


Abstract
Background Studies were reviewed and collected to compare different image guidance systems for pedicle screw placement (PSP) regarding accuracy and safety outcomes. Included were conventional, navigation, robot-assisted, and recent technology such as augmented reality (AR) guiding systems.
Methods This network meta-analysis obtained human comparative studies and randomized controlled trials (RCTs) regarding PSP found in 3 databases (Cochrane, PubMed, and Scopus). Data extraction for accuracy, safety, and clinical outcomes were collected. The network meta-analysis was analyzed, and a surface under the cumulative ranking curve (SUCRA) was used to rank the treatment for all outcomes.
Results The final 61 studies, including 13 RCTs and 48 non-RCTs, were included in the meta-analysis. These studies included a total of 17,023 patients and 35,451 pedicle screws. The surface under the cumulative ranking curve ranking demonstrated the supremacy of robotics in almost all accuracy outcomes except for the facet joint violation. Regarding perfect placement, the risk difference for AR was 19.1 (95% CI: 8.1–30.1), which was significantly higher than the conventional method. The robot-assisted and navigation systems had improved outcomes but were not significantly different in accuracy vs the conventional technique. There was no statistically significant difference concerning safety or clinical outcomes.
Conclusions The accuracy of PSP achieved by robot-assisted technology was the highest, whereas the safety and clinical outcomes of the different methods were comparable. The recent AR technique provided better accuracy compared with navigation and conventional methods.
Level of Evidence 2
Introduction
There have been many advancements in spinal surgery instrumentation and techniques over the past few decades, with posterior fixation being one of the most significant developments.1 In various indications, pedicle screws are used to stabilize and fuse the spine. Biomechanically, posterior fixation provides 3-dimensional (3D) stability to fused segments and has improved spinal fusion surgery outcomes, which has led to its growing popularity and acceptance.2 Several pedicle screw placement (PSP) techniques have been described. The conventional freehand technique is the technique that was originally used. With this technique, the surgeon identifies the screw entry point based on the patient’s spinal anatomical landmarks and inserts the pedicle screws under conventional fluoroscopic guidance.3 However, the rates of screw penetration or misplacement following this technique are not uncommon, potentially leading to serious postoperative complications, such as neurological injuries and hardware failure.4,5
Various assistive intraoperative image guidance technologies have been introduced to help improve the accuracy of the PSP. The intraoperative navigation system was developed and incorporated with different imaging inputs, such as 2-dimensional (2D) fluoroscopy, 3D fluoroscopy, and computed tomography (CT)-based or O-arm navigation (O-arm, Medtronic, Minneapolis, MN, USA). This system has recently gained popularity among spine surgeons.6,7 Several studies demonstrated better accuracy rates of screw placement and fewer screw-related complications compared with the conventional technique, regardless of imaging resources.8,9 The robot-assisted system is one of the latest advanced assistive technologies, which provides excellent screw accuracy comparable to navigation.10 Recently, augmented reality (AR), which is an emerging technology, has provided users with stereoscopic visualizations and integrated computer-generated information into the real-time environment.11 Evidence of the efficacy of AR-assisted PSP has been demonstrated in cadaveric proof-of-concept studies,12–16 among diverse operators,17,18 and in clinical studies that report high potential efficacy,19,20 high efficiency,18,21 and a low-radiation system.22,23 However, few publications provide quantitative evidence of its value compared with other PSP methods.
In this study, we pooled the data from the studies that utilized several image guidance technologies for the PSP, including recent clinical studies using the AR-assisted method, to investigate and compare the effectiveness regarding screw accuracy, safety, and clinical outcomes among these intraoperative image guidance systems.
Materials and Methods
Literature Review and Search Strategy
The protocol for this network meta-analysis (NMA) was registered with PROSPERO (International Prospective Register of Systematic Reviews; no. CRD 42023398773). A systematic literature search of PubMed (1991 to November 2022), SCOPUS (1988 to November 2022), and the Cochrane Database of Systematic Reviews (2000 to November 2022) was conducted to compare different assistive techniques for PSP. The primary outcome was the accuracy of the PSP considering perfect placement, clinically acceptable (safe) placement, screw malposition, intraoperative screw revision, and facet joint violation. The secondary outcomes include safety outcomes consisting of the overall complications, neurological complications, wound and infection complications, and clinical outcomes at 1 year after the index surgery.
The systematic literature review was undertaken independently by 2 investigators (K.R. and T.T.) applying a search approach that incorporated the terms “pedicle screw” AND “freehand,” “fluoroscope,” “CT,” “C-arm,” “O-arm,” “navigation,” “robot,” “AR,” “virtual reality,” or “mixed reality” in combination found in the Title, Abstract, or Keyword. Only literature published in the English language was included. This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement.24
Definition and Classification
Since there has been a continuous development of assistive technology for better PSP, we classified it into 4 major groups, including conventional, navigation, robot-assisted, and AR-assisted techniques. The conventional method included studies recorded as either freehand or C-arm fluoroscopy, as all the included freehand studies also used C-arm fluoroscopy for final checking of the screw placement. The navigation method included studies using any image sources that could be either 2D, 3D, or CT/O-arm-based systems where we specified the details of image guidance in Table 1. The robot-assisted method is the technique that uses a robot to perform PSP instead of a surgeon. The AR-assisted method uses mixed reality combined with more advanced real-time 3D technology imaging to guide the surgeon while performing PSP.
Study characteristics providing information on the study design, comparative intervention, instrument details, study duration, population, number of patients, gender percentages, and body mass index of included patients.
The primary objective of this study was to evaluate the accuracy of PSP, which consists of 5 aspects, including the perfect placement, a clinically acceptable placement, screw malposition, intraoperative screw revision, and proximal facet joint violation. Postoperative CT images were used to classify the accuracy of screw position in the pedicle. The perfect PSP was graded as Grade A (0 mm breech) of the Gertzbein and Robbins’ classification5 or Rampersaud’s classification,27 while the accuracy of clinically acceptable (safe) placement was defined as less than 3 mm of pedicle screw breech (Grades A and B of the Gertzbein and Robbins’ classification, Rampersaud’s classification, and Group I–II of the Learch’s classification).28 Screw malposition was defined as screw penetration beyond the safe placement borderline. Proximal facet joint violation was also recorded as grade 1 or more of the classifications described by Kim et al29 and Babu et al.30
The secondary outcomes include safety and functional outcome aspects. Postoperative complications imply the safety of the procedure, including any adverse events, neurological complications, wound and infection complications, and reoperation or revision incidences. The postoperative clinical changes reported in extracted studies consist of the visual analog scale of the back (VAS back), the VAS leg, and the Oswestry Disability Index (ODI) up to 1-year after the operation.
Selection Criteria
Data from comparative studies (cohort, case-control, or cross-sectional studies) and randomized controlled trials (RCTs) were included in the analysis, whereas descriptive studies, case series, case reports, cadaveric studies, nonhuman studies, systematic reviews, literature reviews, or meta-analyses were excluded. Eligible studies are needed to provide data on measurement accuracy, the prevalence of any adverse events, or clinical outcomes. Inclusion was not limited by the study sample size. Retrieved articles were individually reviewed for eligibility by K.R. and T.T. Discrepancies were discussed and resolved by a third investigator (W.S.).
Data Extraction
A structured data collection form was utilized to derive the following information from each study: the year that the study was conducted, name of the first author, publication year, demographic and characteristic data of the population, intraoperative imaging guidance system used, and types of instruments.
Statistical Analyses
We conducted a contrast-based NMA using Stata 17 (Statacorp LLC, College Station, TX, USA).31 Binary efficacy and safety outcomes were summarized as pooled risk differences (95% CI) between conventional surgery and AR, navigation, or robot-assisted surgery, and a global test of inconsistency was performed. The surface under the cumulative ranking curve (SUCRA) was used for the hierarchical ranking of the treatments, which could be interpreted as the estimated possibilities of being the best treatment. Clinical outcome data were reported by most studies as pre- and postsurgical means, without reporting the SD of the change from pre- to postsurgery. We used the study that reported outcomes in sufficient detail32 to derive a correlation coefficient, which we used to impute an SD of the change from the baseline for the other studies.33 The risk of bias across studies was summarized by the Newcastle-Ottawa quality assessment scale for case-control studies34 and the Cochrane Collaboration’s tool for randomized trials.35 Funnel plots were drawn to assess the risk of publication bias.
Results
Study Selection
A total of 3987 studies were imported from 3 different electronic databases (PubMed, Scopus, and the Cochrane Library), and 1411 duplicate studies were removed. After screening, 2352 studies were excluded because they were not related to pedicle screw insertion in spine surgery. A total of 224 full-text articles were assessed, of which 163 studies were excluded based on the inclusion and exclusion criteria. Thus, we included the final 61 articles, including 13 RCTs and 48 non-RCTs (11 prospective cohort studies and 37 retrospective observational studies), for conducting the systematic review and NMA. A flow diagram of study selection is presented in Figure 1.

The Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow diagram of the selection process of related articles.
Overall Characteristics and Risk of Bias Assessment of the Included Studies
A total of 17,023 patients and 35,451 pedicle screws were included in the study. The mean study sample size was 67 patients (range 20–5805), with an average of 3 pedicle screws per patient. The baseline characteristics of each study are shown in Table 1. The quality of evidence was appraised according to the quality assessment tools for different study designs as previously stated and reported in Table 2 and Figure 2.

The Cochrane Collaboration’s tool for assessing the risk of bias for randomized controlled trials. (a) Risk-of-bias summary: A review of authors’ judgments on each risk-of-bias item for each study included. (b) Risk-of-bias graph: A review of authors’ judgments on each risk-of-bias item, presented as percentages across all included studies.
Newcastle-Ottawa Scale—for cohort studies.
Primary Outcomes
PSP Accuracy
Fifty-six studies used Gertzbein and Robbins’ classification to evaluate the accuracy of the PSP. Four studies employed Rampersaud’s classification, and the other 3 used Learch’s classification. All of these classifications employed postoperative CT to assess the accuracy of the PSP.
Perfect Placement of Pedicle Screws
The NMA of 41 studies gave direct comparisons among 4 different techniques: conventional method, navigation, robot-assisted, and AR technologies, while there were only indirect comparisons between AR and robot-assisted systems (Figure 3a). There was no evidence of inconsistency (χ 2 = 6.05, P = 0.195). Compared with the conventional method, AR had significantly higher accuracy with a risk difference of 19.1 (95% CI: 8.1–30.1; Figure 3a). The robot-assisted and navigation systems had better accuracy vs the conventional method, but the difference was not statistically significant (risk difference: 9.3, 95% CI: −9.1 to 27.7; and 2.9, 95% CI: −9.1 to 14.8, respectively; Figure 3a). Nonetheless, there was no significant difference between robotic-assisted and AR (risk difference of 0.7, 95% CI: −15.3 to 16.6).

The network geometry (left) and interval plots (right) for accuracy outcomes. (a) Perfect placement, (b) safe placement, (c) screw malposition, (d) intraoperative screw revision, and (e) proximal facet joint violation. Of the network geometry, each circular node represents a type of treatment as labels. The circle size is proportional to the total number of pedicle screws. The width of lines is proportional to the number of studies performing head-to-head comparisons. The interval plots of the risk difference demonstrate treatment effect comparison in the studies.
Clinically Acceptable (Safe) Placement and Screw Malposition
Safe screw placement was reported in 36 studies, and NMA provides 53 direct comparisons across 4 different methods. Among those, there was no direct comparison between AR and robot-assisted methods. Inconsistency testing was conducted, and the consistency assumption could be accepted at the overall level of each treatment (χ 2 = 4.66, P = 0.3237). Compared with the conventional method, there was no statistically significant difference found for robot-assisted, navigation, or AR methods (risk differences of −0.74 [95% CI: −12.42 to 10.94], 3.35 [95% CI: −3.34 to 10.04], and 4.3 [95% CI: −4.37 to 12.99], respectively; Figure 3b). On the contrary, screw malposition data extracted from 40 studies giving 55 direct comparisons across 4 methods demonstrated more significant displacement in the conventional technique when compared with robot-assisted (risk difference: −4.81, 95% CI: −7.05 to −2.58) but not compared with AR (risk difference: −4.3, 95% CI: −13.17 to 4.56, P = 0.330) and navigation (risk difference: −1.46, 95% CI: −8.17 to 5.25) methods (Figure 3c). Evidence of inconsistency was not found (χ 2 = 3.23, P = 0.3570).
Intraoperative Screw Revision and Proximal Facet Joint Violation
Other aspects indicating the accuracy of different techniques are, first, the intraoperative screw revision, where mispositioned screws or unsatisfactory screw insertion were revised using either a similar or a backup conventional method, and second, the proximal facet joint violation. Despite not being the primary study outcomes in most included studies, 8 studies provided direct comparisons among conventional, navigation, and robotics. None of the AR studies reported these outcomes. Testing for inconsistency was conducted (χ 2 = 0.29, P = 0.865). In comparison to the conventional method, the robot-assisted and navigation methods demonstrated fewer incidences of intraoperative screw revision (risk difference: −2.27, 95% CI: −5.28 to 0.74, and −0.88, 95% CI: −7.41 to 5.63, respectively; Figure 3d). Facet joint violation, from the 10 included studies, was greater in conventional compared with robot-assisted and navigation methods (risk difference: 8.31 [95% CI: −1.52 to 18.13] and 3.02 [95% CI: −5.24 to 11.29], respectively; Figure 3e). Inconsistency testing was achieved (χ 2 = 2.74, P = 0.0977).
Overall, the SUCRA hierarchical ranking of estimated probabilities, ranging from 0% to 100%, from NMA was used to grade the accuracy of different techniques. A higher SUCRA value and a taller bar graph correspond to a higher ranking and higher accuracy rates. Regarding the perfect placement, the superiority of robot-assisted (S = 83.4) placement is shown, followed by AR (S = 81.2), navigation (S = 35.4), and the reference, which is the conventional technique (S = 0; Figure 4a). Similarly, safe placement and positive grading for screw malposition are found in the robot-assisted PSP. Lastly, the SUCRA ranking showed the best performance for the least intraoperative screw revision and proximal facet joint violation in the robot-assisted technique (Figure 4a).

The surface under the cumulative ranking curve (SUCRA) of a treatment hierarchical ranking for the estimated probability of being the best assistive pedicle screw placement method. (a) Accuracy outcomes, (b) safety outcomes, and (c) clinical outcomes. Abbreviations: ODI, Oswestry Disability Index; VAS, visual analog scale.
Secondary Outcomes
Safety Outcomes
Safety outcomes that were analyzed in this NMA consist of any adverse events, neurological complications (such as neurological deficits and significant painful radiculopathy), wound and infection complications, and reoperation or revision incidences. Wound and infection complications that were reported in the included studies consist of wound problems, such as surgical site infection, seroma formation, wound dehiscence, and delayed wound healing, as well as other nonspecific infections, such as urinary tract infections. All analyzed outcomes were tested for inconsistency and showed a global consistency (χ 2 = 0.24, P = 0.9701; χ 2 = 0.48, P = 0.9232; χ 2 = 2.15, P = 0.5424, respectively). There were no AR studies that mentioned the safety aspect; however, safety outcomes have not been documented in most of the meta-analyses that reported on the PSP. So, we performed NMA across only 3 different methods (conventional, navigation, and robotics) in this study.
Any adverse event was assessed from 15 studies demonstrating insignificantly fewer adverse events in robotics and navigation (risk difference: −3.07, 95% CI: −18.3 to 12.15, −2.64, 95% CI: −37.6 to 32.35, respectively) than those in the conventional method. Nine studies reported neurological complications, whereas wound complications and infection complications were present in 12 studies. Our analysis nonetheless found an insignificant difference across the 3 methods (Figure 5). The SUCRA hierarchy ranking demonstrated superiority in robot-assisted, followed by navigation and then conventional methods for overall complications and neurological complications, whereas the conventional method was ranked the most superior regarding wound complications (Figure 4b).

The network geometry (left) and interval plots (right) for safety outcomes. (a) Any adverse event, (b) wound and infection complications, (c) neurological complications, and (d) reoperation or revision.
Reoperation or revision was reported in 14 studies due to several causes, including pseudoarthrosis, infection, instrumentation irritation causing low back pain requiring removal, and radiculopathy requiring revision decompression or screw removal. Three methods of PSP, including conventional, navigation, and robot-assisted, were directly compared. Testing for inconsistency was performed (χ 2 = 0.45, P = 0.5007). In comparison to the conventional method, both robot-assisted and navigation methods showed insignificantly different revision rates (risk difference: 0.9, 95% CI −1.79 to 3.67, and −0.38, 95% CI: −1.02 to 0.27, respectively); however, robot-assisted methods had fewer reoperation rates than navigation (Figure 5d). The SUCRA hierarchy ranking showed the positive value of robot-assisted methods and the most inferior of the conventional method (Figure 4b).
Clinical Outcomes
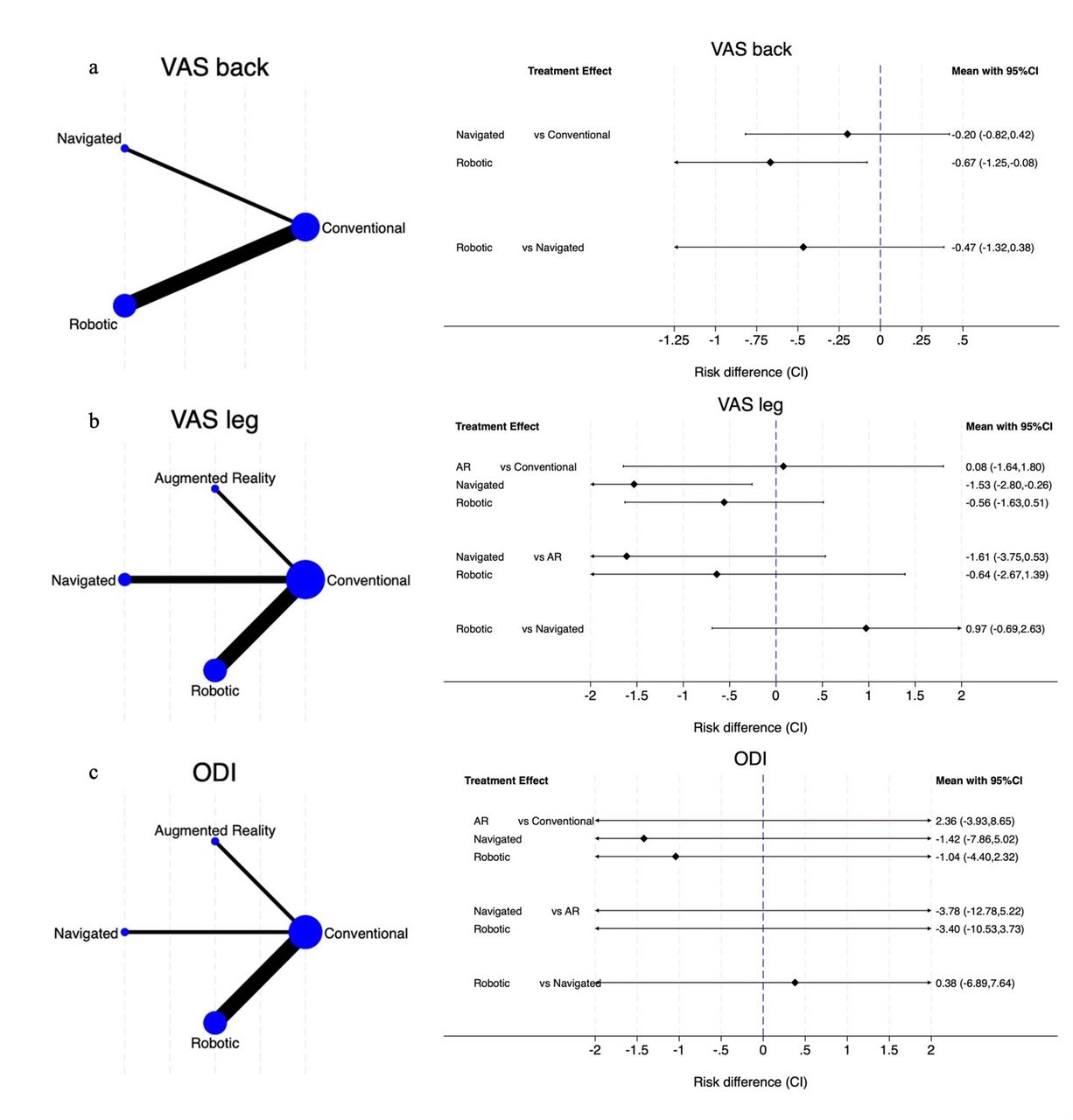
Differences between the preoperative and postoperative clinical outcomes reported in extracted studies were up to 1-year results consisting of the VAS back, the VAS leg, and the ODI. However, limited data were collected, and the inconsistency model thereby failed to develop. With careful interpretation, 5 studies giving direct comparisons for VAS back reported the most superiority in robot-assisted methods, followed by navigation and conventional methods. The VAS leg was reported in 7 studies, including a direct comparison of the AR method (Figure 6). Given the possibility of statistical inconsistencies, careful interpretation is necessary. The SUCRA ranking demonstrated the best improvement in the navigation group for VAS leg and ODI outcomes (Figure 4c).

The network geometry (left) and interval plots (right) for clinical outcomes up to 1 year after the index surgery. (a) Visual analog scale (VAS) of the back, (b) VAS leg, and (c) Oswestry Disability Index (ODI).
Publication Bias
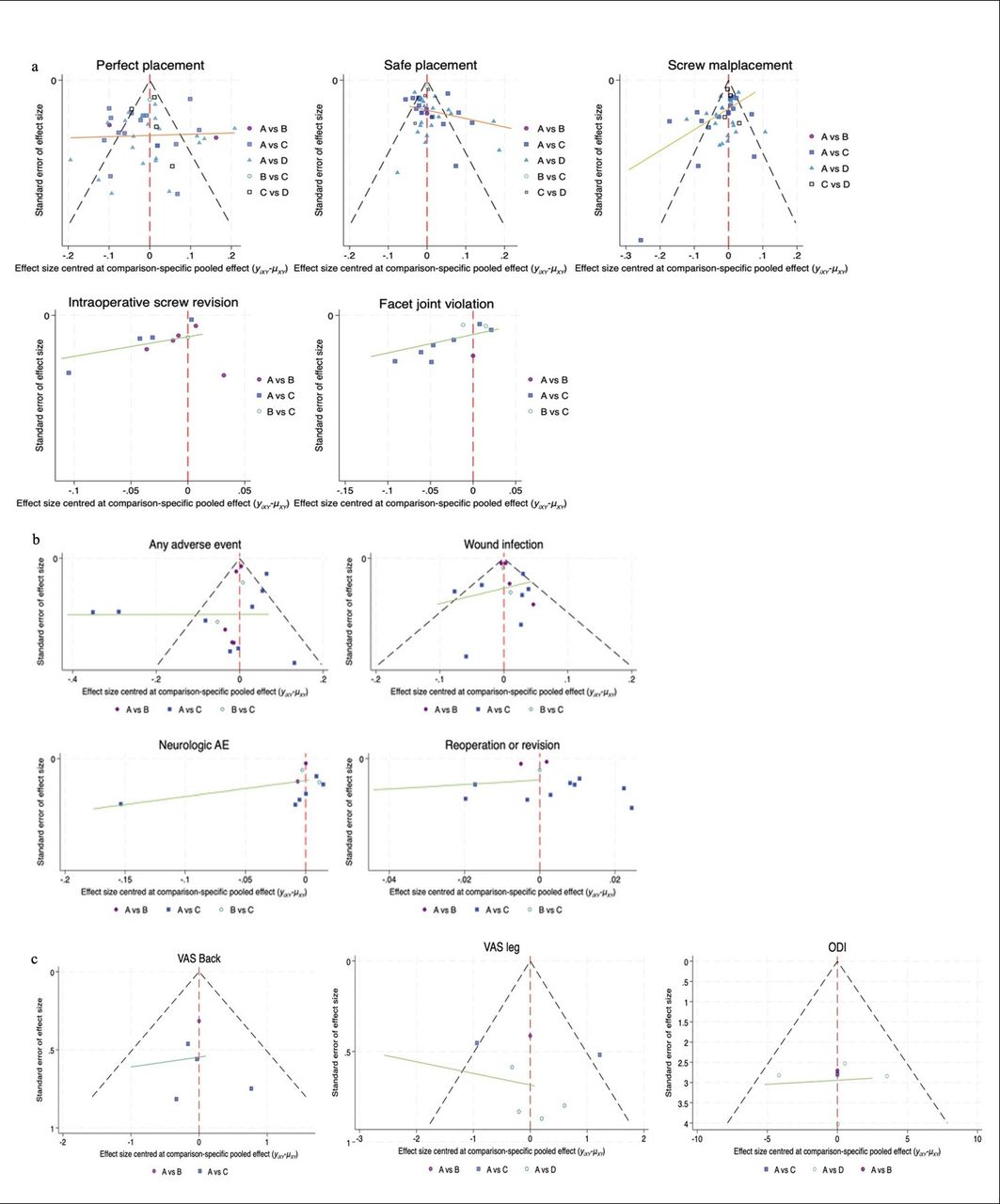
To check for publication bias in NMA, a network funnel plot was made and shown in Figure 7. Visually inspecting for symmetry was clearly demonstrated for the main primary outcomes, namely perfect placement, safe placement, and screw malposition. Additionally, clinical outcomes as well as safety outcomes, namely any adverse event and wound and infection complication, were also assessed. Intraoperative screw revision, facet joint violation, and reoperation/revision were usually not the major study objective in included studies, and combining smaller studies would likely show asymmetry in these outcomes.

Funnel plots for (a) accuracy, (b) safety, and (c) clinical outcomes.
Discussion
Our study provides the first statistical analyses of different advanced assistive techniques for PSP, including the emerging AR guiding technology. We found that the robot-assisted PSP performed the most accurately among the various assistive methods. This was followed by AR and navigation, which were more accurate than the conventional method. This was also in accordance with the safety results that the assistance of any techniques might reduce rates of complications.
The accuracy of the PSP is critically important not only in determining the surgical outcomes but also in contributing to the safety of the procedure due to the proximity of vital neurovascular structures to the pedicle area. Recently, advances in assistive technologies, including O-arm-based navigation and robot-assisted methods, have helped improve the accuracy of the PSP. A prior meta-analysis conducted by Staartjes et al,36 which included controlled studies comparing robot-assisted with conventional and navigation methods, showed a reduction in rates of intraoperative screw revision and postoperative revision due to screw malposition. However, there was little evidence of a direct comparison between robot-assisted and navigation systems. Naik et al later reported the NMA of robot-assisted PSP with a comparison to navigation where image references were derived from different techniques: 2D fluoroscope, 3D fluoroscope, and CT or O-arm. Similarly, the robot-assisted method provided the advantages of significantly improving accuracy, perfect, and optimum placement, and reducing complications, even greater than the navigation.37 According to our analyses, we could not obtain statistically significant differences for the superiority of robot-assisted placement accuracy, both perfect and safe placements, despite the first rank from the SUCRA ranking. Besides, intraoperative screw revision and proximal facet joint violation were better with the assistive devices. Greater screw accuracy and precision from robot-assisted approaches were achieved because of the autonomous operation independent of the surgeon, which could reduce risks from human errors. However, the initial system settings and software conditions could influence the effectiveness of its performances, resulting in heterogeneity of results.
For the past few years, reality has been merged with computer-generated displays, known as AR. Evidence has cumulated where AR has been used and tested in proof-of-concept preclinical settings: phantom agar38,97 and cadavers.12,14,15,98 Several case series and comparative cohort studies suggested not only the high accuracy of screw insertion20,99–102 but also the additional benefits of reducing radiation exposure23 and operative time.19 Since the technology is still in its infancy, there has been no study comparing it with other advanced methods except for the conventional method.103 Thus, we utilized NMA to obtain a bird’s-eye view of the aiding technologies. As a result of our analysis, AR produced significantly more perfectly placed screws compared with the conventional method and ranked second to the robot-assisted method concerning SUCRA probabilities.
Safety outcomes bluntly resulted from the screw accuracy, where common reasons leading to reoperation were painful radiculopathy or nerve root injury due to screw malposition, as stated in the included studies. Based on our analyses, the robot-assisted method reported fewer complications than navigation, and navigation reported a smaller number of adverse events compared with the conventional technique. This finding was aligned with a prior meta-analysis.37 Due to the fact that clinical outcomes were not commonly investigated for assessing the effectiveness of different techniques, a small number of studies were derived for analyses. Therefore, the analysis was not sufficiently powered to draw a meaningful conclusion. In addition, there were wide ranges of diagnoses and operations that directly affected clinical/surgical outcomes.
Although this NMA was able to determine only the possibility of superiority between different assisting technologies, it did demonstrate the impact of advancements in technology that may help improve surgical outcomes. Combining the 2 techniques could also enhance their advantages even further. For example, surgeons could supervise autonomous robotics using AR technologies.104
As an NMA, the present study has some limitations. To obtain a comprehensive sample, we included both RCTs and comparative studies. There were a variety of image guidance systems for navigation, including 2D fluoroscopy, 3D fluoroscopy, and CT or O-arm, which we mentioned in detail if presented, in the characteristic table of the included studies. Also, there were various types of robot-assisted systems in the studies, and we did not compare each system in this NMA. Last, due to the recent development of AR technology, there have been only a small number of studies, resulting in the limited power of direct comparison; nonetheless, this study utilized the NMA method to gain a better understanding of the usefulness of the novel technique.
Conclusions
The robot-assisted methods achieved the most superior accuracy of PSP, whereas the safety and functional outcomes of the different methods were comparable. The AR technology provided better accuracy compared with navigation and conventional techniques.
Acknowledgments
Teerachat Tanasansomboon expresses his heartfelt gratitude to his wife, Thanachaporn Kittipibul, for her unwavering dedication. They joyfully welcome their baby boy “Darwin” into this world.
Footnotes
Funding No funding was received for this study.
Disclosures The authors report no disclosures or conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.
- 26.
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.