


Abstract
Background Adjacent segment disease (ASD) above a previous posterior lumbar instrumented fusion can be managed with minimally invasive lateral lumbar interbody fusion. Earlier procedures with stand-alone lateral cages risked nonunion, and lateral cages with separate lateral plates risked lumbar plexus injury and vertebral fracture. We investigated clinical and radiographic outcomes of an expandable lateral titanium interbody cage with an integrated lateral fixation (eLLIFp) device as a stand-alone treatment for symptomatic ASD above a previous posterior lumbar fusion and performed a comparative cost analysis of eLLIFp to alternative operations for ASD.
Methods In this prospective, observational study, patients with ASD above 1-, 2-, 3-, or 4-level instrumented posterior fusions underwent surgery with lateral expandable titanium cage(s) with an integrated lateral plate with single screws into each adjacent vertebra from August 2017 to August 2019. Multimodality intraoperative neural monitoring was performed. Patient-reported outcomes, computed tomography outcomes, and total costs were analyzed.
Results A total of 33 patients received 35 eLLIFp cages. All clinical outcomes improved significantly. The eLLIFp cages added 2.2° segmental lordosis and 2.7 mm posterior disc height. Interbody fusion rate was 94% at 12 months. There were 2 neurologic complications (6%): 1 patient reported transient anterior thigh numbness and 1 had mild persistent L4 radiculopathy. No cage subsidence, cage migration, screw loosening, or vertebral fracture occurred. No revision lateral surgery, posterior decompression, or supplemental posterior fixation was required. The total eLLIFp cost (AU$19,715) was lower than the cost for all other procedures.
Conclusions eLLIFp provided a minimally invasive, low morbidity, cost-effective, and robust alternative to traditional posterior construct extension surgery for rostral lumbar ASD in selected patients with 1- to 2-level stenosis and minimal deformity.
Clinical Relevance Traditional ASD treatment involves substantial risks and expense. eLLIFp should be considered a safe, effective, and lower cost alternative to posterior construct extension surgery.
Level of Evidence 2.
Introduction
Radiologic degeneration of the disc space adjacent to a previous posterior lumbar instrumented fusion is becoming more common, as more patients undergo lumbar fusion surgery and as life expectancy increases.1 Symptomatic adjacent segment disease (ASD) above a prior posterior lumbar fusion requiring further surgery occurs in 9% to 22% of patients 5 to 10 years later.2,3 Traditional ASD management involves posterior extension of the construct, which is accompanied by substantial risks of infection, major blood loss, cerebrospinal fluid leak, neural injury, and prolonged surgical duration.4
An alternative treatment option is minimally invasive surgery (MIS) lateral lumbar interbody fusion (LLIF), which is a reliable technique for degenerative disc disease, canal stenosis, foraminal stenosis, and spinal deformity5,6 and a good option for rostral ASD.4,7 Stand-alone lateral cages are indicated in the absence of instability, deformity, or reduced bone density8,9 but increase the risk of nonunion; hence, supplemental fixation is recommended.4 Coronal vertebral body fractures have occurred in patients with osteoporosis using a separate lateral plate and unilateral pedicle screws10 and in patients without osteoporosis using 1- and 2-level separate lateral plates.11 Recent studies reported improved segmental lordosis (SL) and restoration of disc height with less subsidence utilizing expandable lateral cages compared with impacted static lateral cages.12–14 Expandable cages with lateral fixation significantly improved segmental stability and prevented anterior cage dislodgment.15 Early experience using these expandable lateral titanium interbody cages with integrated lateral plate fixation (eLLIFp) found the device to be robust and not require supplemental posterior pedicle screw-rod fixation.
To our knowledge, no clinical study has heretofore assessed the eLLIFp device as a stand-alone treatment for ASD. In this study, we investigated clinical and radiographic outcomes of eLLIFp alone for symptomatic ASD above a previous posterior instrumented fusion.
Methods
This prospective observational cohort study included 33 consecutive patients with ASD above a previous posterior instrumented fusion. Patients were evaluated with dynamic (flexion, extension, and lateral bending) radiography, computed tomography (CT) coregistered with isotope bone scans, magnetic resonance imaging, and bone mineral density (DEXA) scans. All patients underwent subsequent MIS LLIF ASD surgery at 1 to 2 contiguous level(s) by a single surgeon from August 2017 to August 2019 via eLLIFp using the ELSA device (Globus Medical Inc., Audubon, PA). Patients were followed for more than 12 months. Radiographic and clinical outcomes were assessed preoperatively and at 2 days, 6 weeks, 6 months, 12 months, 18 months, and 24 months postoperatively. Our institutional ethics committee approved this study. All patients provided written informed consent.
Inclusion and Exclusion Criteria
Inclusion criteria were age between 18 and 80 years; presence of ASD at 1 or 2 levels above a previous posterior lumbar fusion (posterolateral instrumented fusion [PLF] or posterior lumbar interbody fusion [PLIF]); degenerative disc disease, grade 1 degenerative spondylolisthesis, mild or moderate canal stenosis, foraminal stenosis, or facet arthropathy at the ASD level(s); and willingness to attend all follow-up visits.
Patients were excluded if they had 3-level ASD, body mass index (BMI) greater than 40 kg/m2, pars defect, isthmic spondylolisthesis, coronal or sagittal deformity,16 grade 2 or more degenerative spondylolisthesis, moderately severe or severe canal stenosis, bony lateral recess stenosis, osteoporosis (femoral neck T score of −2.5 or less),8 unfavorable psoas muscle anatomy,17 previous complex/extensive retroperitoneal surgery, or prior abdominal/pelvic radiotherapy.
Patient and Treatment Characteristics
Medical records were reviewed to obtain baseline patient information. We also collected treatment information.
Surgery
LLIF was performed under anteroposterior and lateral fluoroscopy. The lateral border of the target disc space was approached via a 90° off-midline retroperitoneal incision and passage through the psoas. Sequential muscle-splitting dilators were inserted under neural monitoring to identify branches of the lumbar plexus and ensure the retractors were placed anterior to the nerves. The tubular retractor was anchored with an intradiscal shim in the posterior one-third of the disc, then opened to a diameter of 22 mm. A Cobb elevator was inserted around the disc to release the contralateral lateral ligament, discectomy was performed, and endplates were prepared using curettes and rasps. Trial cages were inserted to determine the required lateral cage length. The retractor was then opened to 25 mm. The device was inserted at an initial height of 8 mm, then expanded using the lateral torque-limiting driver (Globus Medical Inc.) to obtain a snug fit. Fluoroscopy-guided holes were then made through the integrated lateral plate for fixation using a drill rather than an awl. The superior screw length was usually the same length or 10 mm shorter than the eLLIFp cage length. The inferior screw length was often dictated by the position of the in situ contralateral upper instrumented vertebra pedicle screw. Each screw head was secured to prevent movement. Psoas retraction durations were recorded. The retractor was then released to permit cage backfill with graft and coverage of the ipsilateral cage and exposed psoas muscle with absorbable hemostatic agent (SURGICEL; Ethicon, Inc., Somerville, NJ). The retractor and shim were carefully removed under direct vision.
Interbody Cages and Graft Material
All patients received an eLLIFp device with screws inserted into each adjacent vertebra. The lordosis options were a fixed 6° lordosis at L1-L2 and L2-L3 or an adjustable 5° to 20° lordosis at L3-L4 and L4-L5, permitting customized segmental height and lordosis.
The eLLIFp cages for patients 1 to 28 were filled with recombinant human bone morphogenic protein-2 (BMP) (1.5 mg/mL) applied to an absorbable collagen sponge (Infuse; Medtronic, Inc., Memphis, TN, USA), which was trimmed to the cage volume. The Infuse dose used per level was volume-dependent (ie, the internal cage volume equaled BMP volume in cc). A small kit of BMP (2.8 cc providing a 4.2 mg dose) was used as per the manufacturer’s recommendation following a 1-hour absorption into the carrier period.18 No Infuse was placed outside the cage. The cages for patients 29 to 33 were filled with corticocancellous fibers (Device Technologies, Inc., Belrose, NSW, Australia) because of regulatory withdrawal of Infuse. After cage expansion, all cages were backfilled with granules of synthetic hydroxyapatite bone substitute in an amorphous silica gel (NanoBone; Artoss, Inc., St. Cloud, MN).
Neural Monitoring
All patients underwent multimodal intraoperative neural monitoring (IONM) with transcranial motor evoked potentials, somatosensory evoked potentials, electromyography (EMG), and triggered EMG.
Complications
Complications were identified during hospitalization and after discharge. Perioperative complications were classified as minor (anterior thigh sensory changes or psoas muscle approach-related pain) or major (lumbar radiculopathy, femoral neuropathy, bowel injury, or major vascular injury), as per previous LLIF studies.19
Clinical Outcomes
Preoperative and postoperative assessments of patient-reported outcome measures included back and leg pain (visual analog scale), disability (Oswestry Disability Index), and quality of life (Short Form 12 physical component score and mental component score).
Radiographic Quantitative Measurements
SL was measured as the angle between the cranial endplate of the superior vertebra and the cranial endplate of the inferior vertebra. Lumbar lordosis (LL) was measured as the angle between the cranial endplate of the L1 vertebra and the cranial endplate of the S1 vertebra. Posterior disc height (PDH) was measured between the posterior vertebral margins of the caudal and cranial endplates adjacent to the disc.8 Lordosis and PDH were measured on CT images preoperatively, postoperatively, and at the time of interbody fusion. All measurements were obtained digitally using Inteleviewer software (Interad Medical Systems Inc., Quebec, Canada).
Interbody Fusion
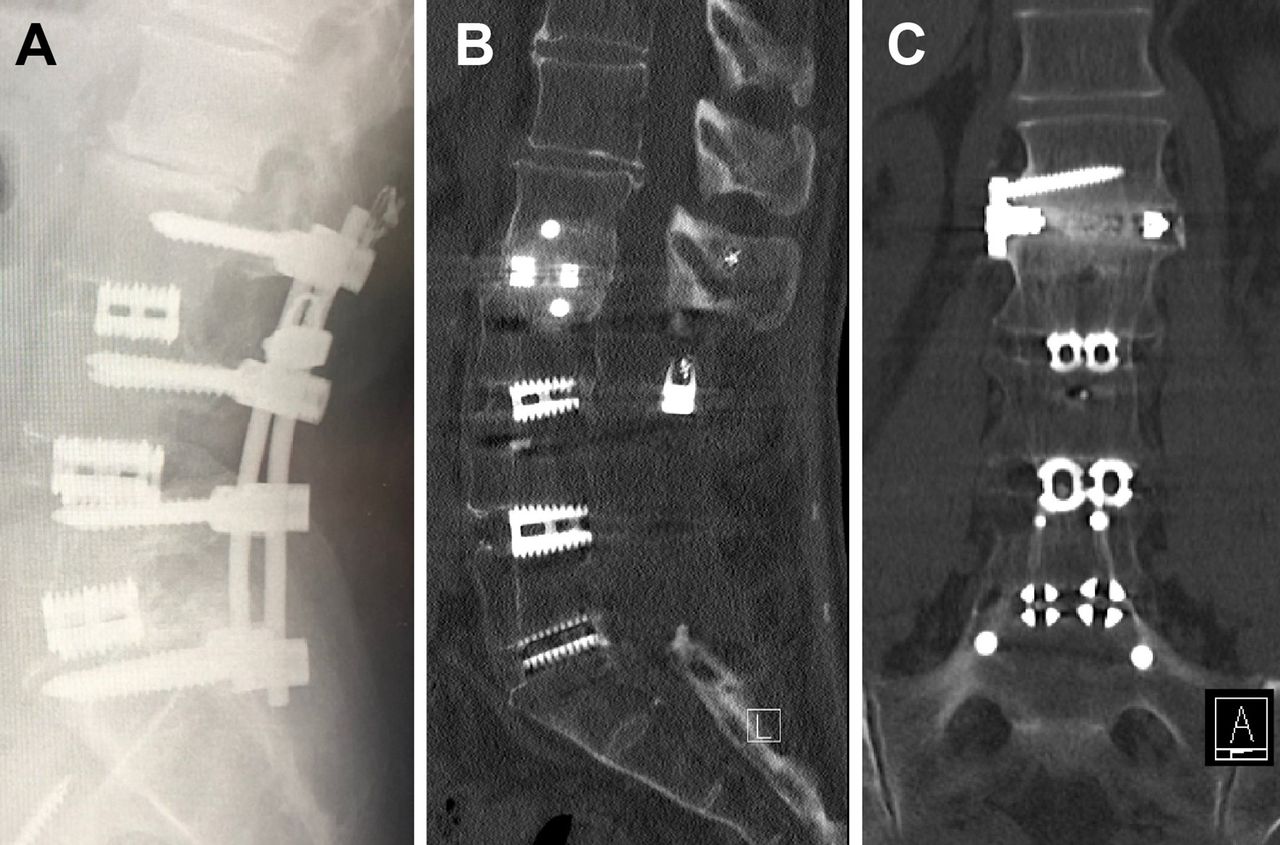
High-definition, low-dose CT images (Somatom Definition Flash; Siemens AG, Erlangen, Germany) were obtained preoperatively and 2 days postoperatively to assess cage and plate-screw position and at 6 and 12 months until solid interbody fusion was confirmed on coronal and sagittal views. All postoperative scans focused on the operative level alone.20 To reduce radiation exposure, no scans were performed after confirming interbody fusion. Fusion was defined as bridging interbody trabecular bone on coronal and sagittal views21 (Figure 1). An independent radiologist interpreted CT results.
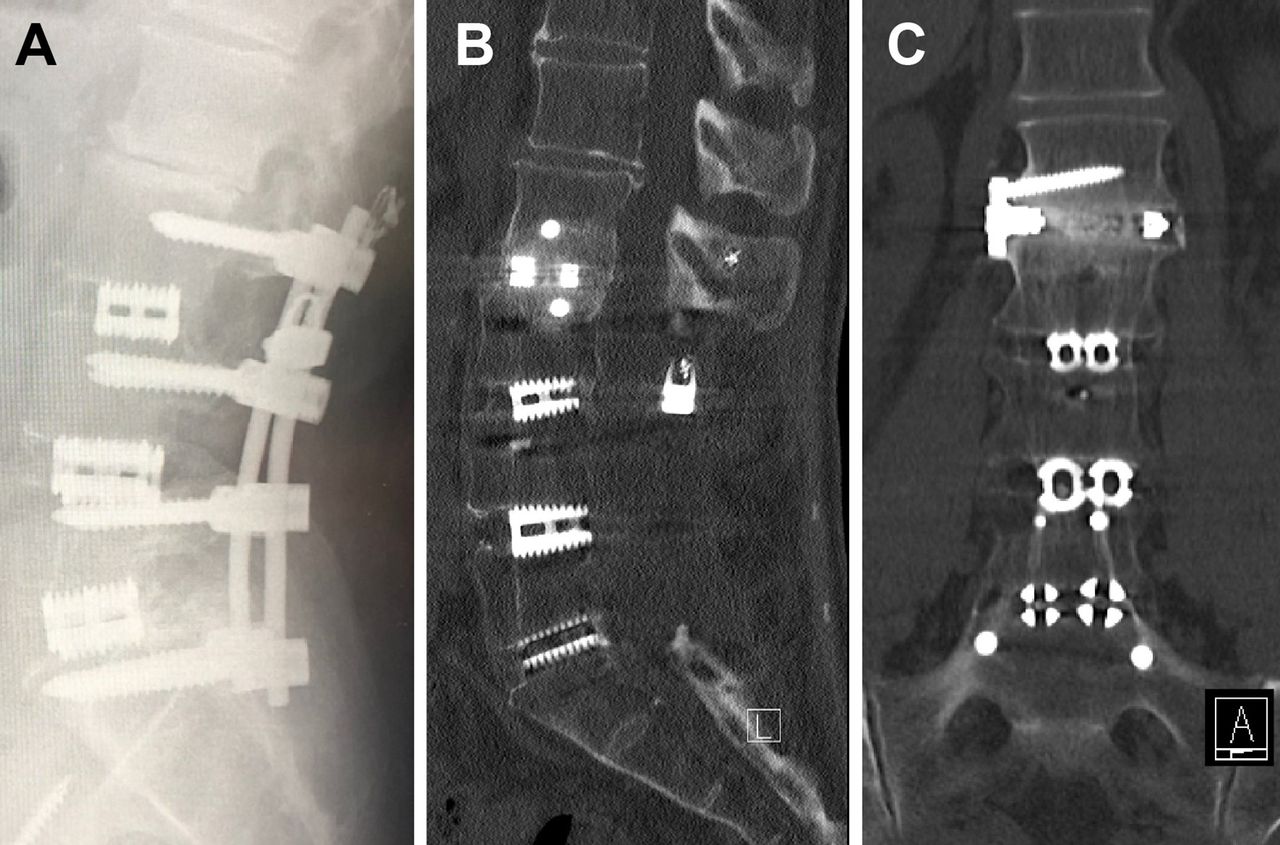
(A) L2-L3 adjacent segment disease above a previous L3-S1 posterior lumbar interbody fusion on a lateral radiograph. The expandable lateral titanium interbody cage with an integrated lateral fixation at the L2-L3 level with solid interbody fusion at 12 months noted on computed tomography. (B) Sagittal and (C) coronal views.
Subsidence
Subsidence was measured radiographically from the vertebral endplate to the caudal or cranial margin of each cage. Subsidence was deemed early cage subsidence (ECS) if evident on postoperative day 2 CT images and was therefore secondary to intraoperative vertebral endplate violation. Subsidence detected only on later CT images was deemed delayed cage subsidence (DCS). Endplate breaches were classified as type 1, subsidence into the contralateral caudal endplate; type 2, bilateral subsidence into the caudal endplate, producing an anterior tilt of the cage; or type 3, bilateral subsidence into both caudal and cranial endplates.22
Cost Analysis
A comparative cost analysis between eLLIFp and alternative procedures for single-level ASD in a private hospital in Australia was undertaken (Table 1). The total implant charges were calculated using the Private Health Insurance Prostheses List23 for the eLLIFp prosthesis compared with a single LLIF cage, single transforaminal lumbar interbody fusion (TLIF) cage, and 2 PLIF cages all with posterior pedicle screw-rod extension, PLF (without cage[s]), and an integrated anterior lumbar interbody fusion (ALIF) cage (without posterior instrumentation). The total operating room (OR) charges were calculated using the mean OR time per procedure (eLLIFp 2 hours; PLF 2.5 hours; TLIF, PLIF, ALIF, and LLIF with posterior instrumentation all 3 hours) times the mean operating theater cost of AU$2500 per hour.24 The total inpatient hospital charges were calculated using the mean length of stay per procedure (eLLIFp and LLIF with posterior instrumentation both 3 days; PLF 4 days; TLIF, PLIF/ALIF all 5 days) times hospital bed cost of AU$1335 per day.25 The specialist fees for the spine and vascular access surgeon (operation item code numbers) and anesthetist (AU$19.80/unit) were calculated using the Medicare Benefits Schedule.26 The cell saver with perfusionist charge is AU$500 per procedure (used in PLIF, PLF, and ALIF). Multimodal IONM with neurophysiologist charge is AU$1500 per procedure (used in eLLIFp and LLIF with posterior instrumentation). The mean total cost per procedure for single-level ASD was then calculated by the sum of the contributing charges.
Comparative cost analysis of single-level eLLIFp, LLIF with posterior fixation, TLIF, PLIF, PLF, and ALIF.
Statistical Methods
Analyses were performed using IBM SPSS Statistics, version 21.0 (IBM Corp., Armonk, New York, USA) and included paired t tests, unpaired t tests, and Fisher exact tests. P values less than 0.05 were considered statistically significant.
Results
Patient Characteristics
Thirty-three patients received 35 eLLIFp devices. Their mean age was 64.9 years, and 18 were women (Table 2). Mean time from posterior fusion to ASD was 7.8 years. The most common ASD pathology was degenerative spondylolisthesis, followed by foraminal stenosis and canal stenosis. One patient with multiple myeloma died before 6-month follow-up. Two-level fusion was the most common previous posterior fusion surgery.
Patient and treatment characteristics.
Surgical Data
The most commonly treated ASD levels were L3-L4 (Figure 2) and L2-L3 (Figure 1). Mean total psoas retraction time was 30.5 minutes. Mean retraction time was 14.4 minutes with the retractor opened 22 mm and 13.9 minutes with it opened 25 mm (Table 2). Estimated blood loss was less than 50 mL for all patients.
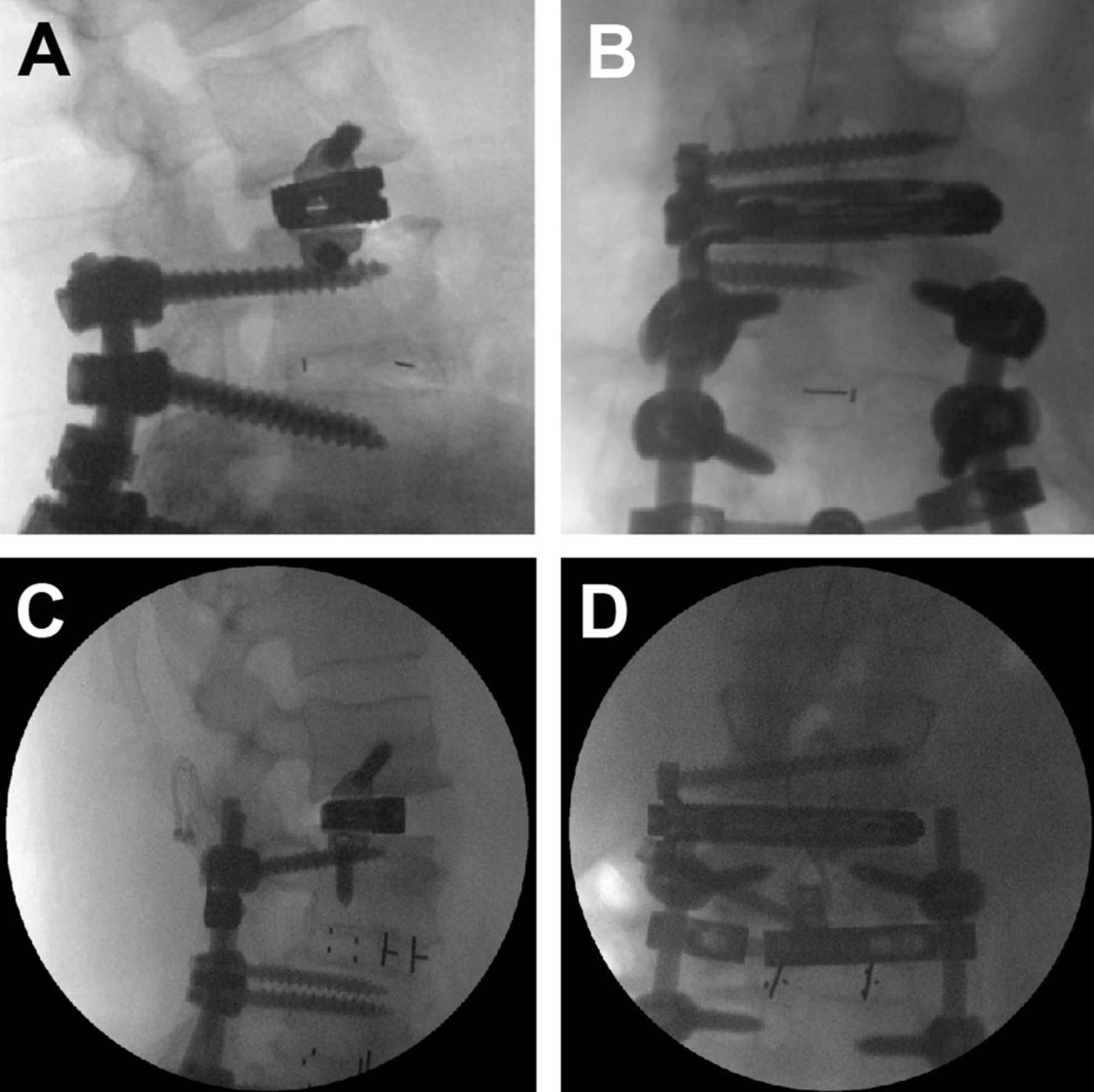
Radiograph of expandable lateral titanium interbody cage with an integrated lateral fixation at the L3-L4 level with the inferior screw of the lateral plate placed above (A, B) and below (C, D) the in situ superior pedicle screw: (A, C) lateral and (B, D) anteroposterior films.
Clinical Outcomes
Mean follow-up duration was 18 months. By last follow-up, mean back and leg pain scores improved from 7.8 to 0.6 and 6.9 to 0.6, representing 92% and 91% improvements, respectively. Oswestry Disability Index improved by 47% at 12-month follow-up (Table 3). Quality-of-life scores also improved from baseline to 12-month follow-up, with physical component score and mental component score improving by 69% and 42%, respectively. All clinical outcomes improved significantly from baseline.
Clinical outcome scores.
Radiographic Outcomes
The eLLIFp cages were expanded to a mean anterior height of 10 mm and lordosis of 8°, which added 2.2° SL, 2.2° LL, and 2.7 mm PDH from preoperatively to fusion time (Table 4). These increases were significant for SL and PDH but not LL. The mean difference in PDH from 6 weeks to 12 months was 2.7 ± 1.5 mm. Interbody fusion rates increased from 53% at 6 months to 94% (32/34 cages) at 12 months (Table 5). The 2 eLLIFp cage nonunions were both at the L4-L5 level. We found no significant difference in eLLIFp fusion rates between the previous 1 to 4 segment posterior fusions. There was also no significant difference in fusion rates between cages filled with Infuse or corticocancellous fibers. No ECS or DCS was observed at any of 35 eLLIFp cages.
Lordosis and posterior disc height on computed tomographic images.
Fusion rates on computed tomography images at 6 and 12 mo postoperatively.
Complications
Total complication rate was 9%, with rates of 6% and 3% for minor and major complications, respectively (Table 6). One patient experienced right anterior thigh pain, which resolved after 2 weeks; one developed anterior thigh sensory loss, which resolved by 4 weeks. Another patient developed new motor deficit with right L4 radiculopathy after L3-L4 eLLIFp despite normal IONM, which improved at 12 months. Neurologic complication rate was 6%. No genitofemoral nerve palsy or femoral neuropathy occurred. There were no bowel injuries or cage migration. No secondary lateral surgery, posterior decompression, or supplemental posterior fixation at the index or adjacent levels was required.
Minor and major complications.
Cost Analysis
The mean total cost of each procedure for single-level ASD included the proportion of total implant charges (26%–40%), total OR charges (25%–28%), and total hospital charges (22%–27%). Mean total cost of eLLIFp for single-level ASD was AU$19,71523 (Table 1). By relative costs using eLLIFp as the index cost, an extension PLF without cage (AU$21,996) was 1.1 times greater; ALIF with integrated plate and screws was 1.3; LLIF with pedicle screw-rod extension and extension TLIF were both 1.4; and an extension PLIF was 1.5 times greater total cost.
Discussion
While MIS fusion has been identified with similar fusion rates, patient satisfaction, patient-reported outcomes, and complications as open techniques, it has the advantages of less blood loss, length of hospital stay, and cost savings.27 However, both clinically symptomatic ASD and radiographic degeneration classifications remain substantial following spinal fusion. Rates of radiographic degeneration adjacent to previous PLIF are 29% to 34% over 5 to 10 years.28 A review of 4206 patients reported incidences of 5.9% and 1.8% per year for adjacent level degeneration and ASD, respectively.28 Sears et al reported 5- and 10-year ASD rates of 9% and 16%, 17% and 31%, and 29% and 40% after 1-, 2-, and 3/4-level PLIF, respectively.2 Accordingly, most patients (75%) in our study had previous 2-level or 3/4-level PLIF.
In this study, the mean duration between primary PLIF and ASD was 7.8 years, which was longer than the 4.7 years observed in a retrospective review of 1000 patients.3 Our mean age at presentation for ASD was 65 years, similar to ages reported previously.3,4 The most common initial ASD pathologies reported previously3 were degenerative spondylolisthesis and canal stenosis, which were similar to our most common pathologies: spondylolisthesis, foraminal stenosis, and canal stenosis.
Sex did not appear to affect the risk of ASD. Women and men were approximately equally represented in this study, which is consistent with previous results.29 Higher BMI is a risk factor for ASD, and our cohort had an average BMI of 29.5 kg/m2. Laminectomy for stenosis adjacent to a fusion also increases the risk of ASD; hence, extension of PLIF2 or LLIF with supplemental posterior fixation3 is recommended.
LLIF is an alternative technique for ASD. It enhances interbody fusion and provides better biomechanical stability.30,31 It preserves all posterior stabilizing ligamentous structures, prevents injury to paraspinal muscles, and avoids denervation or injury to the adjacent superior facet joints. Epidural scarring, perineural fibrosis, cerebrospinal fluid leak, and direct nerve root injury are also avoided.5 LLIF also produces lower infection rates and less estimated blood loss. No wound infections occurred in our study.
Intervertebral cages used with LLIF span both apophyseal cortical rims, providing optimal endplate support to minimize subsidence risk.32 Reported subsidence rates after LLIF range from 10% to 62%.33–35 Higher rates of subsidence with stand-alone LLIF cages occur with reduced bone density (T scores less than −1.0),34 but we found no cases in our patient cohort with eLLIFp cages. Cage geometry is important for avoiding subsidence.32 Subsidence rates are higher with 18-mm polyetheretherketone cages than with 22-mm polyetheretherketone cages (14.1% vs 1.9%).36 The eLLIFp cage width of 20 mm is thus advantageous for avoiding subsidence. Effects of cage length are less clear. Previous studies reported that length does not affect subsidence unless it is insufficient to cover the periphery of the endplates.31,36 However, a greater cage height appeared to increase the rate of subsidence.35 Hence, we took great care to expand the cage using tactile feedback to obtain a snug fit and not torque the expansion mechanism.
Frisch et al reported subsidence rates of 16% with static cages and 0% with expandable cages.12 However, patients with static cages underwent unilateral posterior stabilization, whereas most patients with expandable cages underwent bilateral posterior stabilization requiring repositioning to the prone position. Compared with static cages, expandable cages are inserted at a lower profile and expanded in situ, resulting in less trialing and iatrogenic endplate disruption secondary to impaction. Li et al noted significantly lower subsidence rates with expandable cages compared with static cages at 12-month follow-up.13 The absence of ECS or DCS in our study reflects an experienced lateral surgeon considering the following factors: (1) appropriate case selection; (2) choosing the side of approach best for disc space entry; (3) judicious use of anteroposterior and lateral fluoroscopy; (4) Cobb elevator release of the contralateral lateral ligament; (5) careful endplate preparation; (6) minimal endplate trauma with trials; (7) using angled instruments if indicated (especially at L4-L5); (8) impaction of a wide footprint cage orthogonal to the disc space; (9) the fact that a cage of adequate length is critical to span the apophyseal ring appreciative of ipsilateral osteophytes; (10) careful distraction of the cage avoiding torque release (designed to protect the cage); and (11) lateral plate fixation screws equal to or 10 mm less than cage length.
Biomechanical data for LLIF indicate that spinal segment stability is greater with supplemental fixation than with stand-alone cages.30,37 Indications for supplemental “gold standard” posterior pedicle screw-rod fixation follow a published treatment algorithm and include reduced bone density, facet arthropathy, instability, deformity, pars defect, and at least 3-level pathology.8 The benefits of lateral fixation are a shorter surgical time and no patient repositioning for posterior fixation. Lateral plates reduce lateral bending significantly and also reduce axial rotation, flexion, and extension compared with LLIF cages alone.30,37 However, coronal vertebral body fractures have occurred in osteoporotic patients with a separate 2-hole lateral plate and unilateral pedicle screws10 and in nonosteoporotic patients with 1- and 2-level separate 2-hole lateral plates.11 Separate 4-screw plates are more rigid in all motion planes38 but are technically difficult to insert without causing psoas trauma and are associated with higher risk of lumbar plexus injury. Static lateral cage with integrated 2-screw fixation was initially utilized to limit cage migration after planned or inadvertent anterior longitudinal ligament disruption.39 In our experience, the eLLIFp device was robust with screw lengths equal to or 10 mm less than the cage length to optimize fixation and did not require supplemental posterior pedicle screw-rod fixation.
In our eLLIFp technique, we used a drill, rather than an awl, to create holes for the integrated lateral plate screws and to navigate the superior screw and the inferior screw more accurately. We observed no misplaced screws, cage migration, screw pullout, screw fracture, or vertebral body fracture during follow-up. Likewise, no patient required secondary lateral surgery, posterior decompression, or supplemental posterior fixation at the index or adjacent levels.
The transpsoas approach is associated with anterior thigh pain, weakness, or sensory loss in 27.5% to 38.5% of patients, with the highest risk at the L4-L5 level.40 A rising psoas sign or “Mickey Mouse”-shaped psoas muscle rising away from the vertebral column41 with a more anterior position of the lumbar plexus is associated with a higher incidence of iatrogenic plexus injury.17 In a prospective, multicenter study of over 300 LLIF procedures at L4-L5, mean retraction time was 32 minutes in patients with new postoperative symptomatic lumbar plexus neuropraxia and 23 minutes in those without.42 Despite longer mean retraction times for eLLIFp than for impaction of lateral static cages,43 we observed low rates of anterior thigh pain and sensory changes. The majority of our eLLIFp cages was at the L2-L3 and L3-L4 levels, with only 20% at L4-L5 level. One 79-year-old female patient developed a new motor deficit postoperatively. She had a 12-month history of worsening low back pain and bilateral L4 radicular pain unresponsive to conservative treatment. Magnetic resonance imaging showed moderate central canal and lateral recess stenosis above the L4-S1 PLIF performed 4 years before. L3-L4 eLLIFp was performed, with normal IONM results pre-, intra-, and postoperatively. The patient awoke with severe right L4 radiculopathy, which improved 40% by 6 weeks and 70% by 12 months. The presumed etiology was ipsilateral lumbar plexus traction injury, given the unilateral improving weakness and sensory loss, rather than L4 nerve root tethering from scar in the lateral recesses, which would cause bilateral deficits. The low rate of anterior thigh symptoms and lumbar plexus injury using the eLLIFp in our series is multifactorial. First, an experienced lateral surgeon and operating team took great care in patient positioning to minimize the table break, thus reducing the stretch on the psoas muscle. Second, multimodal IONM detected nerve compromise earlier (compared with electromyography alone), enabling protective adjustments such as reducing table break and repositioning the initial probe and K-wire to ensure the tubular retractor is anterior to the plexus. Critically, the surgeon must directly visualize the target disc space and use triggered EMG to ensure that no nerves, particularly the femoral nerve, cross the operative field. Third, sequential opening of the tubular retractor, initially to a 22-mm diameter for discectomy and then ultimately trialing to a 25-mm diameter, accommodated the eLLIFp prosthesis. Moreover, the eLLIFp is low profile, reducing the risk of psoas muscle and nerve entrapment underneath the insertion. The integrated 2-hole plate is fixed to the cage to prevent posterior plate migration and requires less exposure compared with larger separate lateral plates.
With eLLIFp, back and leg pain improved over 90% by the time of solid fusion. These results were somewhat better than the 80% improvement reported for expandable lateral cages14 and clearly superior to the 49% to 60% improvement with static cages.4,8,13,19 Functional status and disability improved 47% and 69% in our cohort, which were similar to improvements reported for static cages but lower than that reported for expandable lateral cages.13
Our results suggest that indirect neural decompression with eLLIFp was successful, as none of our patients required subsequent posterior direct decompression for either central or foraminal stenoses. In a prospective study of 122 consecutive patients who underwent lateral interbody fusion with impacted 10° lordotic cages, 9% required subsequent unplanned direct posterior decompression for missed unstable spondylolisthesis, bony lateral recess stenosis, or misaligned cages, resulting in contralateral foraminal encroachment.43 The authors concluded that patients with neurogenic claudication and radiculopathy from spinal canal or foraminal stenosis could be successfully treated with lateral interbody fusion, but those with leg pain secondary to bony lateral recess stenosis or unstable degenerative spondylolisthesis may benefit from second-stage direct decompression and fixation.
Solid interbody fusion was achieved for 94% of eLLIFp cages on CT evaluation at 12 months. Our fusion rate was superior to fusion rates reported for stand-alone LLIF cages33 and similar to those for LLIF cages with supplemental posterior fixation.32 A recent study proposed evaluating segmental immobilization in LLIF by both interbody and zygapophyseal joint fusion rather than anterior fusion alone.44 We observed no significant difference in eLLIFp interbody fusion rates between 1 and 4 segment previous fusions, although the 2 nonunions in our study were both found at the L4-L5 level. We suspect the eLLIFp nonunion rate is more dependent on the specific level (L4-L5), rather than on the number of levels (1-, 2-, 3-, or 4-level) of previous posterior fusions, due to the higher biomechanical stress at the L4-L5 segment. The 2 cages in our study without bridging intertrabecular bone showed titanium endplates fused to the vertebrae and no radiolucent lines, subsidence, or screw loosening, consistent with stable locked pseudarthrosis.32 These patients also had no increased mechanical pain indicative of nonunion.
SL and PDH improved significantly from preoperatively to postoperatively and were maintained until fusion, without the need for posterior fixation. The 8 to 17 mm × 5° to 20° eLLIFp cages were expanded to an average 10 mm and 8°, which added 2.2° of SL and 2.7 mm of PDH. These were similar to the changed with static 10 mm × 10° lordotic cages, which increased SL by 2.4° and PDH by 2.6 to 2.7 mm from preoperatively to fusion.19,45 Expandable lateral cages with posterior fixation provide superior SL improvement and similar PDH improvement, compared with eLLIFp. The SL difference may reflect differences in operative levels: 80% of eLLIFp cages were used at less lordotic upper lumbar levels,46 whereas 76% of expandable lateral cages were inserted at L3-L4 and L4-L5.13
We found a comparative mean total cost analysis of eLLIFp (AU$19,715) to single-level PLF, ALIF, LLIF with posterior fixation, TLIF/PLIF (range AU$21,966–30,393) was consistent with median total US costs by the corresponding surgical approach type (range US$18,038–29,640) for single-level lumbar fusions,47 and the mean total cost of lumbar fusions by US national Medicare claims of US$31,716 ± 18,124.48.48 The proportion of our mean total costs for the 6 procedures for lumbar ASD comprising implant charges, OR charges, and hospital charges was similar to the implant, OR, and room charges reported in a cost analysis of single-level lumbar fusions at the University of California.47 The total implant charges were lower for eLLIFp than for alternative procedures (Table 1). Additionally, eLLIFp has lower direct hospital costs with a shorter operation time and hospital length of stay than ALIF, PLF, and TLIF/PLIF.25 Both eLLIFp and LLIF require IONM but no vascular access surgeon,26 cell saver, or perfusionist. None of our eLLIFp patients required intensive care unit admission. These costs have external validity for surgeons in other countries to compare surgical treatment options for symptomatic ASD.
The strengths of this study include the consistent surgical technique performed by a single senior surgeon well experienced in lateral fusion procedures. Furthermore, IONM facilitated a low rate of neurological injury. CT was used for serial radiologic assessments of subsidence, SL, and PDH, with measurements performed using digital software. Additionally, thin-section CT assessments of fusion are superior to evaluating plain static and flexion-extension radiographs.49 It is also the first study to assess efficacy and cost-effectiveness of the eLLIFp device as a stand-alone treatment in appropriately selected patients with 1 to 2 levels of ASD with minimal to no deformity.
Limitations of this study include the relatively small cohort size and intermediate duration of follow-up. Although a comparison cohort was not included, our results are consistent with those reported in the literature. Long-term follow-up of eLLIFp is planned to evaluate the incidence and timing of further ASD. In patients with significant global deformities (sagittal and/or coronal imbalance) more extensive fusion incorporating posterior fixation and osteotomies would be indicated.
Conclusion
This study showed that the MIS eLLIFp provided a low morbidity, cost-effective, and robust alternative to traditional posterior construct extension surgery for rostral lumbar ASD in carefully selected patients with 1- to 2-level stenosis and minimal deformity. Significant changes in SL and PDH were observed during 12-month follow-up. Significant improvements in pain, function, and disability were also demonstrated. By 12 months, there was a high rate of interbody fusion and no cases of subsidence. Expandable cage technology reduced psoas retraction, minimized endplate trauma, and permitted customized lordosis and disc height. Despite longer psoas retraction times, eLLIFp was not associated with increased risk of lumbar plexus injury. Multimodal IONM and an experienced surgeon likely contributed to this low risk. No revision lateral surgery, posterior decompression, or supplemental posterior fixation was required.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Gregory M. Malham reports speaking/ teaching and trips/travel arrangements with Device, Globus Medical, LifeHealthcare, and National Surgical and consulting fees from Globus Medical. The remaining authors have nothing to report.
Ethics Approval Epworth HealthCare, Professor Nikolas Zeps, Group Director of Research and Development, nik.zeps@epworth.org.au
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}