


Abstract
Background Context Conventional open lumbar decompression is a widely accepted procedure for degenerative lumbar disease. However, it is associated with morbidity due to damage to the paraspinal muscles and posterior ligamentous complex. Endoscopic spine surgery (ESS) is considered the least invasive type of spine surgery in modern times and was developed to minimize the iatrogenic injury to the paraspinal muscles.
Purpose Many studies are reported to estimate the paraspinal muscle damage after an open or minimal invasive spine surgery by radiological methods (magnetic resonance imaging [MRI] and computed tomography], biochemistry (creatinine phosphokinase level), or electrophysiology (electoneuromyography). The objectives of this study were to assess paraspinal muscles changes after lumbar endoscopic unilateral laminotomy with bilateral decompression (LE-ULBD) based on preoperative and 6-month postoperative MRIs.
Patient Sample We studied 159 consecutive patients with lumbar degenerative disease who underwent LE-ULBD at a spine specialty hospital from 2018 to 2019.
Study Design The current study was a single-center, single-surgeon, retrospective case study.
Outcome Measures Changes of paraspinal muscles after LE-ULBD measured on lumbar MRI.
Methods Postoperative paraspinal muscles changes are evaluated on a picture archiving and communication system by measuring the cross-sectional area (CSA) of multifidus and erector spinae muscles along with the fatty infiltration of muscle on Kjaer’s scale at the level of surgery on the ipsilateral and contralateral sides on T1W image. Correlations between imaging and visual analog scale (VAS) score for back, Oswestry Disability Index (ODI), and MacNab’s criteria were examined in the preoperative and postoperative periods.
Results Of the 159 patients included, 120 underwent a single level procedure and 39 a multilevel procedure. For single-level LE-ULBD group, mean (SD) preoperative, postoperative, and final follow-up VAS score (7.83 [1.37], 3.15 [0.67] and 2.19 [0.88]; P < 0.001) and ODI (74.09 [7.18], 27.88 [4.40], and 23.88 [4.56]; P < 0.001) improved significantly. Based on MacNab’s criteria, the clinical result was excellent in 37 patients, good in 78 patients, and fair in 5 patients. For the multilevel LE-ULBD group, the mean (SD) preoperative, postoperative, and final follow-up VAS score (7.84 [1.38], 3.50 [0.60],and 2.44 [0.79]; P < 0.001) and ODI (74.1 [7.72], 31.30 [4.46], and 24.90 [4.75]; P < 0.001) also improved significantly . Based on MacNab’s criteria, the clinical result was excellent in 6 patients, good in 31 patients, and fair in 2 patients.
The functional CSA of paraspinal muscles for both groups showed no significant difference in the 6-month follow-up MRI. The fatty infiltration of paraspinal muscles significantly improved from 0.77 to 0.59 (P < 0.05) for the single level LE-ULBD group but not for the multilevel LE-ULBD group (P = 0.320). The mean dural sac CSA increased significantly for both groups (P < 0.001).
Conclusion Adequate neural decompression can be achieved with the preservation of paraspinal muscles after an ESS. Preservation of the paraspinal muscles along with the posterior ligamentous complex improves the stability of motion segment in the postoperative period, which ultimately results in better patient outcomes in related to postoperative pain and rehabilitation.
Key
- endoscopic stenosis lumbar decompression
- functional cross section area
- fatty infiltration scale
- multifidus
- erector spinae
INTRODUCTION
The conventional posterior open lumbar decompression is established as the gold standard for the treatment of lumbar spinal canal stenosis. However, it is associated with significant paraspinal muscle damage, atrophy, iatrogenic instability, and chronic low back pain in long-term follow-up.1,2 Posterior decompression can be combined with the fusion procedure with added stability. However, it is also associated with some complications such as adjacent segment disease.3 The approach-related iatrogenic paraspinal muscle injury has raised major concerns to the spine surgeons in recent times due to associated chronic low back pain and spinal instability. Various theories have been proposed for the mechanism of muscle injuries such as thermal injuries, denervation of paraspinal muscles, or prolonged retraction time associated with the decreased capillary perfusion and ischemia. Endoscopic spine surgery (ESS) is considered the least invasive type of spine surgery in modern times developed to minimize the iatrogenic injury to the paraspinal muscles.4 It gives advantages of minimal soft tissue damage and retraction, less intraoperative blood loss, minimal postoperative pain, and instability with early rehabilitation.5 Many studies are reported to estimate the paraspinal muscle damage after an open or minimally invasive spine surgery by radiological method (magnetic resonance imaging [MRI] and computed tomography [CT]), biochemistry (creatinine phosphokinase level), or electrophysiology (EMG).
To the authors’ knowledge, no previous study has attempted to evaluate the paraspinal muscles atrophy after ESS by lumbar endoscopic unilateral laminotomy with bilateral decompression (LE-ULBD). The purpose of this study is to assess the paraspinal muscles after LE-ULBD by the radiological method.
MATERIALS AND METHODS
Patient Sample
This retrospective case study was approved by the institutional review board of Nanoori Hospital, Seoul, Republic of Korea (NR-IRB 2020-011). Informed consent was obtained from all the patients who participated in the study. We studied 159 consecutive patients with lumbar degenerative disease (78 males, 81 females; mean age 63.89 years) who underwent full endoscopic lumbar endoscopy. We randomly selected these 159 patients from the G-power program, out of the total patients queried between March 2018 and February 2019, to eliminate bias. Out of 159 patients, 120 patients underwent a single-level procedure and 39 patients underwent a multilevel procedure (83 levels). All patients who were having symptoms of low back pain with neurological claudication and had failed at least 3 months of conservative treatment were included in the study. Diagnosis of central canal and lateral recess stenosis was confirmed on MRI and CT. Patients who presented with foraminal stenosis, Grade 2 or more spondylolisthesis, and gross segmental instability were excluded from this study. Patients who had previous decompression or fusion surgery were also excluded from the study due to the presence of pre-existing paraspinal atrophy or artifact due to hardware.
Surgical Procedure
The operative side was decided on the basis of clinical symptoms and preoperative planning. The target point was located under fluoroscopy guidance. Longitudinal incision of size 1 cm was taken over the target point located about 1–1.5 cm from the midline on the ipsilateral side at the desired level. Obturator and serial dilators were introduced through the interval between multifidus (MF) muscle adjacent to the spinous process, and finally, a working channel was introduced along with the endoscope. We used a working channel with an outer diameter of 13.7 mm and a beveled tip. The endoscope has a 15° viewing angle, an outer diameter of 10 mm, a working channel diameter of 6 mm, and a working length of 125 mm (ILESSYS-DeltaR, Joimax GmbH, Germany). Bevel tip is docked over lateral bony structures with working cannula facing medially toward the ligamentum flavum. Soft tissue dissection and hemostasis are carried out with the radiofrequency ablator. Soft tissue and superficial layer of the ligamentum flavum were removed with endoscopic forceps. Bone drilling started at the medial border of the ipsilateral facet joint in a caudal to cranial direction and from deeper to superficial plane up to the spino-laminar junction of cranial vertebra until we observed the free margins of the deep layer of the ligamentum flavum. We prefer to use a 3.5-mm diamond tip endoscopic drill (Primado, NSK, Japan). If required, the base of spinous process along with the undersurface of the contralateral lamina and lateral recess was decompressed (contralateral approach). All the bony procedure was done outside the deep layer of the ligamentum flavum so that neural structures were protected by it throughout the procedure. Finally, the deep layer of the ligamentum flavum was elevated from its sublaminar attachment with the endoscopic dissector and the ligamentum flavum was resected in “en block” fashion with the help of Kerrison’s punch and forceps. The authors called it the “out and in” technique of interlaminar approach.
Outcome Evaluation
Clinical Evaluation
Demographic data such as age, sex, level(s) of surgery, body mass index, bone mineral density, and comorbidity index were collected. All patients were clinically evaluated on the basis of the visual analog scale (VAS) score for the back, Oswestry Disability Index (ODI),and MacNab’s criteria preoperatively, postoperatively, and final follow-up (minimum 6 months). Patients were also assessed for any intraoperative or postoperative complications and recurrence of symptoms.
Adiological Evaluation
A lumbar MRI was performed at preoperative, postoperative day 1, 6-month follow-up, and 1-year follow-up using a GE Signa1.5T HDxT MRI Machine (GE Healthcare, Milwaukee, WI, USA). MRI was performed with the patient in supine position with pillow support under the lumbar spine. The images were obtained using fast spin-echo sequence with a bandwidth of 25 Hz, a slice thickness of 3 mm, and a slice gap of 0.5 mm. All the measurements were taken on T1-weighted axial images parallel to the disc space at the level of surgery using an INFINITT PACS M6 Version (INFINITT Healthcare Corporation, Seoul, Republic of Korea). The radiological measurement was performed by an independent observer (clinical spine fellow), who was blinded to the objectives and outcome of the study.
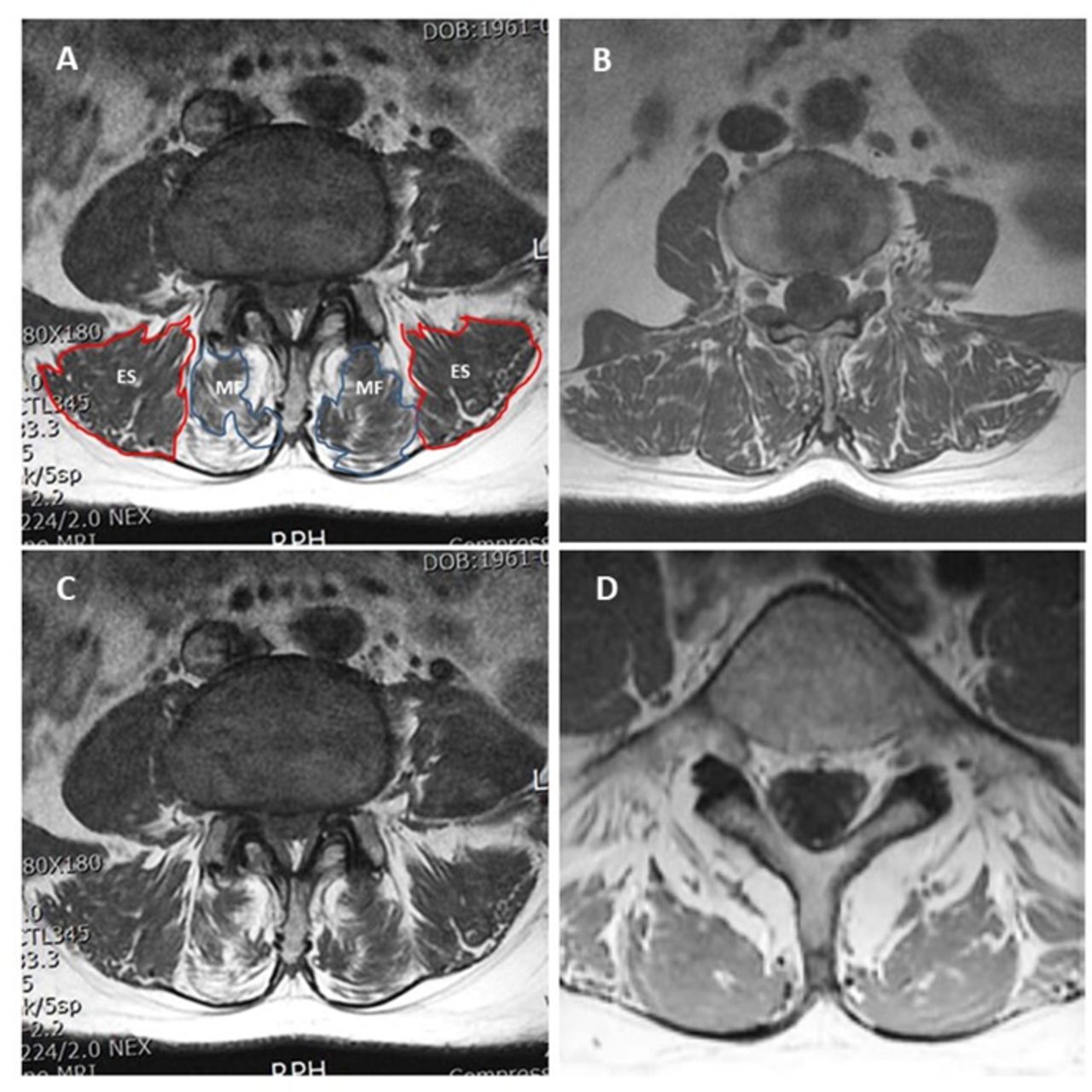
Functional cross-sectional area (FCSA) of paraspinal muscles was measured at the desired level using T1-weighted axial images with cut at mid-discal level parallel to the endplate by drawing region of interest around MF and erector spinae (ES) muscle avoiding adjacent fat, bony osteophytes, and soft tissue. We measured on both ipsilateral and contralateral sides and compared in both preoperative and postoperative periods.
Qualitatively paraspinal muscle atrophy was assessed on T1-weighted axial images on fatty infiltration scale (Kjaer’s scale) from 0 to 2. Grade 0: normal fat content of muscle <10%, grade 1: slight fatty infiltration of muscles 10% to 50% and grade 2: severe fatty infiltration of muscles >50%.6
Dural sac cross-sectional area was measured to evaluate the adequacy of decompression preoperatively and postoperatively (Figure 1).
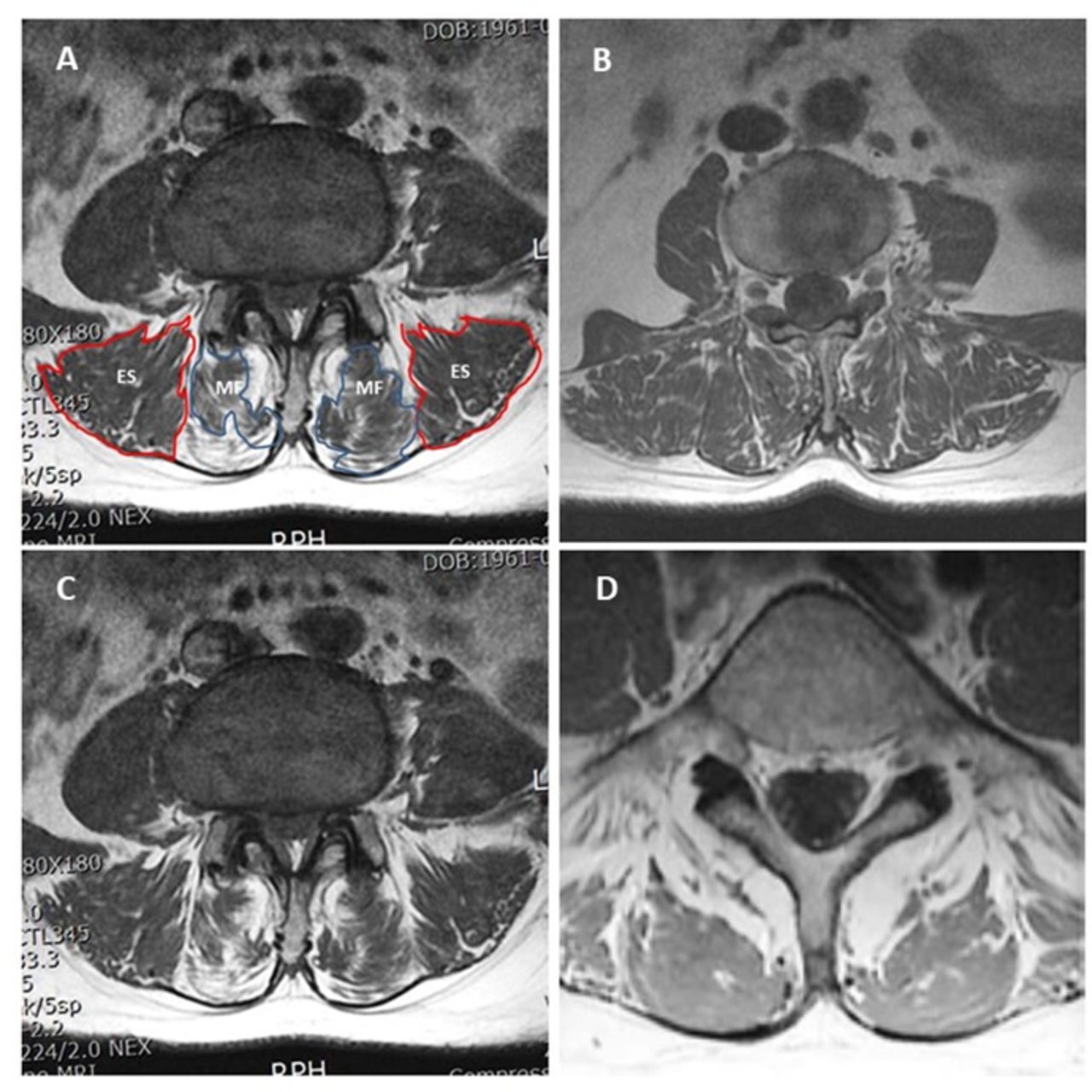
(A) Measurement of functional cross-sectional area of erector spinae outlined with red line and multifidus outlined with blue line on T1 axial magnetic resonance imaging images. Fatty infiltration scale: (B) grade 0 ( 10%); (C) grade 1 (10%–50%); and (D) grade 2 (>50%).
Statistical Analysis
Clinical data were analyzed with SPSS version 18 statistical analysis software (IBM Corporation, New York, USA). The continuous variables were expressed as mean ± SD. The paired t test was used for comparison of preoperative and postoperative values. A value of P < 0.001 considered significant.
RESULTS
Clinical Outcomes
All patients were followed up for 6 months to 2 years with a mean follow-up period of 15.5 months.
For the single-level LE-ULBD group, the mean (SD) preoperative, postoperative, and final follow-up VAS score (7.83 [1.37], 3.15 [0.67], and 2.19 [0.88]; P < 0.001) and ODI 74.09 ± 7.18/27.88 ± 4.40/23.88 ± 4.56(P < 0.001) were improved significantly. Based on MacNab’s criteria, the clinical result was excellent in 37 patients, good in 78 patients, and fair in 5 patients.
For the multilevel LE-ULBD group, the mean preoperative, postoperative, and final follow-up VAS score (7.84 [1.38], 3.50 [0.60], and 2.44 [0.79]; P < 0.001) and ODI (74.1 [7.72], 31.30 [4.46], and 24.90 [4.75]; P < 0.001) also improved singificantly. Based on MacNab’s criteria, the clinical result was excellent in 6 patients, good in 31 patients, and fair in 2 patients (Table 1).
Demographical data and clinical results of single-level and multilevel ESLD.
Radiological Outcomes
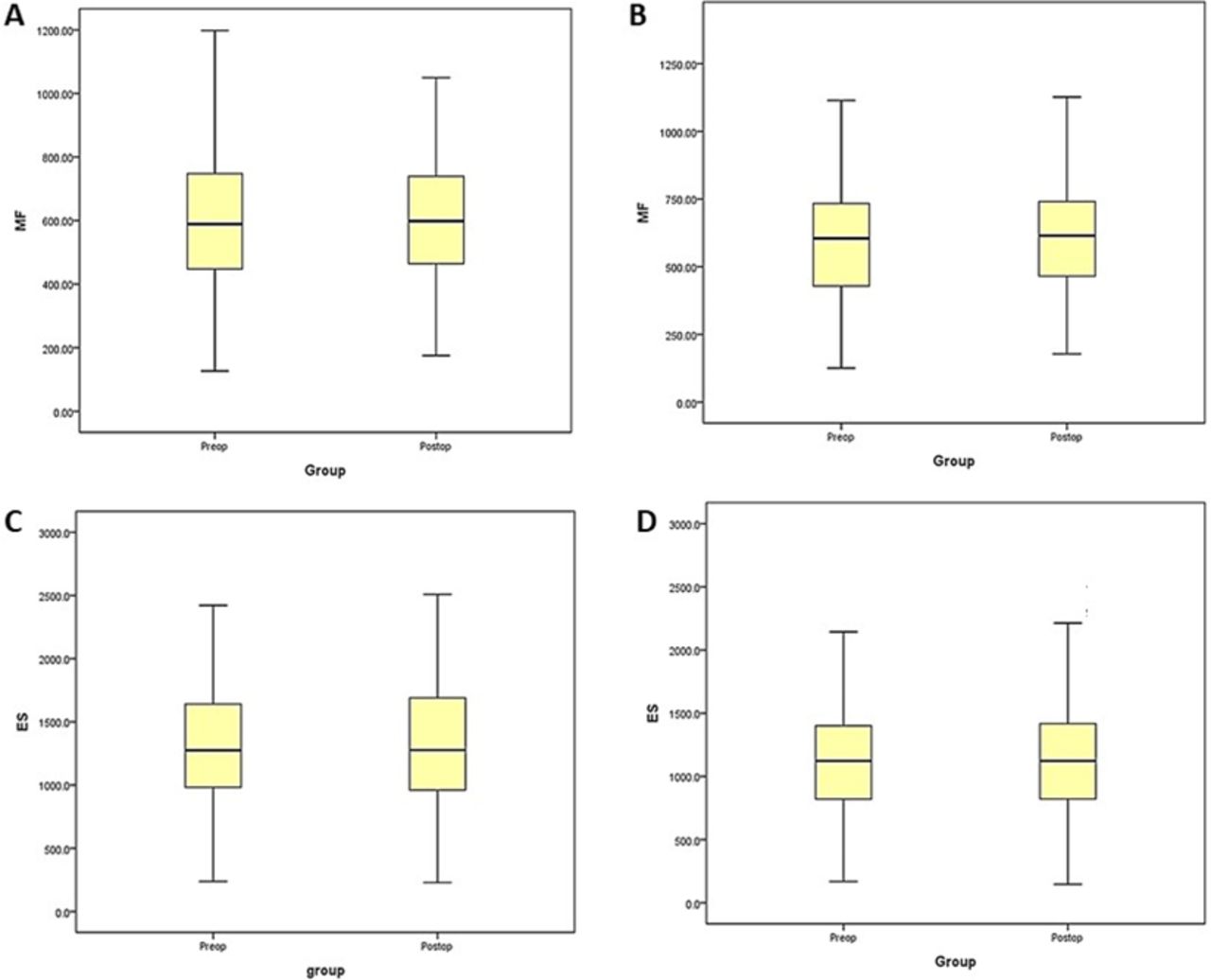
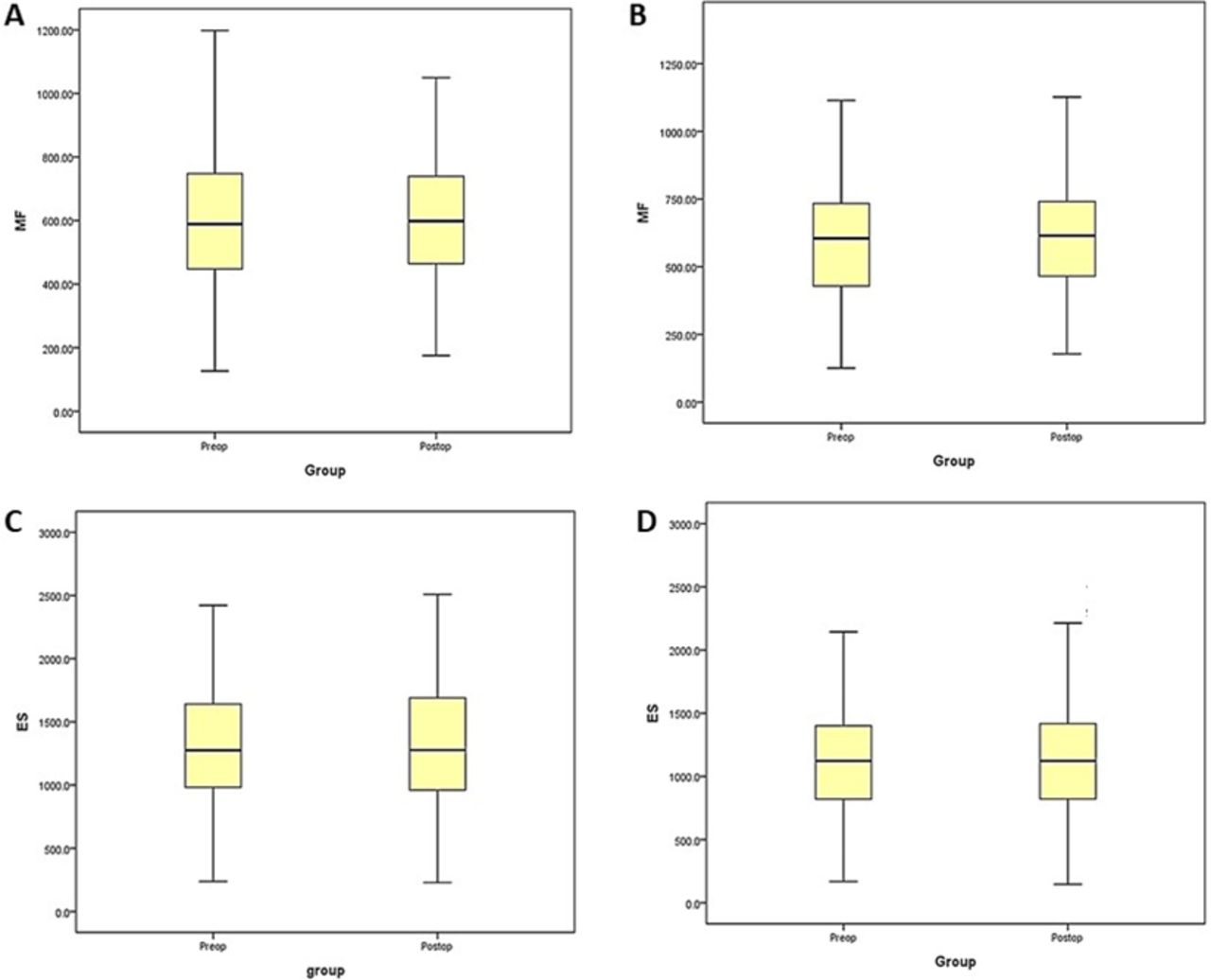
The FCSA of MF for the single-level group (n = 120) showed no significant difference on 6-month follow-up MRI on the ipsilateral side (+1.83% increase in FCSA; P = 0.112) or contralateral side (+2.23% increase in FCSA; P = 0.066). The FCSA of ES showed no difference on ipsilateral side (+6.95 % increase in FCSA; P = 0.123) or contralateral side (+0.56% increase in FCSA; P = 0.621). The mean dural sac CSA increased significantly from 79.23 ± 36.50 to 163.97 ± 78.29 mm2 (P < 0.001) (Figure 2).

Box plot with interquartile range and median value showing for the single-level lumbar endoscopic unilateral laminotomy with bilateral decompression preoperative and 6-month follow-up changes in functional cross-sectional area of (A) ipsilateral multifidus (MF), (B) contralateral MF, (C) ipsilateral erector spinae (ES), and (D) contralateral ES.
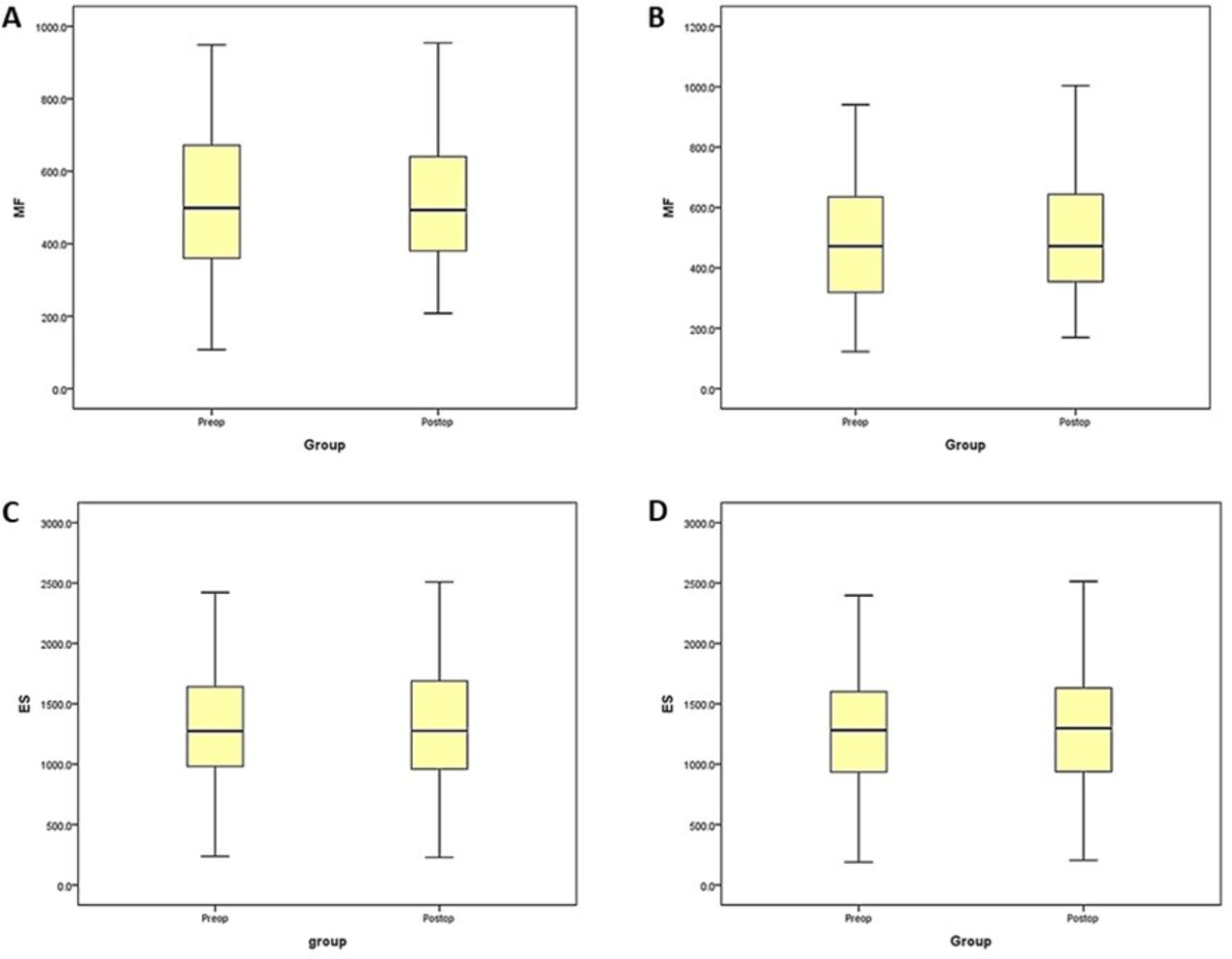
For the multilevel LE-ULBD group (n = 83), FCSA of MF showed no significant difference on 6-month follow-up MRI on the ipsilateral side (+1.38% increase in FCSA; P = 0.458) or the contralateral side (+1.72% increase in FCSA; P = 0.344). The FCSA of ES showed no difference on the ipsilateral side (+1.21% increase in FCSA; P = 0.432) or contralateral side (+1.53% increase in FCSA; P = 0.311). The fatty infiltration of paraspinal muscles changed from 0.67 to 0.65 (P = 0.320). The mean dural sac CSA improved significantly from 69.83 ± 26.78 to 157.81 ± 48.67 mm2 (P < 0.001) (Figure 3).
Box plot with interquartile range and median value showing for the multilevel lumbar endoscopic unilateral laminotomy with bilateral decompression preoperative and 6-month follow-up changes in functional cross-sectional area of (A) ipsilateral multifidus (MF), (B) contralateral MF, (C) ipsilateral erector spinae (ES), and (D) contralateral ES.
The fatty infiltration of paraspinal muscles significantly changed for single-level LE-ULBD; on Kjaer’s scale grade 0 from 47 to 62, grade 1 from 51 to 42, and grade 2 from 22 to 14. However, fatty infiltration on Kjaer’s scale remained unchanged in the postoperative period for multilevel LE-ULBD (Table 2).
Radiological results of single-level and multilevel ESLD.
Recurrence and Complications
We recorded intraoperative complications in the form of dural tear in five patients; it was managed intraoperatively by patch blocking dural repair technique with Tachosil. Clinically, all the patients improved without any sequel such as pseudomenigocele or cerebrospinal fluid leak in long-term follow-up. One patient who experienced canal restenosis was managed with revision LE-ULBD. Aggravation of instability was seen in 3 cases that were eventually managed with endoscopic transforaminal interbody fusion.
DISCUSSION
The conventional posterior open lumbar decompression is the gold standard treatment for the treatment of lumbar spinal canal stenosis. However, it is associated with significant intraoperative blood loss, soft tissue dissection, extensive paraspinal muscle stripping from the spinous process, and iatrogenic instability. Punjabi et al7,8 had proposed the theory of spinal stability, which consists of 3 functionally interdependent subsystems; static subsystem was formed by the posterior osseo-ligamentous complex; dynamic subsystem was formed by the paraspinal muscles and tendons; and neural is formed by the transducers located in the paraspinal muscles and the control centers. The posterior midline approach causes damage to all these subsystems and results in a decrease in trunk muscle strength, iatrogenic instability, and chronic low back pain in long-term follow-up, which is also called “failed back surgery syndrome.”9 MF is the most commonly affected paraspinal muscle in the posterior midline approach. It is supplied by the medial branch of the dorsal ramus and lacks intersegmental nerve supply compared to other paraspinal muscles.10 It makes the MF more vulnerable to go into atrophy. Many studies have been proposed to signify the importance of MF muscle in the spinal stability.11 Wilke et al12 evaluated the effect of paraspinal muscle stiffness on the motion segment stability and proposed MF responsible for two-third of the stiffness of the motion segment. Injury or denervation of MF is responsible for the long-term effect on the spinal stability and chronic low back pain. However, Remes et al13 reported that anterior interbody fusion procedures are also associated with the paraspinal muscles atrophy suggesting that loss of motion affects the paraspinal muscles activity irrespective of the surgical approach. Hence, motion preservation plays an important role in the maintenance of paraspinal muscle integrity. The purpose of this study was to determine whether LE-ULBD is associated with significant paraspinal muscles atrophy.
Kawaguchi et al14,15 demonstrated paraspinal muscle injury during the posterior spine surgery related to operative time and retraction pressure. Gejo et al16 also reported that prolonged retraction time was associated with decreased capillary perfusion and ischemic damage to the paraspinal muscles. In order to overcome this problem, Foley et al17 developed a minimal invasive approach through the internervous plane between MF and ES muscles. Fixed tubular retractors of 20 to 30 mm are used to do bilateral decompression. However, tubular retractors are fixed and impose difficulty for contralateral decompression. Drawbacks of the tubular retractor can be overcome by the endoscopic stenosis decompression (LE-ULBD), where the endoscope is freely mobile and can reach every corner of the spinal canal with simple tilting and rotating maneuver, which avoids sustained pressure on the paraspinal muscles.18 The underwater dissection improves the visualization of the surgical field as well as provides the biological medium for the soft tissue, which minimizes the ischemic damage to the same. Adequate central canal as well as lateral recess decompression can be done by LE-ULBD with maximum preservation of facet joint on both sides.19–21 Preservation of the facet joint and paraspinal muscles maintains the integrity of the motion segments responsible for the early postoperative recovery and rehabilitation.
Many studies have attempted to evaluate the postoperative damage or atrophy of paraspinal muscles by the radiological method (MRI and CT scan),6,22–24 biochemistry (creatinine phosphokinase level),25 or electrophysiology (EMG).26 Hu et al24 highlighted that the measurement of FCSA is a reliable method for the assessment of postoperative paraspinal muscle atrophy. Kjaer et al established the association of fatty infiltration of MF muscle with paraspinal muscle atrophy and chronic low back pain.
Our present study found that FCSA of paraspinal muscles (MF and ES) for both sides did not change significantly for single level (+1.83% MF ipsilateral, +2.23% MF contralateral, +6.95% ES ipsilateral, and +0.56% ES contralateral). For multilevel LE-ULBD, the FCSA remained unchanged (+1.38%, +1.72%, +1.21%, and +1.53%). One of the reasons for an increase in the CSA of paraspinal muscles might be persistence of postoperative muscle edema for more than 6 months. We have observed high T2 signal intensity in few patients; however, the T2 ratio will give a more precise measurement of postoperative muscle edema. Improvement in the fatty infiltration of paraspinal muscles may be another reason for an increase in the FCSA. We had experienced a significant decrease in the fatty infiltration of paraspinal muscles for the single-level LE-ULBD. We felt that the regeneration of the nerve supply (medial branch of dorsal ramus) to the MF after single-level decompression may be the reason for the improvement of an MF atrophy (Figure 4). However, we have not observed significant improvement in the fatty infiltration of paraspinal muscles for the multilevel LE-ULBD. As the Kjaer’s scale is the subjective parameter the potential bias cannot be ruled out. However, it can be overcome by using the digital image analysis with pseudocoloring technique.

Saggital and axial T2-weighted images of a 56-year-old female patient operated for single-level lumbar endoscopic unilateral laminotomy with bilateral decompression L4-5 showing significant increase and maintenance of dural sac cross-sectional area for long-term follow-up without post-operative paraspinal muscle atrophy.
As this study is a retrospective nonrandomized single-center case study, selection bias cannot be ruled out. As radiological evaluation was performed by a single observer (H.D.R.), observer bias is a factor for consideration. Comparative studies with an open decompression or fusion surgery would provide a better understanding of the effect of these surgeries on paraspinal musculature in the future.
CONCLUSION
Patients who had undergone LE-ULBD achieved significant decompression of the dural sac while maintaining significantly less fatty infiltration and no further atrophy of MF muscle after surgery. Preservation of the paraspinal muscles along with the posterior ligamentous complex improved the stability of motion segment in the postoperative period, which ultimately results in better patient outcome in the form of postoperative pain and rehabilitation in our cohort of patients.
Footnotes
Funding This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests The authors report no conflicts of interest or financial disclosures with respect to the research, authorship, and/or publication of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.