


Abstract
The thoracolumbar spine poses unique challenges when considering surgical treatment options. In the era of modern medicine, nonoperative treatments have become more available for pathology of the thoracolumbar spine, including infectious, oncologic, traumatic, and degenerative etiologies. However, surgery is often warranted in the presence of deformity or with spinal cord compression resulting in neurologic deficits. Traditionally, posterior or anterior approaches were used for surgical treatment in the thoracolumbar spine. The mini-open lateral approach for corpectomy in the thoracolumbar spine is relatively new but not yet widely utilized, is less invasive, and is a less morbid surgical option for treating what has historically been a challenging surgical location. A thorough understanding of the anatomy associated with this approach is essential to perform safe and successful surgery with this technique. This review outlines the preoperative and anatomical considerations, surgical technique, contraindications, potential complications, and clinical outcomes associated with performing corpectomies in the thoracolumbar spine via the mini-open lateral approach. This is a safe, successful, and appealing surgical option for appropriately selected patients with diseases of the thoracolumbar region.
INTRODUCTION
Thoracolumbar disease constitutes a significant challenge for surgeons and patients alike. Several etiologies may affect the thoracolumbar spine, including infectious, oncologic, traumatic, and degenerative pathologies. When surgical intervention is warranted, the traditional approach has been posterior or posterolateral, including transpedicular and costotransversectomy techniques.1 The anterior approach was later defined as a means to access the anterior thoracic spine via an open thoracotomy. However, this approach is associated with a high rate of morbidity. As a result, less invasive approaches to this challenging surgical location, such as the anterior thoracoscopic approach, were defined in an effort to provide patients with a surgical option that carried with it less morbidity.2 With additional emphasis placed on the need for more minimally invasive surgical techniques and instruments, the mini-open lateral retropleural/retroperitoneal approach for thoracic and thoracolumbar vertebral body pathologies became a new and viable solution for anterior column disease.3
Lateral approaches to the thoracic and lumbar spine are now frequently used for traumatic, degenerative, oncologic, and infectious pathologies that involve the vertebral body or disc space, or that cause ventral spinal canal compression.4 In thoracolumbar spinal trauma, lateral mini-open access provides an alternative to the traditional posterior approach and offers a favorable surgical window for the removal of fracture elements in the presence of retropulsion causing compression of the thecal sac. The less invasive nature limits the impact on an already ailing mechanical integrity of the spine, reduces the risk for future misalignment, and leads to faster hospital discharge and recovery. Herniated discs of the thoracic spine are rare because the costovertebral joint and rib cage distribute the biomechanical forces, leading to a thoracic disc herniation incidence of less than 1 in 1 million. Most disc herniations occur below the level of T8 due to increased mobility and increased agenesis of the ribs in a caudal direction.5,6 Compression of the spinal cord and progressive myelopathy can necessitate surgical disc removal, and lateral corpectomies provide favorable outcomes with a reasonable risk profile.7,8 Spinal malignancies are a frequent occurrence in an aging society, as two-thirds of patients with malignant tumors will at some point acquire bone metastasis.9 Of these, 10% are located in the spine, primarily in the posterior half of the vertebral body.10 Patients who present with pathologic fractures causing significant deformity or with neurologic deficits due to spinal cord compression may benefit from the lateral mini-open approach for surgical removal of the vertebral body. In addition, other rare primary bone tumors of the spine, such as chordomas and osteosarcomas, may require surgical removal.11,12
Infectious diseases of the spinal column, such as discitis and osteomyelitis of the vertebral body, are commonly managed and eradicated with longstanding medical therapy. The surgical removal of contaminated tissue and spinal reconstruction become vital therapeutic steps in the setting of neurologic compromise. Lateral access to the infectious nidus can obviate the risks of major vessel damage of anterior approaches and increase visibility of both the anterior column and the thecal sac. This access can prevent iatrogenic neural compromise and increase the surgical visibility in an often occult, purulent cavity.13
Approaching and operating on the thoracolumbar spine pose significant surgical challenges due to unique anatomical hindrances that need to be negotiated to avoid damaging the lung parenchyma, peritoneal contents, and associated vasculature, as well as the weight-bearing properties of the thoracolumbar spine.14–16 Moreover, the proximity of the thoracic spinal cord and the conus medullaris in this region poses a significant risk of iatrogenic injury and neurologic morbidity during these procedures.
When this technique is executed well, it can avoid the drawbacks of open anterior approaches (ie, extensive trauma and blood loss) and of posterior approaches (ie, damage to the dorsal musculoskeletal apparatus).17 We review the intricate anatomy, approach, and operative nuances of the mini-open lateral thoracolumbar corpectomy.
MINI-OPEN LATERAL THORACOLUMBAR CORPECTOMY
Preoperative Considerations
Patient selection plays a significant role in obtaining successful surgical outcomes and begins with a thorough history and physical examination. Patients with thoracic spine pathology, including traumatic, infectious, oncologic, and degenerative etiologies, can present with similar symptomatology. Many patients will report axial back pain localized to the pathologic level or in a radicular distribution. Findings of neurologic deficits, including weakness, sensory deficits, pathologic reflexes, or bowel or bladder retention or insufficiency, may also be seen and indicate the presence of thoracic myelopathy. These symptoms are the result of compression of the spinal cord or cauda equina.
Once the above history is obtained, a complete diagnostic workup is required. For suspected tumor and infectious pathologies, magnetic resonance imaging (MRI) with and without contrast is the gold standard used for diagnosis.18 An MRI without contrast is sufficient for workup of lateral thoracic disc herniations and traumatic pathologies. In a patient in whom an MRI cannot be obtained, a computed tomography myelogram is suggested. This imaging helps determine the extent of pathology, including the amount of spinal cord or nerve compression, as well as the degree of associated calcification. MRI provides the added benefit of demonstrating the lateral thoracic spinal anatomy, which is paramount to a less invasive exposure.19 Specifically, determining the size and location of segmental arteries can help when choosing from which side to approach the lesion. Of particular importance is the highly variable great anterior radiculomedullary artery, also known as the artery of Adamkiewicz, which most commonly localizes between the levels of T8 and L1, most often on the left side. Lesions in this artery can lead to major motor and sensory morbidity. However, this artery can potentially be spared using this approach.20,21 Additionally, noncontrast computed tomography and standing radiographs are highly recommended to accurately confirm the vertebral level of pathology and can also provide insight into global spinal alignment. A radioisotope bone scan is a useful imaging modality for patients with known metastases because these scans can elucidate small lesions in the bone and can also highlight osteolytic or osteoblastic activity.22 Finally, diagnostic spinal angiograms can be used when a vascular tumor is high on the differential diagnosis list. Imaging can serve dual purposes: to help diagnose the lesion and to provide a treatment option of preoperative embolization to help reduce blood loss intraoperatively.23
Anatomical Considerations
This technique is technically challenging and requires extensive knowledge of local neurovascular and visceral anatomy. In addition, tubular retractors and minimally invasive instrumentation need to be navigated safely in narrow working corridors. Patient-specific anatomy, such as segmental artery size and location, is important for the appropriate laterality and angles toward the pathology. Prior to the analysis of patient-specific anatomy through MRI, the patient’s spinal column alignment and posture need to be studied for a comprehensive assessment of whether the patient needs spinal column stabilization. Unique anatomical considerations for lateral approaches of the thoracolumbar region primarily relate to the presence of the rib cage and diaphragm, which extends into 2 arcuate ligaments and 2 crura posteriorly. Knowing the anatomy of the diaphragmatic components is particularly important due to its strong variability among healthy patients, with age and weight having a significant influence on the position and shape of the diaphragm.24 The costal insertions of the diaphragm are of primary importance for this approach, as they are violated upon removal of the rib. These insertions guide the surgeon along the appropriate anatomical plane, toward the lumbar attachments at the arcuate ligaments and the crura.25 Awareness of the anatomical spaces, namely the pleural and retropleural spaces in the thoracic cavity and the peritoneal and retroperitoneal spaces in the abdominal cavity, provide the surgeon with a better understanding of the anticipated approach corridor. Furthermore, the diaphragmatic fibers in the intercostal region of the thoracic ribs T11-T12 amalgamate with the intercostal muscles and, therefore, make it difficult to distinguish a dissection plane. These considerations help with the identification of the extracoelomic plane, which facilitates access to the retropleural, retroperitoneal, or a combination of both of these cavities.25
Surgical Technique
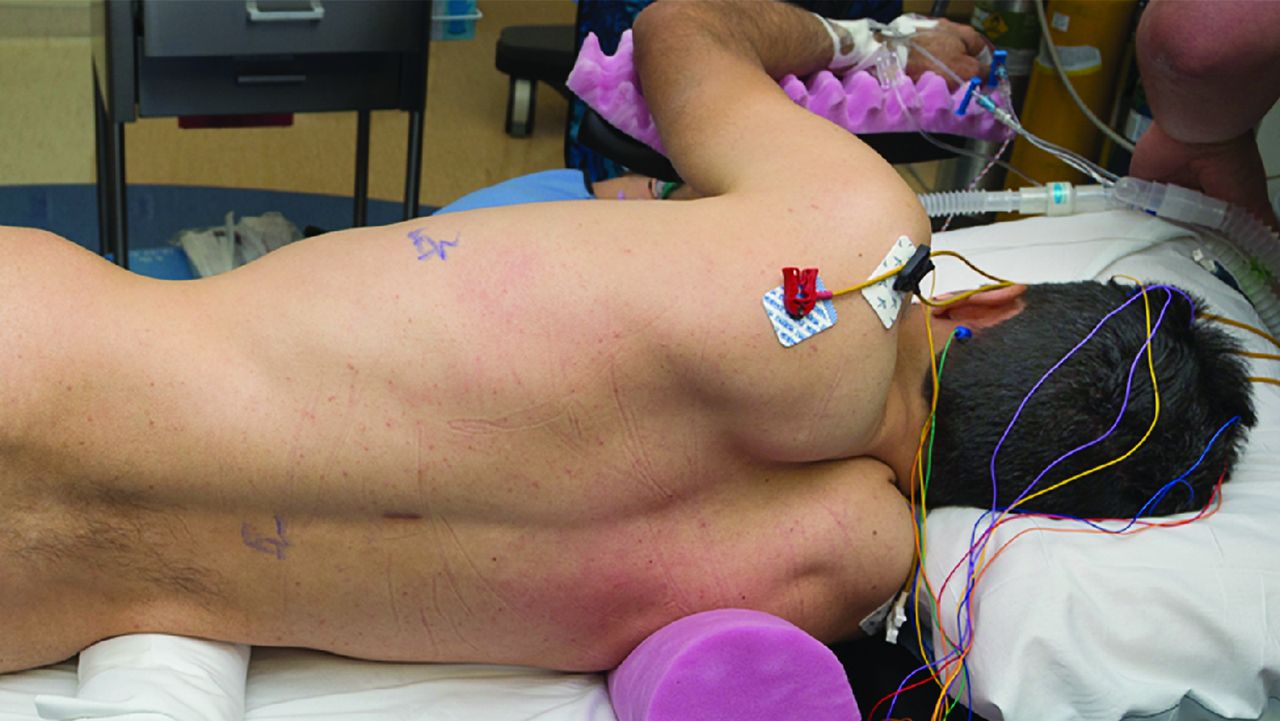
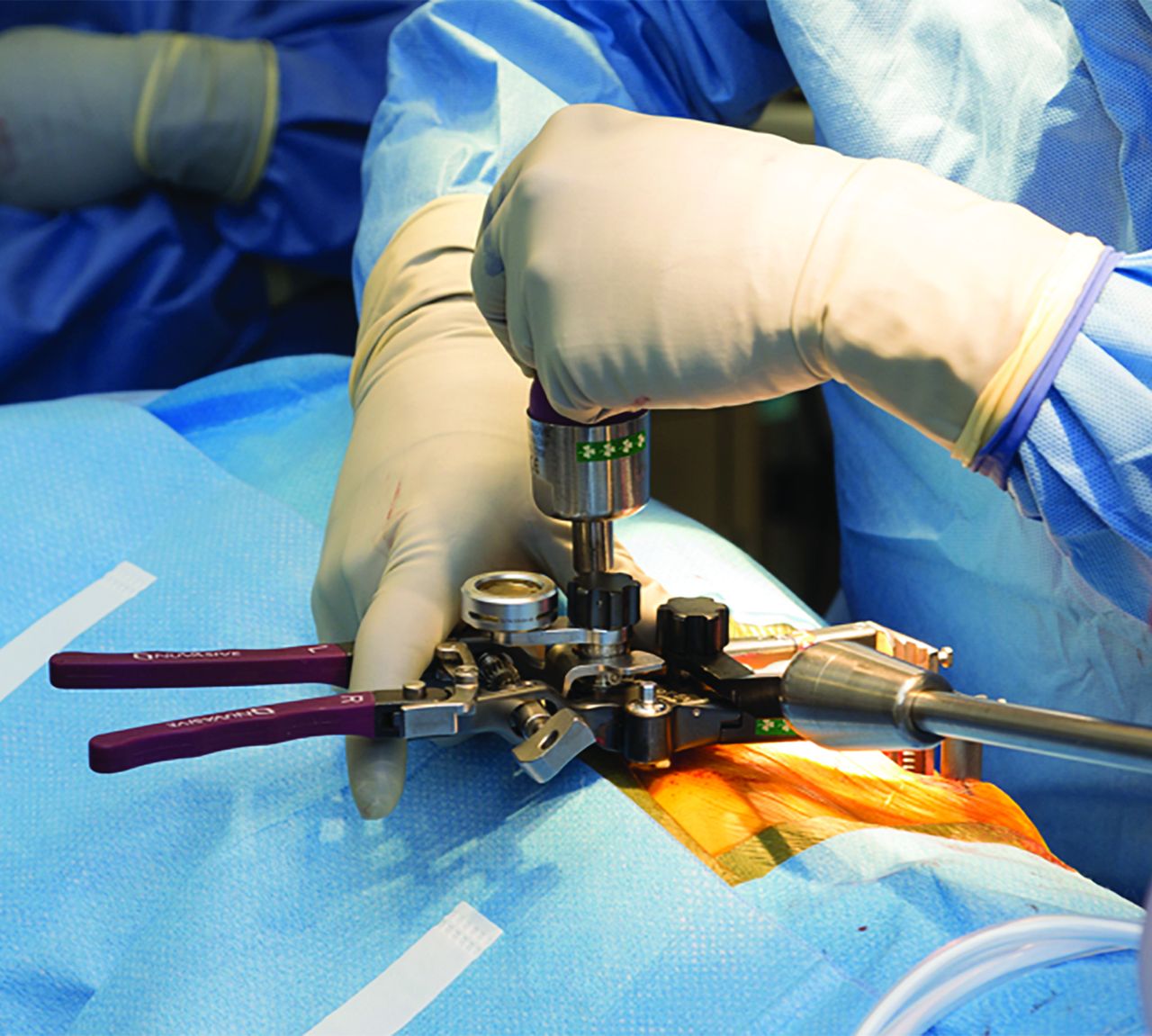
The first step in obtaining access to the thoracolumbar spine via a mini-open lateral approach begins with placing the patient in a standard lateral decubitus position on a surgical table that is flexible and radiolucent, using fluoroscopic guidance (Figure 1). Prior to positioning, we routinely obtain baseline somatosensory evoked potentials and motor evoked potentials and begin electromyography neuromonitoring. Stability of these signals is confirmed after positioning. With the assistance of fluoroscopy, the level of the pathology is localized, and an incision is made parallel to the rib at this level (Figures 2A, B and 3). Dissection is performed, and 5–7 cm of rib is removed and saved for an autograft. The diaphragmatic attachments to the rib are removed, and a finger is utilized to bluntly develop the appropriate plane behind the parietal pleura. Releasing the diaphragm allows this cavity to be connected with the retroperitoneal cavity, in which usual anatomical landmarks, such as the transverse process and psoas muscle, may be palpated. Approaching a lesion below L1 requires a transpsoas approach to be performed in the retroperitoneal cavity. With the assistance of fluoroscopy, a dilator is positioned on the vertebral body. Tubular dilators are then sequentially inserted, and a retractor is placed (Figure 4). If performing a transpsoas approach, standard directional triggered electromyography monitoring should be used to ensure posterior positioning of the lumbar plexus.

The patient is positioned in the lateral decubitus position with an axillary roll underneath the axilla and a towel roll underneath the hip. Used with permission from Barrow Neurological Institute.

(A) After the correct level is identified in the anteroposterior or lateral view, a needle is placed in the spinous process of the surgical level. (B) Using lateral fluoroscopy, the precise anatomy of the thoracic disc level is defined. Used with permission from Barrow Neurological Institute.

The underlying rib is palpated, and a transverse incision is made starting from the posterior edge of the disc space. Used with permission from Barrow Neurological Institute.

The retractor is placed immediately lateral to the disc of interest, and the retractor handles are positioned away from the surgeon. Used with permission from Barrow Neurological Institute.
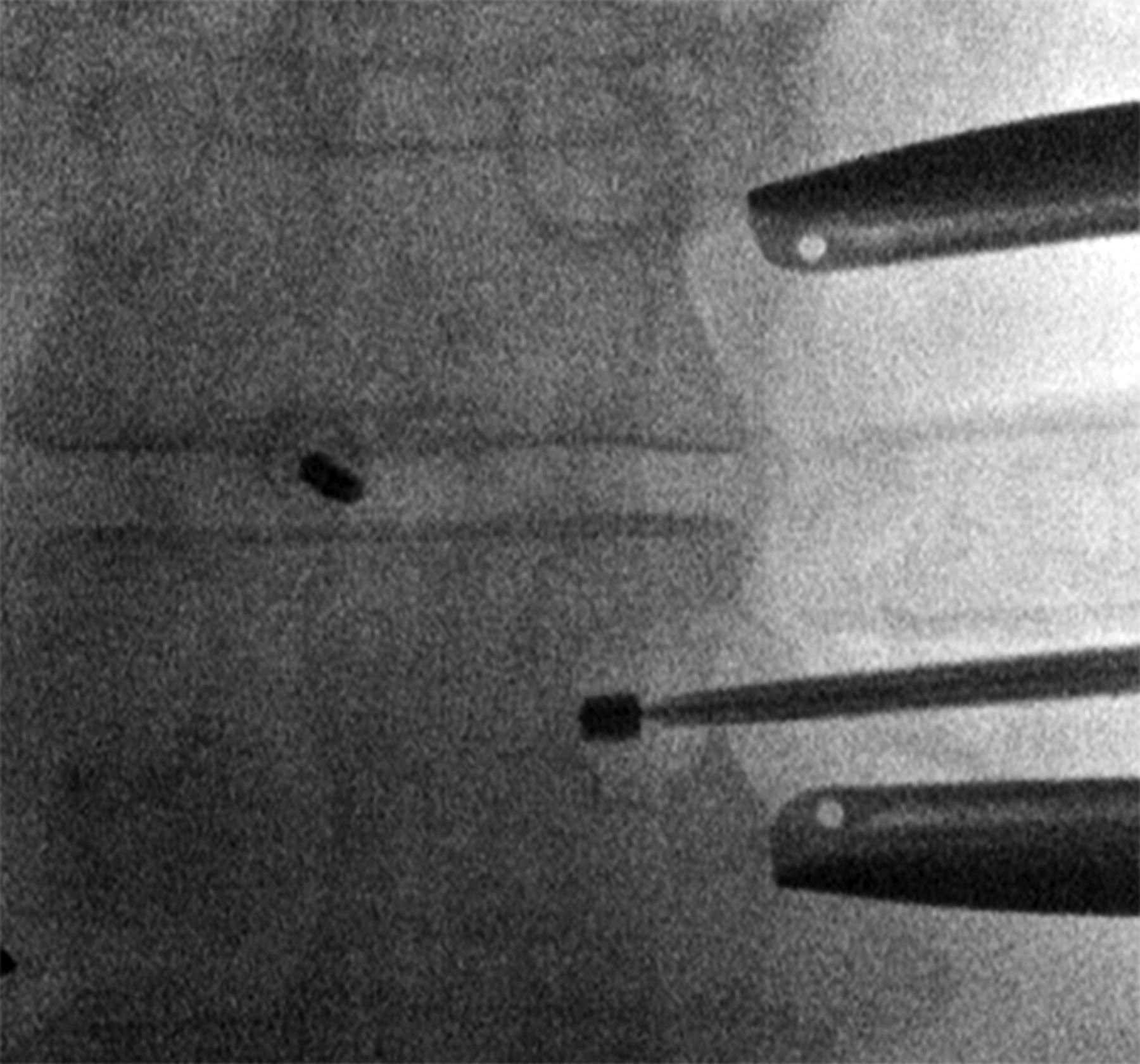
Once appropriate visualization is obtained with the retractor in place, the segmental vessel should be visualized or dissected and cut, if necessary, as it crosses at the level of the midvertebral body. Intraoperative monitoring or adequate visualization, however, should rule out the artery of Adamkiewicz prior to sacrificing the vessel. Specifically, the surgeon can place a temporary clip on the artery in question and assess for any neuromonitoring changes prior to confidently sacrificing the vessel.26 Standard microdiscectomy is performed at the segments above and below the level of pathology. Once these structures are removed, the corpectomy is performed in standard fashion. We prefer using an oscillating ultrasonic drill when feasible (Figure 5). In the case of a neoplasm, the corpectomy may be performed in a piecemeal fashion. Importantly, all movements should be made away from the thecal sac toward the corpectomy cavity. The posterior longitudinal ligament may be exposed and carefully dissected away from the dura. Finding the posterior longitudinal ligament is one way to reliably identify the anterior margin of the spinal canal. If identifying the anterior margin of the spinal canal is found to be challenging, radiography or intraoperative computed tomography may be utilized as well. The posterior longitudinal ligament may be cut and removed, especially in cases where a ventral epidural extension of a pathology causes spinal cord compression, such as in a neoplasm or infectious phlegmon. The anterior longitudinal ligament is also preserved to protect the surrounding structures of the mediastinum and thoracic cavity.

Anteroposterior fluoroscopic images showing drilling of the pedicle. Used with permission from Barrow Neurological Institute.
After the corpectomy is completed and the thecal sac is sufficiently decompressed, interbody fusion is performed. The lower end plate of the rostral vertebral body and the upper end plate of the caudal vertebral body are prepared for arthrodesis with curettes. We typically then place a titanium expandable vertebral body replacement device (cage) filled with morselized allograft and harvested rib autograft. Cage positioning is confirmed with fluoroscopy and sequentially expanded until it is locked into place. A lateral plate may be placed from the rostral to the caudal vertebral body for further fixation. The retractor is then closed and removed slowly while hemostasis is achieved. The incision is then irrigated and closed in a standard layered fashion.
If the pleura is compromised during the case, a means to remove air from the pleural cavity is necessary. This is achieved with placement of a chest tube. To avoid the need for a chest tube, alternatively, one end of a red-rubber catheter can be placed in the pleural space while the other end is placed in sterile saline held below the level of the incision, while a Valsalva maneuver is performed. This technique forces the air in the pleural space out using positive pressure. Once the fascia is closed in an airtight manner and all the air is evacuated, the catheter is pulled while a purse string suture is tied. We do not routinely place chest tubes after the retropleural approach (Figure 6).

Routine postoperative skin closure with a drain left in place; note that no chest tube was placed. Used with permission from Barrow Neurological Institute.
Postoperatively, an immediate and a next-morning chest radiograph are recommended to evaluate for the presence of a pneumothorax. We also recommend admission of these patients to an intensive care unit overnight for close monitoring. Typically, the length of stay for these patients is short, with most discharged on postoperative day 1 or 2.
Contraindications and Complications
As previously mentioned, proper patient selection is key. For thoracic disc herniations, tumors, and infections of the thoracolumbar spine, the key indication for surgery is the presence of spinal cord compression causing myelopathy or severe deformity. Generally, extensive scarring on the lateral thoracic wall and along the retroperitoneal surgical trajectory, in cases of prior surgery, radiation, trauma, and malignancies, can complicate dissection steps, the corpectomy, and the access to the vertebral column. These complications can prolong procedure times and require a wider approach, resulting in the switch to an open approach. Furthermore, lesions above the level of the fifth thoracic vertebra are not accessible from a lateral approach, due to the anatomical constraints caused by the scapula.27 Biomechanically, laterally applied instrumentations are less stable than those that were added from posterior approaches.28 Traumatic injuries frequently cause major damage to the weight-bearing properties of the spine and affect patients of all ages, which can necessitate the most optimal biomechanical instrumentation and approach. However, for patients with metastases, the aim of treatment often revolves around a palliative aim that can be met with the less invasive nature and decreased hospital stays of the lateral approach.29
In their analysis on a retrospective cohort of 80 patients treated through a mini-open lateral approach to the thoracolumbar spine, Baaj et al30 reported a complication rate of 12.5%. The cohort primarily consisted of patients with traumatic (71%) and oncological (26%) disease. Complications showed a wide range without particular outliers, consisting of dural tears, intercostal neuralgia, and deep vein thrombosis (all: n = 2, 2.5%) as well as wound infection, pleural effusion, hardware failure, and hemothorax (all: n = 1, 1.3%).30 Another study of a cohort of 52 patients with traumatic thoracolumbar disease who underwent the same approach reported dural tears, intercostal neuralgia, and deep vein thrombosis in 3.8% as well as pleural effusion and infection rates of 1.9% for both.31 The risk of these complications should be weighed against patient symptomatology.
Outcomes
The lateral retropleural approach had already been used with satisfactory results in the 1990s when McCormick’s analysis of 15 patients with various spinal pathologies as well as Moskovich et al’s comparison to anterior transthoracic approaches in a series of 65 consecutive patients (27 retropleural) were published.32,33 The increased use of minimally invasive techniques and instruments helped minimize the drawbacks of significant approach-associated morbidity and led to a rebirth in retropleural access to the thoracolumbar spine. In their series of 59 patients who underwent minimally invasive lateral corpectomy for traumatic burst fractures, Podet et al found no difference in fusion status at 1-year follow-up compared to an open lateral corpectomy group and a 1.7% revision rate attributable to failure of fusion.26 Significantly shorter mean (SD) operative times (228.3 [27.9] vs 255.6 [34.1] minutes) and time to ambulation (1.8 [1.1] vs 5.0 [0.8] days), however, were observed in the mini-open group. Smith et al found similar results in a cohort of 52 patients with traumatic thoracolumbar disease, with a 13.5% complication rate and 73% of patients reporting either complete neurological recovery or slight residual postoperative deficits.31 Another series of 11 patients with various thoracolumbar pathologies (7 fracture or deformity, 2 neoplasm, and 2 osteomyelitis) reported successful decompression and reconstruction in all patients with mini-open lateral retropleural approaches, with significant improvements in reported back pain and 1 complication (deep vein thrombosis/pulmonary embolism-pneumonia).3 Furthermore, in a series of 23 patients treated for symptomatic thoracic disc herniations, the authors were able to remove all but 2 discs and achieved favorable outcomes without additional neurological deficits in all cases.34 Nurick grades with myelopathy decreased from 3.9 to 2.1 on average, and radicular and axial pain improved significantly (change in visual analog scale from 7.6 to 2.1 and 8.2 to 3.9, respectively).
CONCLUSIONS
The mini-open lateral corpectomy for thoracolumbar pathologies has afforded spine surgeons a new, less invasive, less morbid option for treating what has historically been a challenging surgical location. For surgeons with a comprehensive understanding of the anatomy and technique, we believe this approach can be a safe, successful, and more appealing option for patients with diseases of the thoracolumbar spine.
Acknowledgments
We thank the staff of Neuroscience Publications at Barrow Neurological Institute for assistance with manuscript preparation.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosure JDT receives consulting fees and royalties from NuVasive Medical, Inc, and is a consultant for SeaSpine, Inc, and ATEC Spine, Inc. JSU receives consulting fees and royalties from NuVasive Medical, Inc, and is a consultant for SI-BONE, Inc, and Misonix, Inc.
Ethics Approval No IRB or ethical considerations apply to this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.