


Abstract
Background Vertebral compression fractures (VCF) are usually treated by cementoplasty. Computerized navigation allows more accurate surgery without additional imaging acquisition for guidance and related radiation exposure. New technologies trend to optimize the irradiation for patients and surgeons. The objective was to investigate the radiological results and radiation exposure of O-arm navigation compared with the all-in-one 2-dimensional/3-dimensional (2D/3D) Surgivisio device in navigated cementoplasty procedures.
Methods Patients in the O-arm group comprised an O-arm prospective cohort as well as previous patients. Operations for VCF by navigated cementoplasty took place over 18 months. Patients in the Surgivisio group were the first patients operated on using Surgivisio and were prospectively recruited. Demographic, operative, and irradiation data were collected, as well as the image quality subjectively evaluated by the surgeon. The vertebal filling was evaluated using the Garnier classification and quoted as satisfactory, acceptable, or poor. The effective dose in millisievert (mSv) was calculated for radiation exposure estimation, and the absolute risk of cancer (AR) in percent equivalent to a whole-body irradiation was also calculated.
Results A total of 123 patients were included: 62 in the O-arm group and 61 in the Surgivisio group. A total of 166 vertebrae were analyzed. Compared with the Surgivisio group, the effective dose was significantly higher in the O-arm group, with a mean of 11.47 vs 1.14 mSv, respectively (P < 0.001). The 2D part of the effective dose received by the surgeon was significantly higher in the O-arm group, with an average of 2.25 vs 0.47 mSv, respectively (P < 0.001). Overall AR followed the same trend, with a mean of 4.9 × 10–4% in the O-arm group and 5.7 × 10–5% in the Surgivisio group (P < 0.001). Operative time was significantly higher in the O-arm group (34.52 vs 30.12 minutes respectively, P = 0.03). Image quality was similarly sufficient in 3D, but in 2D, image quality was significantly better in the O-arm group (P = 0.01). Vertebral filling was significantly better in the O-arm group, with 100% of results reported as satisfactory and acceptable versus 85% in the Surgivisio group (P < 0.001).
Conclusions The O-arm delivered a 10-times higher effective dose during navigated cementoplasty in comparison with the Surgivisio device. The O-arm also had a longer operative time, but it had better image quality and radiological results.
Level of Evidence 4.
Introduction
Vertebral compression fractures (VCF) are frequent injuries, mostly related to high energy traumas on young people and bone fragility in the elderly population.1 VCF are successfully treated by cementoplasty, such as vertebroplasty or kyphoplasty.2,3 These procedures require the use of 2-dimensional (2D) imaging for intraoperative control of fracture reduction and cement filling. The 3-dimensional (3D) imaging with computerized navigation offers confidence and ergonomy during surgery with more accurate procedures.4 However, imaging devices currently use x-ray technology and thus have associated cancer risk,5 which is referred to as “stochastic risk.” This risk can be estimated through the effective dose in millisievert (mSv). New technological advances trend to optimize irradiation related to the imaging devices.6 O-arm with navigation (Medtronic, Minneapolis, MN, USA)7,8 and Surgivisio (eCential Robotics, Gières, France)9,10 showed good results and accuracy during spine procedures.
The purpose of this study was to compare the irradiation and radiological results of percutaneous cementoplasty for VCF performed with the O-arm surgical system associated to the navigation with the all-in-one 2D/3D imaging device with integrated navigation named Surgivisio. Hypotheses were that considering the new Surgivisio device, O-arm produces more irradiation with less image quality with radiological results similar to Surgivisio.
Methods
Inclusion and Exclusion Criteria
The O-arm group was composed of 30 patients prospectively recruited and a review of medical records of all consecutive patients who underwent cementoplasty during a previous 18-month period at a private clinic with a fellowship program. The Surgivisio group was prospectively constituted with the first consecutive patients operated at the University Hospital of Grenoble with the Surgivisio device. Exclusion criteria were refusal to participate and lack of information to calculate the radiation exposure.
Study Design
Study design was ambispective.
Ethical Statement
The study was performed in accordance with the canonal Ethical Commission of Vaud and the approved research protocol (No. 2021–00298). All patients provided written consent for participation in the study.
Interventions
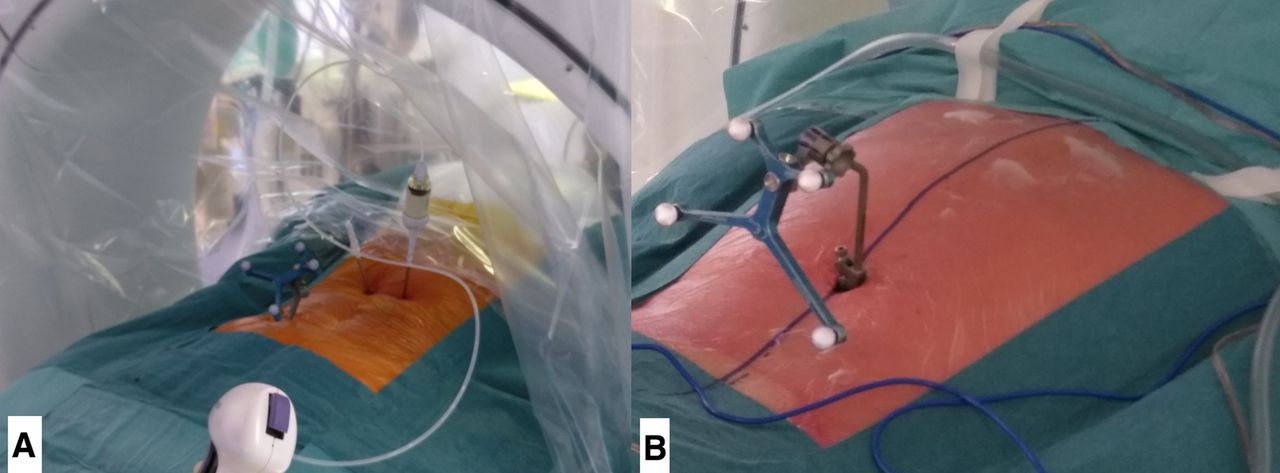
For both groups, patients underwent operations in the prone position under general anesthesia and after antibiotic prophylaxis. For O-arm procedures, a pin was introduced in the posterior iliac crest with patient frame attached (Figure 1). The 2D acquisitions for vertebral landmarking were performed. Then, while the detection camera could reach the patient frame and detectors on the O-arm machine (Figure 1), a 3D acquisition could be performed under medically induced apnea, and the images were transmitted to the Stealth navigation system (Medtronic, Minneapolis, MN, USA).
For the Surgivisio group, the patient frame was attached using 2 to 4 Kirschner wires introduced in the spinous processes of the area of the vertebra to be operated,11 and 2D fluoroscopic landmarking was performed (Figure 2). When detection of all detectors inside the patient frame was reached in an anterior-posterior view, a lateral view was performed, and then the 3D acquisition took place without apnea, the detectors following breath movements of the patient. Considering the 2 machines, operating room personnel could leave the operating room during 3D acquisition, avoiding irradiation. Then, a percutaneous cannulated navigated Jamshidi needle could be introduced inside the pedicle of the fractured vertebra (Figures 3 and 4), and cementoplasty was performed under 2D imaging. The surgeon and other personnel carried a lead apron and a thyroid shield for radiation protection.
In patients with a loss of height of the operated vertebra of more than 20% and a local kyphosis of more than 10°, vertebral augmentation was peformed using a balloon Kyphon (Medtronic, Minneapolis, MN, USA)12 for the O-arm group or a SpineJack device (Vexim, Balma, France)13 for the Surgivisio group, and then polymethyl methacrylate cement was injected in the vertebral body. In other cases for both groups, polymethyl methacrylate cement was injected alone for standard vertebroplasty. For the O-arm group, X’Pede cement was used (Medtronic, Minneapolis, MN, USA), and VertaPlex HV cement (Stryker, Portage, MI, USA) was used for the Surgivisio group.
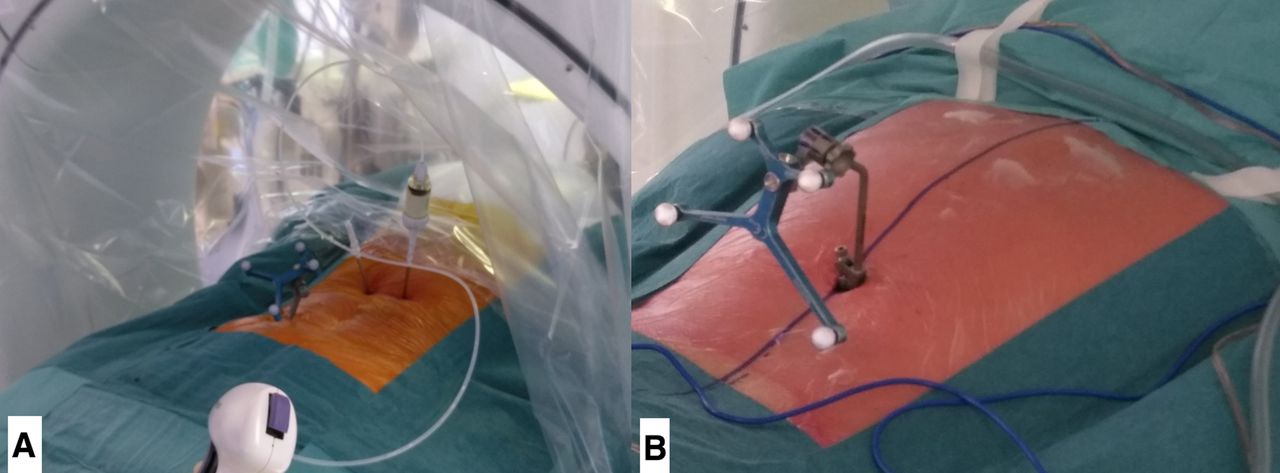
Intraoperative views of the patient frame and the O-arm settings. We can notice the percutaneous insertion of the Jamshidi needles, and the cement filler fixed on its extremity. Note the pin within the posterior cresta iliaca (A). In case of thoracic spine procedure, a spinous clamp may be required (B).

Intraoperative view of the patient frame fixed with Kirschner wires on spinous processes and a navigated Jamshidi needle with Surgivisio.
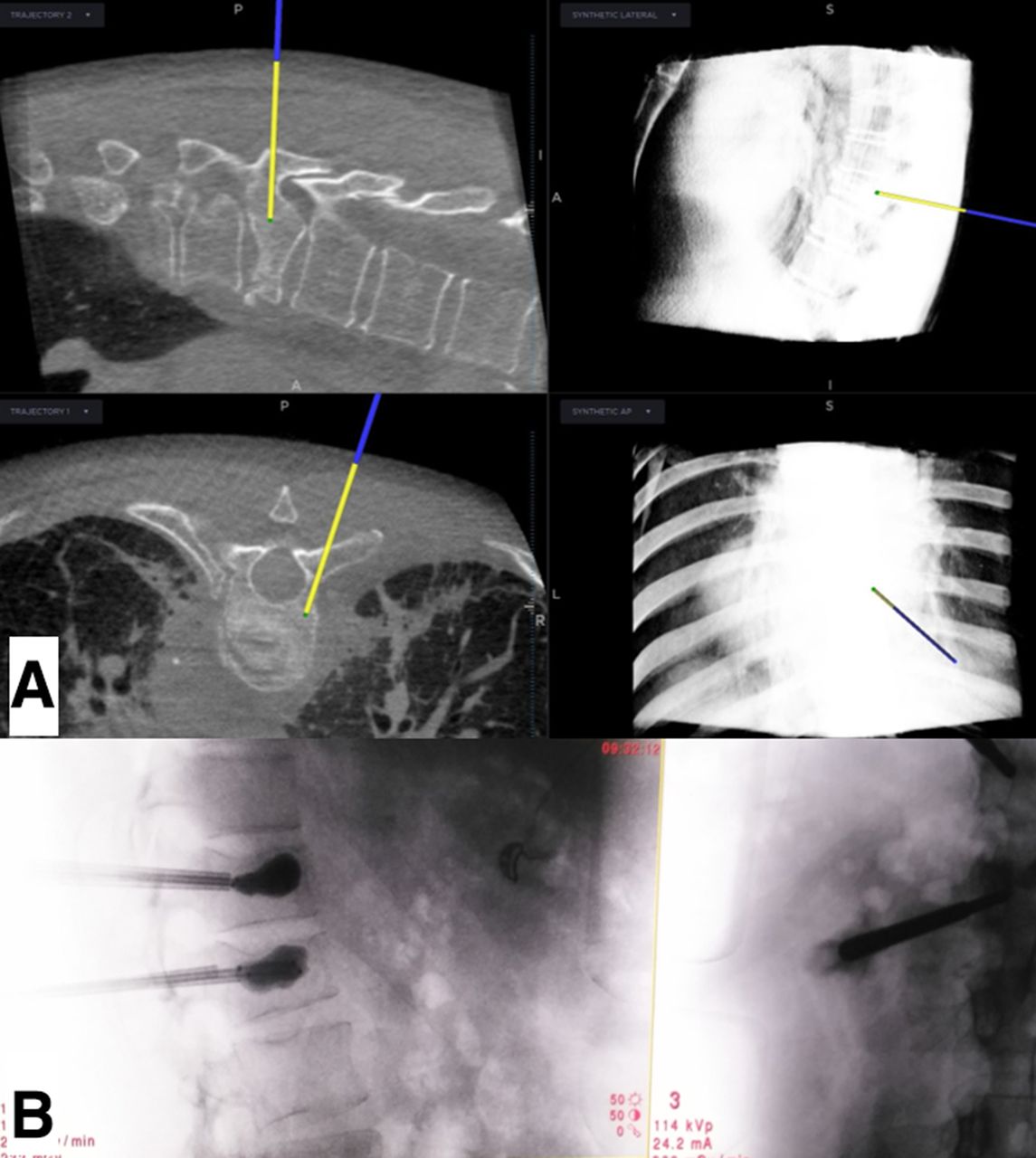
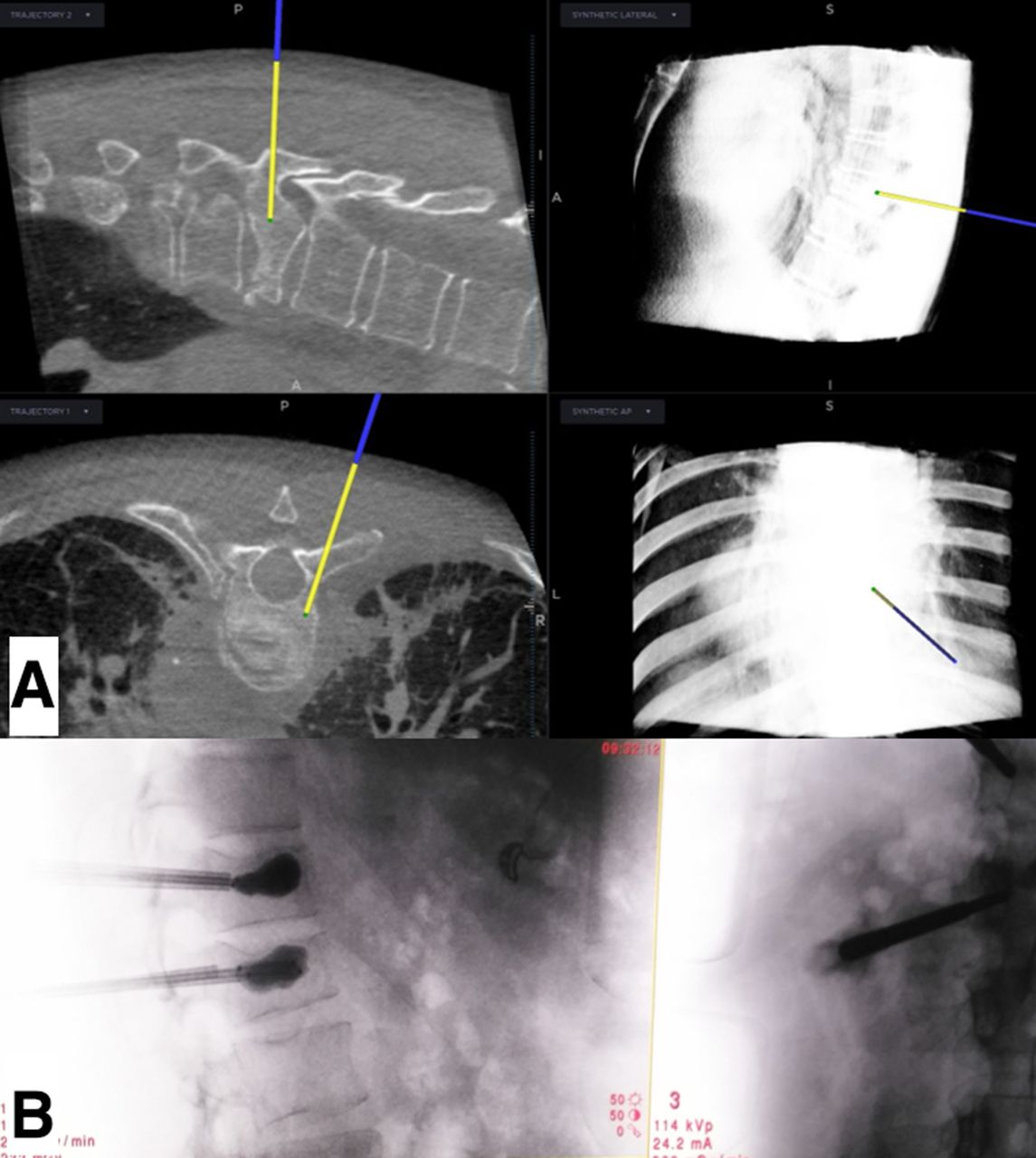
Displayed view of the computerized navigation with O-arm for percutaneous cementoplasty (A).The 2-dimensional view of balloon reduction for percutaneous kyphoplasty (B).

Displayed view of the computerized navigation with Surgivisio for percutaneous cementoplasty.
Data Collection
Demographic data were stored such as age (in years), gender, height (in centimeters), and weight (in kilograms). Surgical data were also collected, such as the Magerl classification14 of the vertebral fractures, the level and the number of operated vertebrae, the operative duration from incision to closure (in minutes), the full 2D imaging duration (in seconds), the surgeon level (junior, such as a resident or registrar or fellow, and senior), and the image quality in 2D and 3D during the procedure, reported as sufficient or insufficient according to the surgeon’s consideration. We also collected irradiation data such as the dose-area product (DAP) in mGy·cm2 from the dosimetric report of the Surgivisio device and of the 2D O-arm fluoroscopy and the dose-length product (DLP) in mGy·cm for the O-arm in 3D mode at the end of the surgical procedure. The effective dose E in mSv was calculated using the DAP and the operative field dimensions, with weight and height of the patient, through a Monte Carlo simulation using the PCXMC 2.0 software (STUK, Radiation and Nuclear Safety Authority, Helsinki, Finland).15 The 3D-related E was calculated with the DLP according to the European Guidelines for Multislice Computed Tomography16 using the corresponding generalized coefficients k (in mSv/[mGy·cm]) related to the irradiated region. For the thoracic region, k was 0.014, for the lumbar region and the whole trunk, k was 0.015. The calculation formula was as follows: E = DLP × k, where E is the effective dose. For approximate calculation of the effective dose related to 2D irradiation, we also utilized conversion factors w (in mSv/[Gy·cm2]) according to the European Commission report No. 180,17 with w of 0.19 and 0.26 for the thoracic and lumbar spine, respectively. We also compared these results with those obtained with PCXMC. The absolute risk of cancer (AR) in percent equivalent to a whole-body irradiation was also calculated, considering a value of 5% per Sv.18 Operative and imaging duration per level were also calculated. The vertebral filling was radiologically appreciated using the Garnier classification19 and quoted as satisfactory (Y3, Z2, Z3), acceptable (X2, X3, Y2), or poor (X1, Y1, Z1). Cement leakage was classified as anterior, cranial, posterior, lateral, or caudal.
Outcome Measures
The main outcome was the overall effective dose; the secondary outcomes were the effective dose per 3D acquisition and received by the surgeon during 2D fluoroscopy, AR, the operative and imaging durations, the image quality in 2D and 3D, and the vertebral cement filling.
Statistical Methods
Statistical analyses were performed using R statistical software,20 v.3.1.3. Student t test was used for comparison of numerical variables, and Fisher exact test was used for binomial comparison. Correlations were determined using the Pearson test and analysis of variance. A threshold ≤0.05 was defined as a statistically significant difference.
Results
Demographic Data
A total of 123 patients were included: 62 in the O-arm group and 61 in the Surgivisio group. Sex ratio (men/women) was 24/38 for the O-arm group and 24/37 for the Surgivisio group. A total of 166 vertebrae were operated: 81 in the O-arm group and 85 in the Surgivisio group. Magerl repartition was as follows: 65 (86%) A1, 6 (8%) A2, and 10 (13%) A3 in the O-arm group; 77 (90%) A1, 5 (6%) A2, and 3 (4%) A3 in the Surgivisio group.
Operative Data
There was a significantly higher operative time in the O-arm group compared with that in the Surgivisio group, with a mean duration of 34.52 vs 30.12 minutes, respectively (P = 0.04). The same trend was observed for the mean operative time per level: 28.75 vs 24.16 minutes, respectively (P = 0.01). Unipedicular approach during vertebroplasty was achieved for 34 (42%) procedures in the O-arm group and 69 (81%) procedures in the Surgivisio group, with a significant difference (P < 0.001). More procedures were performed by junior surgeons in the O-arm group (P = 0.02). These data are detailed in Table 1.
Patient demographics and surgery data.
Radiological Results
For the 2D fluoroscopic duration, an average of 25.99 seconds for the O-arm group and 32.66 seconds for the Surgivisio group were observed, with a significant difference (P = 0.04). Vertebral filling was significantly better in the O-arm group, with 100% of satisfactory and acceptable results vs 85% in the Surgivisio group (P < 0.001). Cement leakage was less frequent but not significant in the O-arm group, with 16 (20%) vs 25 (29%) reported in the Surgivisio group (P = 0.09), with a posterior leakage requiring immediate decompression in the O-arm group. All operative data are detailed in Table 2.
Garnier classification of vertebral filling and cement leakage.
Radiation Exposure
The overall effective dose was significantly higher in the O-arm group compared with the Surgivisio group, with a mean of 11.47 vs 1.14 mSv, respectively (P < 0.001). The same trend was found for the effective dose per level: 9.83 vs 0.88 mSv, respectively (P < 0.001). The 3D-related effective dose was significantly higher in the O-arm group, with a mean of 9.22 vs 0.67 mSv in the Surgivisio group (P < 0.001). The same effect was observed for the effective dose per 3D acquisition: 5.84 vs 0.60 mSv, respectively (P < 0.001), and for the 2D-related effective dose: 2.25 vs 0.47 mSv, respectively (P < 0.001). The comparison between the effective dose related to 2D calculated with PCXMC and with the European Commission w conversion factors found similar results of 2.25 vs 2.40 mSv, respectively, for the O-arm group (P = 0.68), and the same trend for the Surgivisio group, with a mean of 0.47 vs 0.57 mSv, respectively (P = 0.30). In the O-arm group, more 3D acquisitions were performed than in the Surgivisio group: a mean of 1.63 acquisitions per patient vs 1.01, respectively, with a significant difference (P < 0.001). Overall AR followed the same trend, with a mean of 4.9 × 10–4% with the O-arm group and 5.7 × 10–5% with the Surgivisio group (P < 0.001). Irradiation data are detailed in Table 3.
Radiation exposure data comparison in the 2 groups.
Correlation Study
Correlation studies revealed that the effective dose was not correlated to the surgeon level (P = 0.24 and 0.17, respectively) but only to the age and the imaging duration in the O-arm group (P = 0.02 and P < 0.001, respectively) and to the operative time in the Surgivisio group (P < 0.001). The analysis of variance method showed no correlation between surgeon level and operative time in both groups (P = 0.61 and P = 0.12, respectively). Correlation studies are detailed in Table 4.
Correlation of the effective dose and surgeon level with other parameters for the 2 groups.
Image Quality
Image quality always was sufficient in 3D for both groups and significantly better in 2D for the O-arm group than for the Surgivisio group (P = 0.01). These results are summarized in Table 5.
Subjective image quality.
Discussion
The most important finding was the confirmation of most hypotheses with significantly more irradiation with the O-arm in comparison with the Surgivisio device, with a mean 10 times higher radiation exposure. To our knowledge, this is the first time that a comparative study between the O-arm and Surgivisio devices was conducted in clinical practice. However, Rousseau et al performed a dosimetric comparison in experimental conditions.21 The authors found an effective dose related to 3D of 2.41 and 0.35 mSv with the O-arm and Surgivisio device, respectively, and an effective dose related to 2D of 1.54 and 0.30 mSv, respectively. They also reported that organ doses were 5 to 7 times higher with the O-arm in comparison with the Surgivisio device, which followed a trend that aligned with our results.
The first prospective series about kyphoplasty under O-arm guidance was performed by Schils on 16 cases.22 He reported an operative time of 41 minutes, a fluoroscopy time of 3.23 minutes, and a fluoroscopy time per level of 2.43 minutes. The same author published about 54 cases23 with reduced durations: operative time of 38 minutes, fluoroscopy time of 3.1 minutes, and fluoroscopy time per level of 2.5 minutes. Tonetti et al published the first series9 of 65 consecutive vertebroplasties using the Surgivisio device and found a mean operative time of 30 minutes. Other 3D devices were used for percutaneous cementoplasty. Tam et al utilized the Axiom Artis dTA VB31 (Siemens, Germany) and found a mean operative time of 64 minutes.24 Sing and Jeong used the Siremobil isoC3D (Siemens, Germany) and reported a mean operative time of 52 minutes.25 Ruatti et al performed 72 percutaneous procedures under the guidance of the Arcadis Orbic System (Siemens, Germany) and found a mean operative time by level of 46 minutes.26
Absence of correlation between operative time and surgeon level for the 2 groups indicated that the step-by-step process included in the O-arm navigation and in the Surgivisio systems helped to standardize the surgical technique.
Izadpanah et al reported results about 30 computer-navigated kyphoplasties on the thoracic spine (TS) and the lumbar spine (LS).27 They found an average operation time of 67 minutes in the TS and 62 minutes in the LS, a radiation time of 99 seconds in the TS and 74 seconds in the LS, with a DAP of 12,450 and 13,180 mGy·cm2, respectively. Tonetti et al9 found a mean E of 1.32 mSv per level, with the use of the Surgivisio device. However, they utilized European Commission conversion factors w for dose calculation. These results are less accurate than with the use of the PCXMC software,17 with an uncertainty in practice about 10% to 20%. They found similar results than the current study when compared with those obtained with the same conversion factors. Another case reported an effective dose of 1.17 mSv for the use of a 180-image 3D acquisition with the Surgivisio device, in the case of a T1 vertebra osteoid osteoma resection.10 Another study from Boudissa et al about percutaneous pedicle screw insertion using the Surgivisio device11 found a mean effective dose of 1.97 mSv. The study from Farah et al28 about pedicle screw insertion using the O-arm and the AIRO (Brainlab AG, Germany) devices found a mean effective dose of 1.04 and 3.9 mSv, respectively, per navigated vertebra, with 2D imaging used only for landmarking.
Differences between O-arm and Surgivisio may be explained by technological aspects. The O-arm is a 2D and 3D cone beam computerized tomography. The Surgivisio is a 2D and 3D C-arm. Both devices use plan detectors as imaging technology. However, the O-arm performs a 3D acquisition with delivery of 192 images, whereas the Surgivisio could perform 180 or 90 images for a whole 3D acquisition, explaining higher effective dose related to 3D in the O-arm group. Voltage is higher in standard O-arm settings in comparison with the Surgivisio device, leading to higher level of irradiation.21 Higher effective dose and better image quality in 2D mode for the O-arm can be explained by its settings, with a standard 30 pulses per second. Surgivisio produces 8 pulses per second in 2D mode. The O-arm is already known to produce high exposure in 2D.29,30 Operative time reduction in the Surgivisio group may be related to the easy way to put the reference frame on the patient on both LS and TS. Thoracic O-arm cementoplasty may require a spinous clamp with skin incision and muscular dissection around the spinous process before performing the 3D acquisition, increasing the operative duration. Repeated 3D acquisitions increased operative time and also effective dose related to 3D. Putting in perspective the absence of poor radiologic cement filling and less cement leakage in the O-arm group, we could suppose that the better image quality may have improved control of cement injection during O-arm procedures. Higher number of kyphoplasties in the O-arm group may have also helped reducing the rate of cement leakage.31 Additionally, higher age in the O-arm group could lead to poor bone quality and difficulty to clearly see vertebrae during cementoplasty due to osteopenia. Better radiological results were reached by higher necessary irradiation to get adequate image quality. Higher rate of unipedicular vertebroplasties in the Surgivisio group could also explain its inferior radiological results.
According to the as low as reasonably achievable principle,32 there are several ways to decrease dose regarding the results with the O-arm. Using the low-dose mode in 3D, limiting the number of 3D and 2D acquisitions and finally using the collimation of the imaging field may help to decrease the overall dose. For the Surgivisio group, using the 90-image 3D acquisition mode and limiting the number of 3D and 2D acquisitions may also decrease the overall dose.
There were some limitations in this study: its ambispective design was the first; the Surgivisio cohort may have benefited from a Hawthorne effect33 in contrast to the retrospective part of the ambispective O-arm cohort. Second, the effective dose calculation is an estimation using standard and specific measurements for the Monte Carlo simulation. There was a calculation bias in the dose estimation because we could not intraoperatively measure the exact focus to skin distance in clinical practice, considering this distance modifying every time during the surgery and even more during the 3D acquisition with the Surgivisio device. For reproducibility purposes, we considered the standard focus to skin distance of 80 cm for all patients in the 2 groups, according to standard settings of the software. So, the accuracy of the dose estimation could be supported by the consideration of the other parameters.
Conclusion
The O-arm delivered a 10 times higher effective dose during navigated cementoplasty procedures in comparison with the Surgivisio device. Operative time was also higher with the O-arm, while image quality and radiological results were better. Further studies about other minimally invasive spine techniques comparing these devices should be performed to help spine surgeons to determine the best choice for their clinical practice.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Marc Prod’homme, Guillaume Cavalié and Didier Grasset have nothing to disclose. Jérôme Tonetti discloses that he is on the speaker’s bureau of the eCential Robotics company and received consulting honorarium from; he is on the speaker’s bureau for the Spine Art company and received money for consulting from, and he also received a fellowship support from the Zimmer Biomet company. Duccio Boscherini discloses that he was on the speaker’s bureau for the Medtronic company, and he still remains a non-remunerated consultant; he was also on the speaker’s bureau for the Johnson and Johnson company and received money for consulting from. Gael Kerschbaumer discloses that he is a consultant for the eCential Robotics company and received grants for research from. Mehdi Boudissa discloses that he is on the speaker’s bureau as a consultant for the eCential Robotics company received grants for research from; he also received grants for a fellowship training from the Zimmer Biomet company.
Ethical Standards The procedures followed were in accordance with the ethical standards of the responsible committees on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. The ethical commission on human research of the Vaud canton approved the research protocol (Nr. 2021-00298).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Significant Reduction of Radiation Exposure Using Specific Settings of the O-Arm for Percutaneous Cementoplasty in Accordance With the ALARA Principle
- Significant Reduction of Radiation Exposure Using Specific Settings of the O-Arm for Percutaneous Cementoplasty in Accordance With the ALARA Principle