


Abstract
Background Fusion has long been used for treating chronic back pain unresponsive to nonoperative care. However, potential development of adjacent segment degeneration resulting in reoperation is a concern. Total disc replacement (TDR) has been proposed as a method for addressing back pain and preventing or reducing adjacent segment degeneration. The purpose of the study was to determine the reoperation rate at the segment adjacent to a level implanted with a lumbar TDR and to analyze the pre-TDR condition of the adjacent segment.
Methods This study was based on a retrospective review of charts and radiographs from a consecutive series of 1000 TDR patients to identify those who underwent reoperation because of adjacent segment degeneration. Some of the patients were part of randomized studies comparing TDR with fusion. Adjacent segment reoperation data were also collected from 67 patients who were randomized to fusion in those studies. The condition of the adjacent segment before the index surgery was compared with its condition before reoperation based on radiographs, magnetic resonance imaging (MRI), and computed tomography.
Results Of the 1000 TDR patients, 20 (2.0%) underwent reoperation. The mean length of time from arthroplasty to reoperation was 28.3 months (range, 0.5–85 months). Of the adjacent segments evaluated on preoperative MRI, 38.8% were normal, 38.8% were moderately diseased, and 22.2% were classified as having severe degeneration. None of these levels had a different grading at the time of reoperation compared with the pre-TDR MRI study. Reoperation for adjacent segment degeneration was performed in 4.5% of the fusion patients.
Conclusions The 2.0% rate of adjacent segment degeneration resulting in reoperation in this study is similar to the 2.0% to 2.8% range in other studies and lower than the published rates of 7% to 18% after lumbar fusion. By carefully assessing the presence of pre-existing degenerative changes before performing arthroplasty, this rate may be reduced even more.
Traditionally lumbar fusion has been considered the gold standard of surgical treatment for axial low-back pain due to symptomatic degenerative disc disease. However, a potential problem associated with fusion procedures is adjacent segment degeneration, sometimes resulting in additional surgery. Harrop et al.1 differentiated adjacent segment degeneration, which they described as the radiographic finding of degeneration at the level adjacent to a fusion, as compared with adjacent segment disease, which was clinical symptomatic degeneration often resulting in additional surgery.
Numerous studies exist supporting the development of adjacent segment disease due to lumbar fusion procedures. In a literature review Harrop et al.1 reported the rate of adjacent segment disease in patients undergoing lumbar arthrodesis to be 14% (173 of 1216). Errico2 reported that as many as 29% of lumbar fusion patients had recurrence of their pain, which was usually associated with adjacent segment disease. With the advent of total disc replacement (TDR), it was thought that the development of adjacent segment disease might be reduced. Newer studies suggest that TDR may be related to a reduced incidence of adjacent segment disease compared with fusion. European studies involving 100 or more patients with minimum 10-year follow-up have reported the rate of adjacent segment degeneration after TDR to be 2.0% to 2.8%.3, 4 In one such study, David3 concluded that the “rate of reoperation secondary to adjacent segment disease is ten times lower than the rates reported in the literature for fusion.”
In a literature review of 595 TDR patients, Harrop et al.1 identified 7 patients (1.2%) with adjacent segment disease. Cinotti et al.5 performed lumbar arthroplasty in 46 patients. At 2-year follow-up, 10 patients were selected to undergo lumbar magnetic resonance imaging (MRI). No degenerative changes were found at the levels adjacent to the TDR. Other studies have reported overall reoperation rates after lumbar TDR to be in the range of 2.7% to 8.8% with up to 6-year follow-up.6, 7 Considering these rates, not all attributable to adjacent segment degeneration, these studies support the notion that this problem is relatively less frequent after disc replacement than after fusion.
One question that may arise in the discussion of adjacent segment degeneration after fusion or TDR concerns the condition of the adjacent level before surgery. The status of the adjacent segment before the index operation may affect the occurrence of adjacent segment reoperation. The purpose of this study was to determine the reoperation rate of a segment at the level adjacent to a level implanted with a TDR and to analyze the preoperative condition of that segment.
Methods
The series of the first 1000 consecutive TDR patients at a single center was reviewed, and patients who underwent reoperation limited to the adjacent segment for degeneration were identified. These 20 patients were further analyzed based on radiographs obtained before the original procedure, as well as before reoperation. Radiographs including plain film flexion/extension radiographs, MRI, and computed tomography (CT) were reviewed to assess pre-existing pathology that may have predisposed the patient to degeneration at an adjacent segment.
Preoperative MRI T2-weighted sagittal images obtained before the index TDR, as well as those obtained before reoperation, when available, were reviewed and classified with respect to the condition of the disc that was eventually reoperated on for adjacent segment degeneration. This provided a mechanism to evaluate the extent of degeneration that occurred after TDR. Each disc was graded based on the following system (Fig. 1). Discs with well-maintained disc height, bright white signal, normal-appearing morphology, and no evidence of endplate changes were given a classification of normal. Discs with minimal loss of disc height, gray signal, some morphologic changes noted but still maintaining overall shape, and no endplate changes were given a classification of moderate. Discs with extensive loss of disc height, darkened or black signal, distinctly abnormal morphology, and endplate changes were given a classification of severe. MRI studies were also assessed for the presence of facet cysts or fluid within the facets indicative of degeneration or instability.
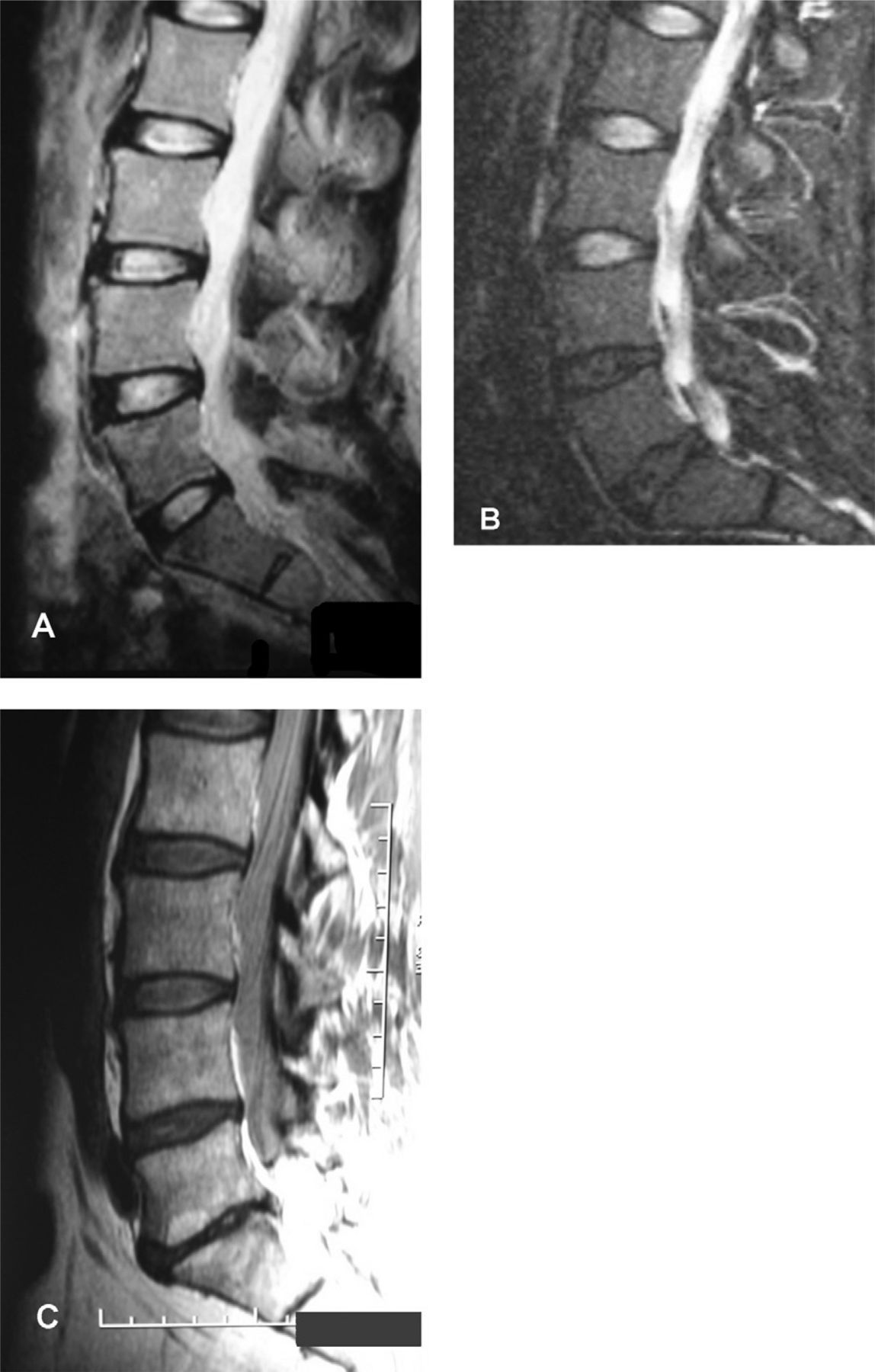
MRI classification: normal discs (A), moderate degeneration of L4-5 and L5-1 discs (B), and severe degeneration of L5-1 disc (C).
Axial CT and post-myelogram CT images, when available, were evaluated both before TDR and before reoperation. Particular attention was focused on the condition of the facet joints. The facets were graded based on the system outlined by Pathria et al.8 Grade 0 indicated normal facet joints without evidence of degeneration. Grade 1 indicated evidence of joint space narrowing. Grade 2 had evidence of joint space narrowing as well as bony sclerosis and/or hypertrophy of the facet joints. Grade 3 had severe osteoarthritis with marked narrowing of the joint space, bony sclerosis, and osteophyte formation.
Patients enrolled in the early arthroplasty studies were randomized to either TDR or fusion. A total of 67 patients were randomized to fusion. In 3 of these patients, adjacent segment disease developed, requiring reoperation. Radiographs, CT, and MRI of these patients, when available, were reviewed as detailed earlier.
All radiographs were reviewed for 2 purposes. First, they were reviewed to identify pre-existing pathology that might be implicated in the development of degeneration at adjacent segments. Retrospectively reviewing levels that subsequently developed degeneration adjacent to a total disc arthroplasty is important to identify characteristics of those levels that could have originally been missed or dismissed as insignificant findings. Second, by evaluating characteristics such as disc height, disc quality, and facet joint condition both before TDR and then again in conjunction with preoperative evaluation for reoperation, quantitative and qualitative data can be applied to the operative segments and provide a more standardized means of assessing these levels.
Results
Of the 1000 consecutive TDR patients, 20 (2.0%) underwent reoperation for adjacent segment disease. This group included 9 men and 11 women with a mean age of 43.2 years (range, 20–61 years) and mean body mass index of 26.6 (range, 18.6–36.2). The mean length of time from arthroplasty to reoperation was 28.3 months (range, 0.5–85 months).
A TDR was initially implanted in 21 levels in these 20 patients. At the time of reoperation, 24 levels were addressed. At reoperation, 10 TDRs, 10 fusions, and 4 laminectomies/discectomies were performed. Of the 10 fusions, 5 were 360° fusions, were standalone anterior lumbar interbody fusions (ALIFs), and 2 were extreme lateral interbody fusions (XLIFs). Five patients had 2 levels addressed at reoperation. One had an additional 2-level TDR, one had a 2-level fusion, 2 underwent 2-level laminectomy/discectomy, and 1 had a single-level fusion followed by a TDR at an adjacent level 4 years later.
Of 20 patients, 14 had a pre-TDR MRI study available for review. Among the adjacent segments that were reoperated on, 7 (38.8%) were normal, 7 (38.8%) were moderately diseased, and 4 (22.2%) were classified as having severe degenerative changes. Among the 8 levels for which post-TDR, pre-reoperation MRI studies were available for review, none had a different grading at the time of reoperation compared with the pre-TDR MRI study. In addition, there were no facet cysts or fluid within the facet joints identified on either the original MRI study or the MRI study obtained before reoperation.
Pre-TDR CT and/or post-myelogram CT images were available for review for 15 patients, with 21 adjacent segments evaluated. Of the facets, 12 (57%) were grade 0, 7 (33.3%) were grade 1, and 2 (9.5%) were grade 2. There were no facets with grade 3 degeneration. Before reoperation, CT images from 8 patients were available for review and compared with CT images obtained at the time of the index arthroplasty. A total of 10 facet levels were assessed; 2 (20%) of these levels progressed 1 grade in severity from the time of the TDR surgery. The remaining 8 levels (80%) showed no changes.
Of 67 patients randomized to lumbar fusion, 3 (4.5%) underwent reoperation for adjacent segment disease. The mean length of time from fusion to reoperation was 59.4 months (range, 40–96 months). There were 2 men and 1 woman with a mean age of 47.0 years (range, 45–51 years) and mean body mass index of 27.25 (range, 26.5–28.1). Two stand-alone ALIFs using BAK cages (Zimmer Spine, Minneapolis, MN) and one 360° fusion made up the index procedure group. Reoperations included 1 TDR, 1 single-level laminectomy/discectomy, and 1 single-level decompression. The patient undergoing the single-level decompression as a reoperation had evidence of moderate disc disease based on MRI findings before the index fusion. MRI was not available before the decompression. CT grading of the facets showed a grade of 0 before the index fusion, which did not change before reoperation. The patient undergoing laminectomy/discectomy as a reoperation had evidence of severe disc disease on MRI at the time of index fusion. This level subsequently herniated, leading to surgical intervention. The facet condition at the time of index fusion was found to be grade 1, and follow-up was not available. The third patient did not have MRI or CT images available for evaluation for this study.
Discussion
Historically, axial low-back pain of discogenic origin has been treated surgically by fusion after nonoperative interventions failed to provide adequate relief. The goal of the procedure is pain relief, and it has generally been beneficial for most patients. One potential shortcoming of fusion is the development of degeneration at adjacent segments, sometimes leading to additional surgery. TDR was designed to help prevent the development of adjacent segment disease.
Among fusion patients, Berg et al.9 reported an overall reoperation rate of 10%, with the most common cause (7%) being symptomatic adjacent segments. Aiki et al.10 reported a rate of 7.7% of patients (9 of 117) requiring reoperation within 7 years after lumbar fusion because of symptomatic adjacent segment disease. In a study of 106 fusion patients, Gillet11 reported that radiographic evidence of adjacent segment degeneration developed in 40 patients (37%), with 19 undergoing surgery (18%). Ghiselli et al.12 reported much higher rates in a series of 215 patients. They found the rate of symptomatic degeneration at 5-year follow-up to be 16.5% and the predicted rate to be 36.1% at 10 years.
In our study 67 patients were randomized to undergo lumbar fusion. Of these patients, 3 (4.5%) underwent reoperation for adjacent segment disease. One of these patients had evidence of severe disc disease based on MRI findings at the time of the index fusion.
In this series of 1000 TDR patients, 2% had adjacent segment degeneration resulting in reoperation. This was similar to the previously published reoperation rates after arthroplasty (2.0% to 2.8%)1, 3–5 and was much lower than the rates reported for fusion (7% to 18%).1, 2, 7–11 It is thought that because TDR allows motion at the operated levels, the adjacent segments are not subjected to additional stresses that may occur with fusion. In a biomechanical study, Dmitriev et al.13 found that TDR was associated with less intradiscal pressure and motion at the adjacent segment compared with fusion.
The 20 patients in our study undergoing reoperation after TDR were further analyzed to assess for the presence of pre-existing pathology that may have predisposed their adjacent segments to symptomatically degenerate. On the basis of available MRI studies, it was determined that no segments progressed with regard to the appearance of disc signal quality. Four patients undergoing reoperation had discs adjacent to the TDR level that were graded severe at the time of the index procedure. Three of these discs had nonconcordant pain based on discography and were therefore not surgically addressed at the time of the index operation. The fourth patient was originally scheduled for a 3-level TDR, but confounding medical and anatomic issues (aortic dilatation) prevented a sufficient anterior exposure to address all 3 levels. It was determined before operation to address the 1 level with arthroplasty that could be reached with an anterior approach and, if symptoms persisted, to address the other 2 levels at a later date (which was performed).
Further evaluation of facet conditions at the time of the index procedure and before reoperation showed progression of degeneration of 2 facet levels. Each level progressed by 1 grade of severity, from 0 to 1. Two patients undergoing reoperation had a facet grading of 2 (unchanged from index operation), with all others grading 0 or 1.
As indicated by these results, 30.0% (6 of 20) of patients undergoing reoperation had evidence of degenerative changes at the time of the index procedure. One patient had 2 levels that had already become symptomatic and required surgical treatment, though addressed at a later date. Not counting this patient in whom surgery at the adjacent segment was planned, the adjacent segment reoperation rate was 1.9%, with 26.3% (5 of 19) having degenerative changes at the adjacent segment before the index surgery. The remaining 5 showed evidence of adjacent segment pathology initially and were predisposed to subsequent degeneration. Of note, not all patients were analyzed for preexisting adjacent segment pathology, and it is likely that there are asymptomatic patients with similar adjacent segment degeneration. It is hoped that this aspect will be addressed in future work.
This study did have limitations. Given the retrospective design, not all patients had radiographs, CT, or MRI available for review from before both the index surgery and the reoperation. The number of patients undergoing reoperation was limited to those who have continued follow-up at our institution. This does not take into account patients who may have sought treatment elsewhere.
Reoperation because of adjacent segment disease after arthrodesis is a well-documented occurrence. With the development of TDR, an alternative now exists for treating axial low-back pain without the same level of risk of developing adjacent segment disease. The 2% incidence of reoperation shown in this study and others is much lower than the published rates of 7% to 18% after lumbar fusion. In addition, by carefully assessing the presence of pre-existing degenerative changes before performing arthroplasty, this rate may be reduced even more. The results of this study support the current available literature suggesting that TDR has the potential to reduce reoperation rates due to adjacent segment disease.
- © 2012 Published by Elsevier Inc. on behalf of ISASS - International Society for the Advancement of Spine Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}