


Abstract
Objectives To describe a rare case of acute intracranial subdural hematoma as a cause of postoperative delirium and headache following cervical spine surgery.
Summary of Background Data Headache is uncommon following spinal surgery, but can be observed in cases of accidental tearing of the dura during surgery. The causes of headache after surgery are thought to include dural tear and CSF leakage. On the other hand, intracranial subdural hematoma can be a cause of headache and cognitive dysfunction. However, only 4 cases as a postoperative complication of spinal surgery have been reported in the literature.
Methods A 55-year-old man underwent re-explorative surgery due to postoperative hematoma causing hemiplegia following cervical laminoplasty. During this operation, accidental dural tear occurred and induced CSF leakage. On the following day, headache and delirium were noted. CSF leakage continued despite intraoperative repair of the dural laceration. Cranial CT at that time clearly demonstrated subdural hematoma.
Results We reexplored the surgical site and attempted to stop the CSF leakage with meticulous suturing of the dural sac under microscopic observation. The intracranial subdural hematoma was carefully observed under consultation with a specialist neurosurgeon. Following this reexploration, the headache and delirium gradually improved, with spontaneous resolution of intracranial hematoma over a two-month period of observation.
Conclusions We have reported a rare case of acute intracranial subdural hematoma caused by CSF leakage following cervical spine surgery. This report demonstrates the possibility of intracranial hematoma as a cause of postoperative cognitive dysfunction or headache, especially when accidental tearing of the dura has occurred in spinal surgery.
Postoperative cognitive dysfunction affects a significant number of patients and may significantly hamper postoperative rehabilitation. It tends to be associated with advanced age, time of operation, method of general anesthesia used, and type of surgery.1–3 Headache after spinal surgery is uncommon but can be observed in patients with accidental tear of the dura. Thus, in patients complaining of headache after spinal surgery, dural tear and cerebrospinal fluid (CSF) leakage must be considered.
Intracranial subdural hematoma can be a cause of headache and cognitive dysfunction. However, it is seldom experienced as a cause of postoperative symptoms after spinal surgery. We encountered a case of intracranial subdural hematoma as a cause of postoperative headache and delirium after cervical laminoplasty. Decrease in intracranial pressure induced by CSF leakage appeared to be related to the formation of intracranial hematoma in this case.
The purpose of this article is to describe the details of this rare case and focus on the importance of screening for intracranial hemorrhage in patients with headache and cognitive dysfunction after spinal surgery.
Case report
Dysfunction of the hand and disturbance of gait developed in a 55-year-old man after initial numbness and pain in his right upper extremity. Cervical magnetic resonance imaging showed multiple compressions of the cervical spine on his visit to our clinic (Fig. 1). Physical examination at the time of admission showed spastic gait with exaggerated deep tendon reflexes and pathologic reflexes in both upper and lower extremities. In addition, mild motor weakness and sensory disturbance in both upper extremities were observed.
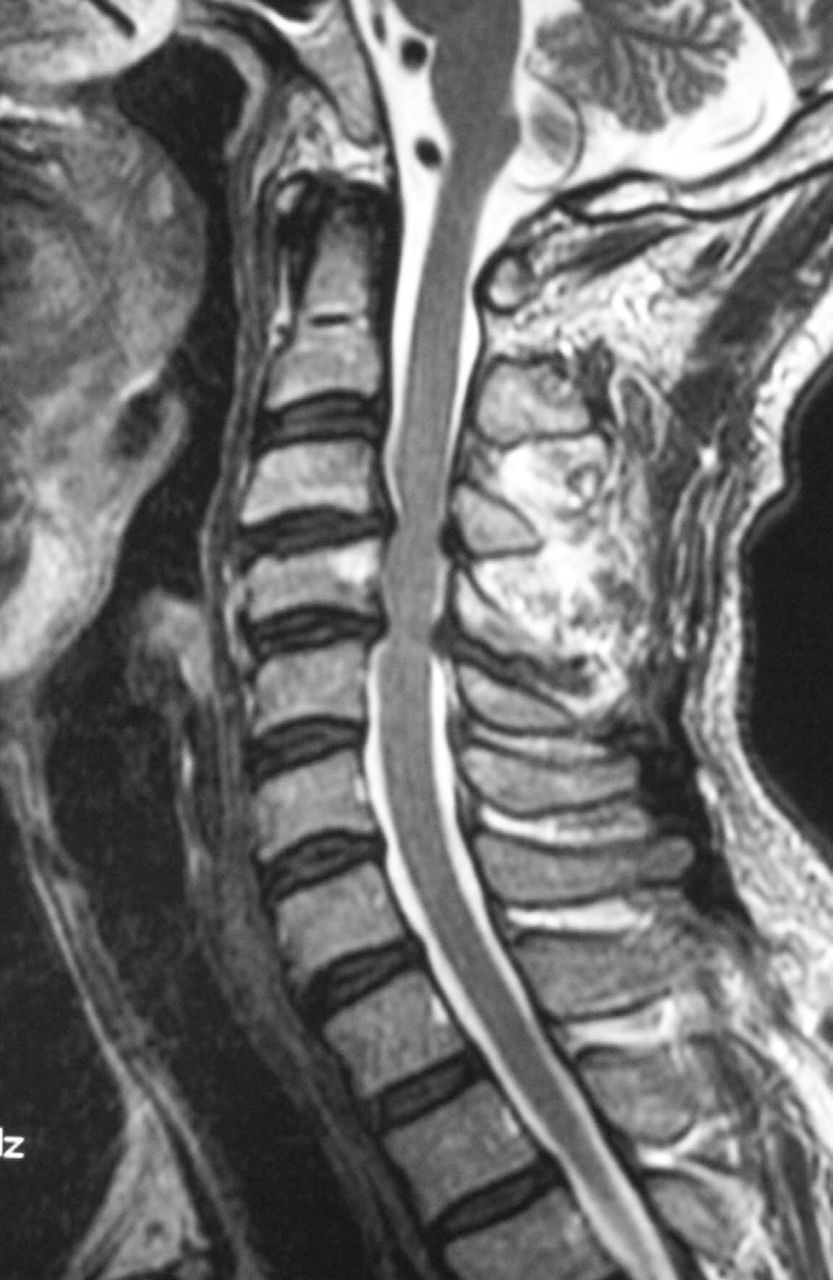
Cervical T2-weighted image on magnetic resonance imaging examination when the patient visited our clinic with the chief complaint of disturbance of walking, showing multiple compressions of the dural sac in the cervical spine.
The patient did not abuse alcohol and was taking no medications. Preoperative laboratory examination showed nearly normal findings, including bleeding time.
Cervical open-door laminoplasty was performed because of the progression of neurologic findings. The surgery was performed without problems. The time of operation was 200 minutes, and the amount of blood loss was 500 mL. Two hours after the conclusion of surgery, the patient complained of severe pain from the cervical region to the left upper extremity, which progressed to right-sided hemiplegia. On the basis of the diagnosis of epidural hematoma based on computed tomography (CT) findings, re-exploration of the cervical spine was performed; it revealed wide hematoma from C4-C7 and deformation of the dural sac. A point of active bleeding was recognized and stopped on the left side around the C3 lateral mass. However, a tear of the dura was unintentionally produced when the C6 lamina was being lifted and resected. The tear was sutured with No. 6-0 nylon, and the wound was closed after insertion of suction drainage.
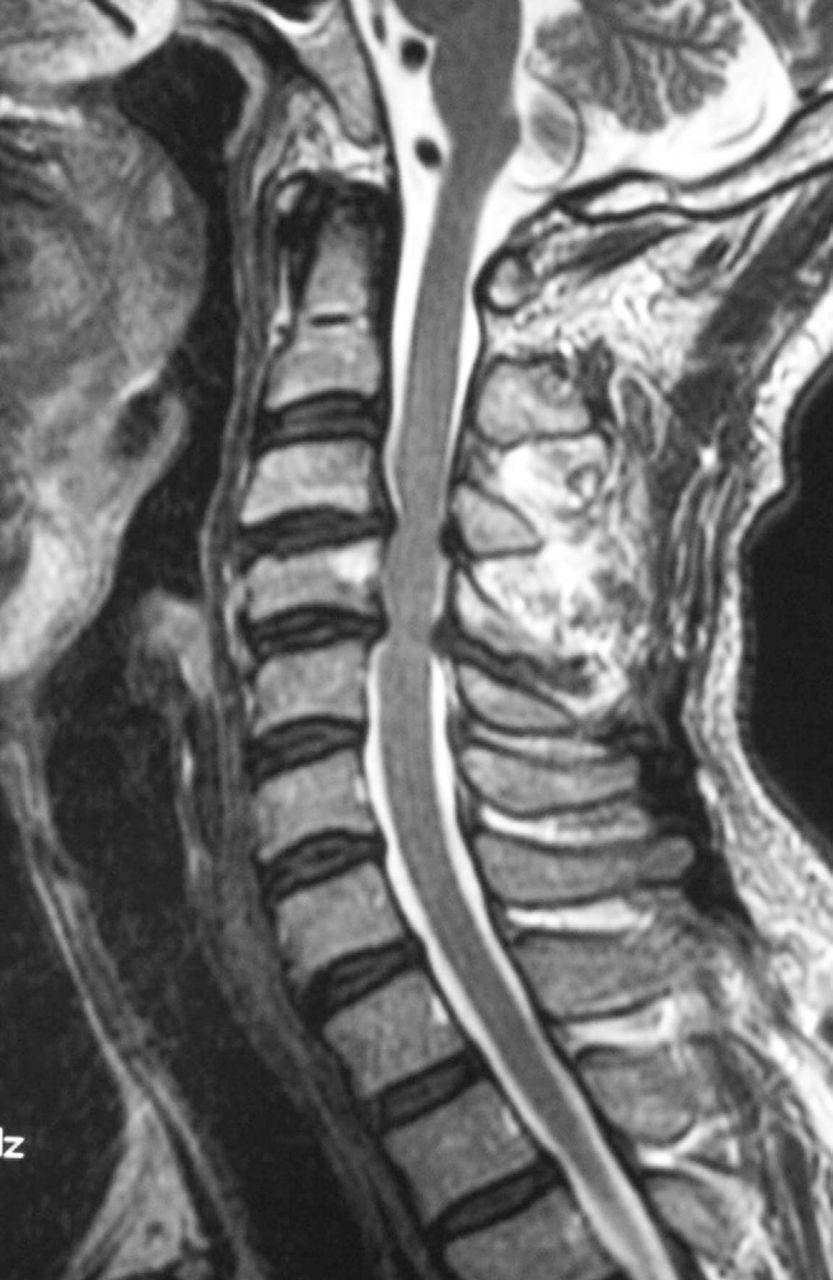
Despite improvement of neurologic findings in the patient's upper and lower extremities, he began to complain of severe headache. Cognitive dysfunction was subsequently observed. During this time period, CSF leakage continued on suction drainage. Because of progression of headache and cognitive dysfunction, cranial CT was performed and clearly showed intracranial subdural hematoma (Fig. 2). After consultation with a specialist neurosurgeon, we reexplored the surgical site and attempted to stop the CSF leakage with meticulous suturing under microscopic observation. The CSF leakage discontinued after this procedure.

Cranial CT scan at the time the patient complained of severe headache clearly showing intracranial subdural hematoma in the left hemisphere.
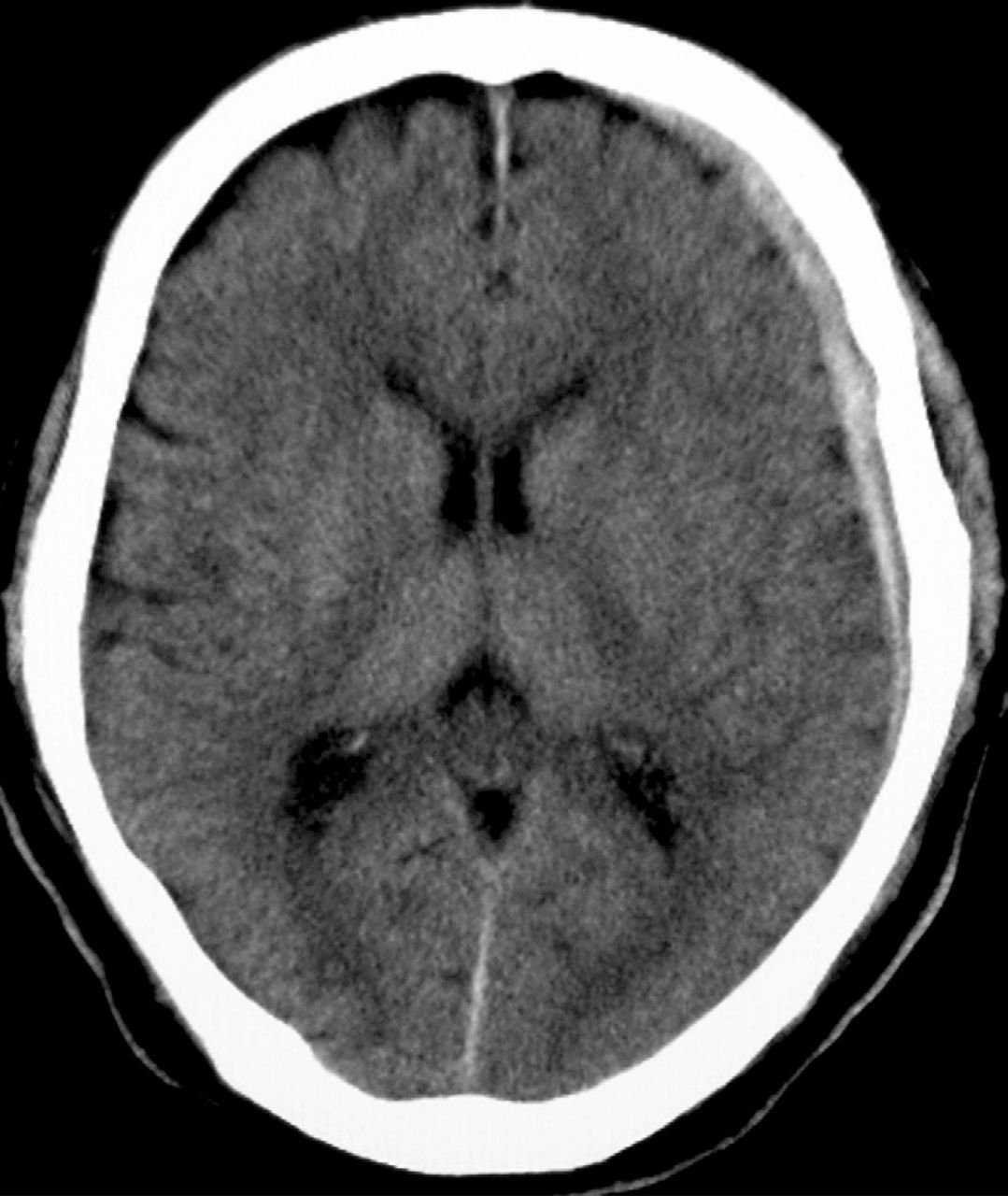
Under careful conservative observation of this subdural intracranial hematoma, the patient's symptoms gradually improved. CT at 2 months after re-exploration showed resorption of the hematoma (Fig. 3).

Cranial CT scan at 2 months after onset of hematoma showing its resorption.
At 2 years after cervical surgery, the patient was asymptomatic and did not complain of difficulty in activities of daily living.
Discussion
Postoperative delirium has been reported in elderly patients as a side effect of general anesthesia. Bruce et al4 reported that delirium occurs more commonly after hip fracture surgery than elective surgery. For spine surgery, however, there have been few reports of postoperative delirium. Kawaguchi et al1 pointed out that postoperative delirium occurred in 12.5% of patients aged 70 years or older undergoing surgery.
On the other hand, headache sometimes occurs after spine surgery, especially when CSF leakage occurs accidentally or is purposely induced during surgery. Headache can persist while CSF leakage continues.5
Intracranial subdural hematoma can be a cause of cognitive dysfunction and headache.6–9 However, this lesion has not been considered a sequela of spinal surgery. Thus far, to our knowledge, only 4 cases of intracranial subdural hematoma after spinal surgery have been reported.
The age at the time of onset ranged from 25 to 59 years, with a mean of 46 years. Headache was the most common clinical symptom. CSF leakage occurred in the lumbar spine in 3 cases and in the thoracic spine in 1 case. Although no cases of cervical spine surgery have previously been reported, the effects of CSF leakage in the cervical spine on intracranial structures would be greater.
The mechanism of formation of intracranial subdural hematoma is still unknown. However, the possibility has been suggested that bridging veins can be lacerated by the decrease in CSF pressure caused by CSF leakage.10–12 Many structural features detected mainly on electron microscopic examination suggest that bridging veins are more fragile in their subdural portion than in the subarachnoid space. Bridging veins are likely to rupture at their weakest point in the subdural space.13 When enlargement of a subdural hematoma occurs, symptoms gradually progress from headache to paralysis and disturbance of consciousness with development of cerebral herniation. Early detection of hematoma is thus important.
In our patient careful observation followed by early detection of intracranial subdural hematoma yielded a satisfactory clinical outcome. The usual course of treatment for a hematoma whose thickness is more than 1 cm or a case in which a mass effect, such as a midline shift, has taken place is to perform a hematoma evacuation with craniotomy; however, we performed conservative treatment because in this case, neither was found. The possibility of intracranial hematoma should be considered in patients with postoperative cognitive dysfunction or headache, especially when accidental tearing of the dura has occurred in spinal surgery.
- © 2011 SAS - The International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.