


ABSTRACT
Background: To update vertebral augmentation literature by comparing outcomes between vertebroplasty (VP), balloon kyphoplasty (BKP), vertebral augmentation with implant (VAI), and nonsurgical management (NSM) for treating vertebral compression fractures (VCFs).
Methods: A PubMed literature search was conducted with keywords kyphoplasty, vertebroplasty, vertebral body stent, and vertebral augmentation AND implant for English-language articles from February 1, 2011, to November 22, 2016. Among the results, 25 met the inclusion criteria for the meta-analysis. Inclusion criteria were prospective comparative studies for mid-/lower-thoracic and lumbar VCFs enrolling at least 20 patients. Exclusion criteria included studies that were single arm, systematic reviews and meta-analyses, traumatic nonosteoporotic or cancer-related fractures, lack of clinical outcomes, or non–Level I and non–Level II studies. Standardized mean difference between baseline and end point for each outcome was calculated, and treatment groups were pooled using random effects meta-analysis.
Results: Visual analog scale pain reduction for BKP and VP was −4.05 and −3.88, respectively. VP was better than but not significantly different from NSM (−2.66), yet BKP showed significant improvement from both NSM and VAI (−2.77). The Oswestry Disability Index reduction for BKP showed a significant improvement over VAI (P < .001). There was no significant difference in changes between BKP and VP for anterior (P = .226) and posterior (P = .293) vertebral height restoration. There was no significant difference in subsequent fractures following BKP (32.7%; 95% confidence interval [CI]: 8.8%–56.6%) or VP (28.3%; 95% CI: 7.0%–49.7%) compared with NSM (15.9%; 95% CI: 5.2%–26.6%).
Conclusions/Level of Evidence: Based on Level I and II studies, BKP had significantly better and VP tended to have better pain reduction compared with NSM. BKP tended to have better height restoration than VP. Additionally, BKP had significant improvements in pain reduction and disability score as compared with VAI.
Clinical Relevance: This meta-analysis serves to further define and support the safety and efficacy of vertebral augmentation.
INTRODUCTION
Vertebral compression fractures (VCFs) are costly and are becoming even more common as more than 10 000 Americans turn 65 years old each day. In the United States, there are 1.5 million VCFs annually, and worldwide a vertebral fracture occurs every 22 seconds.1–3 Symptomatic fractures usually present with sudden onset of back pain and functional debilitation in an elderly patient with osteoporosis, though many fractures may be asymptomatic. VCFs are expensive to treat, costing around $17 billion per year.4,5 Morbidities associated with VCFs are substantial and can result in permanent loss of mobility and quality of life and lead to substantial disability.6
In addition, the deconditioning that affects patients with VCFs leads to mortality at a far higher rate than in age-matched controls.7,8 Increased mortality associated with VCFs has been well established for quite some time, but effects on mortality when patients undergo treatment with vertebral augmentation has only been described recently.9–12 Edidin et al13 reported significant reduction in morbidity and mortality in over a million patients with VCFs treated with vertebral augmentation as compared with patients treated with nonsurgical management (NSM).
Vertebral augmentation, including kyphoplasty and vertebroplasty (VP), have been accepted treatments for VCFs for decades. Balloon kyphoplasty (BKP) has had a large body of data supporting its use since receiving 510(k) clearance in 1998. More recently, interventionalists have started using implants and vertebral body stenting (VBS) in vertebral augmentation. One such implant is Kiva (Benvenue Medical, Inc, Santa Clara, California), a polyetheretherketone implant placed over a nitinol wire. Kiva was approved by the US Food and Drug Administration in 2014 after a randomized controlled trial (RCT) showed noninferiority to BKP, while maintaining an optimal safety profile and significantly improving patients' pain and function.16 VBS uses an expandable metal stent to restore vertebral height and currently is only available in Europe. Level I evidence concludes that although VBS is noninferior to BKP, in terms of patient outcomes, it is associated with a higher number of material related complications.15 The SpineJack (Vexim, SA, Balma, France), CE marked for use in Europe and other countries around the world, showed superiority to BKP in restoring VCF heights in a single-center trial16 and in a cadaver study.17 SpineJack is currently undergoing a comparison study with BKP in Europe and may be approved for use in the United States as early as 2018.
In 2009, 5 major societies developed a consensus statement on percutaneous vertebral augmentation,18 concluding that “percutaneous vertebral augmentation with vertebroplasty and kyphoplasty is a safe, efficacious, and durable procedure in appropriate patients with symptomatic osteoporotic and neoplastic fractures when performed in a manner in accordance with published standards.” Also in 2009, 2 randomized trials on VP as treatment for osteoporotic vertebral fractures (Buchbinder et al19 and Kallmes et al20) were published in the New England Journal of Medicine (NEJM). These studies found no significant difference between vertebroplasty and sham treatment and prompted a debate on the effectiveness of surgical treatment of VCFs, as well as numerous changes in clinical recommendations and adverse decisions on procedure reimbursement. Later, 2 blinded RCTs demonstrated statistically significant benefits in pain improvement and functional improvement of vertebroplasty when compared with sham treatments.21,22 The impact of these studies is being evaluated concurrently.
The purpose of this meta-analysis was to update the existing body of literature using recent highest-quality data to assess the effectiveness of BKP and VP, including vertebral augmenation with implant, compared with NSM in the treatment of patients with painful VCFs. Intertreatment analysis was also peformed. This meta-analysis also provided an updated review to guide an evidence-based approach to the use of vertebral augmentation procedures. This will provide an organizational framework to better define the heterogenous body of vertebral augmentation literature by analyzing the newest Level I and Level II studies.
MATERIALS AND METHODS
Information Source
PubMed, for articles published from February 1, 2011, to November 22, 2016.
Search
A PubMed search was performed with the assistance of a research librarian using keywords kyphoplasty, vertebroplasty, vertebral body stent, and vertebral augmentation AND implant for articles published in the English language from February 1, 2011, to November 22, 2016, resulting in 937 articles. The electronic search strings used by the research librarian to perform this PubMed search are included in Appendix I.
Eligibility Criteria and Study Selection
Inclusion criteria were as follows: prospective comparative studies of vertebral augmentation procedures, studies enrolling at least 20 patients, and studies performed for mid-/lower-thoracic and lumbar vertebral fractures (T5 through L5) due to osteoporosis.
Exclusion criteria were as follows: single-arm studies, kyphoplasty studies not using inflatable balloons, non-English language studies, systematic reviews and meta-analyses, traumatic nonosteoporotic or cancer-related fracture studies, studies without clinical outcomes, non–Level I and non–Level II studies, and studies involving sacroplasty. Vertebral body stenting and KIVA procedures were grouped as a separate treatment group (vertebral augmentation with implants, or “VAI”).14,23–25
Review Protocol and Data Collection Process
A systematic review protocol was established to determine which papers satisfied the inclusion/exclusion criteria and qualified for the meta-analysis. Abstracts for the 937 articles were reviewed by each of 2 reviewers to identify those that failed to meet the inclusion/exclusion criteria. For studies in which the abstracts were not adequate to reach a determination for inclusion/exclusion, the articles were reviewed for further assessment. Any discrepancies for qualification for the meta-analysis between the 2 reviewers were discussed and resolved together. After systematic review, 28 of these studies satisfied the inclusion/exclusion criteria. Follow-up length for these studies ranged from 6 months to 5 years.
Data Items
Outcomes of interest for this meta-analysis were as follows:
Optimal intervention time/age of compression fracture
Cost/benefit of surgical intervention versus NSM
Economic considerations
Quality of life (QOL) improvement as measured by the Short-Form 36 Survey Physical Component Summary (SF-36 PCS), SF-36, EuroQol-5D (EQ-5D), Quality of Life Questionnaire of the European Foundation for Osteoporosis (QUALEFFO), and low-back pain
Disability improvement as measured by the Roland Morris Disability Questionnaire (RMDQ) score, disability days, Oswestry Disability Index (ODI), and the time up-and-go (TUG) metric
Pain scores (10-point back pain, SF-36 bodily pain, visual analog scale [VAS], numeric rating scale, numerical visual scale)
Subsequent adjacent fractures and overall subsequent fractures
Cement extravasation
Spinal canal extravasation
Vertebral height restoration (anterior, midline, posterior)
Kyphotic angle
Serious adverse events (complications)
STATISTICAL METHODS
Data Collection Process
Data was extracted from each study from the provided tables and figures as well as the text in the articles. Extracted data was confirmed for accuracy by 2 reviewers. For each study, the standardized mean difference between baseline and endpoint for each outcome was calculated, as the scale for some outcomes varied across studies. For outcomes measured over time, the last time observed was considered the endpoint.
Synthesis of Results
Treatment groups were pooled using random effects meta-analysis to provide an overall estimate of effect. Pairwise comparisons were implemented using the z test.26 Summary statistics were used to calculate mean and standard deviation if unknown.27 To assess heterogeneity, I2 statistics were calculated for each summary effect size.27 A minimum of 3 studies in each treatment group were required to perform analysis to estimate a within-group effect. Mean effect sizes with 95% confidence intervals in parentheses are reported. The analysis was completed in SAS v.9.4 (SAS Inc, Cary, North Carolina).
Summary Measures
In addition to applying the random effects model for a pooled estimate, response ratios of standardized means between treatment groups within studies were calculated for outcomes of interest. This only included studies that had specific outcome measures for both treatment groups that were being compared.
RESULTS
Of the 28 studies, 3 did not report any outcomes of interest and were excluded, leaving 25 studies for meta-analysis. Six studies compared BKP to NSM (4 randomized versus 2 nonrandomized). Six studies compared VP to NSM (5 randomized versus 1 nonrandomized). Nine studies compared BKP to VP (5 randomized versus 4 nonrandomized). Four studies compared BKP to VAI (3 randomized versus 1 nonrandomized). Of the 25 studies included in the meta-analysis, 10 were Level I studies and 15 were Level II studies, based on the American Academy of Orthopaedic Surgeons guidelines for level of evidence.28 Due to the requirement of 3 studies to estimate within-group effect, some outcomes of interest (optimal intervention time/age of fracture, cost/benefit analysis, economic considerations, cement extravasation, spinal canal extravasation, and serious adverse events) could not be reported, as the minimum number of studies was not reached. Table 1 summarizes the findings of each study included in the meta-analysis. Table 2 summarizes the treatment comparison results across pooled studies, showing standardized mean differences of change from baseline for each treatment group and P values for treatment comparisons.
Summary of study findings.
Extended.
Continued. Extended.
Continued. Extended.
Treatment comparison results across pooled studies indicating standardized mean differences of change from baseline and respective P value. (Note: n/a indicates insufficient number of studies for analysis.)
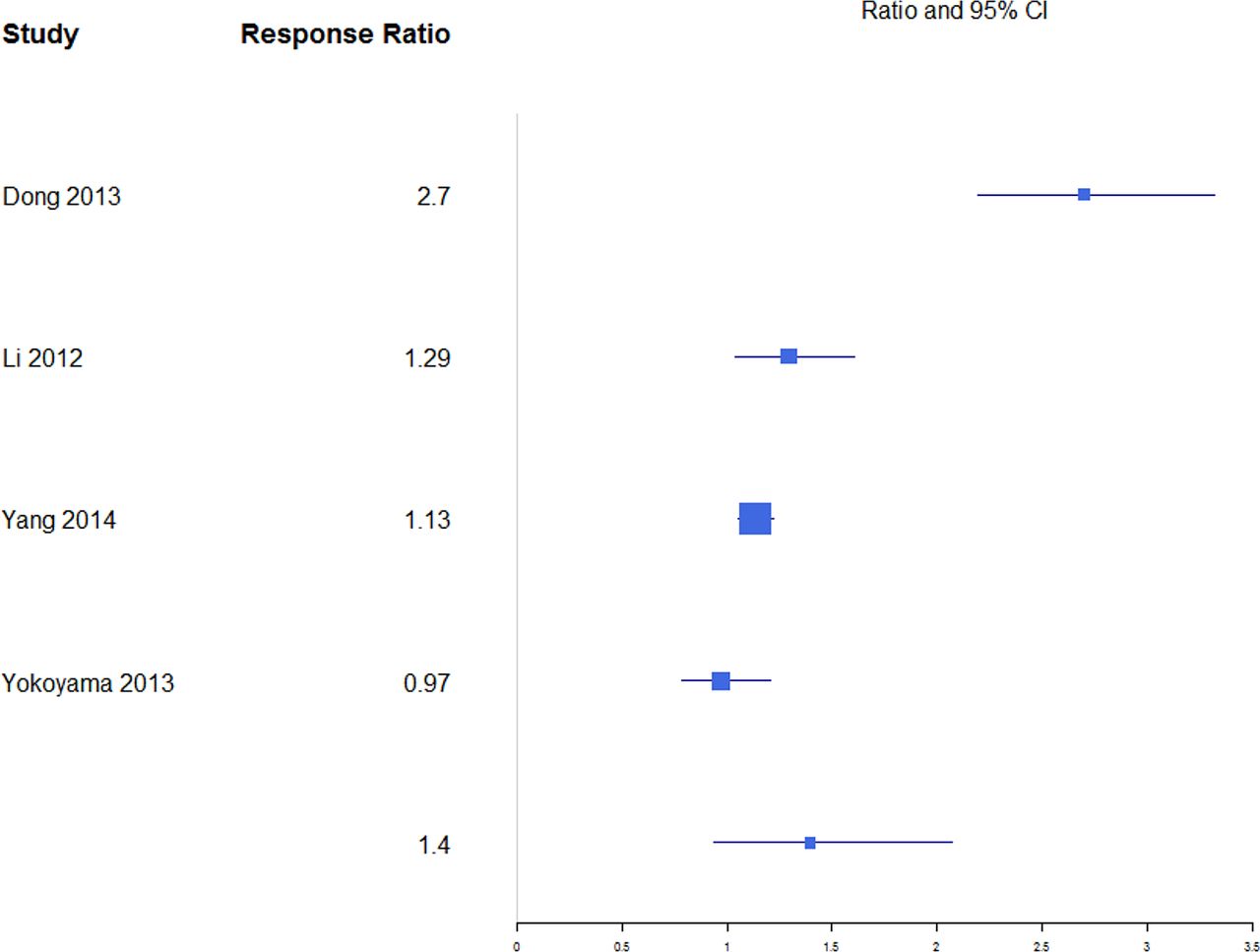
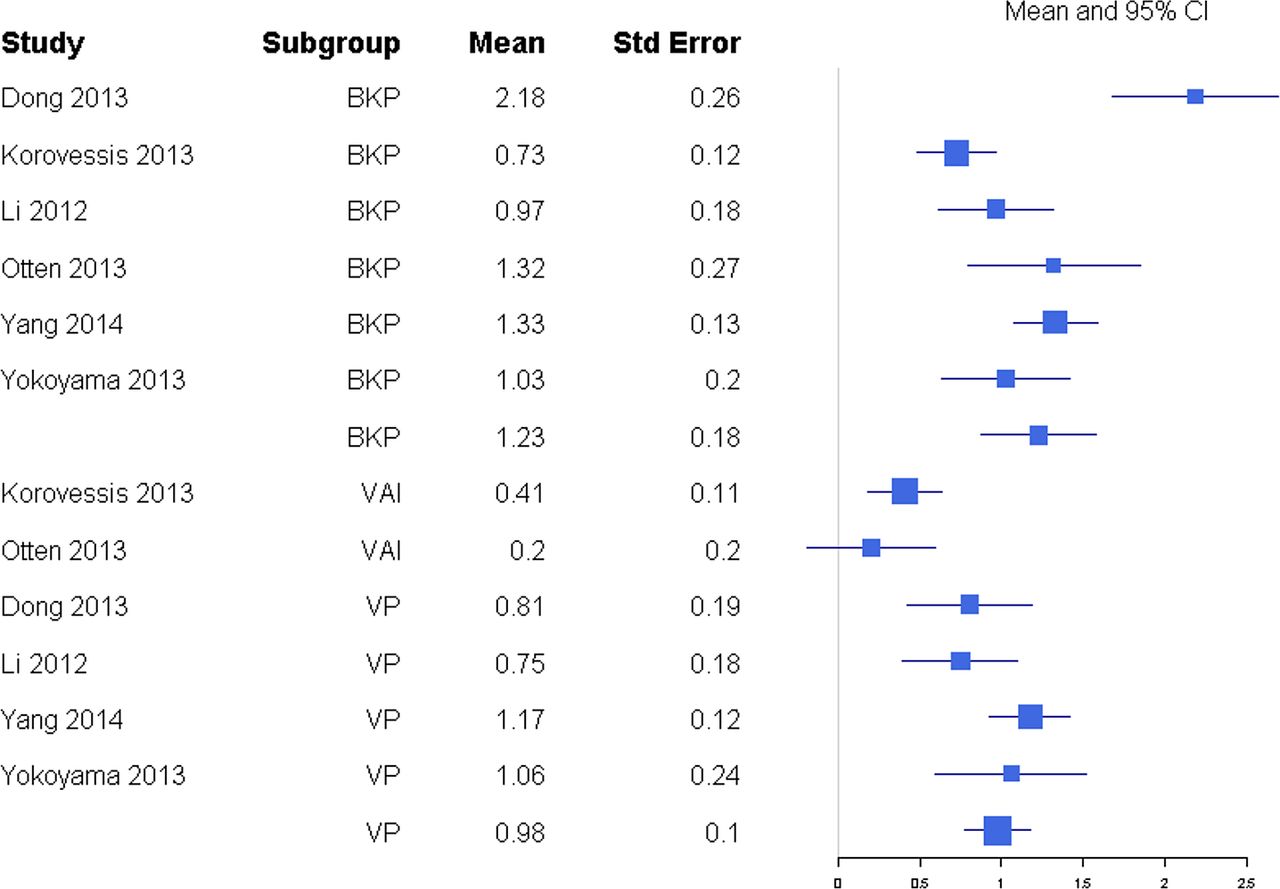
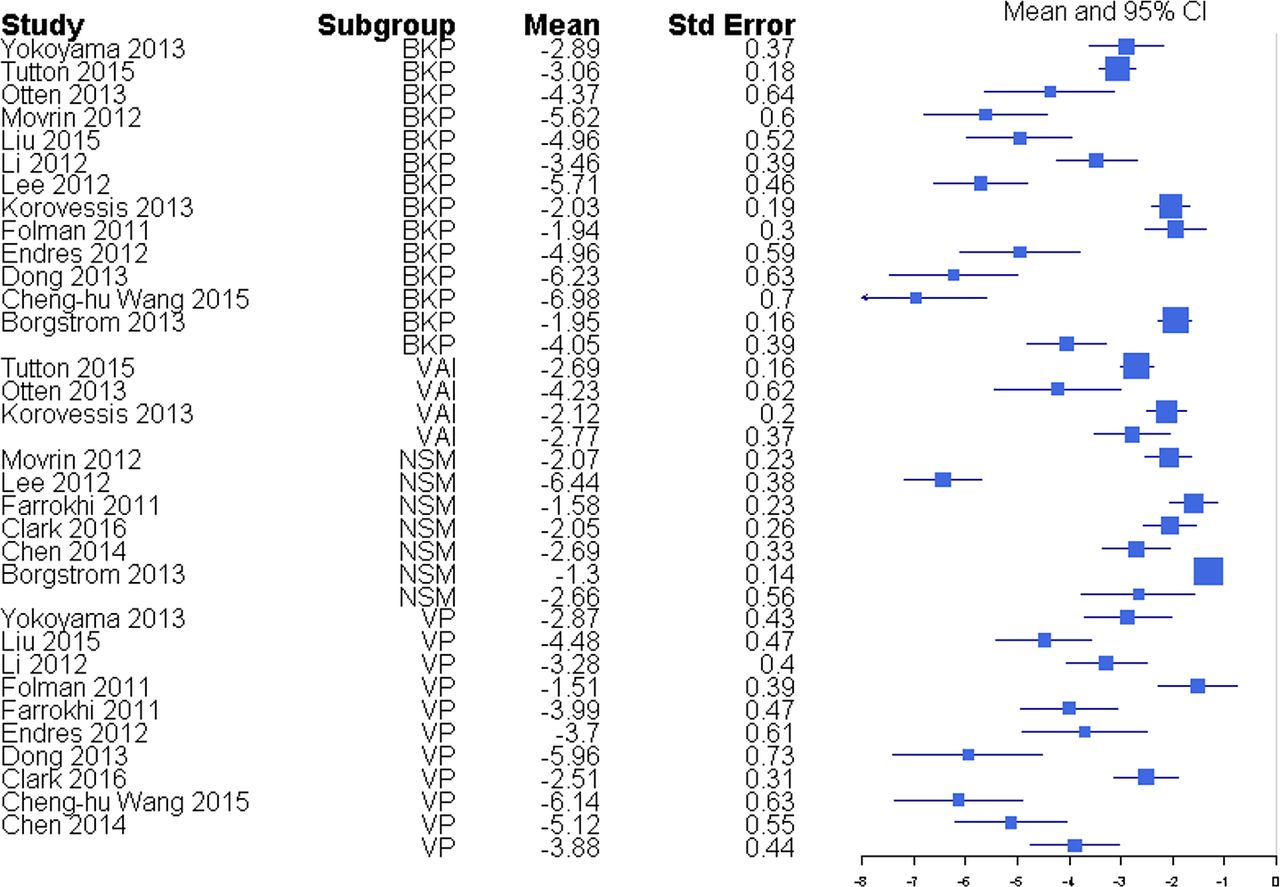
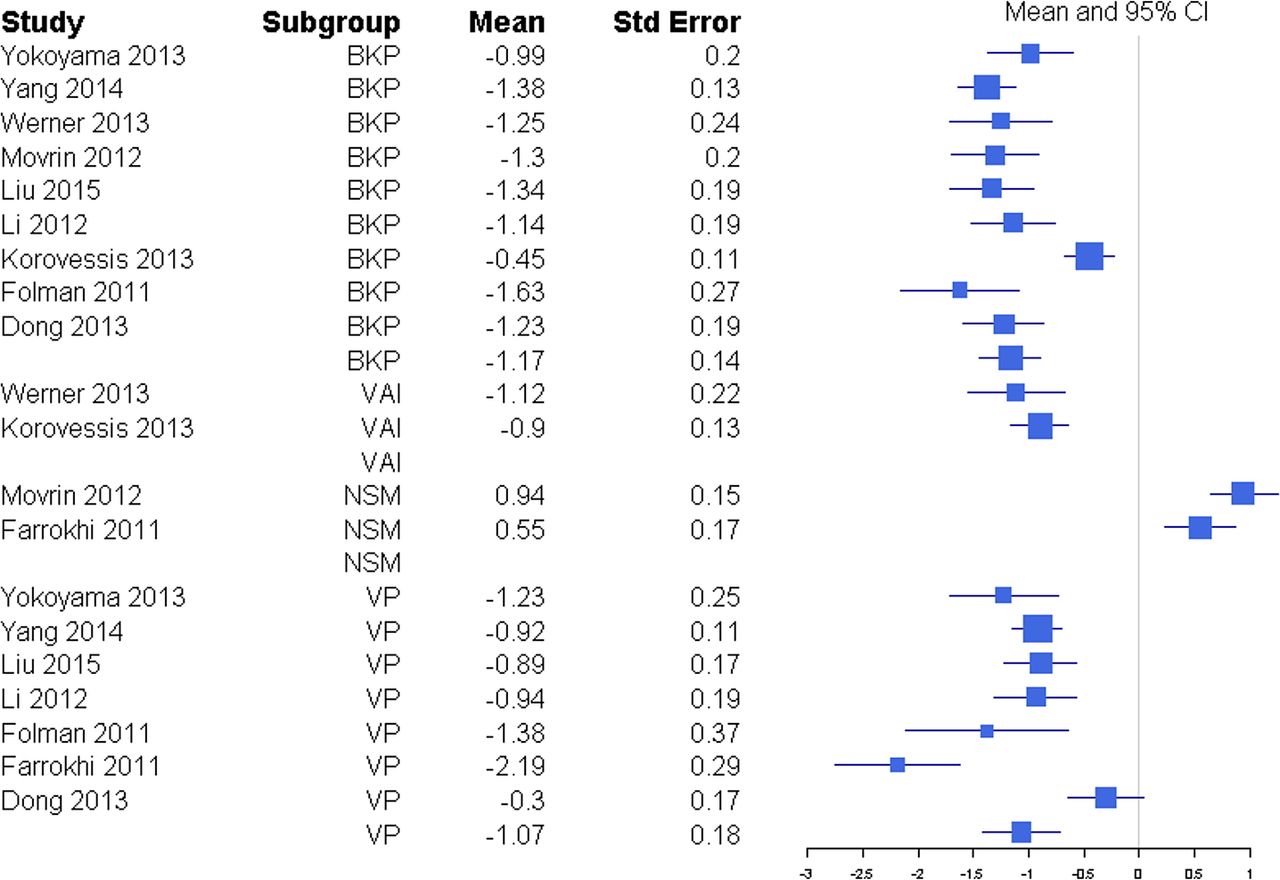
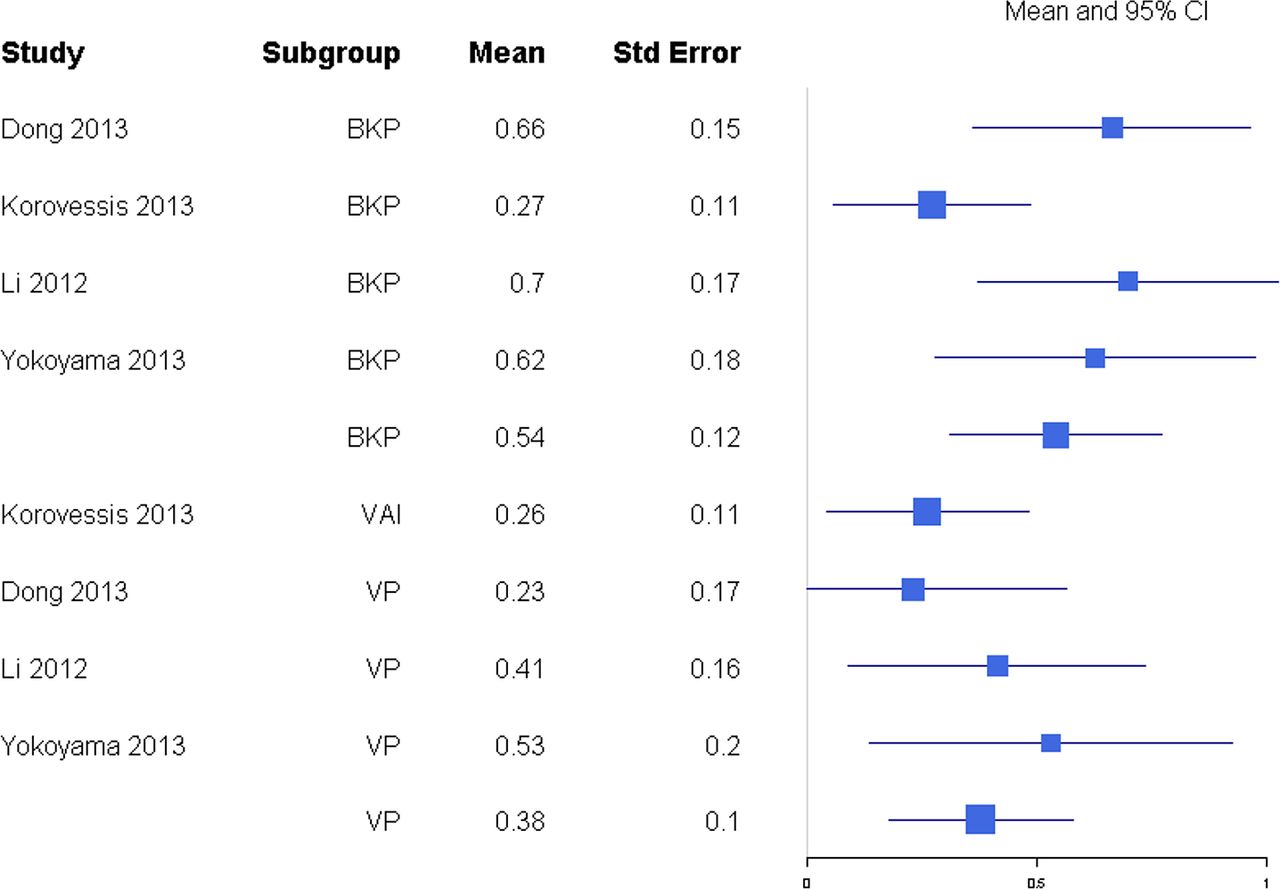
Pain was reported through multiple metrics, including 10-point back pain scores, SF-36 bodily pain score, and VAS score (Table 1), but there was a sufficient number of studies to only compare VAS scores (Table 2). BKP showed some tendency for slightly higher change in VAS scores from baseline than VP and VAI for the majority of studies with an overall response ratio of 1.13 (0.45, 2.83; Figure 1) and 1.04 (0.26, 4.20; Figure 2), respectively. In terms of pain reduction from baseline, BKP (−4.05 [−4.81, −3.29]) was not significantly different than VP (−3.88 [−4.74, −3.02], P = .774) but showed significantly greater improvement compared with NSM (−2.66 [−3.75, −1.56], P = .041; Figure 3) and VAI (−2.77 [−3.51, −2.04], P = .018). The difference between VP and NSM in terms of pain reduction was not significant (P = .085). There was substantial heterogeneity in the BKP (I2 = 95), VP (I2 = 86), VAI (I2 = 84), and NSM (I2 = 96) arms.
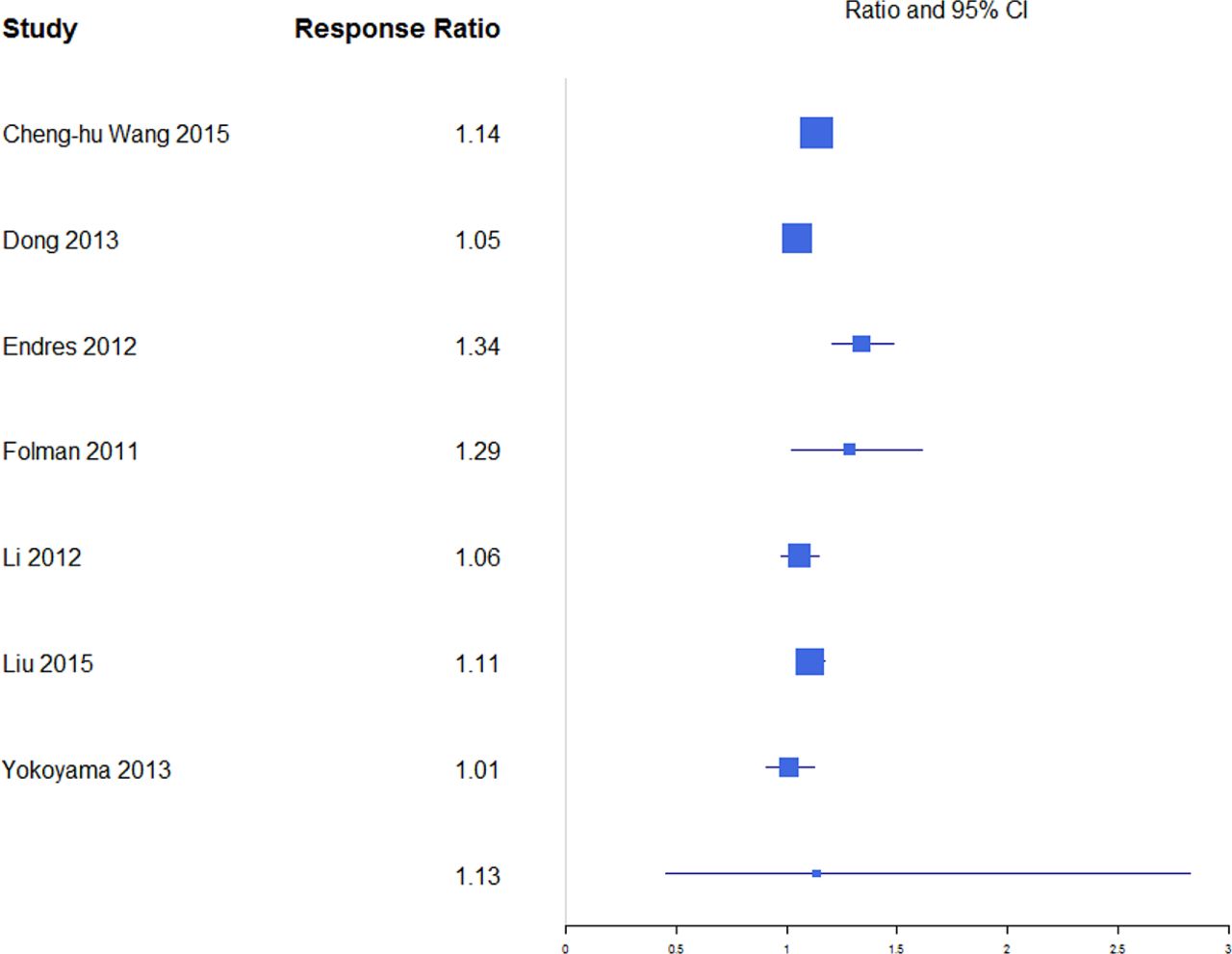
Response ratios of standardized mean differences for visual analog scale pain scores comparing balloon kyphoplasty with vertebroplasty treatment.

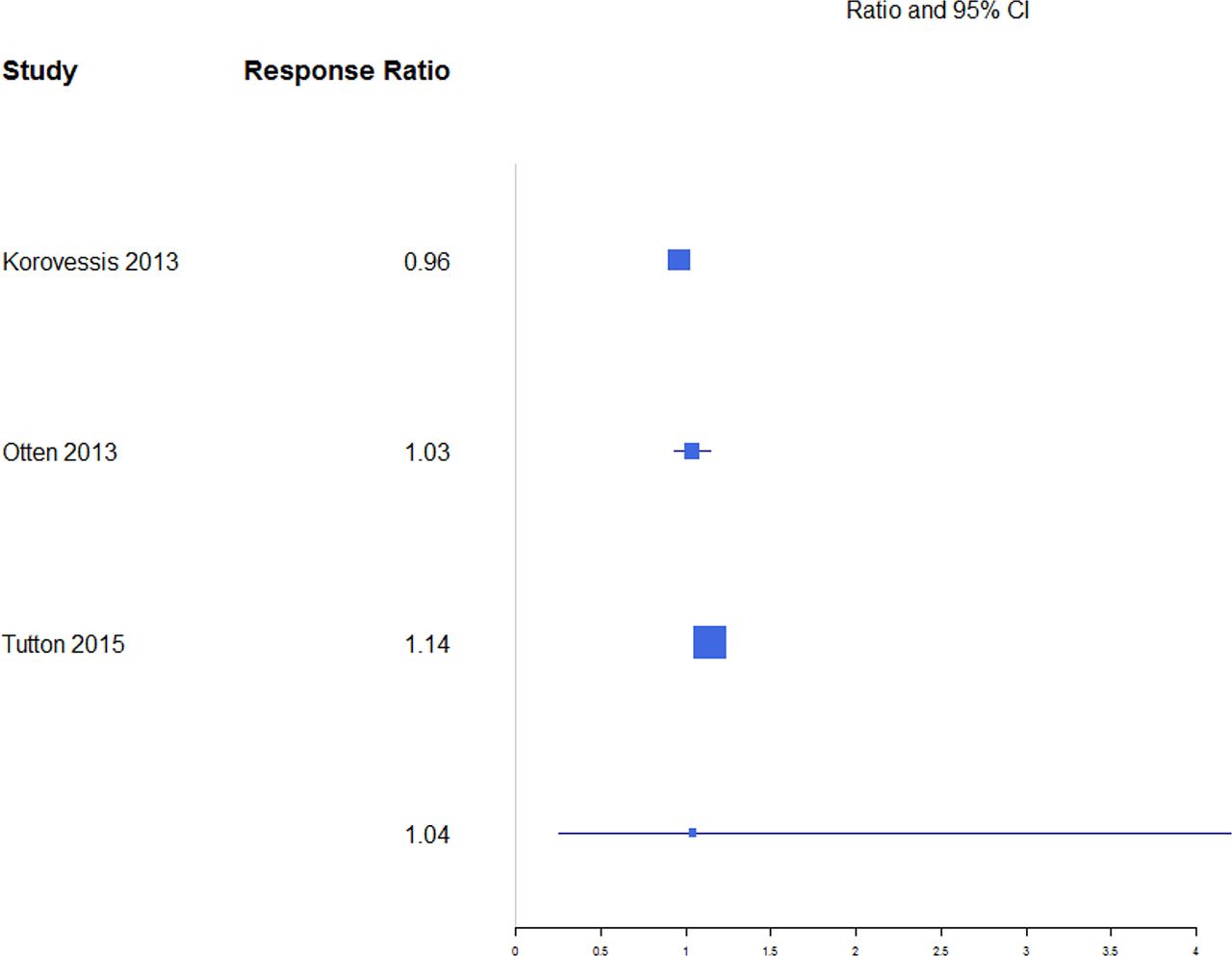
Response ratios of standardized mean differences for visual analog scale pain scores comparing balloon kyphoplasty with vertebral augmentation with implants treatment.
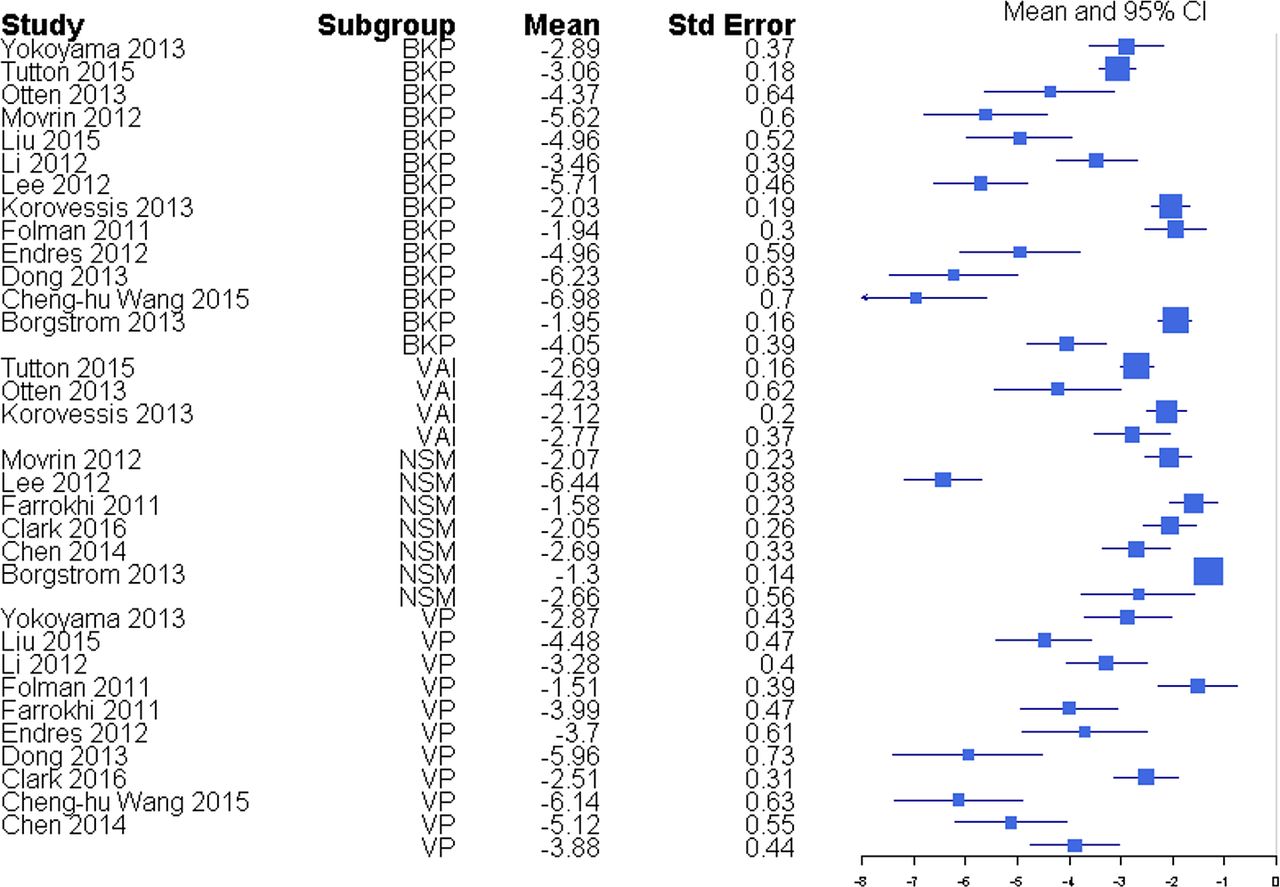
Standardized mean differences of change from faseline for visual analog scale pain scores. Abbreviations: BKP, balloon kyphoplasty; VAI, vertebral augmentation with implants; NSM, nonsurgical management; VP, vertebroplasty.
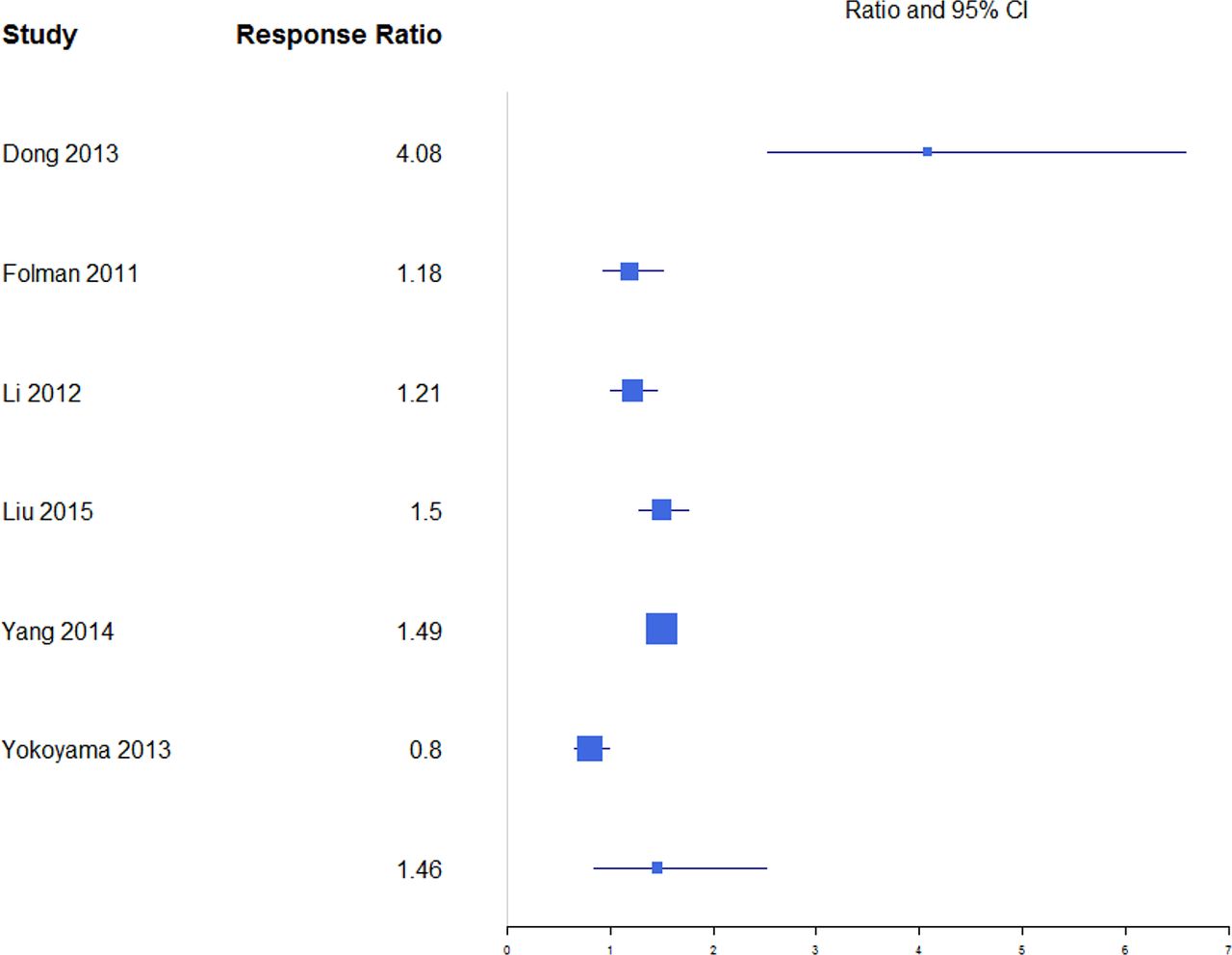
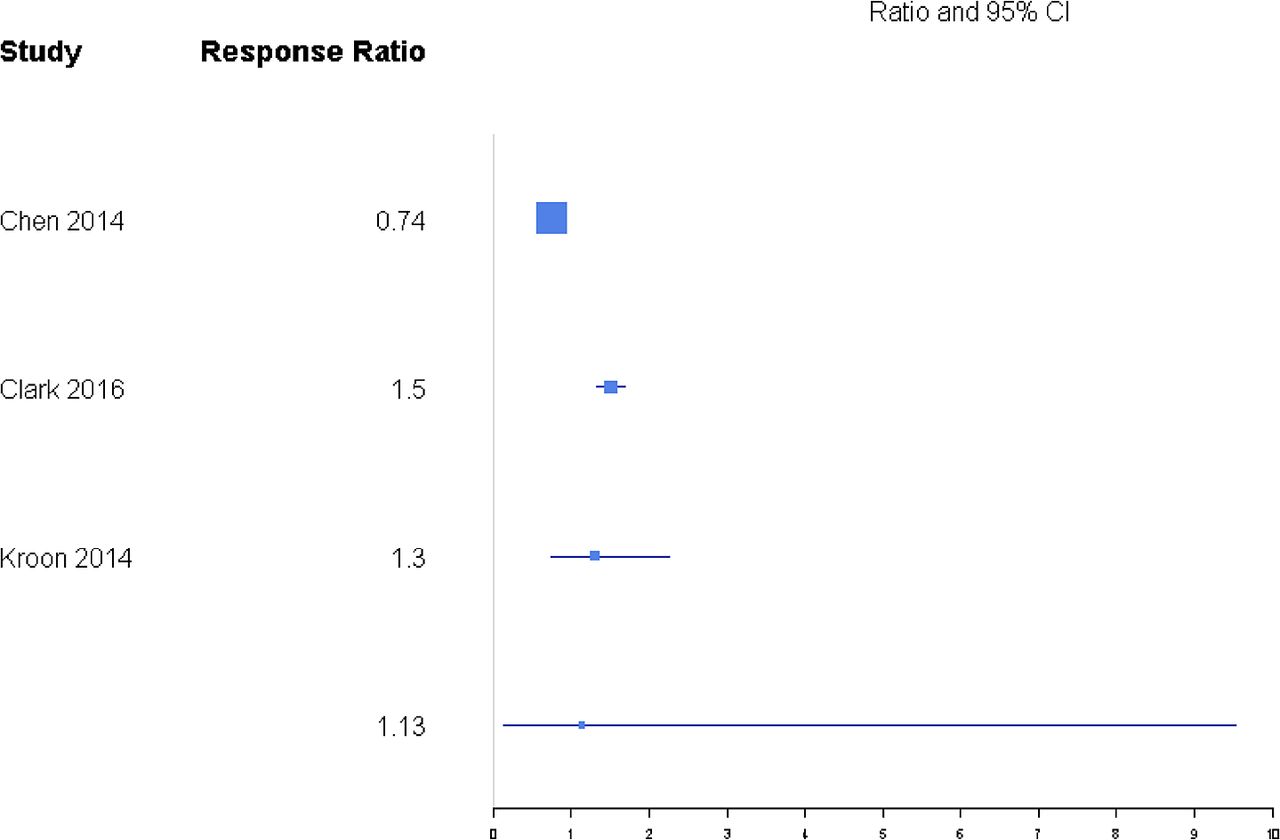
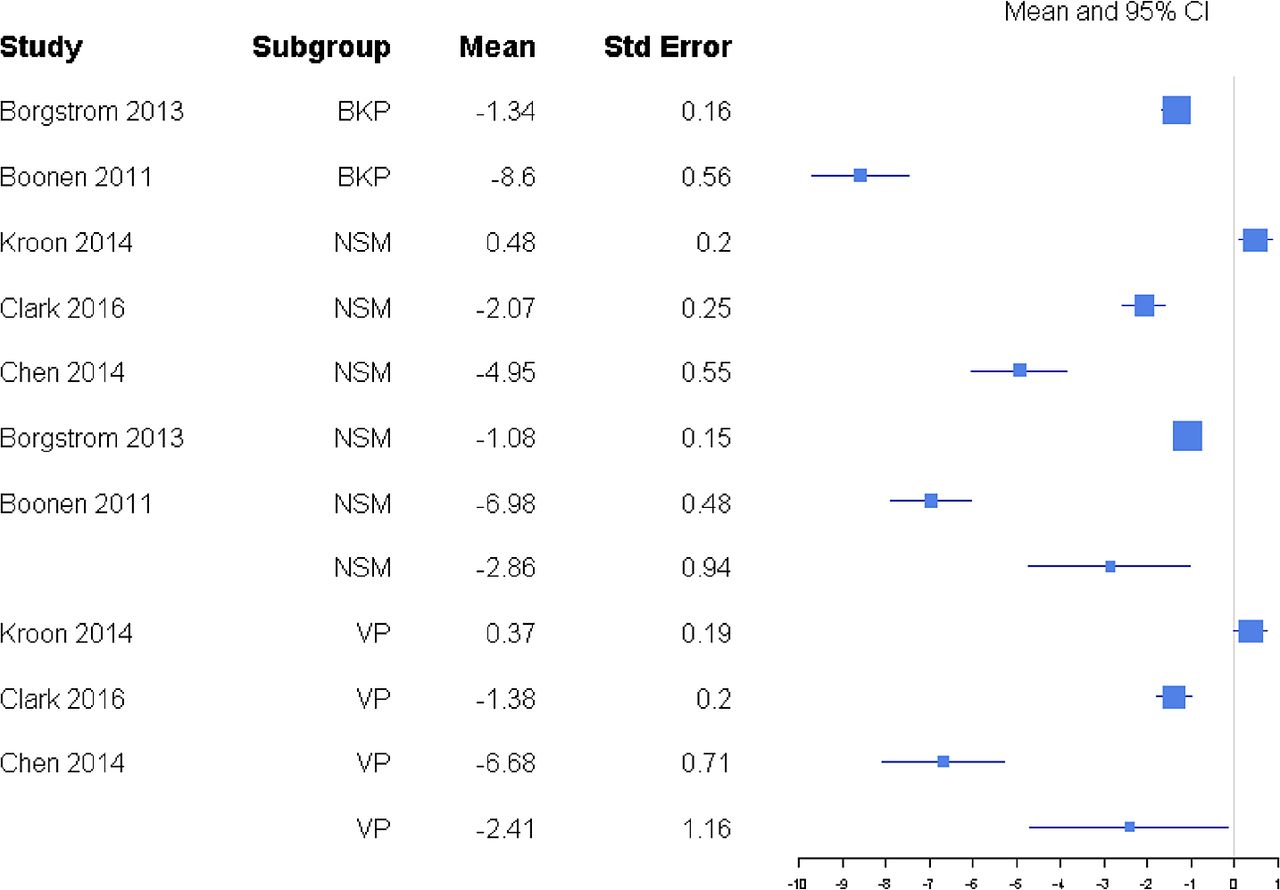
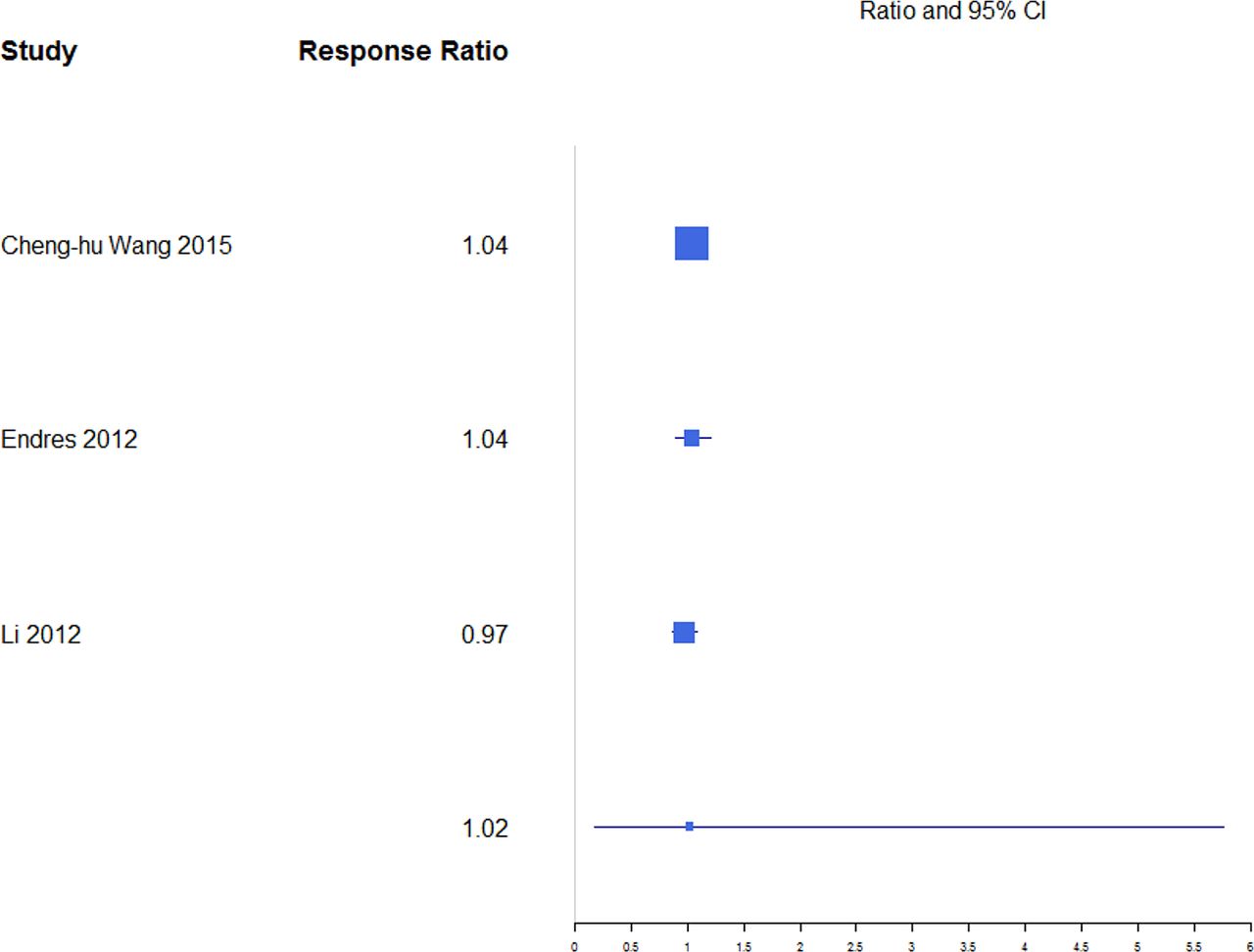
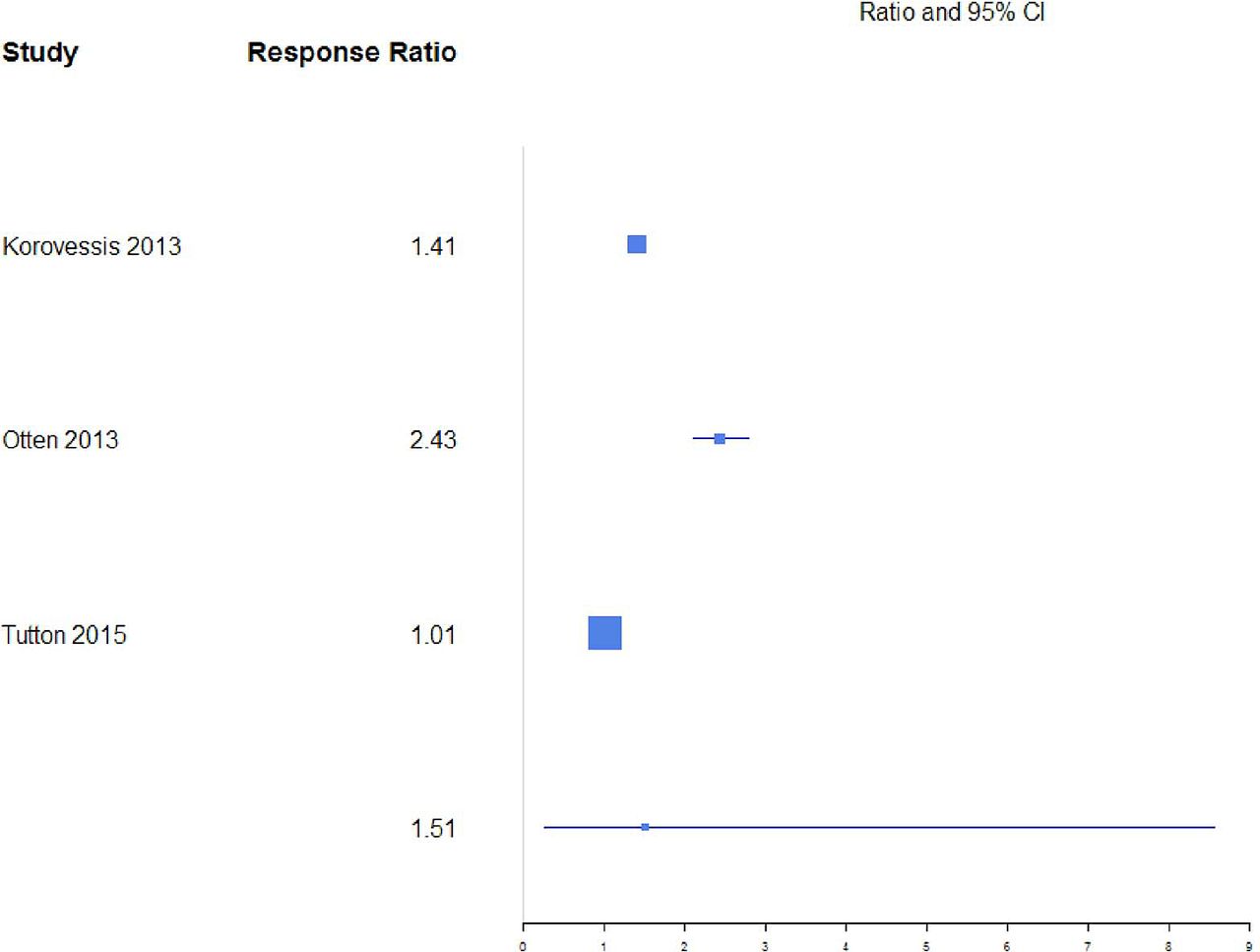
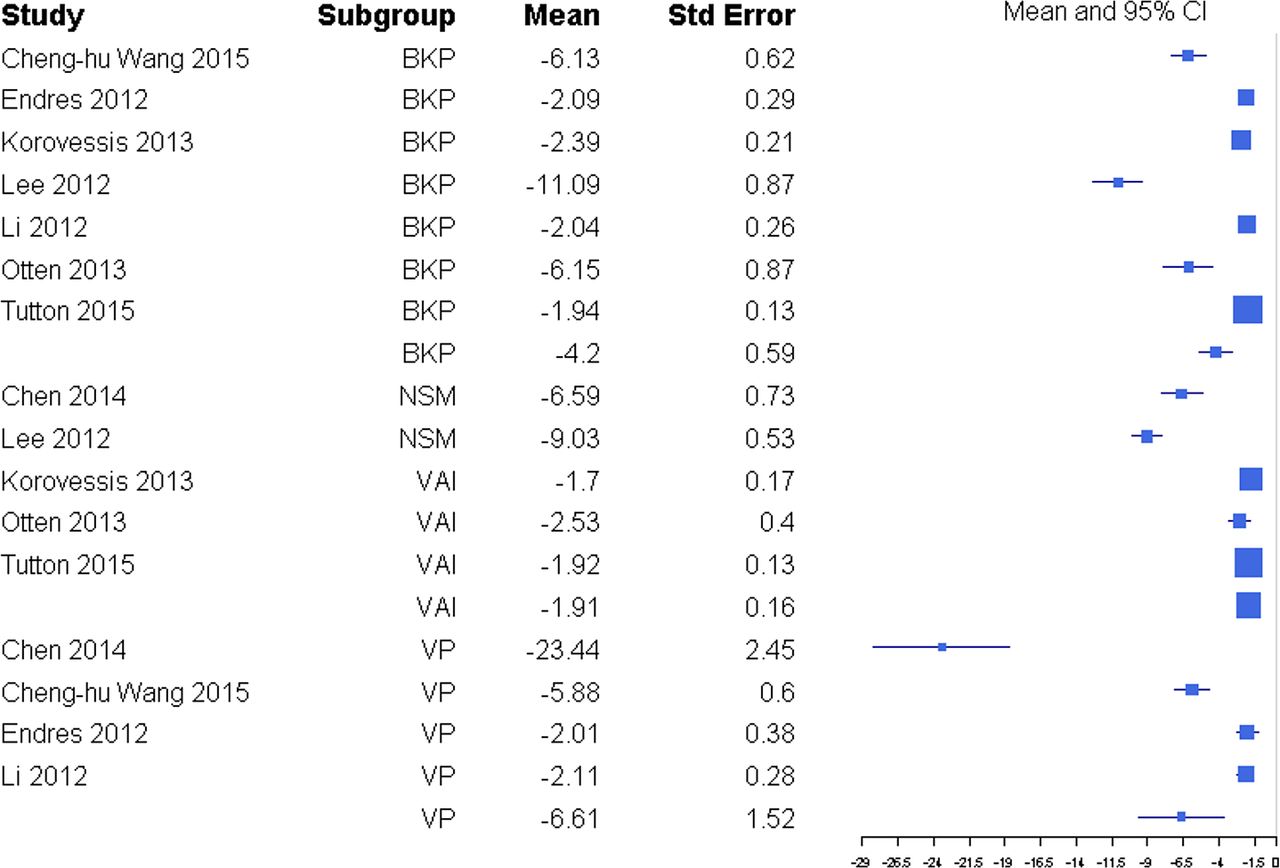
Disability was reported through RMDQ score, disability days, ODI, and TUG metrics (Table 1), but there was a sufficient number of studies to only compare ODI and RMDQ (Table 2). The response ratio plot of RMDQ scores showed NSM had some tendency for slightly higher changes from baseline compared with VP with a response ratio of 1.13 (0.13, 9.53; Figure 4). The overall mean effect of RMDQ for the NSM group was −2.86 (−4.71, −1.01) and for the VP group was −2.41 (−4.68, −0.15) with no significant difference (P = .763; Figure 5). A response ratio plot of ODI scores showed that BKP treatment groups had some tendency to have slightly higher changes from baseline compared with VP groups with a response ratio of 1.02 (0.18, 5.76; Figure 6) and compared with VAI with a response ratio of 1.51 (0.27, 8.58; Figure 7). For disability index (ODI) reduction, BKP (−4.20 [−5.35, −3.05]) showed slightly less improvement versus VP (−6.61 [−9.59, −3.63], P = .140; Figure 8). The reduction in ODI was significantly higher for BKP than VAI (−1.91 [−2.22, −1.61], P < .001). There was substantial heterogeneity in the BKP (I2 = 96) and VP (I2 = 97) arms but less observed heterogeneity in the VAI group (I2 = 47).

Response ratios of standardized mean differences for Roland Morris Disability Questionnaire comparing nonsurgical management with vertebroplasty treatment.

Standardized mean differences of change from baseline for Roland Morris Disability Questionnaire. Abbreviations: BKP, balloon kyphoplasty; NSM, nonsurgical management; VP, vertebroplasty.

Response ratios of standardized mean differences for Oswestry Disability Index comparing balloon kyphoplasty with vertebroplasty treatment.

Response ratios of standardized mean differences for Oswestry Disability Index comparing balloon kyphoplasty with vertebral augmentation with implants treatment.
Standardized mean differences of change from baseline for Oswestry Disability Index. Abbreviations: BKP, balloon kyphoplasty; VAI, vertebral augmentation with implants; VP, vertebroplasty.
Quality of life (QOL) was reported through SF-36 PCS, EQ-5D score, and generally through the SF-36 metric. Due to the limited number of studies, overall mean effects were not calculated for BKP and VP. For quality of life (EQ-5D), NSM showed a mean improvement of 1.41 (−0.29, 3.11). There was substantial heterogeneity in the NSM (I2 = 98) arm.
A response ratio plot comparing BKP with VP for kyphotic angular correction (KAC) (Figure 9) showed high variability across studies, with an overall mean estimate of 1.46 (0.84, 2.51) for response ratios. A forest plot of standardized mean differences from baseline for KAC is shown in Figure 10. There were not enough studies to complete an analysis of the NSM or VAI group. For KAC, BKP (−1.17 [−1.45, −0.89]) showed more kyphotic angle reduction than VP (−1.07 [−1.42, −0.72]; P = .658), although the difference is not significant. There was substantial heterogeneity in the BKP (I2 = 82) and VP (I2 = 83) arms.
Response ratios of standardized mean differences for kyphotic angular correction comparing balloon kyphoplasty with vetebroplasty treatment.

Standardized mean differences of change from baseline for kyphotic angular correction. Negative values indicate reduction in kyphosis angle. Abbreviations: BKP, balloon kyphoplasty; VAI, vertebral augmentation with implants; NSM, nonsurgical management; VP, vertebroplasty.
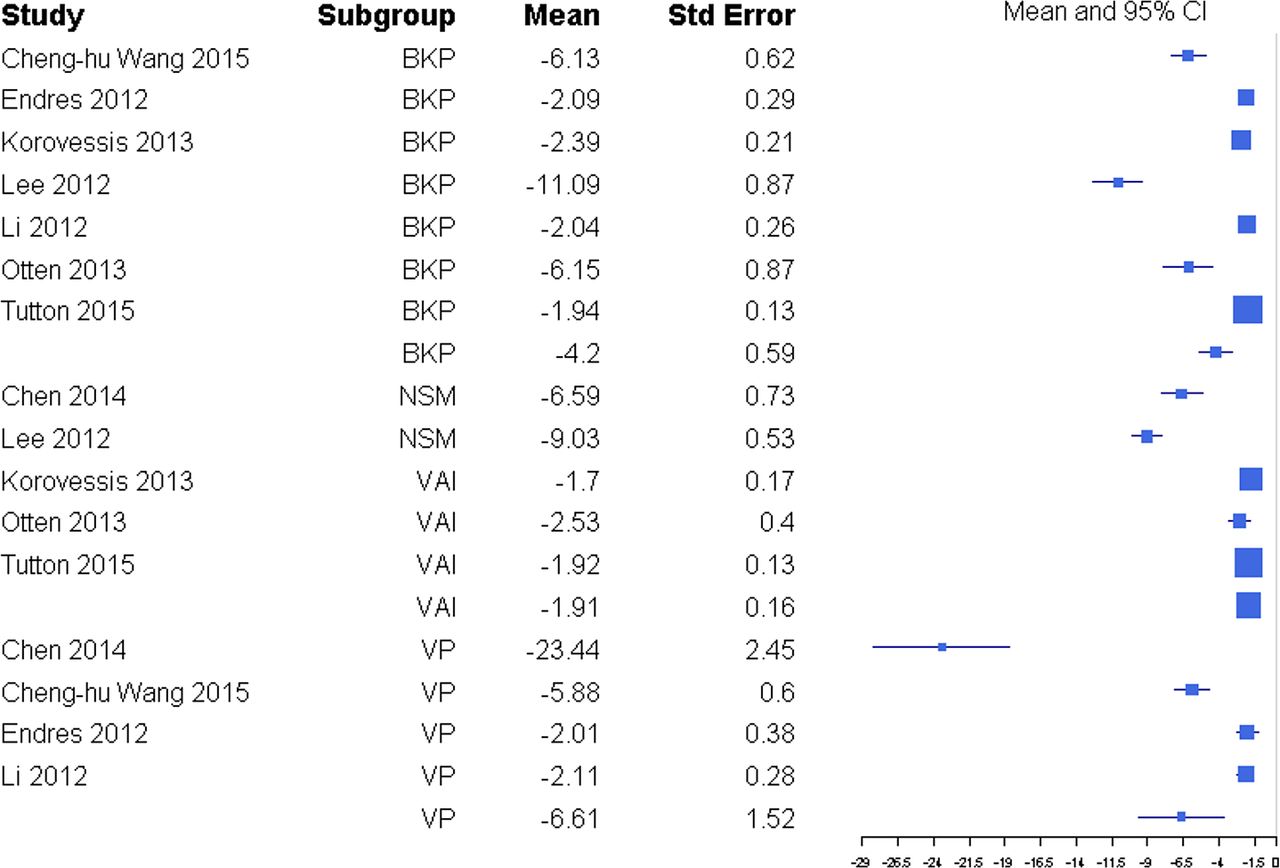
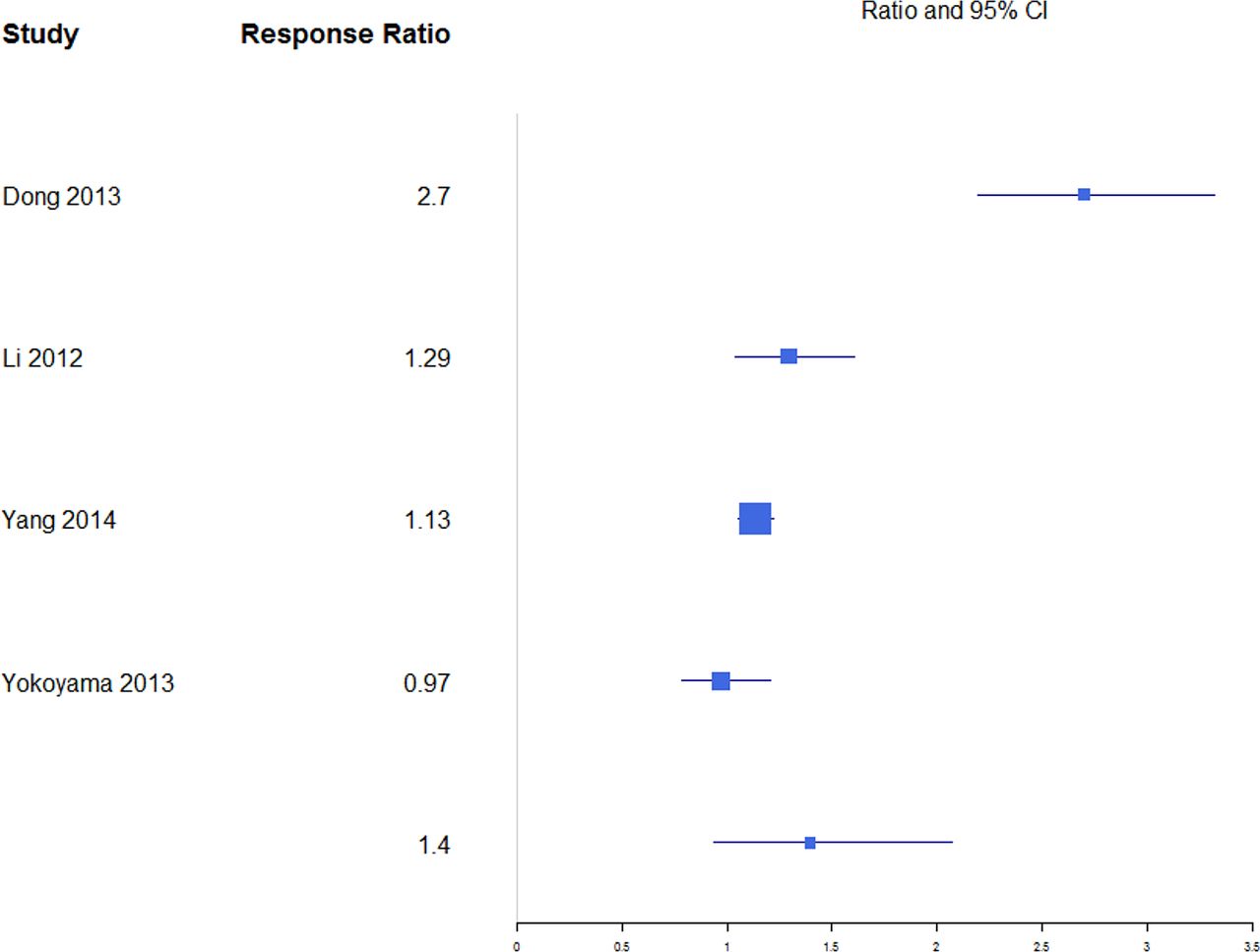
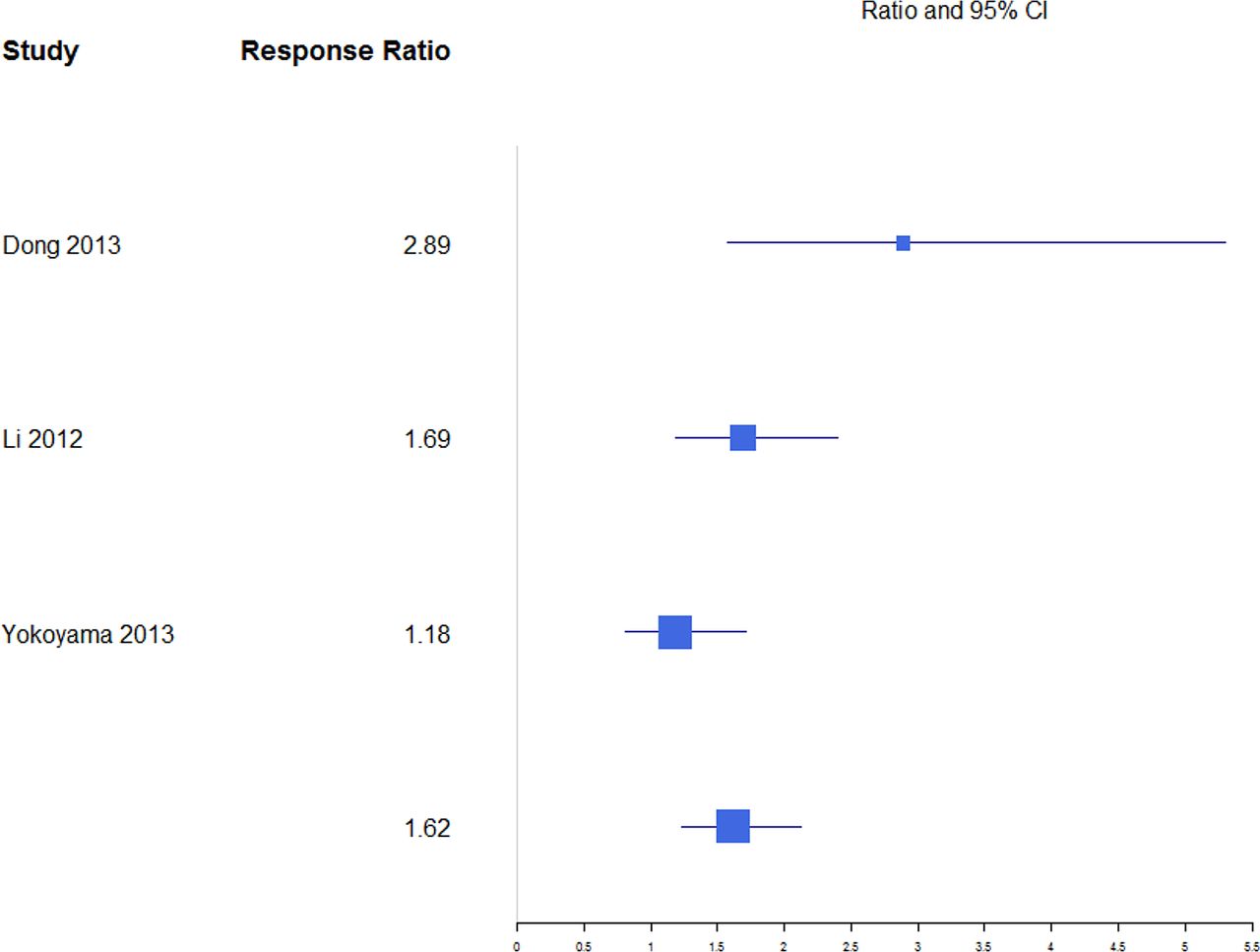
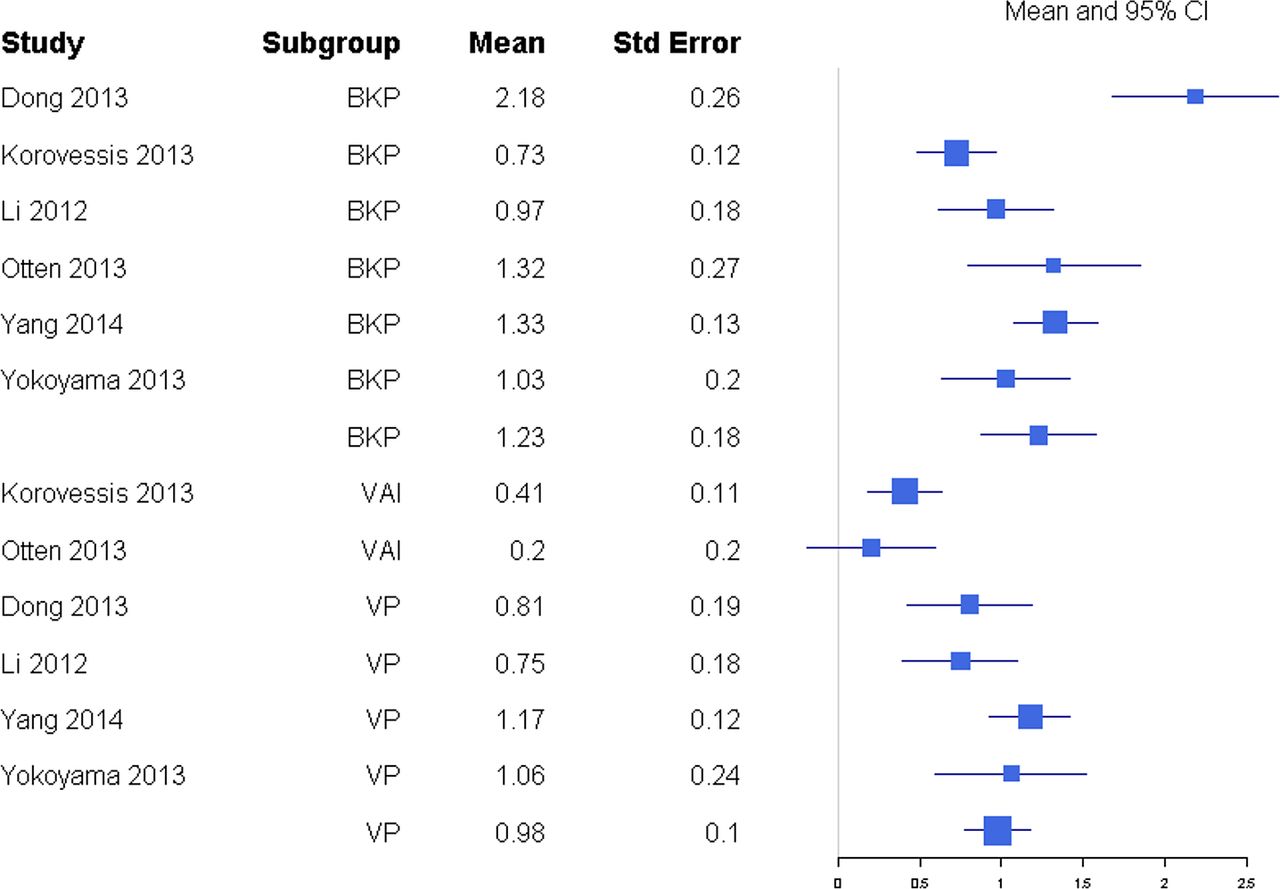
For anterior and posterior vertebral height restoration, BKP showed higher positive change in response compared with VP. Mean estimates for response ratios for anterior and posterior are 1.40 (0.94, 2.07; Figure 11) and 1.62 (1.23, 2.12; Figure 12), respectively, for BKP over VP. Forest plots of standardized mean differences from baseline for vertebral heights are shown in Figures 13 14. Only BKP and VP were compared due to the number of eligible studies.
Response ratios of standardized mean differences for anterior vertebral height comparing balloon kyphoplasty with vertebroplasty treatment.

Response ratios of standardized mean differences for posterior vertebral height comparing balloon kyphoplasty with vetebroplasty treatment.
Standardized mean differences of change from baseline for anterior vertebral height. Abbreviations: BKP, balloon kyphoplasty; VAI, vertebral augmentation with implants; VP, vertebroplasty.
For anterior vertebral height change in response, both treatments showed improvement by increasing restoration. BKP had a mean response change of 1.23 (0.87, 1.58), which was not significantly higher than VP at 0.98 (0.78, 1.17; P = .226). There was substantial heterogeneity in the BKP (I2 = 81) arm but not the VP (I2 = 20) arm.
For midline vertebral height change in response, BKP was 1.12 (0.87, 1.38). There were not enough studies for VP or VAI. There was midheterogeneity in the BKP (I2 = 37) arm.
For posterior vertebral height restoration, BKP (0.54 [0.31, 0.77]) had slightly higher change than VP (0.38 [0.18, 0.58]), but the difference was not significant (P = .293). There was moderate and minimal heterogeneity in the BKP (I2 = 60) and VP (I2 = 0) arms, respectively.
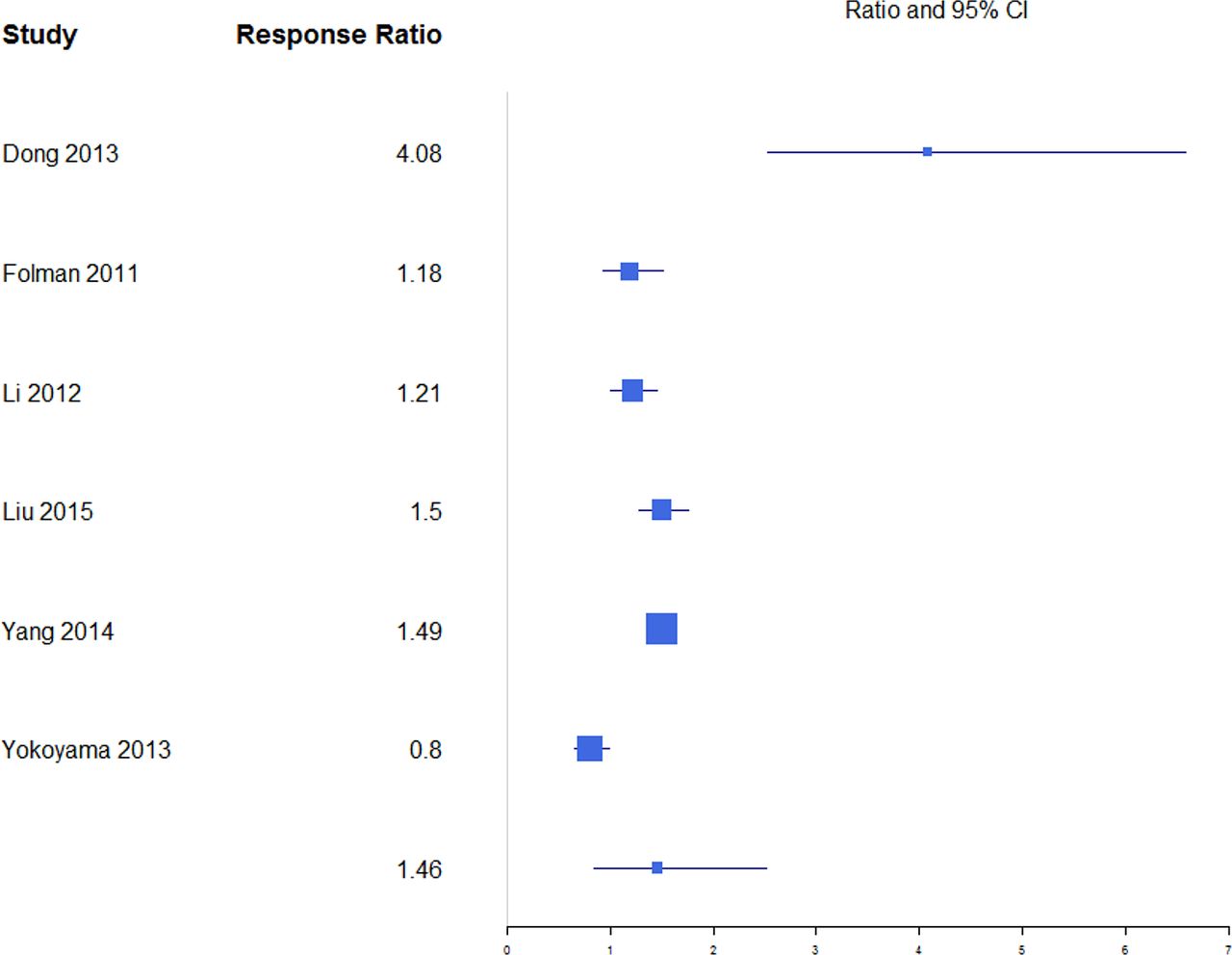
The percentages of patients with subsequent fractures were not significantly different for BKP (32.7%; 95% confidence interval [CI] 8.8%, 56.6%) and VP (28.3%; 95% CI 7.0%, 49.7%; P = .790) or for BKP and NSM (15.9%; 95% CI 5.2%, 26.6%; P = .207; Figure 15). There was also no significant difference between VP and NSM (P = .307). There was substantial heterogeneity in the BKP (I2 = 95), VP (I2 = 96) and NSM (I2 = 81) arms.
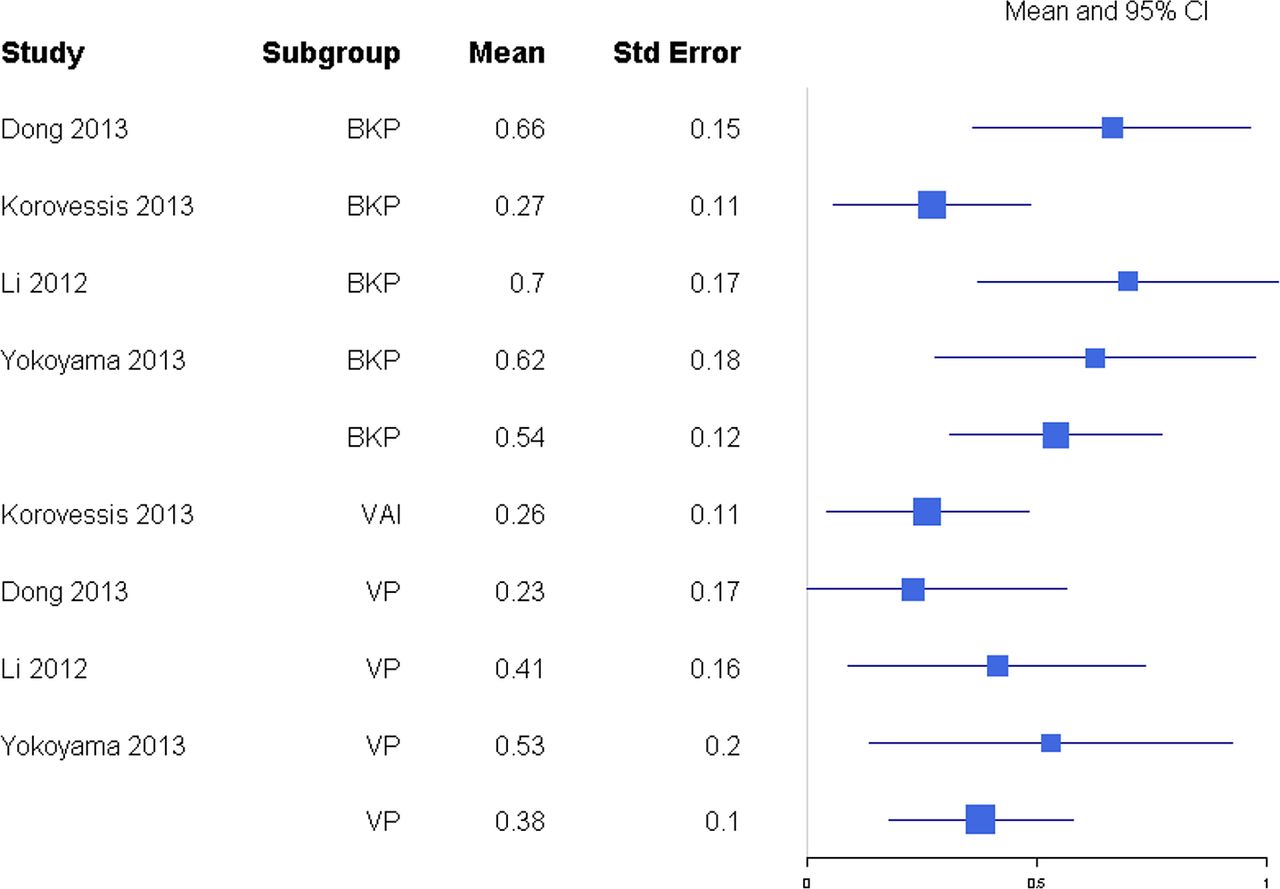
Standardized mean differences of change from baseline for posterior vertebral height. Abbreviations: BKP, balloon kyphoplasty; VAI, vertebral augmentation with implants; VP, vertebroplasty.
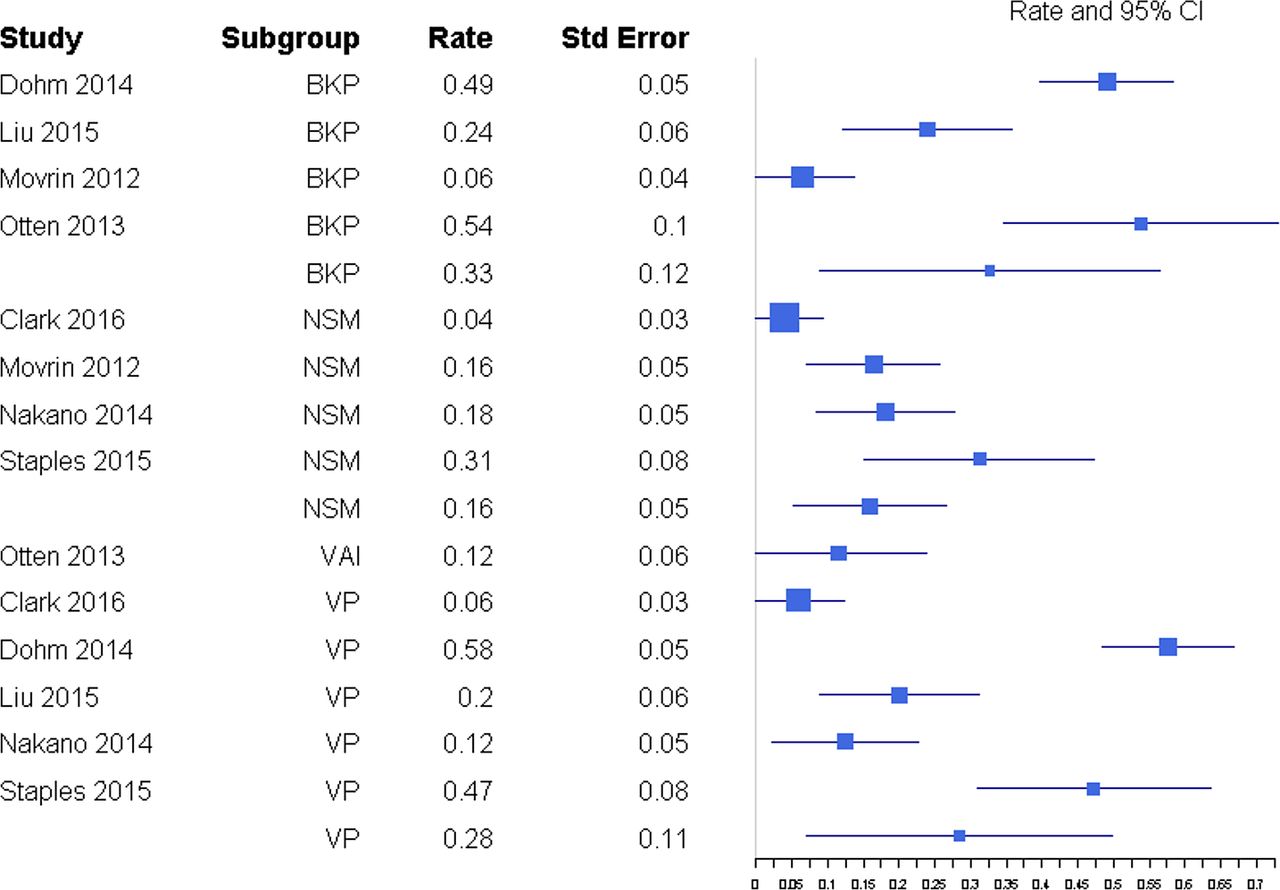
Rate of subsequent fractures. Abbreviations: BKP, balloon kyphoplasty; NSM, nonsurgical management; VAI, vertebral augmentation with implants; VP, vertebroplasty.
DISCUSSION
The drive to produce and collect data in recent years has been enhanced by the controversy initiated by the 2009 sham trials (Buchbinder et al19, Kallmes et al20) published in NEJM. Approximately 250 manuscripts dedicated to vertebral augmentation have been published annually. Much of the output attempts to further define the safety and efficacy of these procedures and investigate differences between the clinical experience with these procedures and the results of the sham trials.
Due to the aforementioned sham trials, there has been a significant decline in the number of vertebral augmentation procedures performed,46–49 and various health technology assessments (HTAs) have used this information to recommend against vertebral augmentation in other countries.
These HTA recommendations are at direct odds with medical societies whose recommendations support vertebral augmentation, including a consensus statement50 from 8 major medical societies that vertebral augmentation remains a proven, medically appropriate therapy for treatment of painful VCFs refractory to nonoperative medical therapy when performed for medical indications outlined in published standards.
An outlier in society recommendations was issued in 2010 by the American Academy of Orthopaedic Surgeons (AAOS).51 This was based on an algorithm using levels of evidence to perform hierarchal qualification of data. At the time the AAOS guidelines were issued, far less data were available, and the existing level of evidence hierarchy placed the Buchbinder et al19 and Kallmes et al20 studies as the highest level of evidence. As a consequence, the AAOS guidelines provided a weak recommendation for kyphoplasty and a strong recommendation against VP.
After the NEJM articles, HTA recommendations, and AAOS guidelines, Papanastassiou et al52 conducted a meta-analysis on the effects of kyphoplasty, VP, and NSM to treat VCFs that reported on 27 Level I and Level II studies. Papanastassiou et al52 concluded that BKP and VP provided better pain relief, resulted in fewer additional VCFs than NSM, and concluded that BKP is favored over VP for QOL improvements and cement extravasation. The authors noted that 2 RCTs in their analysis showed no difference between VP and a sham procedure and pointed to significant data heterogeneity recommending further trials to delineate some confounding variables. Since then, there have been several publications, including double-blind RCTs, other Level I studies on vertebral augmentation, and 2 additional VP versus sham studies, that have added to the literature on vertebral augmenation.
A 2016 sham study trial by Clark et al21 compared VP to sham in patients with acute vertebral compression fractures and concluded that VP significantly reduces pain, improves disability scores, and achieves greater vertebral height restoration. The findings support use of VP over sham surgery in patients with acute VCFs, which differs from the equivocal result of previous sham trials19,20 that concluded no significant difference in pain, function, and QOL between sham patients and patients undergoing VP. A second RCT comparing VP to sham, published in 2016 by Hansen et al,22 concluded that there was a statistically signficant VAS score reduction in the VP group as compared with the sham group during their trial period. An explanation for differences in the conclusions is found in one notable publication since the Papanastassiou et al52 study. Anderson et al53 conducted a meta-analysis in 2013 comparing vertebral augmentation with NSM and analyzed the study quality of the 2009 sham trials19,20 with the levels of evidence of primary research as adopted by the North American Spine Society.53,54 Anderson et al53 found the 2009 sham trials should have been classified as providing Level II evidence instead of Level I, based on inclusion and exclusion criteria and the Kallmes et al20 trial's unacceptably high crossover rate. Both trials were therefore downgraded to Level II evidence based on objective measures of quality for primary research.53
Although the most recent highest-quality literature supports vertebral augmentation over NSM to treat painful VCFs, many HTAs and several national treatment guidelines continue to make outdated, inconsistent recommendations regarding vertebral augmentation. For example, a recent (2015) HTA publication by the Cochrane Collaboration recommended against using VP to treat VCFs in routine clinical practice.55 This recommendation disregarded 11 RCTs and 1 “quasi RCT,” classifying all non–placebo-controlled trials as having high risk of bias, and therefore based the conclusion against VP on only the 2 NEJM sham trials, which were classified as Level I rather than Level II data. This arbitrary classification and selective information culling is one example of how significant discrepancies can arise between HTA reviews and high-quality meta-analyses.
Our present meta-analysis showed differences in outcomes between BKP, VP, and NSM, but fewer than seen in the Papanastassiou et al52 meta-analysis. More pain reduction for both BKP and VP were observed in comparison with NSM, although this was significantly different from BKP to NSM but not statistically significant from VP to NSM. Our analysis also included VAI as a subgroup. We found a significant difference in VAS scores between BKP and VAI, with BKP having more reductions in pain score. BKP had some tendency for slightly better pain reduction than VP, but the difference in this meta-analysis was not statistically significant. This evaluation also showed no difference in disability improvement between BKP and VP and no difference in rates of subsequent fractures. BKP showed significantly better outcomes than VAI in terms of disability improvement (ODI). Patients undergoing BKP were found not to have significantly greater amounts of anterior and posterior vertebral height restoration than VP patients, nor was a difference seen in kyphotic angle correction between VP and BKP groups.
Along with the various outcome measures, a few studies in this meta-analysis examined economic costs of BKP and VP. Folman and Shabat32 concluded that BKP and VP had similar success levels of pain relief, but due to higher costs of BKP, the cost-benefit advantage of VP was clear. However, though an analysis of Medicare data showed no differences in adjusted, cumulative treatment costs for VP and BKP patients in the first 9 months postsurgery, BKP patients were subsequently associated with significantly lower adjusted treatment costs in remaining periods through 2 years postsurgery.56 A survival and cost analysis by Lange et al12 comparing BKP and VP using German claims data showed 4-year mean overall costs were lower for the BKP group than for VP (BKP: €39 014 versus VP: €42 510), due to higher initial BKP costs being offset by pharmacy costs in VP patients. In a multicenter, randomized, controlled cost-effectiveness analysis, Fritzell et al33 determined that it was not possible to demonstrate that BKP was cost effective compared with standard medical treatment in VCF patients. Three other studies (Ström et al,57 Svedbom et al,58 and Klazen et al59) analyzed cost effectiveness using quality adjusted life years and confirmed vertebral augmentation was cost effective compared with NSM.
In a comparison of BKP and VBS, Werner et al15 found no substantial differences in cost, even though costs of vertebral fracture treatment were generally lower for BKP than VBS for treating 1 to 3 vertebral levels.
This meta-analysis yielded insufficient data to determine the QOL differences and optimal intervention time relative to age of the VCF. There were also insufficient data to determine differences in extravasation rates or serious adverse events. We demonstrated comparable findings to those of a recent meta-analysis comparing NSM with VP by Mattie et al.60 When evaluating 11 studies containing 1048 participants, Mattie et al60 reported VP was better than NSM with respect to pain relief up to 1 year after VP. This provides additional information supportive of the efficacy of VP, similar to previous meta-analyses by Anderson et al53 and Papanastassiou et al52 and trends shown in several of the 25 articles included in this meta-analysis. The level of evidence of the meta-analysis of Mattie et al60 was designated as Oxford Level I, which should be taken into account by not only treatment guidelines but also policy recommendations and HTAs. The meta-analysis also focused specifically on percutaneous vertebroplasty as compared with conservative therapy, while only evaluating studies in which the primary outcome was pain relief. No requirements were made of retrospective or prospective studies, minimum number of patients, or site of the procedure.
CONCLUSION
This meta-analysis revealed a large number of high-quality articles (25 Level I and Level II studies), including 17 randomized trials since February 2011. We were unable to include findings from a recently completed prospective, multicenter evaluation of the safety and efficacy of BKP in Medicare patients (EVOLVE trial61), as it had not yet been published in a peer-reviewed journal. The results of this EVOLVE trial included statistically significant improvements in patients' pain, function, quality of life, self-care indices, and vertebral deformity correction. Our current meta-analysis showed statistically superior pain reduction for BKP in comparison with NSM, but pain reduction was not statistically significant for VP in comparison with NSM. There was significantly improved pain reduction and disability improvement for BKP over VAI. BKP tended to show greater anterior and posterior vertebral height change than VP, though this was not statistically significant. The overall number of statistically significant categories was less than in a previous 2011 meta-analysis. It is noteworthy that the analysis includes a VP versus sham trial that offers Level I evidence of statistically significant differences in pain reduction and disability improvements in a study with higher statistical power than previous sham trials, which showed no difference between VP and sham. Also notable is the refinement of evidence, including reclassification of 2 previous sham trials to Level II evidence and conclusions of best-quality literature that serve to further define the safety and efficacy of vertebral augmentation. Despite the preponderance of high-quality data, all endpoints demonstrated substantial heterogeneity in the treatment arms even between randomized trials.
Footnotes
Disclosures and COI: This meta-analysis was conducted with funding from the International Society for the Advancement of Spine Surgery (ISASS); Benvenue Medical, Inc; DePuy Synthes Spine, a division of DePuy Orthopaedics, Inc; DFINE Inc; Globus Medical, Inc; Medtronic Sofamor Danek USA, Inc; and Stryker. Douglas Beall reports the following disclosures unrelated to the preparation of this manuscript: compensation, grants, and personal fees from Medtronic related to consultancy, research and teaching; grants from Benvenue, Alphatech Spine, Medical Metrics, Liventa, Vexim, and Mesoblast; consultancy fees from DEFINE and Osseon; other from Lilly, Smith & Nephew, Biomet, Vertiflex, Synthes, and Integral Spine Solutions. Morgan Lorio reports the following disclosures unrelated to the preparation of this manuscript: royalties from Choice Spine Thunderbolt, stock ownership in Orthogenerex, stock options with OrthoKinematics, intellectual property with Transformer Spine, investigator for Acadia Facet IDE Trial. B. Min Yun and Maria J. Runa are employees of Exponent, a scientific and engineering consulting firm. They have no other disclosures. Kevin Ong reports the following disclosures: employee and shareholder of Exponent, a scientific and engineering consulting firm. Exponent has been paid fees by entities in the biomedical arena for consulting services, including Zimmer Biomet, Stryker Orthopaedics, Joerns Healthcare, Ossur, DJO, Ethicon, Ferring Pharmaceuticals, Pacira Pharmaceuticals, Paradigm Spine, and Medtronic. Christopher B. Warner reports no disclosures.
- ©International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Outcomes and Safety Comparison of Vertebroplasty, Balloon Kyphoplasty, and Vertebral Implant for Treatment of Vertebral Compression Fractures
- Cost-effectiveness and willing-to-pay thresholds for vertebral augmentation of osteoporotic vertebral fractures, what are they based on: a systematic review
- Management of Osteoporosis and Spinal Fractures: Contemporary Guidelines and Evolving Paradigms
- Response to: The evidentiary basis of vertebral augmentation: a 2019 update
- ISASS Policy 2018--Vertebral Augmentation: Coverage Indications, Limitations, and/or Medical Necessity