


Abstract
Background There is a lack of consensus on the use of postoperative bracing for lumbar degenerative conditions. Spine surgeons typically determine whether to apply postoperative braces based primarily on clinical experience rather than robust, evidence-based medical data. Thus, the present study sought to assess the impact of postoperative bracing on clinical outcomes, complications, and fusion rates following lumbar fusion surgery in patients with degenerative spinal conditions.
Methods Only randomized controlled studies published between January 1990 and 20 October 2023 were included in this meta-analysis. The primary outcome measures consisted of pre- and postoperative assessments of the Oswestry Disability Index (ODI) and visual analog scale (VAS) scores. Improvements in VAS and ODI scores were analyzed in the early postoperative period (1 month after operation) and at final follow-up, respectively. The analysis also encompassed fusion rates and complications.
Results Five studies with 362 patients were included in the present meta-analysis. In the early postoperative period, the brace group showed a relatively better improvement in ODI scores compared with the no-brace group (19.47 vs 18.18), although this difference was not statistically significant (P = 0.34). Similarly, during the late postoperative period, the brace group demonstrated a slightly greater improvement in VAS scores in comparison to the no-brace group (4.05 vs 3.84), but this difference did not reach statistical significance (P = 0.30). The complication rate was relatively lower in the brace group compared with the no-brace group (14.9% vs 17.4%), although there was no statistical difference between the 2 groups (P = 0.83). Importantly, there were no substantial differences in fusion rates between patients with or without braces.
Conclusion The present meta-analysis revealed that the implementation of a brace following lumbar fusion surgery did not yield substantial differences in terms of postoperative pain relief, functional recovery, complication rates, or fusion rates when compared with cases where no brace was employed.
Clinical Relevance This meta-analysis provides valuable insights into the clinical impact of postoperative bracing following lumbar fusion surgery for degenerative spinal conditions.
Level of Evidence 1.
Introduction
Lumbar fusion surgery has become a widely accepted and effective treatment option for a variety of lumbar spinal conditions, including degenerative disc disease, spondylolisthesis, and spinal stenosis.1–3 However, postoperative care and management protocols for patients undergoing lumbar fusion remain subjects of ongoing research and debate. Conventional wisdom postulates that postoperative lumbar support immobilization serves to diminish intervertebral motion and alleviate biomechanical loading in the surgical region, potentially resulting in heightened fusion rates and diminished patient-reported pain.4,5 Nevertheless, the application of such supports necessitates a thorough consideration of accompanying concerns, including the potential for skin irritation, impediments to rehabilitation progress, and the possibility of atrophy in the lumbar musculature due to extended external immobilization.6,7
Given the clinical importance of this topic, a growing body of literature has examined the role of postoperative bracing after lumbar fusion. These studies have aimed to investigate its impact on postoperative pain levels, disability, the occurrence of complications, and the success of fusion. However, there is a dearth of consensus on the imperative nature of postoperative bracing for lumbar degenerative conditions. Frequently, spine surgeons formulate decisions regarding the application of postoperative braces based primarily on clinical experience rather than robust, evidence-based medical data.
This updated meta-analysis aims to provide a thorough examination of the effect of postoperative brace immobilization following lumbar fusion surgery. By pooling the data from multiple studies, we intend to analyze the collective evidence and determine whether postoperative bracing significantly influences postoperative pain, disability, complication rates, and the success of fusion in patients undergoing lumbar fusion. This analysis can offer valuable information for both clinicians and patients when making decisions regarding postoperative care and rehabilitation strategies following lumbar fusion surgery.
Methods
Search Strategy
Systematic electronic searches were performed in the PubMed, Embase, and Web of Science databases to retrieve English-language literature on postoperative bracing interventions following lumbar fusion procedures. The search strategy incorporated subject terms, keywords, and their amalgamation with the following search query: “brace” OR “orthosis” OR “corset” AND “lumbar fusion.” The scope of the search encompassed the period from January 1990 to 20 October 2023.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: (1) patients who have undergone lumbar spinal fusion procedures for the management of degenerative spinal pathologies; (2) studies that incorporate postoperative brace, girth, or other protective gear interventions within a controlled group; (3) primary outcome measures include clinical indicators, complications, and fusion rates; and (4) research designs that adhere to the methodology of randomized controlled trials (RCTs).
Exclusion criteria were as follows: (1) studies not aligning with the focus on postoperative brace therapy; (2) articles not published in the English language; (3) duplicate publications or redundant datasets; and (4) non-RCTs.
Data Extraction
The data extraction process was meticulously conducted independently by 2 researchers involving a comprehensive review of the full text of selected articles.8 The extracted data consist mainly of the following: the first author’s name, publication year, sample size, gender distribution, diagnostic criteria for inclusion, surgical approach, specifics related to brace type and duration of utilization, duration of follow-up, and statistical presentation of results. The primary observables included perioperative parameters (operative time, estimated blood loss, and length of hospital stay), clinical outcomes (visual analog scale [VAS] pain score and Oswestry Disability Index [ODI] functional score), complication rates, and fusion rates. Among clinical outcomes, separate analyses were conducted to assess improvement in VAS and ODI scores in both the early postoperative period (1 month after surgery) and the late postoperative period (at the final follow-up).
Literature Quality and Bias Assessment
The quality assessment of the literature was carried out using the Cochrane Risk of Bias Assessment Tool.9 Within this framework, each of the 7 domains, including randomized sequence generation, allocation concealment, double blinding of implementers and participants, blinded outcome assessment, handling of incomplete outcome data, selective reporting, and potentially other sources of bias, was evaluated. For each domain, 3 levels of bias were ascribed, namely high, low, and unknown.
The evaluation of the quality and bias of the literature was carried out independently by 2 investigators. In the event of discrepancies, resolutions were reached through deliberative discussions, with the possibility of consultation with a third party when necessary.
Statistical Analysis
Statistical meta-analysis was conducted utilizing Review Manager 5.3. For continuous data, the calculations involved the derivation of weighted mean differences (WMD) and the corresponding 95% confidence intervals (CIs). Dichotomous outcomes were expressed as odds ratios (OR) accompanied by their respective 95% CIs. To gauge heterogeneity, the χ 2 test (Q) was employed. In cases where no statistical heterogeneity was observed (P > 0.1, I 2 < 50%), the analysis was executed using a fixed-effects model. Conversely, in the presence of substantial heterogeneity (P < 0.1, I 2 ≥ 50%), the analysis was conducted utilizing a random-effects model. Statistical significance was established at a threshold of P < 0.05. Separate effect size analyses were performed for each article using Cohen’s d test.
To assess the presence of publication bias, funnel plots were incorporated into the analysis to visualize potential asymmetry in the data.
Results
Search Results and Study Characteristics
The initial search yielded a total of 434 pertinent articles. Following the removal of duplicates, the assessment of titles and abstracts, and a comprehensive rescreening of full texts, a final selection resulted in the inclusion of 5 English-language studies (Figure 1). These 5 studies10–14 collectively encompassed a cohort of 362 patients, consisting of 144 men and 218 women (Table).

Flowchart of study selection for meta-analysis. RCT, randomized controlled trial.
Characteristics of included studies.
Mean Operative Time
An analysis of 4 independent studies, involving a combined total of 290 patients, provided data related to the mean duration of the operation. The results of the analysis showed that there were no statistically significant differences in operative time between the brace and nonbrace groups (P = 0.90, WMD: 0.84; 95% CI: −12.60 to 14.27, Figure 2A).

Forest plots comparing (A) operative time in minutes, (B) blood loss in mL, and (C) hospital length of stay in days between the brace and the no-brace groups. IV, Inverse Variance .
Estimated Blood Loss
Two independent studies, involving a total cohort of 163 patients, provided data on the estimated mean blood loss. The results of this analysis did not reveal statistically significant differences between the use of brace and no-brace in terms of blood loss (P = 0.24, WMD: 40.49; 95% CI: −26.87 to 107.85, Figure 2B).
Hospital Length of Stay
Three separate studies, comprising a combined total of 247 patients, provided data on the mean duration of hospitalization. The findings from this analysis demonstrated no statistically significant differences between the utilization of brace and no-brace in terms of length of hospital stay (P = 0.63, WMD: 0.17; 95% CI: −0.52 to 0.85, Figure 2C).
Changes in VAS Score
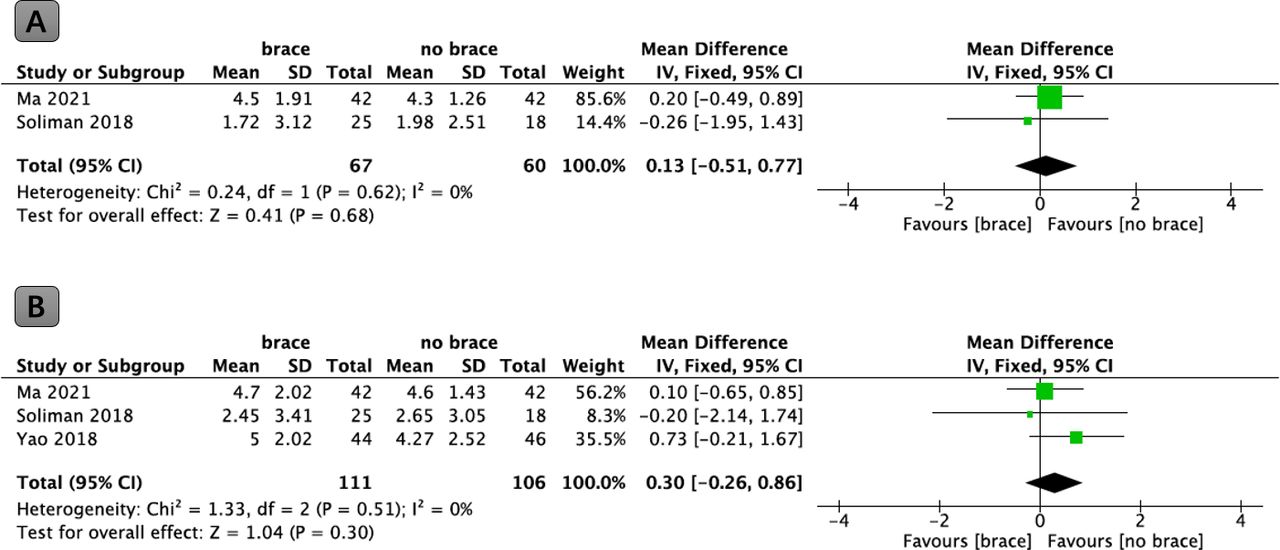
Two studies, involving a total of 127 patients, reported changes in VAS scores for low back pain between the preoperative and early postoperative period (1 month ). The analysis of the results showed that there were no significant differences in the improvement of VAS scores in the early postoperative period in the brace group compared with the nonbrace group (P = 0.68, WMD: 0.13; 95% CI: −0.51 to 0.77, Figure 3A).

(A) Forest plot comparing changes in VAS in the early postoperative period in the brace group compared with the no-brace group. (B) Forest plot comparing changes in VAS at last follow-up period in the brace group compared with the no-brace group. IV, inverse variance; VAS, visual analog scale.
Three studies, involving a total of 217 patients, reported changes in VAS scores for low back pain between the preoperative and final postoperative period. The analysis of the results revealed that there was a relatively better improvement in VAS scores in the late postoperative period in the brace group compared with the no-brace group (4.05 vs 3.84). However, this observed difference did not reach statistical significance (P = 0.30, WMD: 0.30; 95% CI: −0.26 to 0.86, Figure 3B). The 3 studies included reported Cohen’s d values of 0.0503, 0.28, and −0.082. These values suggest that while discernible effects were observed in the study, they were of relatively modest magnitude.
Changes in ODI
Two articles, involving a total of 127 patients, reported changes in ODI scores between the preoperative and early postoperative period. Meta-analysis showed a slightly better improvement in ODI score in the early postoperative period in the brace group compared with the nonbrace group (19.47 vs 18.18), but the difference was not statistically significant (P = 0.34, WMD: 2.83; 95% CI: −2.93 to 8.59, Figure 4A). The 2 studies included reported Cohen’s d values of 0.238 and −0.0375.

(A) Forest plot comparing changes in ODI in the early postoperative period in the brace group compared with the no-brace group. (B) Forest plot comparing changes in ODI at the last follow-up period in the brace group compared with the no-brace group. IV, inverse variance; ODI, Oswestry Disability Index.
Three studies, involving a total of 217 patients, reported changes in ODI scores between the preoperative and final postoperative period. The analysis of the results indicated that there was no significant difference in the improvement of ODI scores in the late postoperative period in the brace group compared with the no-brace group (P = 0.49, WMD: 1.51; 95% CI: −2.77 to 5.78, Figure 4B).
Fusions
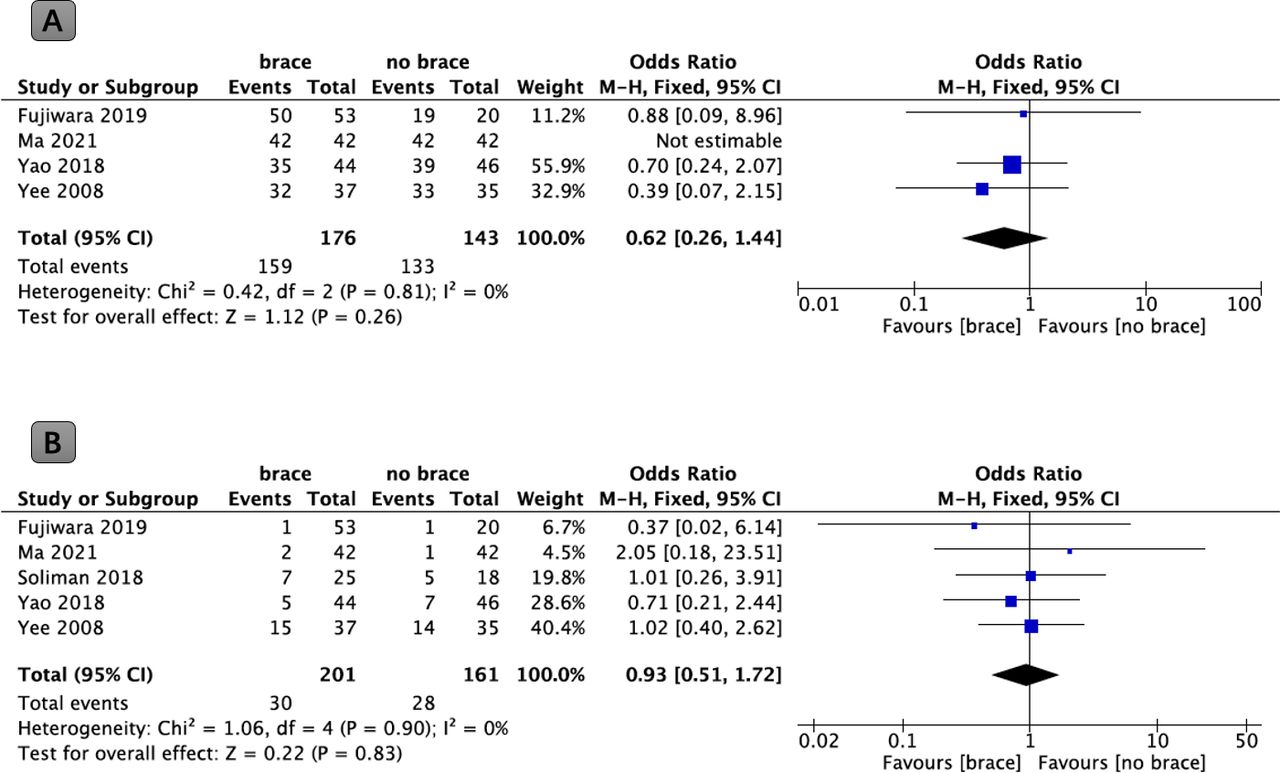
Four studies, involving a total of 292 patients, reported the final fusion rates. The meta-analysis did not identify statistically significant differences in fusion rates when comparing the brace group with the no-brace group (90.3% vs 93.0 %; P = 0.26, OR: 0.62; 95% CI: 0.26–1.44, Figure 5A).

(A) Forest plot comparing fusion rates between the brace and the no-brace groups. (B) Forest plot comparing complications between the brace and the no-brace groups. M-H, Mantel-Haenszel.
Complications
Five studies, involving a total of 362 patients, reported complications between the preoperative and final postoperative period. The analysis of the results revealed that there were relatively low complication rates in the brace group compared with the no-brace group (14.9% vs 17.4%). However, it should be noted that this observed difference did not reach statistical significance (P = 0.83, OR: 0.93; 95% CI: 0.51–1.72, Figure 5B).
Quality Analysis and Publication Bias
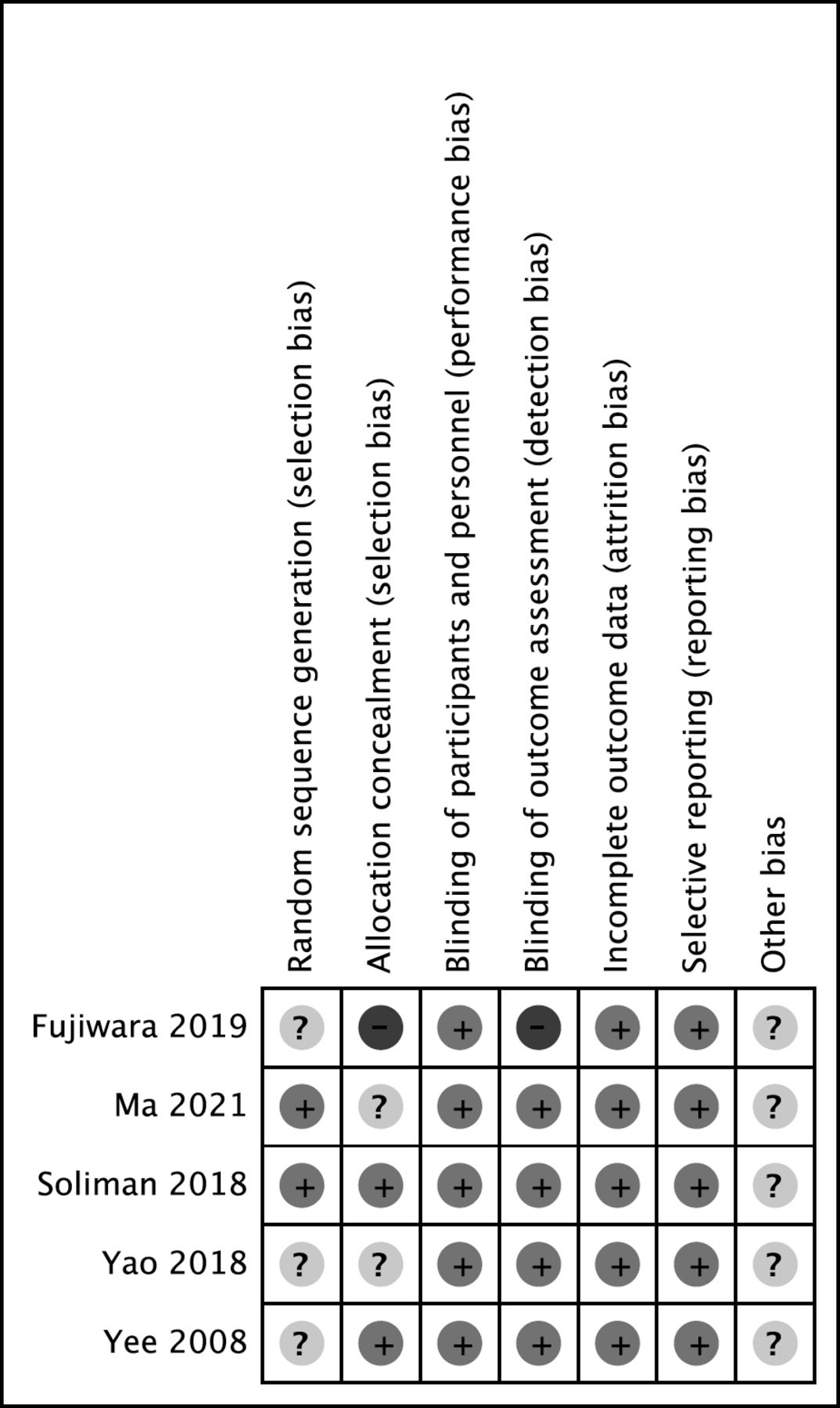
The quality of the included literature was assessed using the Cochrane Risk of Bias Assessment Tool (Figure 6). In general, the studies exhibited a high level of quality, with the potential for bias identified solely in the domains of allocation concealment and blinded outcome evaluation, as observed in the study by Fujiwara et al.

Study quality assessment using the Cochrane Risk of Bias Assessment Tool. Green indicates low risk of bias, yellow indicates unclear risk of bias, and red indicates high risk of bias.
Regarding the evaluation of publication bias in the context of complications, an assessment was performed through visual inspection of the funnel plot (Figure 7).

Funnel plot of publication bias for complications.
Discussion
The present meta-analysis provides a comprehensive evaluation of the influence of postfusion bracing on critical clinical outcomes in the context of lumbar degenerative diseases. The results of our analysis showed that the group that used the brace after lumbar fusion had slightly better ODI improvement in the early postoperative period, slightly greater pain relief in the late postoperative period, and a slightly lower rate of complications compared with the group that did not use the brace. However, it is worth noting that these observed differences did not reach statistical significance.
Effect of Postoperative Bracing on Pain and Functional Disability
The primary objective underlying the adoption of postoperative braces is the improvement of pain and the mitigation of functional impairment in patients. In the context of this study, we conducted an analysis that included 5 RCTs, each exploring the impact of postoperative brace use on postoperative pain and functional outcomes after posterior lumbar fusion. Our findings, although not statistically significant, revealed a subtle advantage in terms of early postoperative functional recovery (19.47 vs 18.18) and eventual pain relief (4.05 vs 3.84) in patients who underwent bracing compared with those who did not.
Previously, spine surgeons have advocated the use of postoperative bracing during the early recovery period after spinal fusion procedures as a protective measure aimed at preventing the emergence of early spinal instability and related symptoms of discomfort.5,14,15 The rationale underpinning this practice is based on the potential of braces to curtail intervertebral motion, ameliorate biomechanical stresses within the operating region, and increase structural support provided by the musculoskeletal system.16,17 Furthermore, it has been posited that the implementation of braces may increase spinal stability by increasing the baseline activation levels of the trunk musculature.5,16 Contrary to these theoretical expectations, our findings suggest that the use of postoperative bracing after posterior lumbar fusion does not provide a statistically significant reduction in postoperative pain or improve the functional prognosis. Emerging evidence underscores the importance of avoiding excessive activity restriction after lumbar spine surgery, as it has been associated with adverse outcomes such as a diminished quality of life, prolonged hospitalization, and heightened rates of rehospitalization.18,19 Hence, it is imperative to consider patient education and early mobilization as pivotal components of postoperative rehabilitation following lumbar fusion procedures to avert the aggravation of distressing pain.20
These findings suggest that postoperative bracing may offer certain advantages in terms of early pain management and functional recovery, which is consistent with conventional wisdom suggesting that bracing may help stabilize the surgical area and provide comfort to patients during the early postoperative phase. Nonetheless, the absence of statistical significance implies that the clinical relevance of these differences may be limited. The use of braces can potentially provide psychological comfort and support for patients, but their impact on long-term pain management and functional recovery may be less pronounced.
Impact of Postoperative Bracing on Fusion Rates and Complications
The efficacy of routine postoperative bracing after posterior instrumented lumbar fusion for degenerative indications, with the aim of improving fusion rates, remains a controversial issue within the medical community.21,22 Several historical studies have indicated that postoperative bracing can potentially increase fusion rates by providing stabilizing support at the surgical site, thus reducing intervertebral motion.23,24 However, our study did not produce findings that demonstrated a significant increase in fusion rates associated with bracing use after posterior lumbar fusion.
One hypothesis to elucidate this observation is the advent of modern spinal instrumentation, which has markedly elevated the rigidity and load-bearing capacity of internal fixation. This technological progress has ostensibly contributed to improved fusion rates among patients undergoing lumbar spine surgery, which is responsible for the relatively limited influence of bracing therapy.25,26 Additionally, early biomechanical investigations have suggested that the wearing of a brace exerts minimal impact on spinal segmental stability and the forces acting upon internal fixation.27,28
In parallel, contemporary research has shed light on the potential importance of well-developed paraspinal musculature in influencing clinical outcomes, encompassing heightened postoperative fusion rates and a reduction in adjacent segmental degeneration.29 However, prolonged use of braces can induce atrophy within paraspinal muscles, thus introducing a potential adverse factor in the interbody fusion process. This intricate interplay underscores the multifaceted nature of the factors influencing the outcomes of the fusion, highlighting that the role of the bracing, while historically valued, can be subject to certain constraints in specific clinical contexts.4
Although the historical literature has documented the contribution of postoperative bracing in promoting improved fusion rates, the contemporary landscape of spinal instrumentation and biomechanical advances introduces a more nuanced perspective. Current paradigms suggest that the added benefits of bracing may be relatively modest, particularly in cases involving lumbar internal fixation fusion, where advancements in internal fixation methodologies and the influence of the paraspinal musculature may be of greater importance.6,13
Complication rates represent a critical aspect of surgical outcomes. Our analysis did not reveal statistically significant differences in the rates of complication associated with the use of postoperative bracing. This suggests that the adoption of bracing did not significantly impact the occurrence of postoperative complications in patients undergoing lumbar fusion for degenerative disease.
Perspectives of Peers
In a prior questionnaire-based study conducted in 2009 that involved the participation of 98 physicians, the necessity of brace immobilization following lumbar spine surgery was examined.30 The study aimed to obtain information on the prevailing practices among physicians regarding the use of orthotic bracing after lumbar spine surgery. The key findings of this survey can be summarized as follows: (1) Lack of Significant Difference: The study found that there were no statistically significant differences in the frequency of orthotic brace use between patients undergoing no instrumented lumbar fusions (surgery without the use of internal fixation devices) and those undergoing instrumented lumbar fusions (surgery with the use of internal fixation devices). This suggests that the decision to use braces did not depend on the type of fusion performed. (2) Duration of Orthotic Use: Among the respondents who employed orthotic braces, it was observed that, in most cases, these braces were prescribed for a duration of 3–8 weeks. This duration likely reflects the early postoperative period when spinal fusion is crucial and stability is required to support the healing process. (3) Reasons for Orthotic Use: The most commonly cited reason for surgeons who opted to use orthotic braces was to limit patient movement. This implies that surgeons believed that immobilization was necessary to support patient recovery and facilitate the fusion process. (4) Lack of Consensus: The study’s conclusion emphasized the lack of consensus among the survey respondents regarding the most appropriate type of brace, the duration of brace use, and the specific clinical indications for immobilization. This finding highlights the variability in clinical practices among physicians in this context.
Subsequent to the 2009 survey, a similar study conducted by the Spine Society of Belgium in 2019 aimed to explore the practices of orthopedic and neurological spine surgeons concerning postoperative brace utilization following lumbar spine surgery.15 This survey involved the participation of 105 surgeons, and its findings can be summarized as follows: (1) Overall Frequency of Brace Use: The study revealed that the overall frequency of brace utilization after lumbar spine surgery was 38%. This suggests that a substantial proportion of surgeons used bracing as part of their postoperative management strategy. (2) Differences Based on Surgery Type: Bracing straps were used more frequently after fusion surgery, with 52% of surgeons opting for brace use in fusion cases, as opposed to 21% after nonfusion surgery. This observation underscores the differing practices in brace utilization based on the type of lumbar surgery performed. (3) Consideration of Brace Use: Most surgeons (approximately 59%) indicated that they considered braces after at least 1 type of lumbar spine surgery. This suggests that brace use was considered in the postoperative care plan for a significant number of patients with lumbar surgery. (4) Orthopedic vs Neurosurgery Spine Surgeons: The study revealed a notable disparity in the prescription of braces between orthopedic and neurosurgery spine surgeons. A significantly higher proportion of orthopedic spine surgeons (73%) prescribed postoperative bracing, compared with neurological spine surgeons (44%). This discrepancy highlights differing practices and preferences between these 2 groups of specialists. (5) Primary Purpose for Bracing: Among the surgeons surveyed, pain relief was identified as the primary purpose of prescribing postoperative bracing, with 67% of the respondents citing this as a key objective. This indicates that bracing was often used to manage postoperative pain. (6) Desire to Improve Fusion Rates: A notable finding was that 42% of surgeons expressed a desire to enhance fusion rates by using bracing after lumbar fusion surgery. This suggests that some surgeons believed that bracing could have a positive impact on fusion outcomes.
A recent study published in 2021 showed that 73 US physicians participated in the questionnaire.31 Most of them had background in orthopedic surgery (78%), had undergone fellowship training (84%), and were affiliated with academic institutions (73%). The survey aimed to investigate the practices and preferences of these surgeons about orthotic use after lumbar spine surgery. The key findings of this survey are summarized as follows: (1) Orthotic Utilization: A significant proportion of the respondents, representing 60%, reported not using orthoses after lumbar spine surgery. This indicates a notable segment of surgeons who do not incorporate orthotic bracing into their postoperative management strategies. (2) Frequency of Orthotic Use: Among surgeons who used orthoses, the overall frequency of orthotic use was 26%. This suggests that for those who chose to employ bracing, it was not consistently used in all cases. (3) Varied Utilization Based on Surgery Type: Respondents tended to use orthoses more frequently after independent lateral spinal fusion, with 43% of surgeons indicating this practice. This observation underscores that the decision to use orthoses was often influenced by the type of lumbar surgery performed. (4) Frequency Differences Between Fusion and Nonfusion Surgery: The survey revealed that the mean frequency of orthotic use after lumbar fusion surgery was 34%, which was notably higher than the mean frequency of orthotic use after nonfusion surgery, at 16%. This indicates that surgeons were more inclined to employ orthotic bracing following fusion procedures. (5) Preferred Type of Brace: The brace most frequently used among the survey respondents was the standard lumbosacral orthosis, which represented 66% of the orthotic choices. This suggests a preference for readily available, standard orthotic solutions. (6) Primary Purpose for Orthotic Use: A significant proportion of the surgeons (42%) used orthoses to improve patient pain. This underscores that pain management was a key objective of orthotic utilization in the postoperative period. (7) Duration of Orthotic Use: Among the surgeons who employed orthoses, the majority (57%) reported the longest duration of use to be in the range of 2–4 months. This suggests that when orthotic bracing was used, it was often incorporated into the early postoperative period.
Limitations
This meta-analysis possesses certain limitations, including a limited number of studies, insufficient information regarding the specific type and duration of postoperative bracing, and the absence of statistically significant differences in clinical outcomes. In addition, cost effectiveness was not addressed in the published studies, and as orthoses can be very expensive, this should be addressed in future studies. Also, patient compliance with bracing was not addressed, so we cannot ascertain whether the braces prescribed were actually worn as directed. However, it is important to emphasize that the absence of statistical significance does not inherently negate the potential advantages associated with postoperative bracing. In particular, this brace may provide psychological comfort to patients and may facilitate their adjustment to the early postoperative phase. This is particularly important because patient comfort and confidence during the recovery period are integral and important aspects of the postoperative experience.
Conclusions
The current meta-analysis revealed the absence of statistically significant disparities between the 2 cohorts despite slightly superior trends in early postoperative functional rehabilitation, enhanced late-stage pain mitigation, and a modest reduction in complications within the brace-immobilized group compared with the nonbrace group following lumbar fusion. Furthermore, fusion rates between the 2 groups exhibited no distinguishable differences.
In the ultimate analysis, the decision-making process for treatment should be highly individualized, taking into meticulous consideration the unique requirements and predilections of each patient. Moreover, this process should remain responsive to the constantly evolving landscape of emerging empirical evidence.
Acknowledgments
The author (G.X.L.) wishes to acknowledge the financial support of the Xiamen Health System Discipline Leaders and their Backup Candidates, Senior Management Talent Training Candidates Training Program (2021).
Footnotes
Funding This research was funded by the Natural Science Foundation of Fujian Province, grant number 2021J05282; funded by Xiamen Municipal Bureau of Science and Technology (3502Z20224033). The funder had no role in the design of the study or collection, analysis, or interpretation of data or in writing the manuscript.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This is a meta-analysis study, so ethics committee approval was not required.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.