


Abstract
Background Posterior fossa decompression (PFD) has been widely accepted for the surgical treatment for Chiari malformation type I (CM1). However, inadequate decompression causes surgical mortality and complications such as cerebrospinal fluid leakage, meningitis, or progression of syrinx and symptoms. The authors report a novel technique of PFD under navigation.
Methods Five female patients with CM1 who developed severe symptoms and underwent surgical treatment were evaluated (mean age 14.0 years; mean follow-up 1.3 years). Surgical outcomes, surgical time, intraoperative blood loss, and operative complications were assessed.
Results Four patients with CM1 who developed severe symptoms and underwent surgery were evaluated (mean age 14 years; mean follow-up 1.2 years). All patients were treated with PFD, C1 (and partial C2) laminoplasty to decompress the spinal cord under navigation guidance. Suboccipital craniectomy with 3 cm in diameter around the foramen magnum was performed. The postoperative radiograms and computed tomographic images showed adequate bony resection for CM1. Average surgical time was 114 minutes and average blood loss was 82 mL. There were no postoperative complications. After surgery, the numbness and muscle weakness of the patients were improved. The final follow-up magnetic resonance imaging displayed a good decompression of cerebral tonsile, and cervical syringomyelia was decreased.
Conclusions PFD under navigation guidance can reduce inappropriate decompression and may decrease a revision surgery. During decompression surgery, cerebrospinal fluid leakage can be prevented using an ultrasonic bone cutter and navigation.
Level of Evidence 5.
Introduction
Chiari malformation type I (CM1) has traditionally been defined as a downward herniation of the cerebellar tonsils of ≥5 mm through the foramen magnum.1 Incidence of CM1 in pediatric population is about 2%.2,3 Spinal cord syrinx is one of the most common comorbidities, with a reported occurrence of between 23% and 80%.3–6 Symptoms of CM1 are headache (74%), paresthesia (35%), cerebellar symptoms (23%), and dysphagia (21%).6 Most asymptomatic individuals with CM1 remained asymptomatic (93.3%) even in the presence of syringomyelia.6 However, if the patient has severe symptoms (eg, cough-associated headaches that impact the quality of life, large or enlarging syrinx), objective abnormal neurological findings or myelopathy, and cerebrospinal fluid (CSF) flow abnormalities, surgical intervention is indicated.7
Several surgical techniques such as posterior fossa decompression (PFD),8 tonsillectomy,9 and cerebrospinal fluid diversion10,11 are reported. PFD is the most popular and safe procedure, and its success rate was reported 83%.8 However, inadequate decompression caused surgical mortality in 1.3% of cases and complications (e.g., CSF leakage, meningitis, progression of syrinx and symptoms) in 22% of cases.12 To perform PFD precisely, intraoperative ultrasonic monitoring is recommended.13 In this technical note, we present a novel technique to utilize a navigation system and a ultrasonic bone cutter to perform PFD adequately and safely.
Methods
This study was approved by the ethics committee of our institute (No. 356). Necessary consents were obtained from the patients. All surgeries were performed at Okayama Rosai Hospital between August 2020 and August 2022. Five patients with CM1 who developed severe scoliosis or neurological deficit due to syringomyelia and underwent surgical treatment were evaluated retrospectively (mean age 13.5 years; mean follow-up 1.2 years). All patients were treated with PFD with outer layer of dural plasty. Surgical time, blood loss, complications, and surgical results of the patients were evaluated.
Results
Four patients with CM1 who developed severe symptoms and underwent surgery were evaluated (mean age 14 years; mean follow-up 1.2 years). All patients were treated with PFD, C1 (and partial C2) laminoplasty to decompress the spinal cord under navigation guidance. Suboccipital craniectomy with 3 cm in diameter around the foramen magnum was performed. The postoperative radiograms and computed tomography (CT) images showed adequate bony resection for CM1. Average surgical time was 114 ± 12 minutes, and average blood loss was 82 ± 51 mL. Preoperative symptoms of the patients were scoliosis (5/5), headache (3/5), muscle weakness (2/5), and numbness of hands (2/5). Postoperatively, all symptoms were improved but scoliosis. Three patients underwent second-stage scoliosis corrective surgery. One patient had postoperative epidural hematoma and needed revision surgery but had a full recovery after revision surgery (Table).
Summary of clinical results.
Case Presentation: Chiari Malformation Type 1
Patient History
A 13-year-old girl with scoliosis was referred to our orthopedic department with back pain and severe scoliosis. She was followed up at our department with a brace for 1 year. Recently, she had muscle weakness in both of her hands.
Physical Examination
She had cough-associated headaches. Her shoulder balance was horizontal, but her waist line was asymmetrical. Rib hump and hyperreflexia of bilateral legs were detected, and Babinski reflex was negative on both sides. The patient had slight muscle weakness in her right hand.
Preoperative Imaging
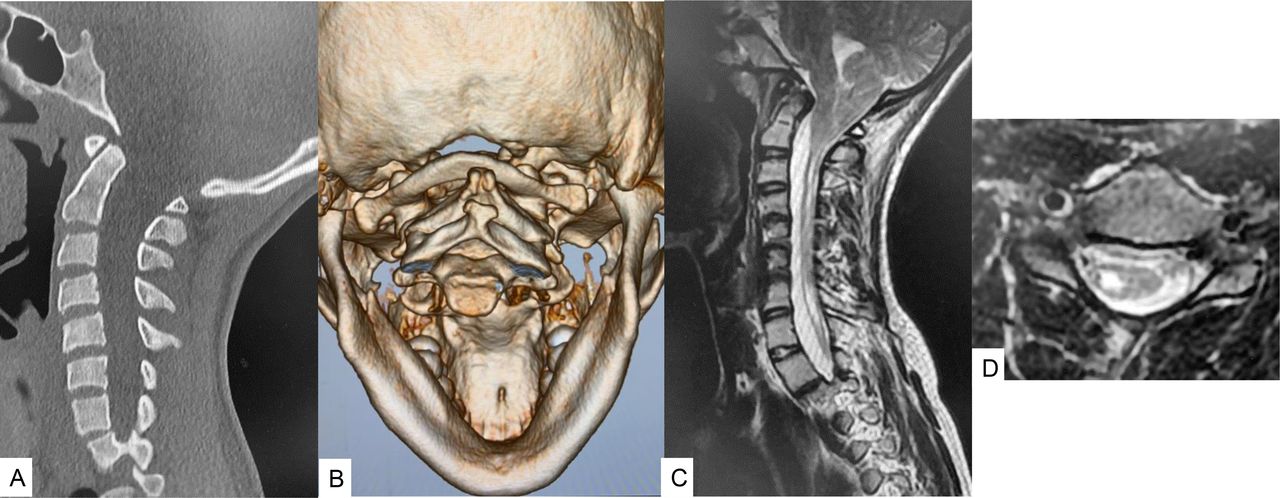
Radiograms at the initial visit demonstrated severe scoliosis (Cobb 45°), and bracing treatment was done. Scoliosis was also present in her cervical spine (Figure 1). Preoperative CT showed slight enlargement of C1 anteroposterior diameter (Figure 2). Magnetic resonance imaging (MRI) revealed downward migration of the cerebral tonsil into the foramen magnum and a syrinx in the cervical cord (Figure 2).
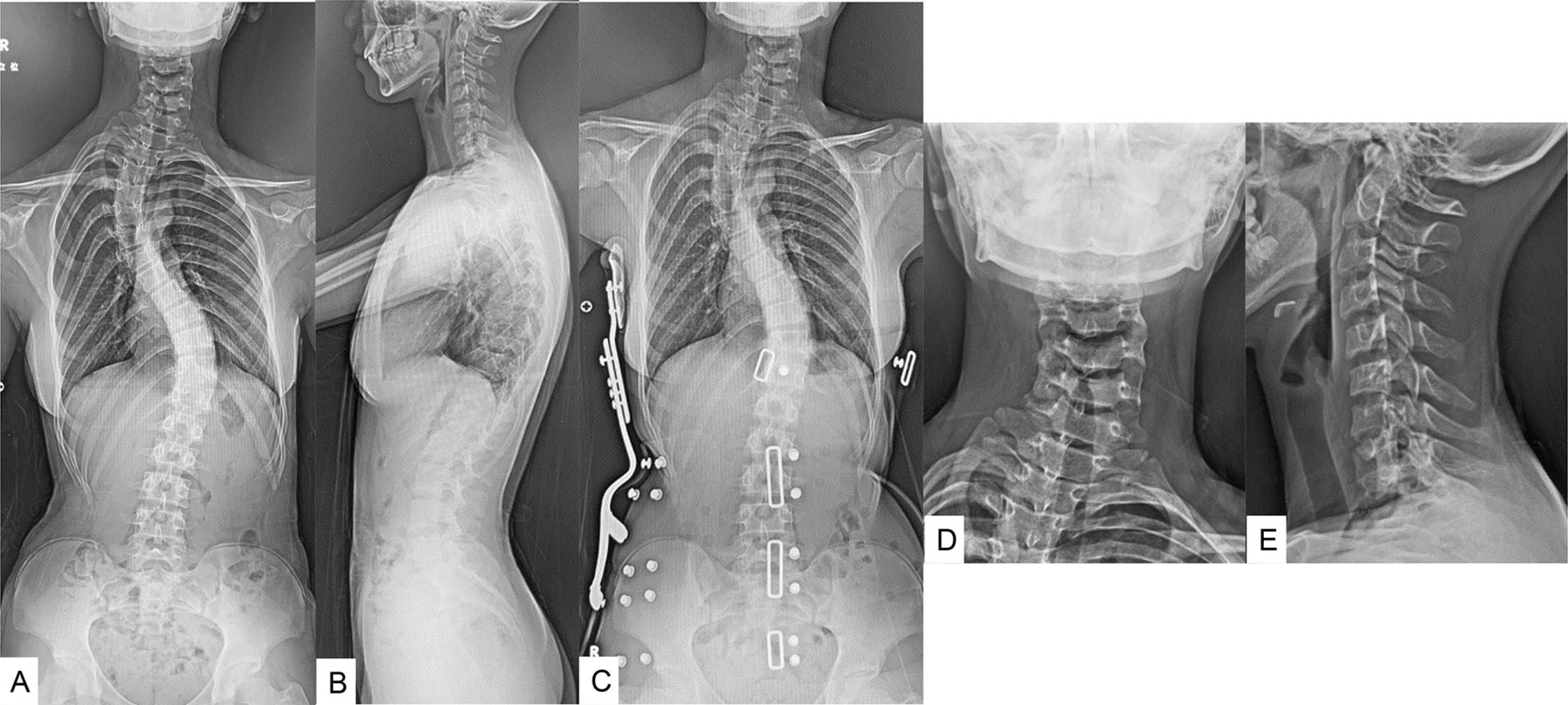
Preoperative radiograms of a 13-year-old girl with Chiari malformation type 1. (A and B) Severe scoliosis was shown, and its Cobb angles were 48° in the upper thoracic and 49° in main thoracic curve. (C) Bracing. (D and E) Cervical spine also had slight scoliosis.
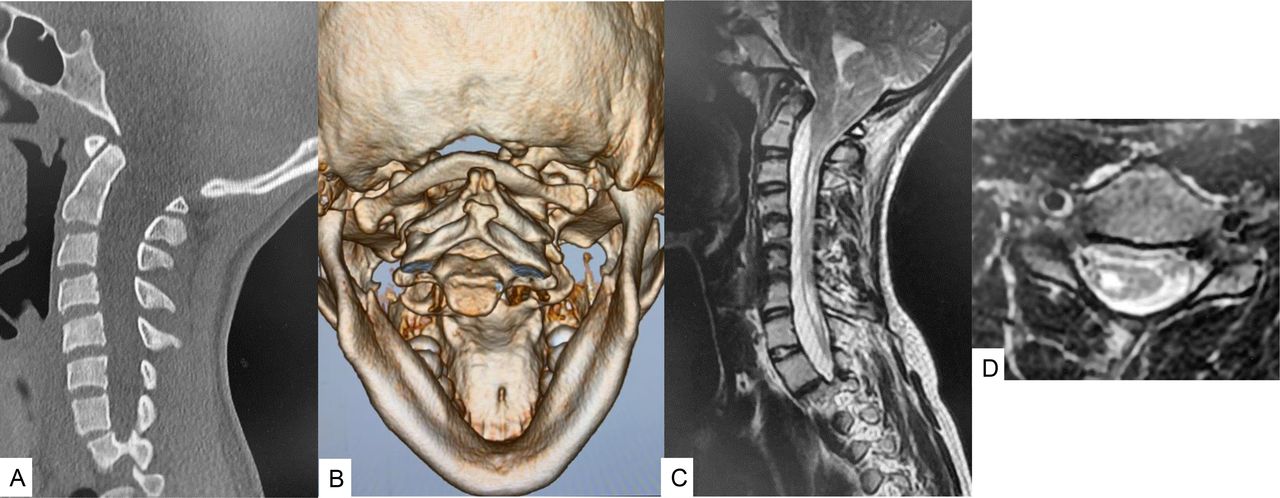
Preoperative images of a 13-year-old girl with Chiari malformation type 1. (A) Sagittal reconstruction computed tomographic (CT) image; (B) 3-D CT image; (C) Mid-sagittal T2-weighted magnetic resonance image (MRI) showed the cerebral tonsile was downward into foramen magnum. (D) Axial T2-weighted MRI at C5 indicated a syrinx in the cervical cord.
Surgery
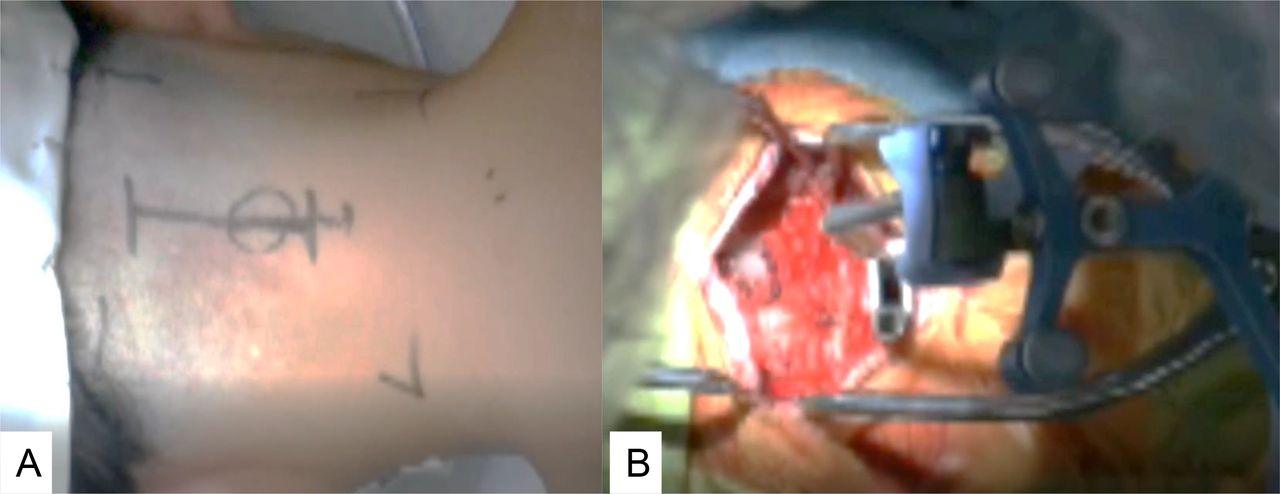
The patient was positioned in a prone position with full carbon operating table and Mayfield skull cramp. Neuromonitoring was used to prevent neurological compromise. An approximately 7-cm skin incision was made from the greater occipital protuberance to the C2 spinous process. Dorsal cervical muscles were dissected from the linea alba down to the posterior aspect of the occiput, C1, and C2 lamina. First, a reference frame was attached to the C2 spinous process (Figure 3). An O-arm scan was performed, and 3-D images were sent to a navigation system. Every instrument, such as the pointer and navigated high-speed burr, was registered for further use.
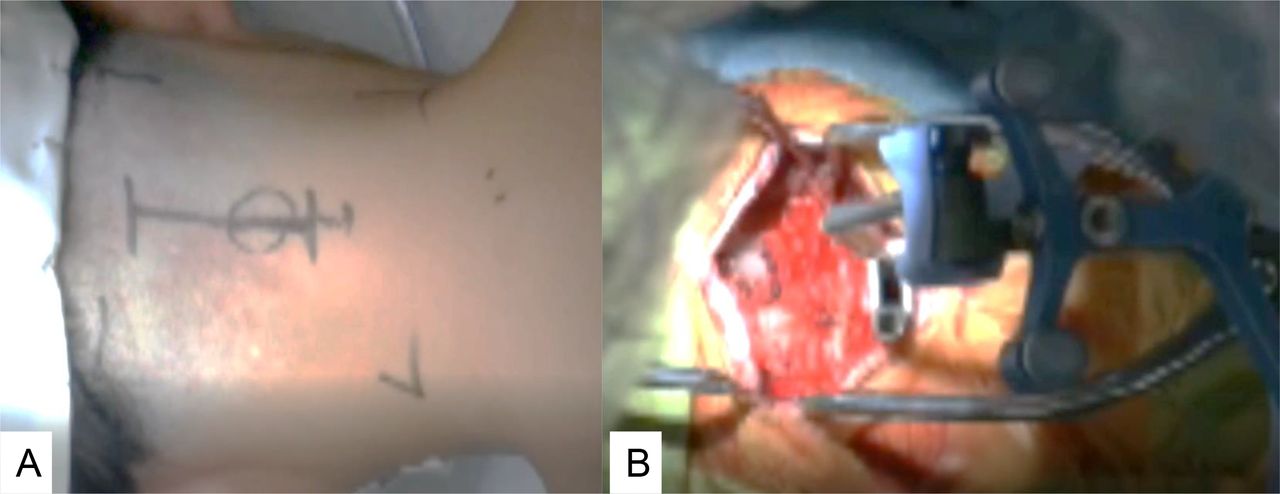
Skin incision and reference frame (A). Approximately 7 cm skin incision was made from greater occipital protuberance to C2 spinous process (B).
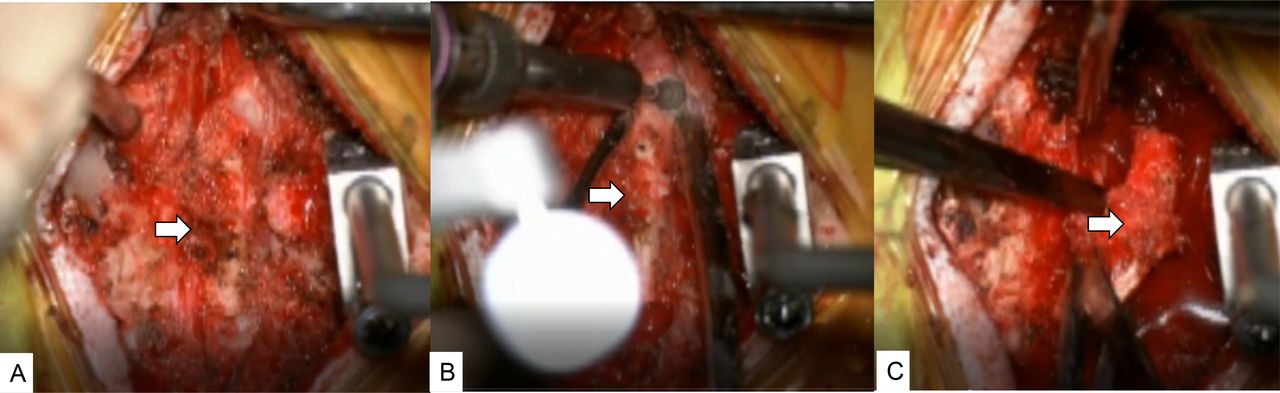
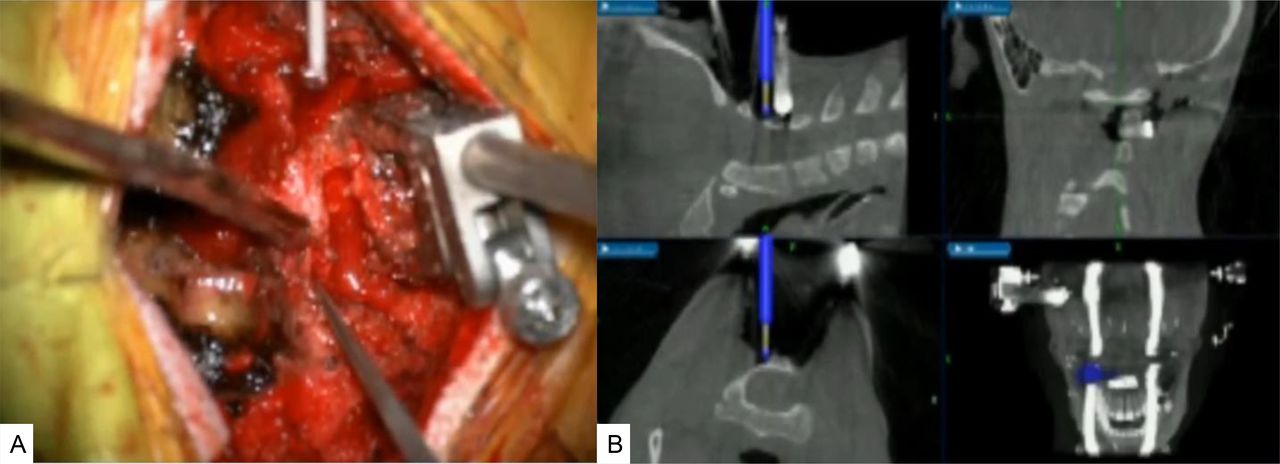
Second, C1 posterior arch was removed with a navigated high-speed burr (Figure 4). In this case, the cranial half of the C2 lamina was also removed because of the degree of tonsillar herniation (Figure 5). Meticulous care was paid not to injure the vertebral arteries.

Removal of C1 lamina. (A) Before removal. (B) Cut with a navigated high-speed burr. (C) Removal of C1 lamina.
Removal of a half of the C2 lamina. (A) Cut with a navigated high-speed burr. (B) Navigation monitor.
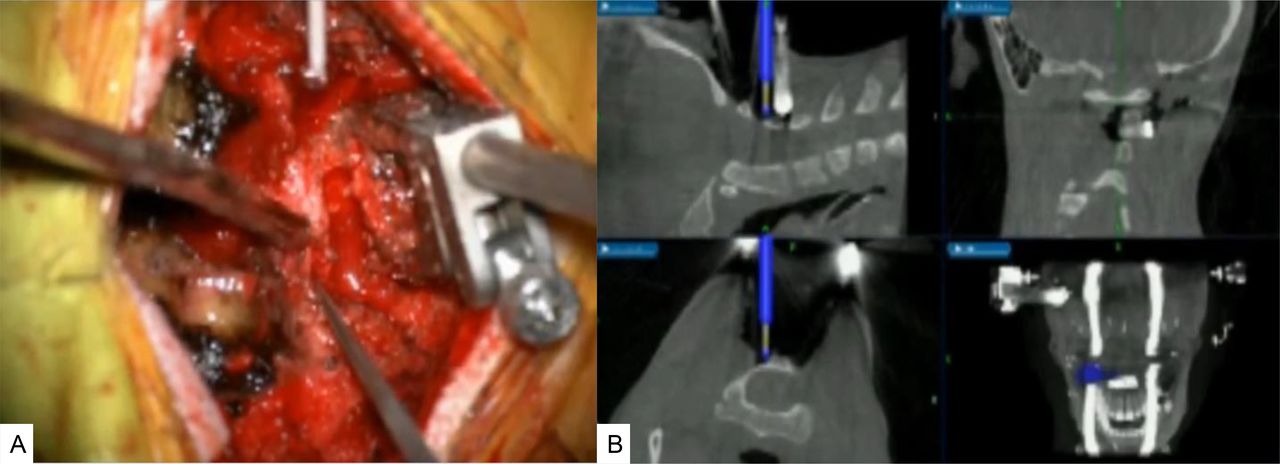
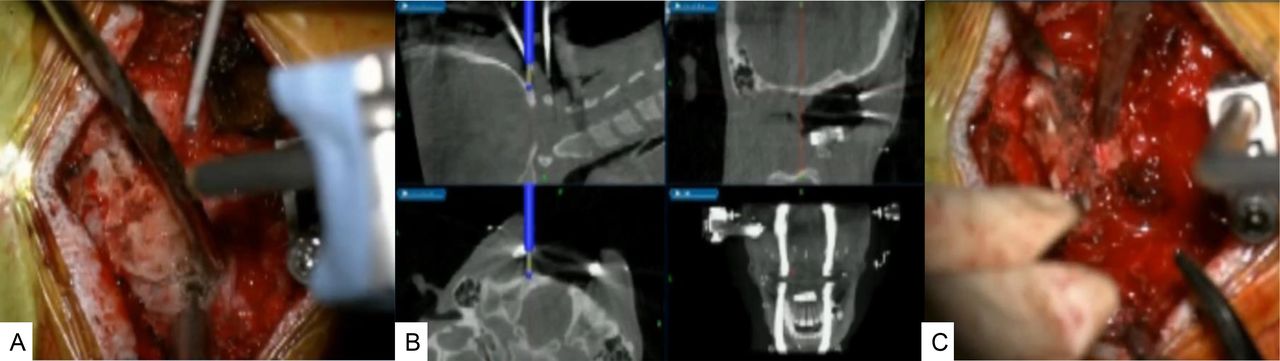
Third, suboccipital craniectomy with 3 cm in diameter around the foramen magnum was performed under navigation guidance. The width of the occipital bone and the exact location of the foramen magnum were identified easily using navigation (Figure 6).
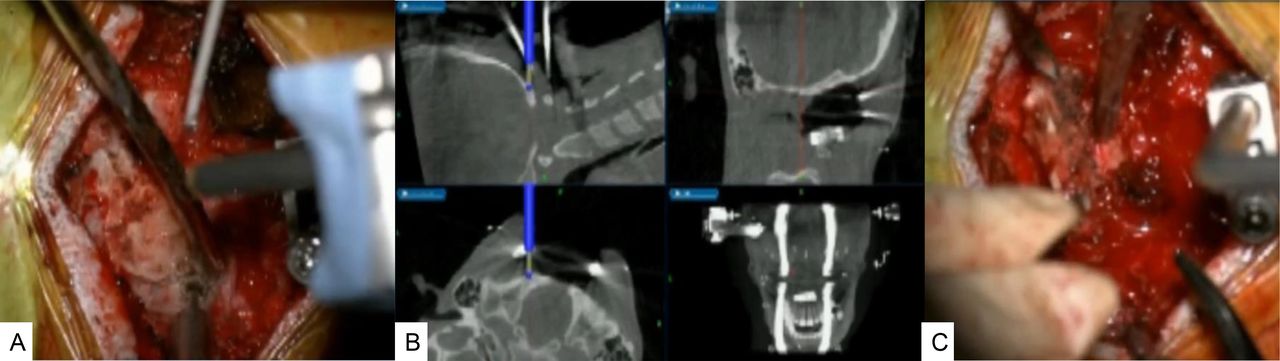
Posterior fossa decompression. (A) Intraoperative image. (B) Navigation monitor. (C) Intraoperative image.
Finally, the outer layer of the dura was split and enlarged (Figure 7A). After dural plasty, intraoperative ultrasonic monitor was used to check the adequate decompression and CSF flow (Figure 7B, C). If the CSF flow was not detected, there were 2 options: (1) extend the bony decompression or (2) expand the dural plasty by artificial dura. Surgical time was 190 minutes, and intraoperative blood loss was 150 mL.

Outer layer dural plasty and intraoperative ultrasonic monitoring. (A) Outer layer dural plasty. (B and C) Intraoperative ultrasonic monitoring. Red arrows show the subarachnoid space between the tonsile and dura.
Postoperative Imaging
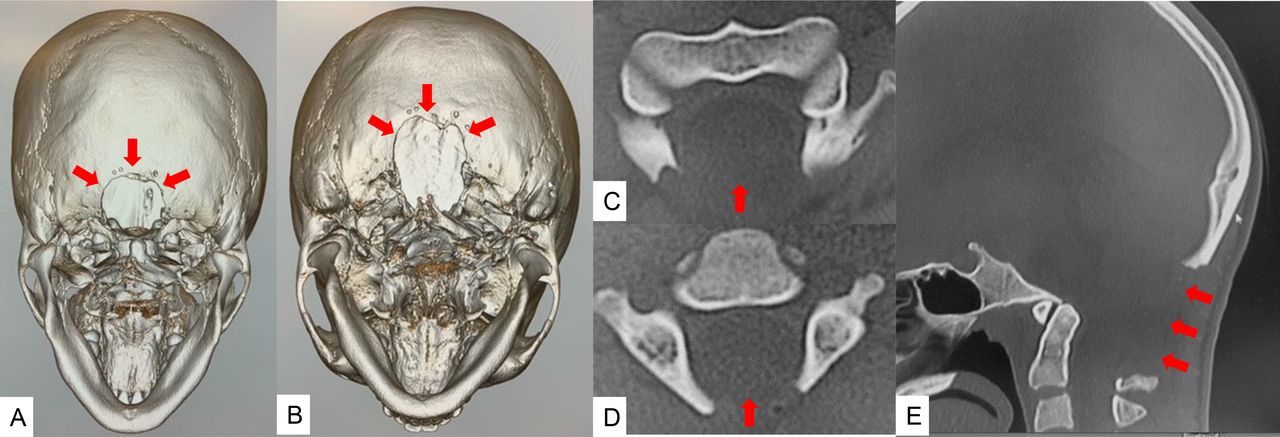
The postoperative radiograms and CT images showed adequate bony resection for CM1 (Figure 8).
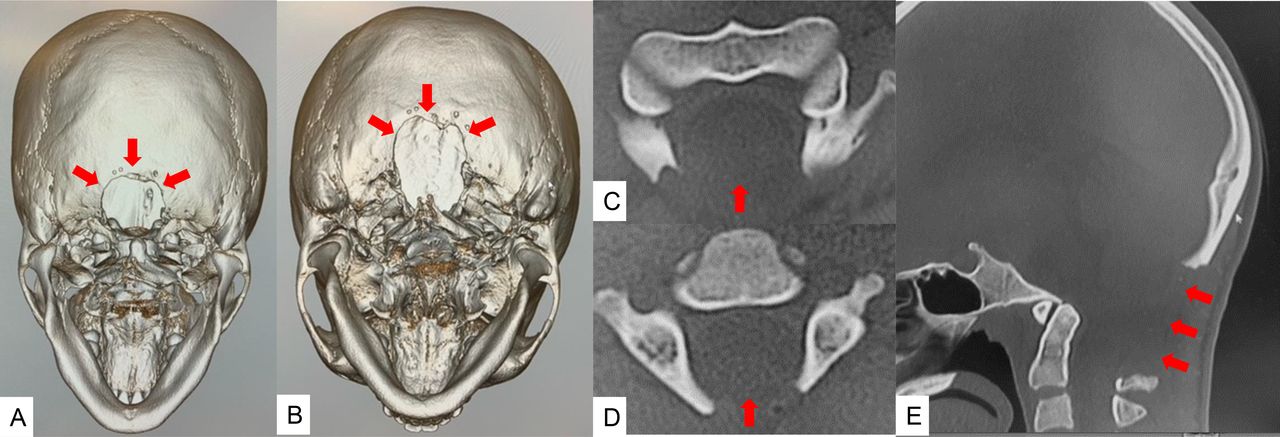
Computed tomographic (CT) images of a 13-year-old girl with Chiari malformation type 1. (A) 45° 3-dimensional (3-D) CT image. (B) 60° 3-D CT image. (C) Axial image at C1. (D) Axial image at C2. (E) Mid-sagittal reconstruction CT image. The foramen magnum was efficiently decompressed (red arrows).
Follow-Up
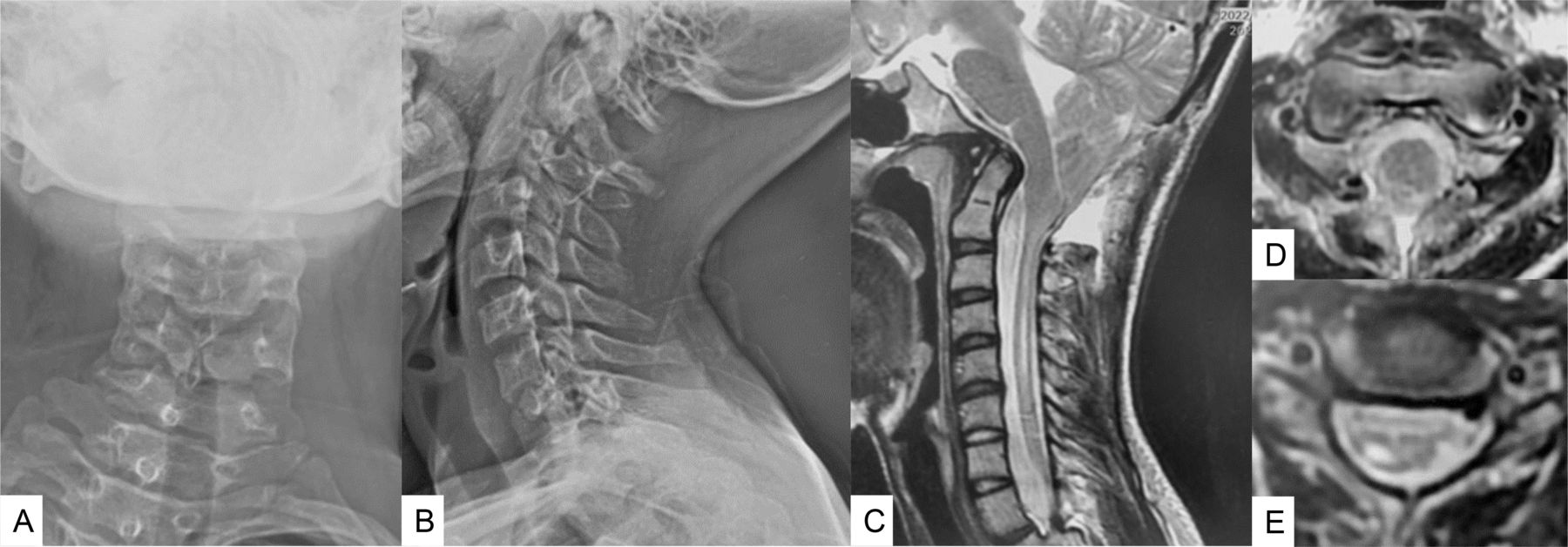
After surgery, the numbness and muscle weakness of the patient were improved. Two weeks later, the patient was discharge from the hospital. She was nearly capable of full activity at 1 month. The final follow-up MRI displayed a good decompression of cerebral tonsile, and cervical syringomyelia was decreased (Figure 9).

Follow-up images of a 13-year-old girl with Chiari malformation type 1. (A) Anteroposterior cervical radiogram. (B) Lateral cervical radiogram. (C) Mid-sagittal T2-weighted magnetic resonance image (MRI). (D) Axial T2-weighted MRI at C1. (E) Axial T2-weighted MRI at C5. MRI showed cerebral tonsile was released, and syringomyelia was reduced.
Discussion
CM1 constitutes a significant burden among children and young adults.14 With increased propensity to perform diagnostic imaging, CM1 can now be recognized in younger children.15 The concepts of Chiari malformation came into view toward the end of the 19th century from Chiari’s initial descriptions of “alterations in the cerebellum resulting from cerebral hydrocephalus” published in 1891.16 His first case description was of a 17-year-old woman who suffered from hydrocephalus but with “no symptoms referable to the cerebellum or medulla.”17 Several pathological mechanisms of CM have been proposed. Significant reduction in the volume of the posterior fossa volume is the most widely accepted hypothesis.18 This decrease in the volume may lead to tonsillar herniation and obstruction of CSF flow between the cortical and spinal subarachnoid spaces. William proposed the cranial-spinal dissociation theory, which states that the pressure gradient between the 2 compartments exacerbates the tonsillar herniation and obstruction of CSF flow results in CSF displacement into the central canal, resulting in syrinx formation.19
Patients with this condition present with a wide range of symptoms ranging from vague and transient symptoms to more debilitating and life-threatening ones.20 By far, headache is the most common symptom related to CM1.21 It is usually described as a suboccipital headache, which is increased on Valsalva maneuver or flexion/extension of the neck. Other more commonly reported symptoms are dizziness, syncope, muscle weakness, numbness of an extremity, and spasticity.22 Some patients may have shortness of breath, sleep apnea, blurred vision, sensitivity to light, ringing in the ears, tinnitus, and ear pain. Psychological and cognitive effects are also seen in patients suffering from CM1.23 MRI is the gold standard for the diagnosis of CM1.22 Cerebellar tonsillar descent ≥5 mm below the foramen magnum is considered diagnostic of CM1.24 Between 60% and 85% of CM1 cases are associated with syringomyelia.25 The cervical spine is most frequently affected, although syringomyelia can occur at any level of the spine, even as low as the conus.26,27 The relevance of the degree of tonsillar herniation and the prospect of syrinx formation is disputed.27
With no definitive correlation between magnitude of tonsillar herniation and clinical manifestations of cervicomedullary junction compression, arguments persist over the indications for operative vs nonoperative management of CM1,21 especially for those patients with mild or no symptoms.28 In a retrospective series in 2011, Benglis et al conservatively managed 124 (43 asymptomatic and 81 symptomatic at presentation) pediatric CM1 patients. The authors found that in a majority of patients, there was no clinical or imaging progression during a mean follow-up period of 2.8 years.21 CM1 patients managed conservatively do not show significant clinical progression on imaging. However, surgery is indicated in patients with symptoms that impact the quality of life, with neuroradiological abnormalities of CM1 associated with syringomyelia.29
The aim of surgery is to decrease the compression at the cervicomedullary junction, which re-establishes the CSF circulation and helps in reducing the size of the syrinx.30 PFD is the preferred treatment option to expand the posterior fossa volume in patients with CM1. The extent of bony decompression and choice of adjunctive techniques vary.31 Adjunctive techniques include lysis of epidural membranes, duraplasty, arachnoid membrane release, intradural lysis of adhesions, obex plugging, shrinking of cerebellar tonsils, and partial tonsil resection.30 Syringosubarachnoid or syringopleural shunt can be put in patients with syrinx with no response to treatment.32,33 In a survey by the American Association of Pediatric Neurosurgeons on surgical technique practice patterns for CM1 with syringomyelia, 85% reported that they perform PFD as the first-line treatment, whereas less than 3% offer syrinx drainage as first-line therapy. Additionally, bony decompression alone was done by 7%, duraplasty by 36%, and tonsil reduction by 27%.34 Despite the advantages and disadvantages of different surgical techniques being set forth by numerous studies, the most contentious issues in CM1 surgery are the adequate extent of bony resection and the choice of adjunctive techniques.30 A combination of posterior fossa craniectomy, C1 laminectomy, and duraplasty is a widely accepted treatment.35 It has also been reported that complementary tonsilar resection does not offer substantial benefits compared with PFD with duraplasty; in addition, only complete opening of the dura achieved slightly better results than a simple incision in the outer dura layer alone.36
The most important aspect of CM1 surgery is bony decompression, the optimal extent of which varies from surgeon to surgeon. A small craniectomy might fail to alleviate compression, whereas a large one has the risk for descent of the cerebellum through the craniectomy defect.30 We introduce a novel technique of performing PFD with the help of navigation system and ultrasonic bone cutter. There is a dearth of literature on the use of navigation system for PFD in CM1. With this technique, the area around foramen magnum can be easily and safely approached with excellent accuracy (Figure 6). It gives an ability to visualize and predict the location of important anatomic structures in a relatively small working area and aids in the placement of the burr holes, allowing real-time intraoperative guidance. In CM1, the normal anatomy can be distorted, where it can be associated with abnormality at the skull base and the craniocervical junction like platybasia and hypoplasia of basiocciput.37 It can also be linked with atlantoccipital assimilation and vertebral segment and fusion abnormality at C1 and C2 leading to block vertebra.38,39 Performing PFD and cervical laminectomy can be a challenging task with this concomitant abnormal anatomy, and the use of a navigation system may decrease the risk of iatrogenic complications in these cases.
The average age in our study was 14 years, and the high association with scoliosis in our patient profile could be credited to the fact that our hospital caters to deformity patients. The average surgical time in our study was 114 minutes, and average blood loss was 82 mL. In a study by Limonadi et al in 2004, the average surgical time was 249 minutes, and average blood loss 80 mL.40 Average surgical time in a study by Mutchnick et al in 2010 was 201 minutes.41 Our lower figures in surgical time could be attributed to the use of navigation and ultrasonic bone cutter. The ultrasonic bone cutter can be a useful instrument for performing decompression, especially around the lateral edge of the foramen magnum, where the use of rongeurs has a risk of injuring the vertebral artery or the epidural venous plexus.42 Furthermore, to monitor the adequacy of decompression and CSF flow, we used intraoperative ultrasonography, also described by David et al in 2006.43 If the ultrasound finding failed to show adequate CSF flow and pulsation, we either extended the decompression or performed duraplasty.
There are several limitations of this study. The sample size was small. With a larger patient population, accuracy comparisons, statistical differences, complications as well as patient outcomes should be assessed for the navigationally supported study vs the current methods toward CM1 treatment.
Conclusions
PFD under navigation guidance can reduce inappropriate decompression and may decrease a revision surgery. During decompression surgery, CSF leakage can be prevented by the ultrasonic bone cutter and navigation.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.