


ABSTRACT
Background: Treatment options for aortic-iliac pathology may include endovascular repair and open surgical repair. Treatment options for degenerative disc disease (DDD) are varied but commonly include anterior reconstruction. When both the aortic-iliac and spinal pathologies are significant and surgical intervention is indicated for each pathology, the opportunity exists for concurrent treatment of both the aortic-iliac pathology and DDD in the same operation. The purpose of this case series was to document the safety and feasibility of a surgical strategy whereby a combined elective reconstructive procedure was performed for aortic and anterior lumbar spinal pathologies.
Methods: The case histories of 5 patients who were treated for both spinal and vascular pathology are presented. Surgical outcome measures included operative time, blood loss, length of stay, and complications. Spine-specific outcome measures included Oswestry Disability Index, Roland Morris Disability Questionnaire, and visual analogue scores (back and leg).
Results: The spinal reconstructions performed included 1 L4-5 total disc replacement (TDR), 1 L4-5, L5-S1 anterior lumbar interbody fusion (ALIF), 1 L5-S1 ALIF, and 2 hybrid procedures (L4-5 TDR with L5-S1 ALIF). Vascular reconstructions included 4 aorto–bi-iliac bypass grafts and 1 aortic tube graft. The average operative time was 365 minutes (ranging between 330 and 510 minutes), the average blood loss was 1699 mL (range between 1160 and 2960 mL), and the average length of hospital stay was 14 days (range from 8 to 22 days). There were no in-hospital complications, and all patients experienced significant improvement in both back and leg pain. One patient developed kinking of the iliac limbs of the vascular graft 1 year postoperatively, which was managed with endovascular stenting of the graft.
Conclusions: Aortic-iliac pathology and DDD are significant pathologies often treated in isolation. This study illustrates that, despite its complexity, highly trained individuals in a specialized setting can perform combined surgery to achieve a satisfactory outcome for the patient.
Level of Evidence: Level IV evidence.
- abdominal aortic aneurysm
- total disc arthroplasty
- anterior lumbar interbody fusion
- aortic iliac occlusive disease
- multidisciplinary approach
INTRODUCTION
The incidence of symptomatic degenerative disc disease (DDD) increases with age, with the lifetime prevalence estimated at 60% to 90% (see Figure 1).1–3 Disc degeneration is the initial step in the cascade of degenerative spinal changes, followed by osteophyte development, disc narrowing, facet decoupling, arthritis, and spinal stenosis.4 The benefits of spinal reconstruction for patients with symptomatic DDD and radiculopathy are well established in the literature.5,6 Anterior reconstructions, in particular, have been shown to reduce the risk of neurological complications5 and morbidity7 postoperatively in comparison with other approaches. Patients with chronic low back pain (CLBP) due to DDD who have failed to respond to conservative management can benefit from surgical intervention, with both fusion and total disc replacement (TDR) being accepted treatment options.8 Surgical intervention has been shown to have positive effects on both back and leg pain as well as self-rated quality of life.9–12

Sagittal view of both degenerative disc disease and abdominal aortic aneurysm pathologies.
The prevalence of both aortic-iliac occlusive disease (AIOD) and abdominal aortic aneurysm (AAA) also increases with age, with the incidence of AAA estimated at 4% to 7% of men and 1% to 2% of women older than 65 (see Figure 2).13,14 Modern surgical techniques allow for treatment of aortic disease with either open aortic surgery or through endovascular aneurysm repair.15 Lower mortality and morbidity rates are present for endovascular aneurysm repair than open aortic surgery; however, late complications, higher reintervention rates, and decreased late survival16 may offset this advantage.17 While aortic and spinal conditions often present separately, with regard to patient symptoms, they can often coexist. Further, arterial occlusion can significantly decrease nutrition of the disc and lead to progressive disc disease.18 Kurunlahti et al19 revealed that this association between atheromatous lesions in the abdominal aorta and DDD is significantly higher in patients with low back pain.

Computed tomography scan revealing aortic-iliac occlusive disease and abdominal aortic aneurysm.
A patient presenting with severe chronic back and leg pain may have a significant vascular pathology that weighs equally in consideration for surgical review and possible treatment (see Figure 1). If it is considered to be at risk of rupture, there is clear consensus that the vascular pathology needs surgical repair.15,20 The issue of how and when to treat vascular and spinal pathologies is complex and yet to be resolved. The treatment of the AIOD first and separately would preclude an anterior reconstruction and its associated benefits. A 2-stage procedure means 2 anaesthetics for the patient, 2 surgical procedures, a longer overall stay in hospital, and a delay in resolution of their symptoms. Additionally, it doubles the preoperative stress response and postoperative pain as well as leading to higher costs of treatment.21
Considering that operating rooms can consume up to and in excess of 40% of a hospital's annual budget,22 optimization of resources and providing quality care are paramount. For example, bilateral total knee and hip arthroplasty, in which a patient has both joints replaced under a single anaesthetic, is 36% and 25% less costly than 2 unilateral arthroplasties, respectively.21 Regarding the cost of open compared with endovascular repair of abdominal aortic aneurysms, the overall costs have been found to be higher with endovascular techniques.23 Extrapolating, a combined strategy employing open vascular techniques has the potential to reduce overall health care costs not only by avoiding staged surgery but also by avoiding the need to employ endovascular techniques and their associated higher rate of late complications.
A systematic search of the literature revealed no published reports of surgery to concurrently treat AIOD and DDD in a single operative event. While a case series is considered to be a low level of evidence, the absence of any literature provides rationale for one. Therefore, the purpose of this case series was to document the feasibility and safety of a combined reconstructive procedure performed for aortic and lumbar spine pathologies and the outcome of 5 patients who have undergone this procedure.
PATIENTS AND METHODS
A prospective, uncontrolled clinical case series in a single institution was conducted. Between September 2012 and March 2016, 2756 new cases presented at a specialist spinal clinic. A total of 5 cases (incidence proportion of 0.18%) presented with dual pathologies of DDD with radiculopathy and significant AIOD, subsequently undergoing a combined surgical technique.
Two experienced surgical teams were involved and detailed preparation was undertaken in advance of the procedure. In theater, there was utilization of a radiolucent modular operating table, separate vascular and spinal nursing teams and surgical assistants, a neuromontitoring team, blood reperfusion processes backed by cross-matched blood, and experienced radiographers, as well as management of the anesthetic by a vascular anesthetist.
Patient demographics, individual surgical information (including operative time, blood loss, and transfusion requirements) and postoperative information (including length of stay and complications) have been reported in all cases and are presented in Table 1. Spine-specific outcome measures, including Roland Morris Disability Questionnaire, Oswestry Disability Index, and visual analogue score for both back and leg pain, were assessed preoperatively and at 3, 6, and 12 months postoperatively and can be found in Table 2.
Demographic, preoperative, and postoperative information for cases 1 to 5.
Outcome measures for spinal surgery with 12-month follow-up.
ELIGIBILITY OF PATIENTS FOR CONCURRENT PROCEDURE
Decision making regarding elective repair of both AAA and DDD requires careful assessment of multiple criteria. The indications for spinal surgery were 1- or 2-level degenerative disc disease and/or spondylolisthesis with associated radiculopathies. All patients presented with debilitating symptoms of at least 6 months' duration that had not improved with appropriate nonoperative treatments. This criterion has previously been applied for hybrid procedures in which both TDR and ALIF were utilized for the treatment of DDD.12
The criteria applied to warrant AAA repair commonly involves an aneurysm of 5.5 cm or greater.17 While this threshold is based off the best available evidence, it is not possible to apply a single threshold diameter which can be generalized to all patients; hence the need of an individualized approach which considers the factors of rupture risk, operative mortality, and life expectancy.17
With relevance to the current case study, all 5 cases are substantially younger (average age of 61.6 years) than the typical vascular patient,24 in which maximum AAA incidence rates have been shown between 75 and 79 years.25 Therefore, all cases had a significant potential for an extended life beyond presentation and longevity of the vascular intervention was of considerable importance. Given the subset of younger patients and the higher life expectancy, repair was warranted within the patients who presented with an AAA of less than 5.5 cm in diameter.
The spinal procedures undertaken in these cases utilized open surgery with either a retroperitoneal or transperitoneal approach and consequently would involve displacement, distortion, compression, and stretching of the aorta to allow access. Without prophylactic repair, the AAA sac would limit access to the spine, and, thus, the risk of rupture during spinal surgery necessitates addressing the vascular lesion at the time of spinal reconstruction. Therefore, without treatment of the vascular lesion, the appropriate anterior spinal procedure would not have been possible.
The standard anticoagulation protocol followed in this case series was 5000 units of heparin administrated before the cross-clamping of the aorta. If the clamp time exceeded 90 minutes, an additional 1000 units was given. No reversal agents are administered after closure, unless ooze or a leakage is detected. Postoperative physical and chemical prophylaxis consisted of ted stockings, gentle physical therapy, and 40 mg of clexane subcutaneously twice daily. This was continued for 4 weeks.
CASE 1
A 61-year-old female presented for assessment of CLBP and bilateral sciatica with symptoms suggestive of both neurogenic and vascular claudication. Despite appropriate nonoperative treatment, her symptoms had deteriorated to the extent that she required walking sticks to ambulate. She also reported a smoking history. Preoperative outcome measures pertaining to case 1 are reported in Table 1.
Clinical examination revealed flattening of her lumbar lordosis and a restricted range of motion in the lumbar spine. Neurological examination of the lower limbs was normal. Pedal pulses were absent. Electromyography (EMG) examination confirmed bilateral L5 radiculopathies. Spinal imaging (magnetic resonance imaging [MRI], computed tomography [CT], and discogram) showed advanced DDD in the lower lumbar spine, with L3-4 autofused, disc degeneration with an annular tear at L4-5, and disc degeneration with loss of disc height and bilateral neuroforaminal stenosis at L5-S1. Significant calcification throughout the aorta and iliac arteries was also noted. She was referred for vascular assessment, and a CT angiogram was performed. This showed severe AIOD with complete occlusion of the distal aorta and both iliac arteries. After consultation between spine and vascular services and shared decision making with the patient, it was decided to proceed with a combined lumbar hybrid procedure (L4-5 TDR and L5-S1 ALIF) and aorto–bi-iliac bypass.
Surgery was performed through a standard midline laparotomy, using a transperitoneal approach. The spinal reconstruction was performed first. The L4-5 level was exposed and reconstructed with TDR, after ligation of the iliolumbar vein and mobilization of the aorta and vena cava to the right. The L5-S1 level was approached and reconstructed with ALIF between the iliac vessels, after ligation of the median sacral vessels. On completion of spinal reconstruction, an aorto–bi-iliac bypass was performed using a 14-mm bifurcation graft. Total operative time and blood loss were, respectively, 8 hours, 26 minutes and 2960 mL (requiring 2 units of postoperative transfusion).
The patient was monitored in the ICU overnight and then transferred to the ward. After increasing her mobility on the ward, the patient was discharged home (total of 16 days inpatient stay). There were no postoperative complications, and good perfusion was restored to both lower limbs. The 12-month follow-up of outcomes postsurgery for case 1 can be seen in Table 2, with improvements made in all outcome measures pertaining to the spinal surgery.
CASE 2
A 60-year-old male presented for assessment of CLBP and right-sided sciatica that had failed conservative management. He had undergone a L5-S1 laminectomy 20 years earlier. Preoperative outcome measures pertaining to case 2 are reported in Table 1.
A CT scan showed a degenerate disc with an extrusion compressing the right L5 nerve root at L4-5, an autofused L5-S1 level, and a 6-cm infrarenal AAA. Clinical examination revealed a Trendelenburg gait and weakness of ankle dorsiflexion on the right side. EMG examination showed bilateral L5 radiculopathies as well as a left L4 radiculopathy. The patient was referred for a vascular assessment, and the AAA was deemed suitable for either open or endovascular repair. After consultation with spine and vascular services and shared decision making with the patient, it was decided to proceed with a combined open AAA repair and L4-5 TDR, with removal of the disc extrusion.
Surgery was performed through a standard midline laparotomy. The aorta was clamped just below the renal arteries, then opened, and the proximal end of the graft was attached. This was folded out of the way, and the aorta was then transected above the bifurcation with control of the iliac vessels. The L4-5 disc was then exposed. After discectomy and removal of the extruded fragment, a TDR was inserted. The remnants of the aortic wall were placed back over the top of the TDR, and then the distal anastomosis was completed. Total operative time and blood loss were, respectively, 5 hours, 30 minutes and 1375 mL. No postoperative transfusion was required.
The patient had an uncomplicated postoperative course, was mobilized on the ward, and was discharged home (total of 12 days inpatient stay). The 12-month follow-up of outcomes postsurgery for case 2 can be seen in Table 2, with improvements made in all outcome measures pertaining to the spinal surgery, and no postoperative complications were reported at any time during data collection.
CASE 3
A 66-year-old male presented for assessment of CLBP and bilateral sciatica that had failed conservative management. Preoperative outcome measures pertaining to case 3 are reported in Table 1.
Examination revealed loss of lumbar lordosis and wasting in the buttocks bilaterally. He was tender over the lower lumbar spine, and pedal pulses were reduced. EMG examination showed bilateral L5 and right S1 radiculopathies. Imaging studies showed advanced DDD at L4-5 and L5-S1, with neuroforaminal stenosis at both levels, and a focal AAA was noted at L4-5.
The patient was referred for a vascular opinion, with CT angiogram confirming a 4-cm AAA with an associated 23-mm right common iliac aneurysm. After consultation with spine and vascular services and shared decision making with the patient, it was decided to proceed with a combined aorto-iliac bypass and L4-5, L5-S1 ALIF.
Surgery was performed through a standard midline laparotomy. At the time of surgery, the aortic disease had progressed almost up to the renal arteries, and the left common iliac was seen to be elongated and tortuous. The aorta was clamped just below the renal arteries. A 20 mm × 10 mm bifurcated graft was then attached end to end proximally and end to end on the right. On the left the graft was also attached end to end but initially left long to allow for the spinal reconstruction. The L5-S1 ALIF was then performed between the iliac vessels, and then the L4-5 ALIF was performed, after mobilizing the vena cava and left common iliac vein to the right. At the end of the spinal procedure, the left iliac graft was shortened and reattached end to end. Total operative time and blood loss were, respectively, 5 hours, 29 minutes and 1160 mL. No postoperative transfusion was required.
The patient had an uncomplicated early postoperative course, was mobilized on the ward, and was discharged home (total of 8 days inpatient stay). There was development of right sacroiliac joint pain at 12 months postoperatively, which responded well to an intra-articular steroid injection. The 12-month follow-up of outcomes postsurgery for case 3 can be seen in Table 2, with improvements made in all outcome measures pertaining to the spinal surgery.
CASE 4
A 48-year-old man presented for assessment of CLBP and bilateral leg pain that had failed conservative management. Preoperative outcome measures pertaining to case 4 are reported in Table 1.
Examination revealed loss of lumbar lordosis, significant restriction in range of motion in the low back, and mild weakness of ankle dorsiflexion bilaterally. An MRI of the lumbar spine prior to assessment by the spine service had shown an isthmic spondylolisthesis of L5 on S1, with a degenerative disc above at L4-5. The MRI also revealed a 7-cm AAA, with an associated 3-cm left common iliac aneurysm. EMG confirmed bilateral L5 radiculopathies. The patient had a vascular review prior to spinal review and, given the size of the aneurysm, surgical repair was advised. After consultation with spine and vascular services and shared decision making with the patient, it was decided to proceed with L4-5 TDR and L5-S1 ALIF at the same time as the aorto-iliac bypass.
The surgery was performed through a midline laparotomy. The aorta was clamped just below the renal arteries and the proximal end of a bifurcation graft attached end to end. The right iliac graft was then attached. The left-sided repair was performed after the spinal reconstruction. The L5-S1 disc was exposed between the iliac vessels. The disc space was released and discectomy performed. Reduction of the spondylolisthesis was achieved and ALIF performed. The L4-5 disc was then exposed and discectomy performed, followed by insertion of a TDR. At the end of the spinal reconstruction, occlusion of the right iliac graft limb was noted and required thrombectomy and revision of the anastomosis. The left iliac anastomosis was then completed and the abdomen closed. Total operative time and blood loss were, respectively, 7 hours, 10 minutes and 2000 mL (mostly due to flushing of the blood vessels and graft limbs). No transfusion was required postoperatively.
The patient was monitored in the ICU before transferring to the ward to mobilize. He had an uncomplicated early postoperative course and was discharged home (total of 10 days inpatient stay). At 12 months postoperatively the patient developed vascular claudication in both legs, and a CT angiogram showed kinking of the iliac graft limbs due to extension and expansion of the aortic limb of the graft. The patient was taken to the catheterization laboratory, where endovascular stenting of both iliac grafts was performed, consequently restoring normal blood flow to the lower limbs. The 12-month follow-up of outcomes postsurgery for case 4 can be seen in Table 2, with improvements made in all outcome measures pertaining to the spinal surgery.
CASE 5
A 73-year-old male presented with CLBP as well as left leg pain with associated weakness that had failed conservative management. Preoperative outcome measures pertaining to case 5 are reported in Table 1.
Examination revealed loss of lumbar lordosis and a painful step at L5-S1. Weakness was present in dorsiflexion in both legs, with the left weaker than the right. Radiology revealed a grade 2 spondylolisthesis of L5-S1. MRI and CT scan revealed significant neuroforaminal stenosis. EMG revealed bilateral L5 and S1 radiculopathies. The radiology also revealed a small AAA and a vascular opinion was arranged together with CT-angiography. A saccular AAA measuring 40 mm × 35 mm was noted together with extensive calcific atherosclerosis. The calcification, which is normally in the media, remained in the major saccular enlargement, suggesting a thin layer of adventitia and thus raising the possibility of dissection and rupture. After consultation with spine and vascular services and shared decision making with the patient, it was decided to proceed with L5-S1 ALIF and an AAA repair.
A standard transperitoneal approach was performed. An aorto-bifemoral technique was decided upon, with the proximal connection being performed first. The AAA was found to have a friable adventitia only of 3 mm thickness. The vessels distally were prepared, which allowed exposure to L5-S1 for an ALIF. Following this, the femoral anastomosis was performed. Total operative time and blood loss were, respectively, 3 hours, 50 minutes and 1800 mL. There was no postoperative transfusion required.
The patient had an uncomplicated surgery and was then transferred to ICU for 2 days, then to the spinal ward (10 days) and rehabilitation ward (10 days; total of 22 days inpatient stay). The 12-month follow-up of outcomes postsurgery for case 5 can be seen in Table 2, with improvements made in all outcome measures pertaining to the spinal surgery, and no postoperative complications were reported at any time during data collection.
DISCUSSION
Given the overlap of risk factors for both aortic disease and DDD, it is not surprising to discover that patients present to primary care with both pathologies on a regular basis. In many cases, one or both conditions are managed with observation. There are occasions, however, in which surgical intervention is indicated for both conditions due to the risk of spontaneous bleeding, significant pain levels, neurological decline, and negative effects on quality of life. Our experience is that successful use of this combined technique requires substantial preoperative discussion, particularly around informed consent, and intraoperative coordination.
The aim of this case series was to document the feasibility and safety of a combined reconstructive procedure performed for aortic and lumbar spine pathologies. A systematic search of the literature revealed no published research whereby concurrent aortic and lumbar pathologies were treated in the same operation. Therefore, documenting this case series provides insight into the type of patients who can undergo such a procedure and the associated postoperative outcomes.
The results of this study revealed substantial improvements in all outcome measures (Roland Morris Disability Questionnaire, Oswestry Disability Index, visual analogue score) for both conditions that were maintained for a 12-month period postoperatively with minimal complications. Regarding transfusion, case 1 was the only patient that required a postoperative transfusion (2 units), with total intraoperative blood loss among all patients between 1160 and 2960 mL. The mid- to long-term survival benefit to these patients from prophylactic treatment of the AIOD in this setting cannot be evaluated but one would expect it to be favorable and appears to be consistent with historical studies.23
Two out of the five cases (case 3 and 4) developed a complication 12 months postoperation; case 3 had right sacroiliac joint pain which was treated with an intra-articular steroid injection, and case 4 developed bilateral vascular claudication and underwent an endovascular stenting of both iliac grafts. This case series revealed an average ICU stay of 2.8 days and ward stay of 8.8 days. The operative times varied from 220 to 506 minutes (average 365 minutes). These time frames appear to be reasonable considering the patients were recovering from 1 combined procedure which treated 2 significant pathologies.
Previous articles have highlighted the incidence of atypical back pain and subsequent vertebral lysis and pain due to an AAA26 and the indication of AAA repair due to the proximity of a large osteophyte in the lumbar spine27; however, this is the first instance of a combined technique. In one of these studies, only the AAA was repaired, with the large osteophyte not requiring treatment, and in the other the vertebral bodies were stabilized with pedicle screws, while the AAA was left due to healthy renal arteries and distal flow from collaterals. While the left retroperitoneal approach is often preferred for AAA repair due to its ability to expose the entire infradiaphragmatic aorta with access to the suprarenal aorta,28 the anterior approach was required for the spinal surgery in these instances. This approach was utilized to ensure the task was safely performed and extensile as required. It is commonly used for larger AAA repairs28 and may allow a larger working space and natural orientation to anatomical landmarks.29
For this particular combination of surgical procedures (vascular and spinal), a multidisciplinary approach is considered crucial in planning for success in surgical outcomes.30 Consultation across a number of specialties and close study of preoperative vascular imaging is required to address suitability, priority, the effect of comorbidities, and the development of a surgical plan. It is proposed that this type of approach has the potential to improve efficiency and outcomes while reducing adverse events and overall costs, as well as leading to high levels of patient satisfaction.30 Substantial improvements in all outcome measures and acceptable complication levels confirm the feasibility and safety of this combined procedure in a subset of patients that would otherwise face a compromise in their treatment options.
CONCLUSION
While AIOD and DDD commonly coexist, simultaneous treatment of vascular and lumbar spine pathologies is indicated in rare circumstances. This case series shows that, despite it being a complex treatment strategy, it is feasible and can produce significant benefits concerning both pathologies without an excessive complication profile for patients. This procedure brings together unique clinical circumstances and highly trained individuals in a specialized setting to achieve a desirable outcome for the patient.
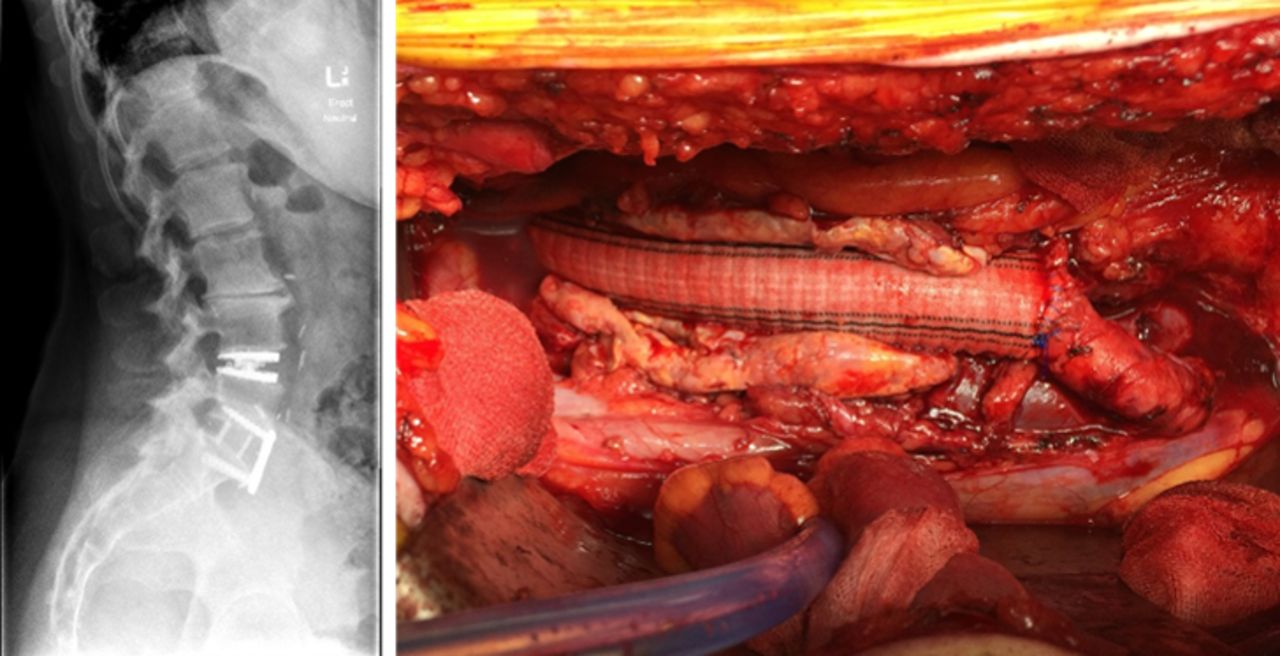
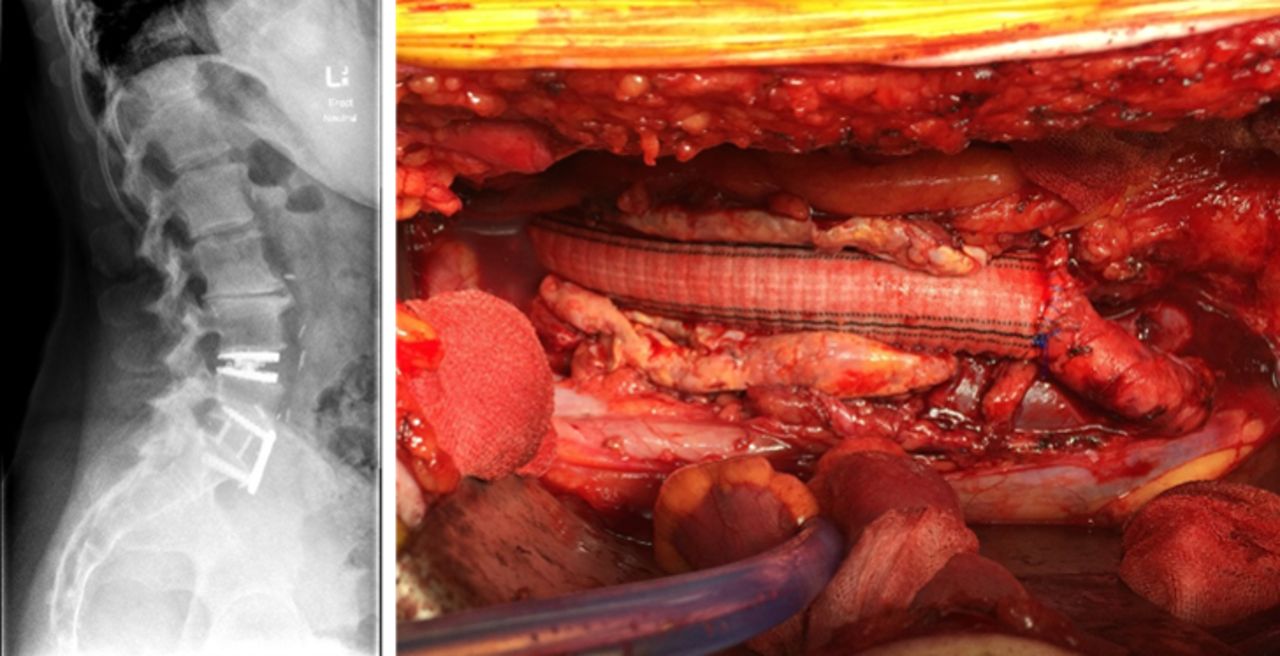
Surgical reconstruction involving a total disc replacement, anterior lumbar interbody fusion, and abdominal aortic aneurysm open repair.
- ©International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.