


ABSTRACT
Background: Low back pain (LPB) is the main cause of disability worldwide with enormous socioeconomic burdens. A major cause of LBP is intervertebral disc degeneration (IDD): a chronic, progressive process associated with exhaustion of the resident cell population, tissue inflammation, degradation of the extracellular matrix and dehydration of the nucleus pulposus. Eventually, IDD may lead to serious sequelae including chronic LBP, disc herniation, segmental instability, and spinal stenosis, which may require invasive surgical interventions. However, no treatment is actually able to directly tackle IDD and hamper the degenerative process. In the last decade, the intradiscal injection of stem cells is raising as a promising approach to regenerate the intervertebral disc. This review aims to describe the rationale behind a regenerative stem cell therapy for IDD as well as the effect of stem cells following their implantation in the disc environment according to preclinical studies. Furthermore, actual clinical evidence and ongoing trials will be discussed, taking into account the future perspective and current limitations of this cutting-edge therapy.
Methods: A literature analysis was performed for this narrative review. A database search of PubMed, Scopus and ClinicalTrials.gov was conducted using “stem cells” combined with “intervertebral disc”, “degeneration” and “regeneration” without exclusion based on publication date. Articles were firstly screened on a title-abstract basis and, subsequently, full-text were reviewed. Both preclinical and clinical studies have been included.
Results: The database search yielded recent publications from which the narrative review was completed.
Conclusions: Based on available evidence, intradiscal stem cell therapy has provided encouraging results in terms of regenerative effects and reduction of LBP. However, multicenter, prospective randomized trials are needed in order confirm the safety, efficacy and applicability of such a promising treatment.
- intervertebral disc degeneration
- stem cell
- disc regeneration
- intradiscal injection
- mesenchymal stem cells
INTRODUCTION
Low back pain (LBP) is the leading cause of disability worldwide and is estimated to affect up to 80% of individuals at least once in a lifetime.1 The prevalence of activity-limiting LBP is low during childhood but steeply increases with adolescence, when approximately 40% of teenagers experience an episode of LBP.2 However, LPB becomes significantly more common with aging, peaks in midlife and mainly affects the female and working populations.3 The social burden of LBP is enormous: the Global Burden of Disease study calculated that LBP alone was responsible for about 60.1 years lived with disability, an increment of more than 50% compared to 1990.4 As a consequence, economic costs associated with the treatment of LBP account for a large portion of healthcare expenses. In 2018, approximately $90 million were spent in the United States for the diagnosis and management of LBP alone, with spinal fusion accounting for 7.1% of costs of hospital stays among all inpatient procedures.5
A major cause of LBP is intervertebral disc degeneration (IDD): a chronic, progressive process associated with aging,6 genetic predisposition,7 smoking,8 diabetes,9 overweight,10 and additional risk factors (ie, heavy physical labor or inactivity, atherosclerosis of spinal vessels, inflammatory diseases11). During IDD, the increased catabolic activity along with the gradual reduction of functional cells (due to both cell apoptosis and the acquisition of a defective senescent phenotype) of the intervertebral disc (IVD) dramatically reduces its capacity to produce an adequate amount of extracellular matrix (ECM) and preserve its structural integrity.12 As a consequence, dehydration of the nucleus pulposus (NP) occurs with subsequent reduction of disc height and shock-absorbing capacity, thus leading to transmission of circumferential forces to the annulus fibrosus (AF) eventually resulting in AF tears which predispose to discogenic LBP, herniations and further degenerative changes.13
To date, the treatment of LBP and its sequelae remains an unsolved challenge, as neither conservative nor surgical strategies can directly tackle IDD. Therefore, a strenuous research effort is being made to develop minimally invasive approaches to hamper IDD or, ideally, regenerate the IVD. The use of stem cell–based treatments has been extensively investigated during the last 2 decades with promising results at both preclinical and clinical levels.14
The purpose of this review is to outline the rationale of a stem cell–based therapy for IDD and to discuss the main biological and clinical outcomes depicted by recent studies on the topic. Furthermore, principal limitations of this approach and challenges in the near future will be debated.
THE RATIONALE OF A STEM CELL–BASED THERAPY FOR IDD
During IDD, the number of healthy resident cells progressively decreases, with catabolic events predominating over normal tissue anabolism.15 Stem cells are undifferentiated cells able to self-renew and proliferate producing committed, differentiated elements that renovate the cell pool in a specific tissue. To date, stem cells have been isolated from several tissues where they reside in specialized microenvironments defined as niches.15 Therefore, stem cells can be harvested from multiple sources and transplanted into host tissues where they may differentiate into mature cells, secrete growth factors and cytokines to support resident cell activity, and/or recruit local progenitor cells to induce endogenous repair of the degenerated IVD.14 Nonetheless, these cells should be able to survive in the harsh degenerative IVD microenvironment, which is characterized by hypoxia, low glucose levels, acidic pH, hyperosmolarity, inflammation, and mechanical loading.15
In order to exert a direct local effect and considering the avascular nature of the IVD, the main route of stem cell transplantation adopted in most studies is through a minimally invasive transannular intradiscal injection. Although considered reasonably safe, AF puncture has been shown to promote IDD as well as to increase the risk of disc herniation and endplate changes both in preclinical16 and clinical studies.17 Therefore, an alternative transpedicular route to access the NP without violating the AF has been proposed for the administration of therapeutic agents inside the IVD.18 However, a recent study from Decante and colleagues19 showed that both the transannular and the transpedicular approaches induced IDD as demonstrated by magnetic resonance imaging (MRI) and histological analysis in an ovine model. In addition, the transpedicular approach caused persistent endplate defects, with Schmorl-like herniations and osseous displacement within the NP. For this reason, further studies are needed to define the best route to safely approach the IVD in the clinical setting.
The application of several types of stem cells for IVD regeneration has been described in the literature, including mesenchymal stem cells (MSCs), induced pluripotent stem cells (iPSCs), embryonic stem cells, muscle-derived stem cells, hematopoietic stem cells, and olfactory mucosa stem cells.20 These cells may be transplanted either in an undifferentiated state, following an in vitro preconditioning and/or predifferentiation using diverse biological stimuli (e.g., growth factors, biomaterials, signaling molecules, IVD-like nutrition conditions) or modified to overexpress specific markers to achieve a discogenic phenotype before implantation.21–25 In the near future, the use of clustered regularly interspaced short palindromic repeat (CRISPR) genome editing may open new possibilities by directly inhibiting the expression of cytokine receptors or senescence markers or increasing the expression of matrix proteins in MSCs.26
MSCs harvested from the bone marrow (BM-MSCs) and the adipose tissue (adipose-derived stem cells [ADSCs]) are the most widely investigated cell types for several reasons, including the ease of harvest, the extensive availability, the differentiation capacity into IVD-like cells, and the anabolic and anti-inflammatory potential in the site of transplantation. Although belonging to the same lineage, BM-MSCs and ADSCs are characterized by different biological properties and diverse responses to the IVD microenvironment that have been outlined by recent investigations.15 BM-MSCs have been demonstrated to better tolerate the hypoxic IVD environment as low O2 upregulates the hypoxia-inducible factor 1α and yes-associated protein pathways resulting in increased proliferation, stemness preservation, and protection from apoptosis.27,28 On the other hand, in a recent in vitro study conducted by Binch and colleagues,29 ADSCs cultured in an IDD-mimicking media (5% O2 and preconditioning with a proinflammatory stimulus) showed significantly higher levels of pain-associated neurotrophic and angiogenic factors in ADSC cultures compared to BM-MSCs, which may in turn promote neurovascular invasion of the degenerated IVD and thus contribute to discogenic LBP. However, when cultured in IVD-like hyperosmolar conditions (400 mOsm), ADSCs have demonstrated a higher expression of NP cell differentiation markers as well as ECM components through epigenetic regulation.30
Recent studies have identified a population of progenitor cells exhibiting MSC markers and properties within the AF, the NP, and the cartilaginous endplates in both healthy and degenerative IVDs.31 These cells are characterized by the specific expression of angiopoietin-1 receptor and diasiloganglioside 2 and have showed a higher proliferative capacity in hypoxic and acidic conditions and an increased chondrogenic differentiation potential compared to other MSCs in vitro.32 Rather than a source for stem cell harvest and subsequent transplantation, IVD progenitor cells may be involved in endogenous tissue repair upon activation, recruitment, and nucleopulpogenic differentiation under the stimulus of growth factors, chemokines, and cytokines released by locally injected stem cells.14
iPSCs are pluripotent, highly proliferating stem cells that are directly generated from somatic mature cells through genetic reprogramming in order to acquire a specific phenotype.33 In several studies, iPSCs have been successfully reprogrammed in vitro towards NP-like,34 notochordal cell–like,35 or MSC-like phenotypes36 able to express NP-specific markers and support resident cells both in vitro and in vivo. However, the high costs required by genetic manipulation and safety concerns regarding iPSC tumorigenesis potential still limit their application in the clinical setting.
THE EFFECT OF STEM CELLS IN THE DEGENERATIVE IVD ENVIRONMENT
Differentiation Into IVD-Like Cells
The acquisition of a NP-like phenotype and the consequent capacity to synthesize novel ECM has been originally proposed as the most likely regenerative effect of stem cells after intradiscal implantation. This capacity has been demonstrated by several preclinical studies,37–39 although prolonged cell survival in the hostile IVD microenvironment remains controversial. Indeed, several in vitro and in vivo reports have showed that stem cells become rapidly undetectable soon after or a few weeks following transplantation as a consequence of nutrient deprivation and low pH as well as due to the pressure generated during the procedure itself.37,38,40 In a recent study from Henriksson et al,41 iron sucrose–labelled autologous BM-MSCs were injected in the IVDs of 4 patients subsequently undergoing discectomy and fusion surgery. The results showed that viable MSCs and their progeny were retrieved in harvested IVD tissues up to 8 months postinjection as both large cell clusters and solitary cells.
Support of Resident Cell Activity
According to numerous preclinical studies, stem cells are able to stimulate resident IVD cells through the secretion of several growth factors, chemokines, ECM components, and anti-inflammatory mediators via a paracrine mechanism. Indeed, several in vitro investigations42 have reported that the MSC coculture with NP cells was associated with an increase of cell proliferation and ECM synthesis,43,44 with a reduction of cell senescence and metalloproteinase levels. In a recent study from Hingert et al,45 a secretome analysis conducted on BM-MSC conditioned media revealed 753 unique peptides, mostly represented by ECM proteins (20.16%), enzymes (22.48%), glycoproteins and proteoglycans (12.4%), and growth factors and their modulators (6.98%, including vascular endothelial growth factor, bone morphogenetic protein 1, connective tissue growth factor, insulin-like growth factor binding protein, metalloproteinase inhibitors, antiapoptotic factors, and several more. Furthermore, when cultured in hypoxic conditions (5% O2), BM-MSCs have shown an incremented expression of genes involved in chondrogenic differentiation (ACAN, KRT19, BARX1), immunomodulation (CXCL5, SFN), and cell survival and proliferation (GPX3, TXNIP) compared to BM-MSCs cultured under atmospheric O2.46
In an investigation from Chen et al,47 BM-MSCs and NP cells were cocultured under static mechanical loading. Compared to NP cells alone, BM-MSCs significantly reduced compression-induced NP cell apoptosis in the coculture group via the inhibition of the mitochondrial pathway. Indeed, BM-MSCs decremented reactive oxygen species (ROS) and proapoptotic marker (caspase-3, caspase-9, cytochrome c) levels and maintained mitochondrial membrane potential and integrity.47
Furthermore, MSCs may improve the mechanical properties of NP cells by directly reducing cellular and matrix stiffness. Indeed, Liu and colleagues48 have shown that the coculture of MSCs with degenerated NP cells significantly decreased the mechanical moduli of the latter, while increasing cell proliferation and both collagen type II and aggrecan expression. These changes were associated with the upregulation of stromal cell–derived factor-1 and its receptor, CXC receptor 4, which have been previously correlated with stem cell migration and homing.
The anabolic and anti-inflammatory effects of MSCs may not be restricted to the IVD only but could also positively affect surrounding tissues. In a study from James et al,49 the intradiscal injection of MSCs following a stab AF lesion in an ovine model prevented fibrotic and adipose tissue deposition within the multifidus muscle, whilst increasing the levels of tumor necrosis factor-α (TNF-α) and transforming growth factor β at the site of injury.
Immunomodulation
During IDD, several proinflammatory cytokines secreted by IVD resident cells and immune system cells foster ECM breakdown and promote chemotaxis, neoangiogenesis, and the release of additional cytokines, thus perpetrating the inflammatory response.50 The main mediators involved in this process include several interleukins (IL; among which IL-1β plays the most important role), TNF-α, interferon-γ, prostaglandin E2, and multiple chemokines.51,52 Collectively, these molecules are able to trigger cell apoptosis, senescence, and autophagy as well as upregulating the release of numerous metalloproteinases, including the matrix metalloproteinases and the a disintegrin and metalloproteinase with thrombospondin motifs families, as well as ROS.50 Furthermore, inflammation may significantly affect MSC metabolic activity, differentiation, and viability. In a recent study from Borem et al,53 ADSCs and amnion-derived MSCs were cultured under proinflammatory conditions with or without the supplementation of IL-1β and TNF-α. While the former showed increased proliferation with upregulation of proinflammatory cytokines and enhanced osteogenesis, the latter displayed an increment of anti-inflammatory cytokines and improved chondrogenesis. In addition, exposure to inflammatory stimuli in vitro has been demonstrated to reduce the expression of aggrecan and SOX9 and to increase cell apoptosis in NP-MSCs, as well as promoting neurogenic differentiation which may contribute to IVD reinnervation and the development of chronic LBP.54
However, previous studies have also demonstrated that MSCs are capable of secreting anti-inflammatory cytokines, anticatabolic mediators, and growth factors when cultured under IDD-like conditions both in vitro55 and ex vivo,56 hence demonstrating an immunomodulatory effect on resident IVD cells. According to recent investigations, MSCs may exert this anti-inflammatory effect by primarily inhibiting the p38 mitogen-activated protein kinase signaling pathway.57 Furthermore, BM-MSCs have been shown to tackle mitochondrial damage subsequent to increased oxidative stress through mitophagy, even if this response was effective only at an early stage, with prolonged oxidative exposure causing apoptosis.58 Therefore, mitophagy may be a key factor in protecting MSCs from the hostility of the degenerative microenvironment.
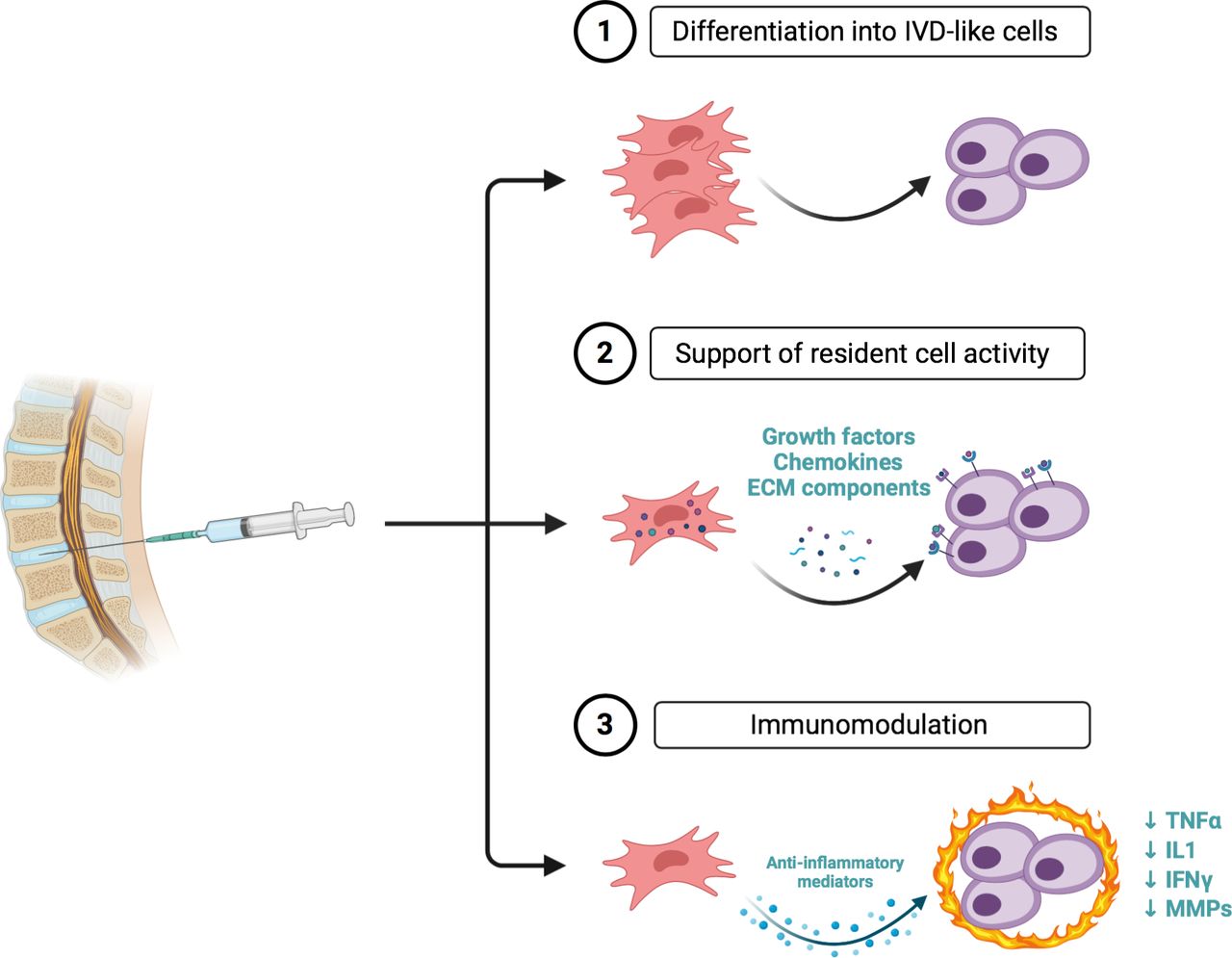
A summary of the regenerative effects of stem cells following transplantation in the disc environment is depicted in Figure 1.

The main effects of stem cells following transplantation into the intervertebral disc. IVD, intervertebral disc; ECM, extracellular matrix; TNFα, tumor necrosis factor-α; IL, interleukin; IFN, interferon; MMP, matrix metalloproteinase. Created with BioRender.com.
CURRENT CLINICAL EVIDENCE
The consistent body of preclinical research investigating the use of stem cells for IVD regeneration has provided the basis for several clinical studies with promising results. Safety and feasibility of this approach have been validated in 7 cohort studies59–66 on individuals affected by discogenic LBP (≥ stage II according to Pfirrmann grading) not responsive to standard conservative treatments. Cell sources used in these studies included autologous ADSCs62, ADSCs from the stromal vascular fraction (SVF),63 bone marrow aspirate concentrate (BMAC),60,61 and autologous59,65 and allogeneic64 BM-MSCs and allogeneic mesenchymal precursor cells (MPCs)66 at a highly variable concentrations (10–60 × 106 in 1–3 mL) and delivered via a fluoroscopic-guided transannular intradiscal injection. Collectively, most patients (65.4%) reported an improvement in Oswestry disability index (ODI) and visual analogue scale (VAS) throughout a follow-up of 6–72 months and in one study,60 30.77% of patients reported an improvement of ≥ 1 Pfirrmann grade at 12 months. None of these studies reported serious adverse events.26 However, the low number of participants (5–26) and the high variability in cell source and concentration across the aforementioned studies must be taken into account.
The first clinical investigation reporting the results of an intradiscal injection of autologous BM-MSCs was performed by Orozco and colleagues.59 In this pilot phase I study, the authors included 10 patients affected by LBP not responsive to conservative treatment for ≥ 6 months associated with 1- or 2-level IDD with intact AF as demonstrated by discography. Following inclusion in the study, patients underwent bone marrow harvesting from the iliac crest. BM-MSCs were then isolated and expanded in vitro until passage 3. Subsequently, 3–4 weeks after the first procedure, patients received an intradiscal injection of BM-MSCs (10 ± 5 × 106 per disc) under slight sedation and were discharged 2 hours later. Patients were reevaluated at 1 week and at 3, 6, and 12 months after the injection. LBP and associated disability were assessed at each follow-up visit using the VAS and ODI scales. Disc height and hydration were examined at 6 and 12 months with MRI. Both VAS and ODI were significantly reduced at 3 months following MSC transplantation, with a modest additional improvement at 6 and 12 months and a reported efficacy of 71%. No relevant change of disc height was noted, although NP water content was significantly increased at 12 months. No adverse reactions were reported. Despite the small number of patients, the absence of a control group, and the short follow-up, this study demonstrated for the first time that BM-MSC intradiscal transplantation was a safe procedure with a promising role for the treatment of IDD.
Pettine et al60,61 conducted a prospective nonrandomized cohort study including 26 patients affected by chronic LBP unresponsive to conservative treatment with a modified Pfirrmann score of 4–7 at MRI. According to the number of levels involved, patients were divided in 2 groups receiving 1- or 2-level intradiscal injection. Differently from other studies, the authors proposed a 1-stage procedure with bone marrow harvesting, intraoperative processing and production of BMAC, and intradiscal transplantation. Patients were reviewed at 3, 6, 12, and 24 months; VAS and ODI were assessed at each follow-up visit. MRI was obtained at 12 months and the Pfirrmann score of treated IVDs was recalculated. The results showed that BMAC was able to reduce pain and disability at each time point (71% VAS and 64% ODI improvement at 2 years), with approximately 30% of patients reporting an improvement of the Pfirrmann score at follow-up MRI.61 Five patients did not respond to the treatment and 2 of these underwent a reinjection at 6 months, with a significant improvement at 12 months. No adverse events, including heterotopic ossifications or osteophyte development, were noted. Reported total nucleated cell concentration was 121 ± 10 × 106/mL, although less than 0.005% expressed MSC phenotypic markers. Nonetheless, patients receiving a higher number of cells experienced a significantly faster and greater reduction of ODI and VAS. Compared to autologous or allogeneic expanded MSCs, the use of BMAC was associated with reduced operative time, decreased costs and risks of infection, disease transmission, or simple mismatch.60 However, as stem cell quantity and quality in BMAC largely depend on individuals' age and harvesting procedure, it is not possible to generalize the results and to compare them with other studies using MSCs alone.67
Elabd and coauthors65 performed a long-term safety and feasibility study on 5 patients undergoing single-level intradiscal injection of autologous BM-MSCs. Individuals with LBP not responsive to conservative treatment for ≥ 3 months associated with IDD and/or a positive provocative discography were included. Before receiving the injection, bone marrow was obtained and BM-MSCs were isolated and cultured in hypoxic conditions (5% O2). On the day of the procedure, BM-MSCs were resuspended in autologous platelet lysate until reaching a volume of 0.25–1 mL. Cell number significantly varied among the participants (15.1–51.6 × 106). Patients were reviewed at 4–6 years with a physical examination, an MRI, and a quality-of-life questionnaire. The majority of patients reported an improvement in quality of life, strength, and mobility, as well as an apparent reduction of disc protrusion. However, the restricted sample size, the lack of validated endpoint measurements, and the absence of intermediate time points significantly limit the outcomes of the study.
Kumar et al62 conducted another single-arm phase I clinical trial including 10 patients with LBP not responding to conventional treatment for ≥ 3 months, signs of IDD (Pfirrmann score 3-4 at 1 or 2 levels), and discogenic etiology of LBP as confirmed by discography. Three weeks before injection, participants underwent abdominal liposuction; samples were then transferred to a laboratory were ADSCs were isolated and expanded in vitro until passage 3. ADSCs were then injected in the affected IVDs in combination with a hyaluronic acid (HA) derivative, namely 1% Tissuefill®. Two MSC doses were tested: 5 patients received 20 × 106 cells per disc and 5 patients received 40 × 106 cells per disc. Patients were reexamined at 1 week and at 3, 6, and 12 months after the injection, with VAS, ODI and Short Form 36 (SF-36) being evaluated at each time point and spine imaging (lumbar spine x-ray and MRI) at 1, 6, and 12 months. 6 of 10 patients were demonstrated to reach the final treatment success milestone (reduction ≥ 50% in VAS and ODI compared to pretreatment). No significant difference was found between the 2 doses. Additionally, no decrease in disc height and no change in Pfirrmann score were reported, with 3 patients showing signs of increased NP hydration at the final follow-up. As in previous studies, no adverse events were reported. Potential causes of treatment failure were evaluated in 4 patients, 2 of whom were overweight, 1 presenting with a L4–L5 grade I spondylolisthesis and facet joint arthritis, and another with depressive symptoms. Therefore, authors pointed out that accurate patient selection may be crucial for achieving success in intradiscal stem cell treatments.
In an open-label prospective study, Comella et al63 evaluated the effect of an intradiscal injection of autologous SVF blended with platelet-rich plasma (PRP) in patients with LBP not responsive to conservative treatment for ≥ 6 months due to 1-, 2-, or 3-level IDD as demonstrated by MRI. Patients enrolled underwent a 1-stage procedure with lipoaspirate harvesting, intraoperative SVF extraction, PRP preparation from a whole blood sample, and intradiscal injection of 1 mL SVF/PRP (containing circa 30–60 × 106 cells). Patient were evaluated at 2 and 6 months. Low back range of motion, VAS, ODI, present pain index (PPI), Beck depression inventory (BDI), Short Form McGill pain questionnaire (SM-MPQ), Short Form 12 (SF-12), and the Dallas pain questionnaire were assessed. Overall, patients reported increased lumbar flexion, significant reduction of VAS and PPI at 2 and 6 months, significant improvement of SM-MPQ and SF-12 at 6 months, and no statistically significant change of BDI and ODI. However, the notable variability in cell concentration and the short follow-up importantly limit the possibility to state the efficacy of this methodology for IVD regeneration.
The first randomized controlled trial (RCT) to evaluate the efficacy of an intradiscal stem cell therapy for IDD was conducted by Noriega and colleagues.64 In this phase I–II trial, 24 patients with chronic LBP unresponsive to conservative treatment for ≥ 6 months associated with 1- or 2-level IDD (Pfirrmann score 2-4) were randomly allocated to the experimental or the control group. The former received an intradiscal injection of allogeneic BM-MSCs (25 × 106 per disc), while the latter received a sham infiltration within the paravertebral musculature. Patients were followed up at 1 week and 3, 6, and 12 months after the injection. VAS, ODI, and SF-12 were assessed at each time point, and MRI was performed at 6 and 12 months. A significant improvement in VAS and ODI was documented in the control group at 3 months and was maintained until the last follow-up. Although no significant difference regarding disc height and water content was reported between the 2 groups, a statistically significant improvement in Pfirrmann score was encountered in treated disc.
Recently, Amirdelfan et al66 have reported the results of a multicenter RCT investigating the safety and efficacy of the intradiscal administration of stromal precursor antigen-3 (STRO-3)+ MPCs combined with HA. In this phase II study, 100 patients affected by chronic LBP (≥ 6 months) associated with 1-level moderate IDD (modified Pfirrmann score 3-6) were randomized to receive 6 × 106 MPCs with 1% HA, 18 × 106 MPCs with 1% HA, 1% HA only or sham. Patients were reviewed at 1, 3, 6, 12, 24 and 36 months following the injection. VAS, ODI, SF-36 and Work Productivity and Activity Index (WPAI) were evaluated at each timepoint, while MRI was performed at 6 months. Patients treated with intradiscal MPCs showed significant improvements in pain and function at various timepoints, although no apparent change in modified Pfirrmann score was evident among groups.
The characteristics of clinical investigations reporting the effect of MSCs for IVD regeneration are depicted in Table 1.
Previous cohort studies investigating the application of stem cells for intervertebral disc regeneration.
To date, 10 clinical trials using stem cells for IVD regeneration are ongoing (Table 2). Of these, 7 (NCT02412735,68 NCT03340818,69 NCT03692221,70 NCT03737461,71 NCT03461458,72 NCT04759105,73 EudraCT no. 2019-002749-4074) are RCTs with a control group receiving a sham injection, while the remaining 3 (NCT03912454,75 NCT04414592,76 NCT0449910577) are open-label cohort studies. Inclusion criteria generally admit adult individuals affected by chronic LBP not responsive to conservative treatments and with radiological evidence (mostly confirmed by MRI according to the Pfirrmann grading) of single or multilevel IDD. However, one of these studies (NCT0441459275) will evaluate the use of stem cells in patients with sciatica due to lumbar disc herniation following fully endoscopic lumbar discectomy. These clinical trials will test MSCs from various sources, including autologous BM-MSCs (NCT03692221,70 NCT04759105,73 EudraCT no. 2019-002749-4074), allogeneic BM-MSCs (NCT02412735,68 NCT0373746171) and autologous ADSCs (NCT0346145872), with 2 studies (NCT04414592,76 NCT0449910577) investigating the regenerative potential of allogeneic human umbilical cord mesenchymal stem cells. Cell concentration among the studies is highly variable (2–25 × 106 cells) and in one trial (NCT0241273568) MSCs will be delivered in a 1% hyaluronic acid solution instead of saline. Moreover, 2 trials (NCT03340818,69 NCT0391245475) will use BMAC. The objective of these studies is to evaluate the efficacy of an intradiscal transplantation of MSCs mainly in terms of safety and improvement of pain and disability. In addition, assessment of IVD structural changes with x-ray and MRI will be investigated, as well as the use of pain-relieving medications and variations of the patients' occupational status.
Ongoing clinical trials investigating the application of stem cells for intervertebral disc regeneration.
MAIN LIMITATIONS AND FUTURE PERSPECTIVES
IVD regeneration through the intradiscal administration of stem cells is an attractive approach with promising results as shown by preclinical and early clinical studies. However, several questions still remain unanswered.
Numerous animal studies have depicted the feasibility and the strong regenerative potential of the delivery of stem cells within the degenerated IVD. However, such results cannot be directly translated to humans due to multiple factors, including biomechanical considerations (quadrupeds versus bipeds); different IVD structure, size, and cellularity (higher representation of notochordal cells); and shorter lifespans and unphysiological onset of IDD in animals.26
Additional important issues to be addressed are the timing of the treatment from the pain onset, the stage of degeneration to treat, and dosing of implanted cells. Ideally, a regenerative approach is advisable at early stages of IDD, before the development of structural degenerative changes and the complete exhaustion of the local stem cell pool. A study from Maidhof et al78 evaluated the intradiscal administration of MSCs in a rat stab model at 3, 14, or 30 days postinjury in terms of cell fate and glycosaminoglycan synthesis. The results showed that cells transplanted at the earliest time point were retained inside the IVD while in other cases they tended to migrate out from the NP. In addition, MSCs administered at 3 days postinjury increased glycosaminoglycan content more significantly than at other time points. This suggests that MSCs transplanted at earlier stages of IDD may promote stem cell anabolism, while treating more advanced stages of degeneration may blunt the regenerative potential of this approach. Indeed, as IDD progresses, the disc microenvironment becomes increasingly harsher with severe repercussions on both resident and transplanted cells. The endplate undergoes progressive calcification with reduced nutrient diffusion and decreased levels of O2 and glucose. As a consequence, cell metabolism shifts to an anaerobic response, with higher levels of lactic acid and a gradual drop of the local pH. Increased acidity, together with lack of nourishment and tissue inflammation, gradually reduces cell viability and upregulates the expression of metalloproteinases favoring ECM breakdown and disruption of IVD microarchitecture, eventually leading to tissue damage and cellular overstress.15 In this regard, as IVD cell density is normally 2–3 × 106 cells/mL in a normal human disc, increasing local cell concentration by 10–20 times through MSC implantation would increase nutrient demand and ultimately result in competition with the remaining viable IVD cells for available metabolites. In the worst scenario, this would cause the majority of resident cells and implanted MSCs to die.26 Therefore, cell concentration should be carefully evaluated before injection based on the degree of IDD.
In addition, the diagnosis of discogenic LBP is intrinsically challenging as many patients suffer from LBP in absence of radiological signs of IDD, as well as many others who show even mild–advanced IDD at MRI but are completely asymptomatic.79 Therefore, additional studies are needed in order to refine the diagnosis of discogenic LBP and to identify candidates who would concretely benefit from IVD regeneration with stem cells.
Furthermore, as LBP may notoriously have a strong psychological component susceptible to the placebo effect,80 the results from multicenter, prospective RCTs are highly expected in order to define the exact contribution of the regenerative therapy on the perception of LBP. In this regard, the use of validated scales such as the Örebro musculoskeletal pain screening questionnaire and the STarTBack tool, which contain questions about pain duration, emotional distress, fear-avoidance beliefs, self-perceived functioning, and expected return to work, may help assess psychological and social factors that are linked with an understated or overstated response to the treatment.81
CONCLUSION
LBP due to IDD is a pandemic condition with ever-increasing economic and social burdens. IVD regeneration following stem cell transplantation has been proposed as a promising approach to revert degenerative changes owing to the capacity of stem cells to differentiate towards NP-like cells as well as their anti-inflammatory and anticatabolic effects. Several preclinical and early clinical studies have confirmed such proof of concept and provided encouraging results in terms of regenerative effects and LBP reduction, respectively. Definitive outcomes from RCTs are now highly expected in order to translate this innovative therapy from bench to bedside. More specifically, developing a safe approach, defining the optimal MSC source, and obtaining a sustained relief from LBP with improvement of disc hydration will be crucial points in the future establishment of a cell therapy for IVD regeneration.
Footnotes
Disclosures and COI: None declared.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
- 1 .↵
- 2 .↵
- 3 .↵
- 4 .↵
- 5 .↵
- 6 .↵
- 7 .↵
- 8 .↵
- 9 .↵
- 10 .↵
- 11 .↵
- 12 .↵
- 13 .↵
- 14 .↵
- 15 .↵
- 16 .↵
- 17 .↵
- 18 .↵
- 19 .↵
- 20 .↵
- 21 .↵
- 22 .
- 23 .
- 24 .
- 25 .↵
- 26 .↵
- 27 .↵
- 28 .↵
- 29 .↵
- 30 .↵
- 31 .↵
- 32 .↵
- 33 .↵
- 34 .↵
- 35 .↵
- 36 .↵
- 37 .↵
- 38 .↵
- 39 .↵
- 40 .↵
- 41 .↵
- 42 .↵
- 43 .↵
- 44 .↵
- 45 .↵
- 46 .↵
- 47 .↵
- 48 .↵
- 49 .↵
- 50 .↵
- 51 .↵
- 52 .↵
- 53 .↵
- 54 .↵
- 55 .↵
- 56 .↵
- 57 .↵
- 58 .↵
- 59 .↵
- 60 .↵
- 61 .↵
- 62 .↵
- 63 .↵
- 64 .↵
- 65 .↵
- 66 .↵
- 67 .↵
- 68 .↵
- 69 .↵
- 70 .↵
- 71 .↵
- 72 .↵
- 73 .↵
- 74 .↵
- 75 .↵
- 76 .↵
- 77 .↵
- 78 .↵
- 79 .↵
- 80 .↵
- 81 .↵
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Single cell RNA sequencing reveals shifts in cell maturity and function of endogenous and infiltrating cell types in response to acute intervertebral disc injury
- Allogenic bone marrow-derived mesenchymal stromal cell-based therapy for patients with chronic low back pain: a prospective, multicentre, randomised placebo controlled trial (RESPINE study)