


Abstract
Background Transpedicular screws are currently placed with open free hand and minimally invasive techniques assisted with either fluoroscopy or navigation. Screw placement accuracy had been investigated with several methods reaching accuracy rates from 71.9% to 98.8%. The objective of this study was to assess the accuracy and safety for 2-D fluoroscopy-guided screw placement assisted with electrophysiological monitoring and the inter-observer agreement for the breach classification.
Methods A retrospective review was performed on 125 consecutive patients who underwent minimally invasive transforaminal lumbar interbody fusion and transpedicular screws placement between the levels of T-12 and S-1. Screw accuracy was evaluated using a postoperative computed tomography by three independent observers. Pedicle breach was documented when there was a violation in any direction of the pedicle. Inter-observer agreement was assessed with the Kappa coefficient.
Results A total of 470 transpedicular screws were evaluated between the levels of T-12 and S-1. In 57 patients the instrumentation was bilateral and in 68 unilateral. A substantial degree of agreement was found between the observers AB (κ=0.769) and A-C (κ=0.784) and almost perfect agreement between observers B-C (κ=0.928). There were a total of 427.33 (90.92%) screws without breach, 39.33 (8.37%) minor breach pedicles and 3.33 (0.71%) major breach pedicles. The pedicle breach rate was 9.08% Trajectory pedicle breach percentages were as follows: minor medial pedicle breach 4.68%, minor lateral pedicle breach 3.47%, minor inferior pedicle breach 0.22%, and major medial breach 0.70%. No intraoperative instrumentation-related or postoperative clinical complications were encountered and no surgical revision was needed.
Conclusions Our study demonstrated a high accuracy (90.2%) for 2-D fluoroscopy-guided pedicle screw using electromonitoring. Only 0.71% of the 470 screws had a major breach. Knowing the radiological spine pedicle anatomy and the correct interpretation of EMG are the key factors for this technique.
Introduction
Application of transpedicular screws for spinal instability had undergone technique refinements pursuing 100% accuracy. Techniques can be classified as open free-hand and minimally invasive assisted with either fluoroscopy or navigation.1 Pedicle screw fixation is a well-known and safe technique for spine surgeons with a low rate of complications.2 However, risk of serious neurological lesions,3 cerebrospinal fluid leaks,4 vascular5, 6 and visceral injures7 have raised interest to evaluate safety and accuracy for pedicle screw placement.
The objective of this study was to asses the accuracy and safety for 2-D fluoroscopy guided pedicle screw placement assisted with electrophysiological monitoring through a mini-open approach used for minimally invasive spine surgery transforaminal lumbar interbody fusion (MISS-TLIF).
Materials and Methods
A retrospective imagenological review was performed on 125 consecutive patients who underwent MISS TLIF and transpedicular screw placement between the levels of T-12 and S-1 by a single neurosurgeon (JASS), during a period between January 2010 to November 2014 at the ABC Medical Center in Mexico City, Mexico. The Education and Research Department of the --ABC Medical Center-- approved this study.
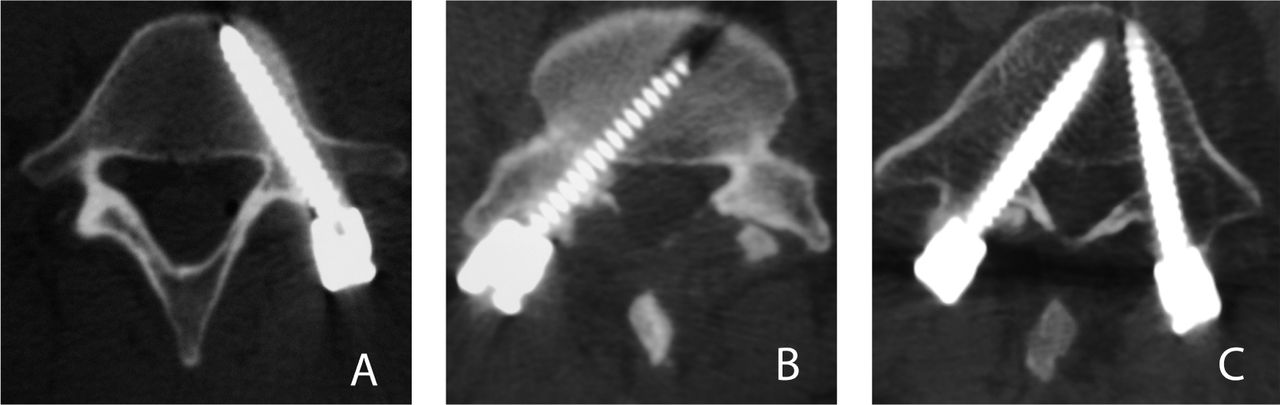
All patients were treated electively of 1, 2 or 3 levels using a minimally invasive transforaminal lumbar interbody fusion for the treatment of degenerative disk disease and spondylolisthesis of the lumbar spine. First time and revision cases were included in the study. Clinical follow up and postoperative computed tomography (CT) were available and reviewed for the 125 patients. CT (Brilliance 64, Phillips) images were assessed using “bone window” in the axial, coronal and sagittal planes by three independent observers, all of them neurosurgeons. Pedicle breach was documented when there was a violation in any direction of the pedicle as previously reported by Smith et al.8 and was classified in three grades: 1) No breach. 2) Minor breach, when the breach was ≤2 mm. 3) Major breach, when the pedicle violation was ≥3 mm (Figure 1).
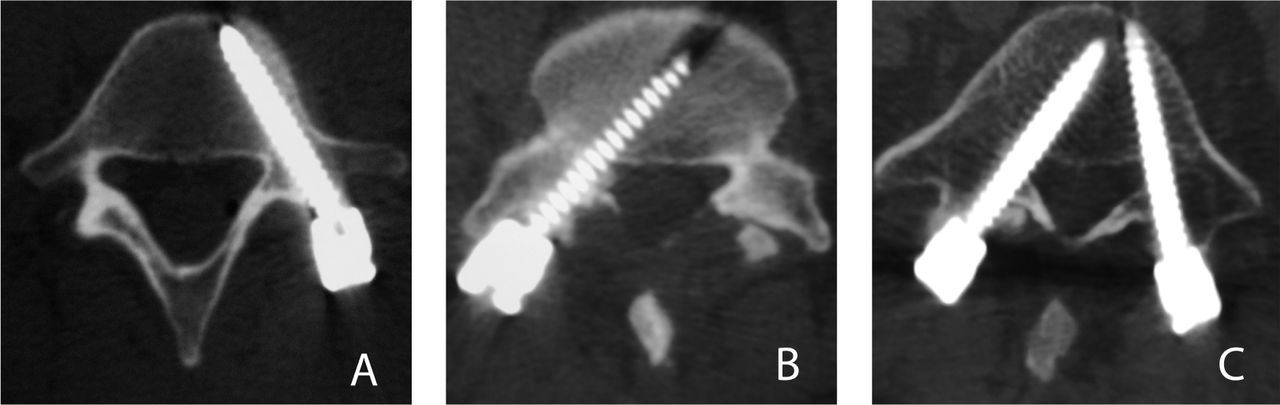
Postoperative axial CT image depicting the classification used for accuracy assessment. A. No breach. B. Minor breach ≤2 mm. C. Major breach ≥3 mm.
Operative technique
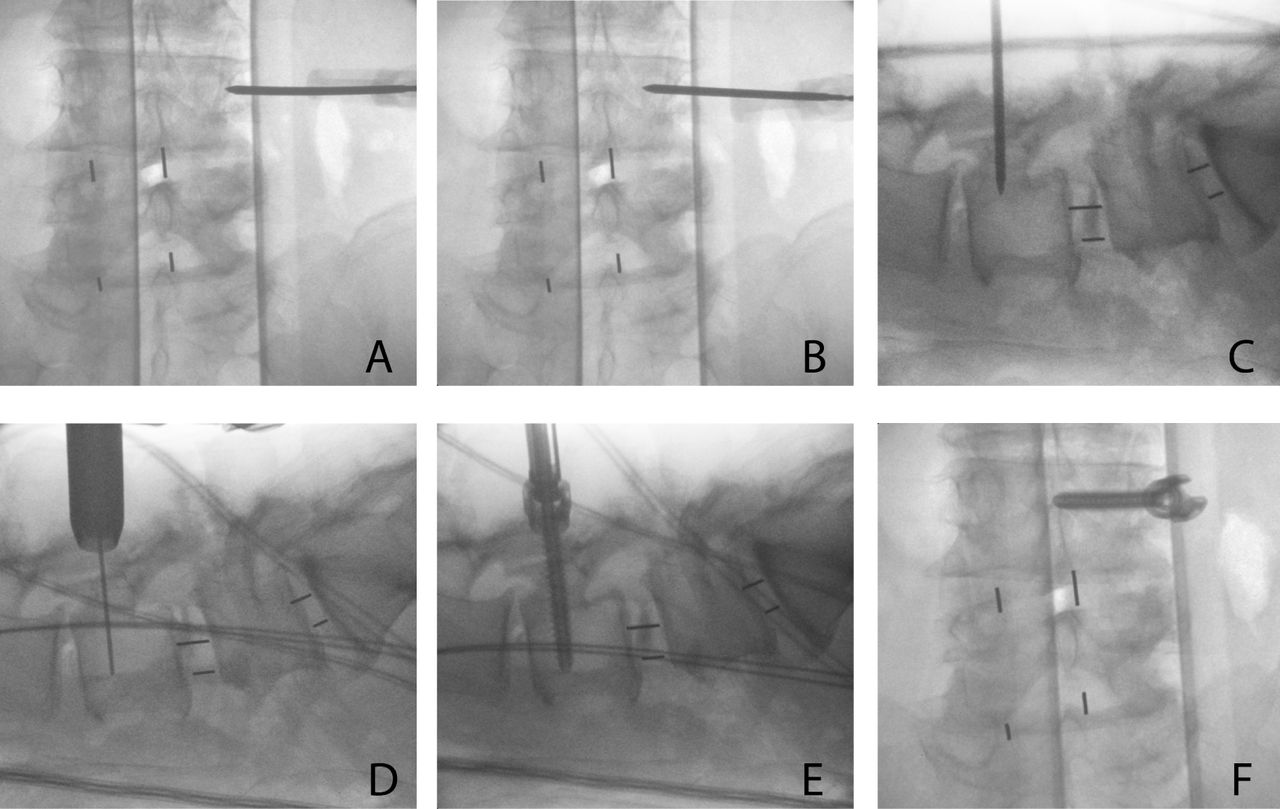
All of the cases were performed under general anesthesia using a radiolucent operating table, a 2-D C-arm fluoroscope, electromyography (EMG), somatosensory evoked potentials, and motor evoked potentials. Following intubation, patient was placed in prone position; the lumbar spine was prepared and draped in sterile fashion. We used a 2 cm incision that was 1.5 cm lateral to the ipsilateral pedicle marked by AP fluoroscopy. Monopolar dissection was made through the subcutaneous tissue. The thoraco-lumbar fascia and muscle erector spinae fascia was opened and the plane between the iliocostalis and the longissimus muscles was identified. A 16 to 18 mm tubular retractor (METRx System, Medtronic) was inserted in between the muscles by dilating over a precisely placed guide tube over the facet joint. The facet complex was drilled out with a straight high-speed match head cutting drill. Discectomy and MISS-TLIF were performed using Peek cages (JULIET OL, Spineart) filled with demineralized bone matrix. Following decompression and interbody fusion, fluoroscopic guided pedicle screws were placed using the true AP and lateral views technique. Jamshidi needle was introduced with the true AP view at the most lateral part of the elliptical pedicle (Figure 2A); the needle was introduced until the medial border of the pedicle was reached (Figure 2B). Fluoroscopic lateral view was obtained to confirm that the tip of the needle was beyond the pedicle, anterior to the spinal canal (Figure 2C). The Jamshidi needle was introduced deep into the vertebral body. The guide wire was introduced inside the Jamshidi needle (Figure 2D), the path was prepared with the tap and finally the screw was placed confirming the final position with lateral and AP views (Figure 2E, Figure 2F). Jamshidi needle and screws were introduced using a stimulation threshold according to previous stimulation series reported in the literature.9–11 In case of occurrence of root irritation related to the insult of the medial wall of the pedicle, the surgeon was alerted. A stimulus intensity of 7 mA was applied to the top during the introduction of the Jamshidi needle. This stimulus was increased to 15 mA while placing the screws. If there was any response to stimulation during surgery, screw was moved over and placed in a different position and trajectory. The rod was secured through the same incision. When contralateral fixation was needed; the screws were placed using a mini-open contralateral approach.

Fluoroscopic-guided screw placement technique using the true AP and lateral views.
Statistical Analysis
Statistic analysis was performed with IBM SPSS Statistics Software version 20.0. The accuracy was examined according to the spinal levels that were treated. Pedicle breach rates were analyzed in terms of occurrence and as the degree of breach: no breach, minor (≤ 2 mm) or major (≥3 mm) breach. Kappa coefficient was calculated for testing inter-observer agreement. Kappa coefficients were interpreted as follows: Almost perfect agreement >0.81, substantial agreement 0.61-0.80, moderate agreement 0.41-0.60, fair agreement 0.21-0.40 and slight agreement 0.01-0.20.12
Results
In 125 patients, a total of 470 transpedicular screws were assessed between the levels of T-12 and S-1. Clinical follow up and postoperative CT were performed to all the patients. In 57 patients the instrumentation was bilateral and in 68 unilateral. Kappa analysis was performed to ascertain the degree of agreement for screw accuracy classification (No breach/Minor breach ≤2 mm/Major breach ≥3 mm) between the three observers. A substantial degree of agreement was found between the observers A-B (κ=0.769) and A-C (κ=0.784) and almost perfect agreement between observers B-C (κ=0.928). Table 1 shows the breached pedicle results, screws and percentages are expressed as the mean of the three observers.
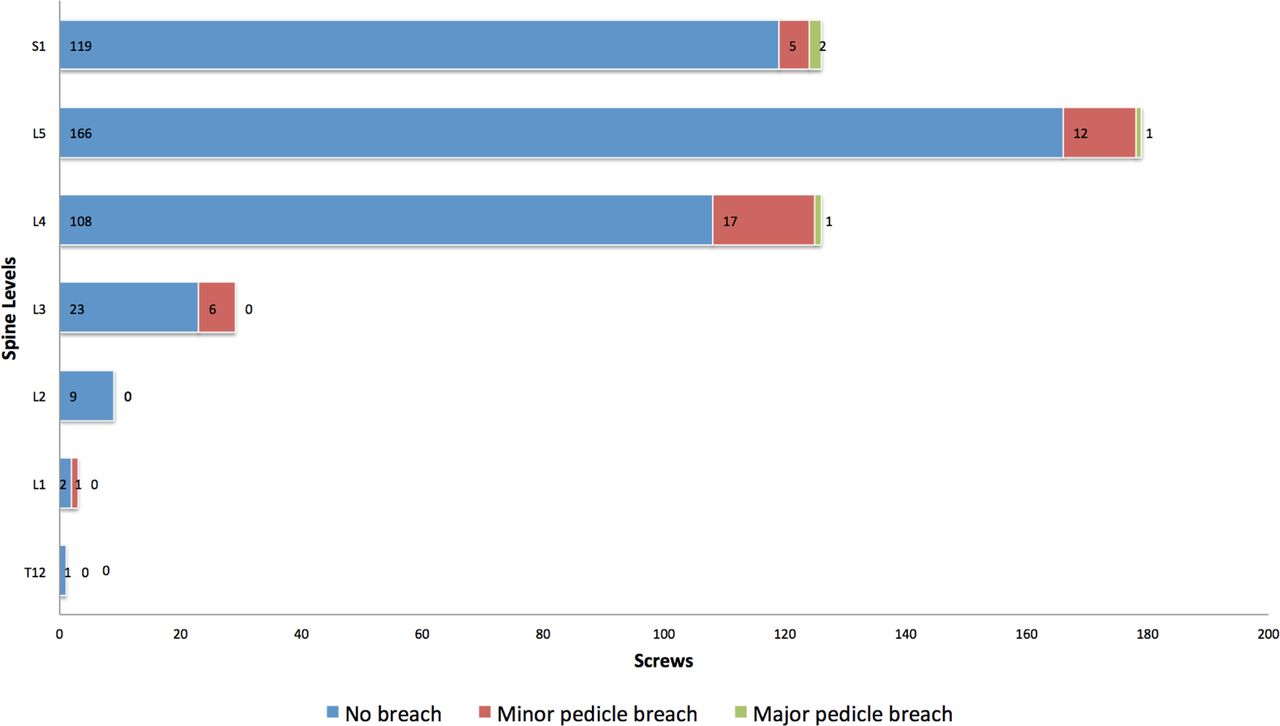
There were a total of 427.33 (90.92%) screws without breach, 39.33 (8.37%) minor breached pedicles and 3.33 (0.71%) major breached pedicles (Figure 1); of the 125 patients, 31 patients (26.4%) had a pedicle breach. The incidence of pedicle breach per level using observer C (Figure 3) results was as follows: L-2 0/9 (0%), L-3 6/29 (20.68%), L-4 18/125 (14.4%), L-5 13/178 (7.30%), S-1 7/124 (5.64%). There was one screw in L-1 with a minor medial breach; the other two cases at T-12 and L-1 did not have any breach. Trajectory pedicle breach percentages were as follows: minor medial pedicle breach 4.68%, minor lateral pedicle breach 3.47%, minor inferior pedicle breach 0.22%, and major medial breach 0.70%. There were only three major medial pedicle breaches for two observers (L-5 and S-1) and four for the other observer (L-4, L-5, S-1), all of them measured less than 5 mm. Right breach pedicles (26/57.77%) were more common than left (19/42.22%).
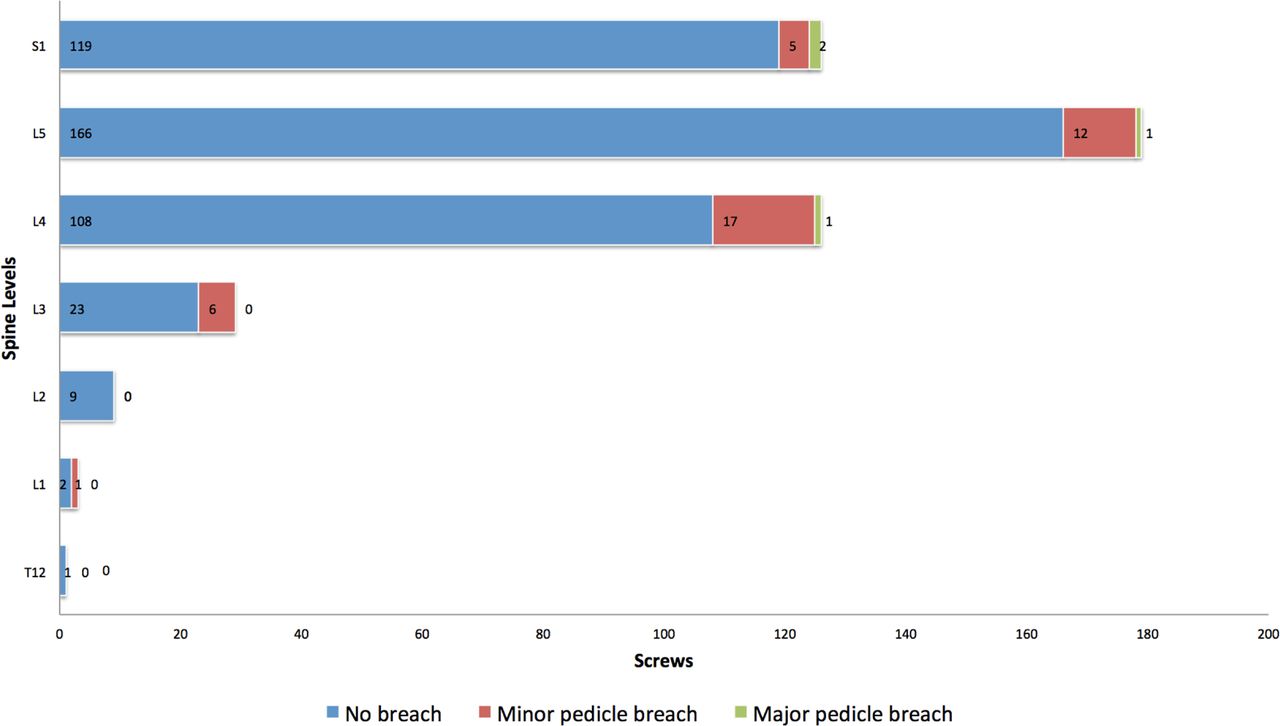
Stacked bar graphdemonstrating the number of pedicles without pedicle breach, minor pedicle breach and major pedicle breach at each level.
No intraoperative instrumentation-related or postoperative clinical complications were encountered. From the major breached cases (0.71%), no one had nerve root injuries or required screw surgical revision.
Discussion
Although surgical anatomy remains the key factor for pedicle screw placement success, minimally invasive techniques rely on mastering radiological spine anatomy. Our mini-open technique utilizes 2-D fluoroscopy for radiological visualization of the pedicle and the aid of electrophysiological monitoring for the accurate placement of transpedicular screws.
In previous studies, using fluoroscopic guidance in two planes, Castro et al.13 reported a pedicle breach of 40% using open landmarks, however most of them were minor (less than 2 mm). Parker et al.10 used a free-hand technique with an intraoperative lateral radiography achieving a pedicle breach of only 1.7%. Nevertheless, this percentage is not comparable because this study defined breach as more than 25% of the screw diameter. MISS techniques under 2-D fluoroscopic guidance had a pedicle breach from 2.38% to 29.48%.8, 14–23 Malham G.M. et al.14 reached 97.5% pedicle screw accuracy using dynamic EMG and 2-D fluoroscopy; 99% of 201 screws were found to be within the margins of the pedicle when EMG response was negative to a stimulus ≥ 11 mA. In our results, the pedicle breach rate was 9.08% of 470 screws using a stimulus intensity of 7 mA during the Jamshidi needle introduction and 15 mA while placing the screw. If there was any response to stimulation, screw was placed in a different trajectory. In comparison with navigation-aided pedicle screw placement in which the accuracy is between 92.5-97.3%,24–29 our study had a high radiological accuracy (90.92%) just below these studies. No clinical complications were encountered, which is similar to the symptomatic breach rate of 0.2% reported with lumbar percutaneous pedicle screw placement using 3-D stereotactic navigation.30 Even though surgeon's radiation exposure and pedicle breach are markedly reduced with 3-D CT or fluoroscopy-navigation methods, they have a significant equipment cost limitation, incapability to get real-time location of guide wires in the vertebral body, radiation exposure to the patient is increased 31 and clinical outcome benefits have not been definitively demonstrated.
Robot-assisted pedicle screw insertion is a new safe and useful tool for the spine surgeon.32–36 A multicenter retrospective series found 89.3% of screws without breach and 9% with a minor breach using the SpineAssist Surgical Robot. Higher rate of laterally misplaced screws were found in two studies35, 36 and in one of them, conventional placement had superior accuracy than robot-assisted screws.35 The main advantages of the robotic-assisted system are that it does not rely on bony landmarks or camera tracking mechanisms. However, in some cases screw trajectory had to be revised manually and fluoroscopy backup is necessary.36
The accuracy of pedicle screw placement using 2-D fluoroscopic guidance relies in radiologic-anatomy correlation. The pedicle is an ellipse with a vertical long axis in the AP projections, the width increases when progressing from L1 to S1, becoming an oblique ellipse at L-4 and L-5 and a triangle at S-1. The radiological pedicle is within the true cortical border of the pedicle, which gives a safety cortical pedicle halo for the accurate placement of the screw.37 Mastering radiological anatomy of the pedicles is of utmost importance, especially in deformity cases in which the angles and anatomy are modified. S-1 pedicles are not always well observed with fluoroscopy; it is important to localize the medial cortical border, which is the continuation of a trabecular line that forms de sacroiliac joint, and the lateral cortical border, which is always lateral to the S-1 foramen.37
One of the main disadvantages for our technique is the surgeon's radiation exposure. However the major pedicle breach rate (0.71%) was very low because fluoroscopy guidance was used meticulously in every step for the screw placement and neuromonitoring was carefully interpreted. Even though we know the thresholds are variable, the combine use of intensive fluoroscopy with neuromonitoring gives excellent clinical results without complications.
Conclusion
Our study demonstrated a high accuracy (90.2%) for 2-D fluoroscopy-guided pedicle screw using electromonitoring. Only 0.71% of the 470 screws had a major breach. No clinical complications were documented. Knowing the radiological spine pedicle anatomy and the correct interpretation of EMG are the key factors for this technique.
Author contributions to the study and manuscript preparation include the following. Conception and design: Soriano-Sánchez. Acquisition of data: Ortega-Porcayo, Gutiérrez-Partida, Ortíz-Leyva, Ramírez-Barrios. Analysis and interpretation of data: Soriano-Sánchez, Ortega-Porcayo, Sánchez-Escandón. Drafting the article: Ortega-Porcayo. Critically revising the article: Soriano-Sánchez, Ortega-Porcayo, Gutiérrez-Partida, Ortíz-Leyva, Ramírez-Barrios, Rodríguez-García, Sánchez Escandón.vReviewed submitted version of manuscript: Soriano-Sánchez, Ortega-Porcayo, Gutiérrez-Partida, Ortíz-Leyva, Ramírez-Barrios, Rodríguez-García. Sánchez-Escandón Approved the final version of the manuscript on behalf of all authors: Ortega-Porcayo.
Disclosures
No funding, financial support or industry affiliations were used for this work.
- Copyright © 2015 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.