospective nature of our study. We attempted to minimize selection, recall, or hindsight bias by incorporating diagnostic facet and nerve blocks.39–41 Lastly, a short follow-up (mean of 16.8 months) could be considered as problematic even though long-term follow-up was available in several early patients (follow-up to 60 months).
CONCLUSIONS
Clinical outcomes of our series with the surgical treatment of synovial cysts in the spine are comparable to prior reports. Synovial cysts are uncommon in the cervical and thoracic spine. The present work shows the efficacy and safety of minimally invasive surgery using a tubular retractor system in the treatment of these lesions, many of them requiring fusion due to instability related to the underlying degenerative disease of the spinal motion segment and its progression.26 A high rate of spondylolisthesis, adjacent segment disease, or development of a synovial cyst on the contralateral side of the primary cyst resection should be expected.
Footnotes
Disclosures and COI: We have no conflicts of interest nor any financial relationship or funding to disclose.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}