


ABSTRACT
A 61-year-old woman with no past medical history presented with low back pain and radicular pain in the right lower extremity. Magnetic resonance imaging of the lumbar spine showed a heterogeneous intensity mass in the lateral recess of the spinal canal at the L4-5 disk level. Postoperatively, her radicular pain resolved within a few days with excellent low back pain relief. Ligamentum flavum hematoma is a rare differential diagnosis for cystic lesions in the lumbar spine that can be removed simply by surgery with excellent relief of symptoms and improvement in strength of the right lower extremity and increased sensitivity.
INTRODUCTION
Ligamentum flavum hematoma (LFH) is one of the rare causes of radiculopathy and low back pain. Actually, the manifestation of symptoms is similar to that caused by disk herniation and occurs mostly in the lumbar and lower thoracic spine.1 The exact mechanism of LFH is not clear, but surgical removal of the hematoma provides excellent results.2,3 Most of the cases that have been reported are male.4 This study report is a rare case of LFH presenting with radiculopathy of the right leg and low back pain that underwent total laminectomy and removal of hematoma at the L4-5 disk level.
CASE REPORT
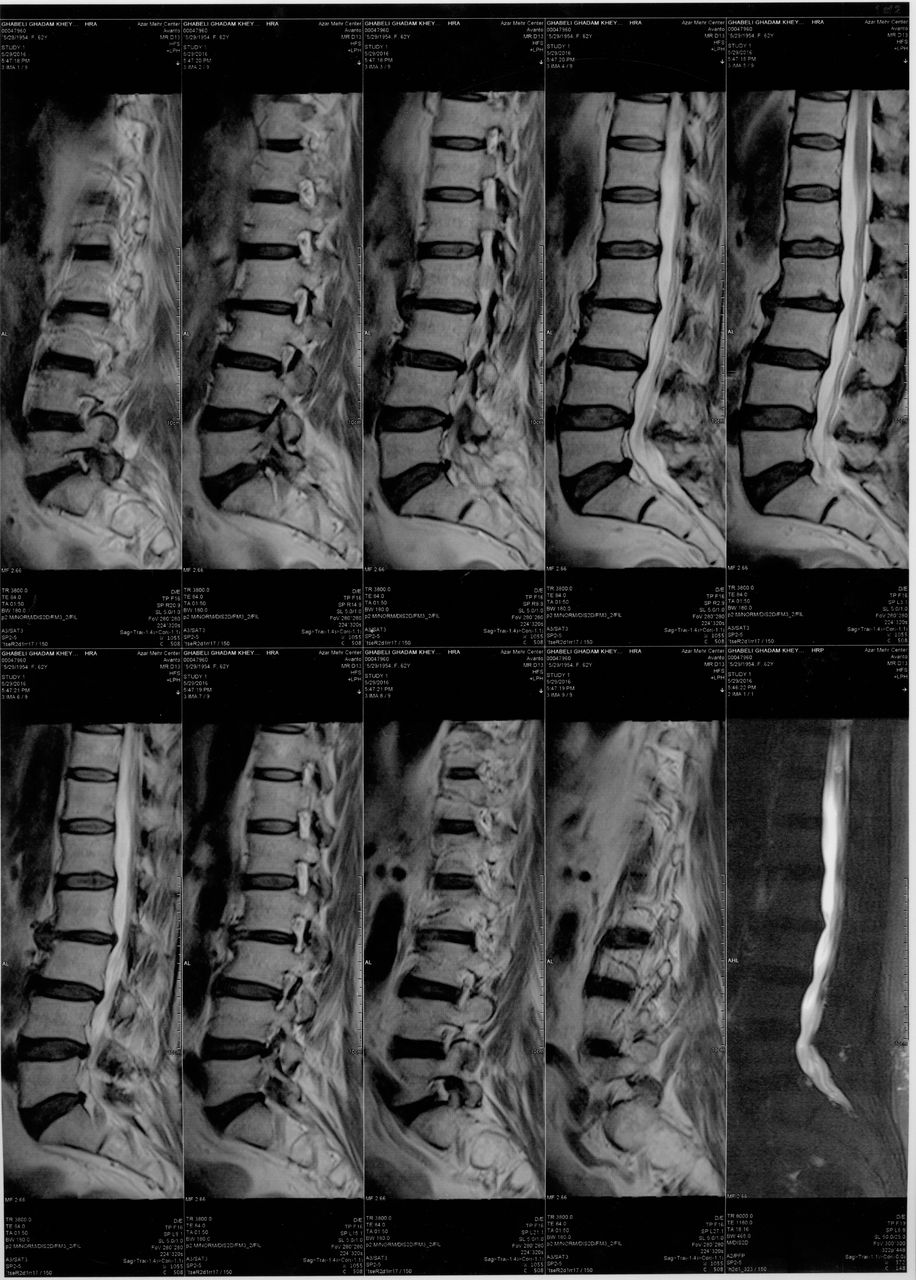
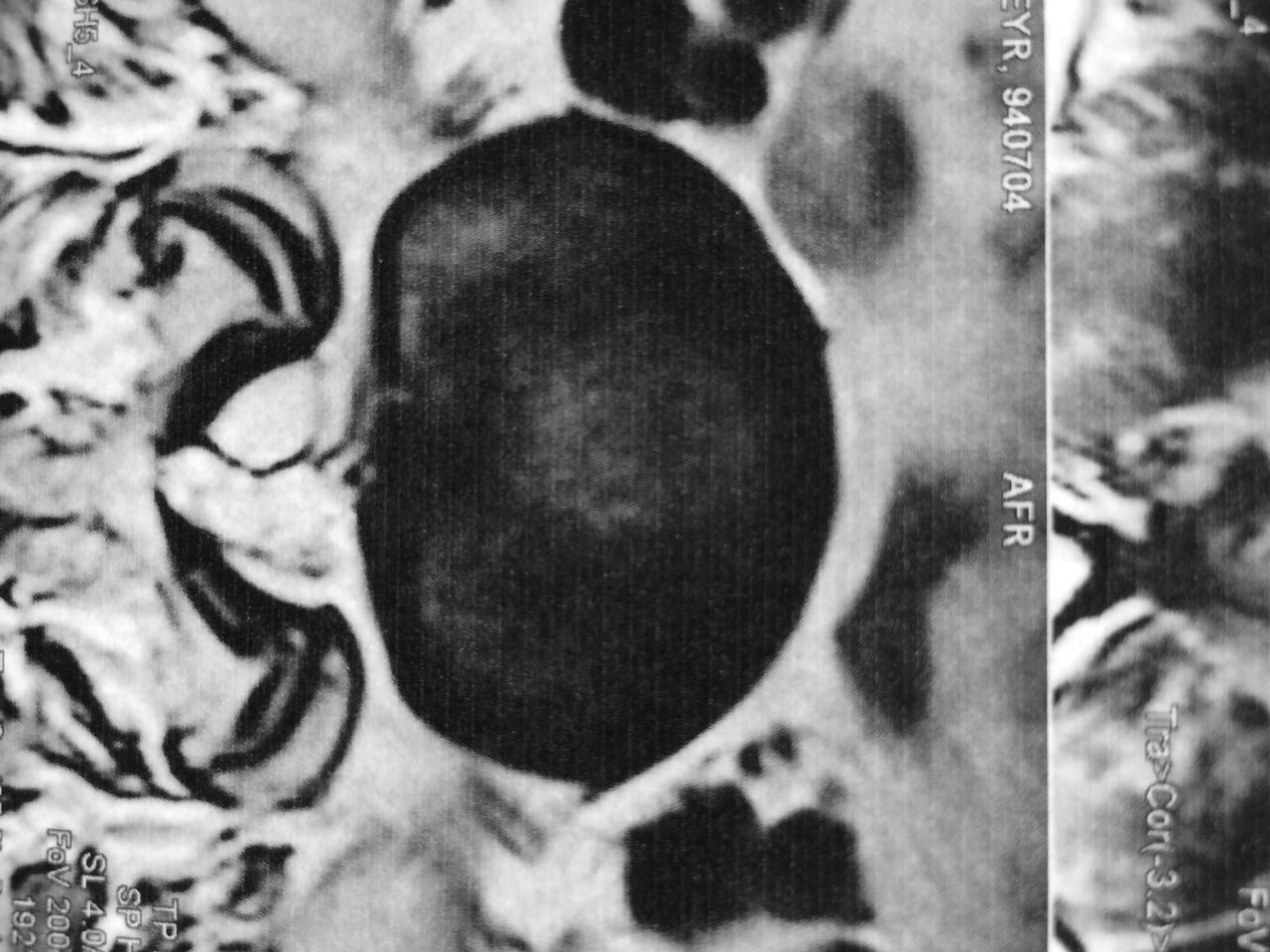
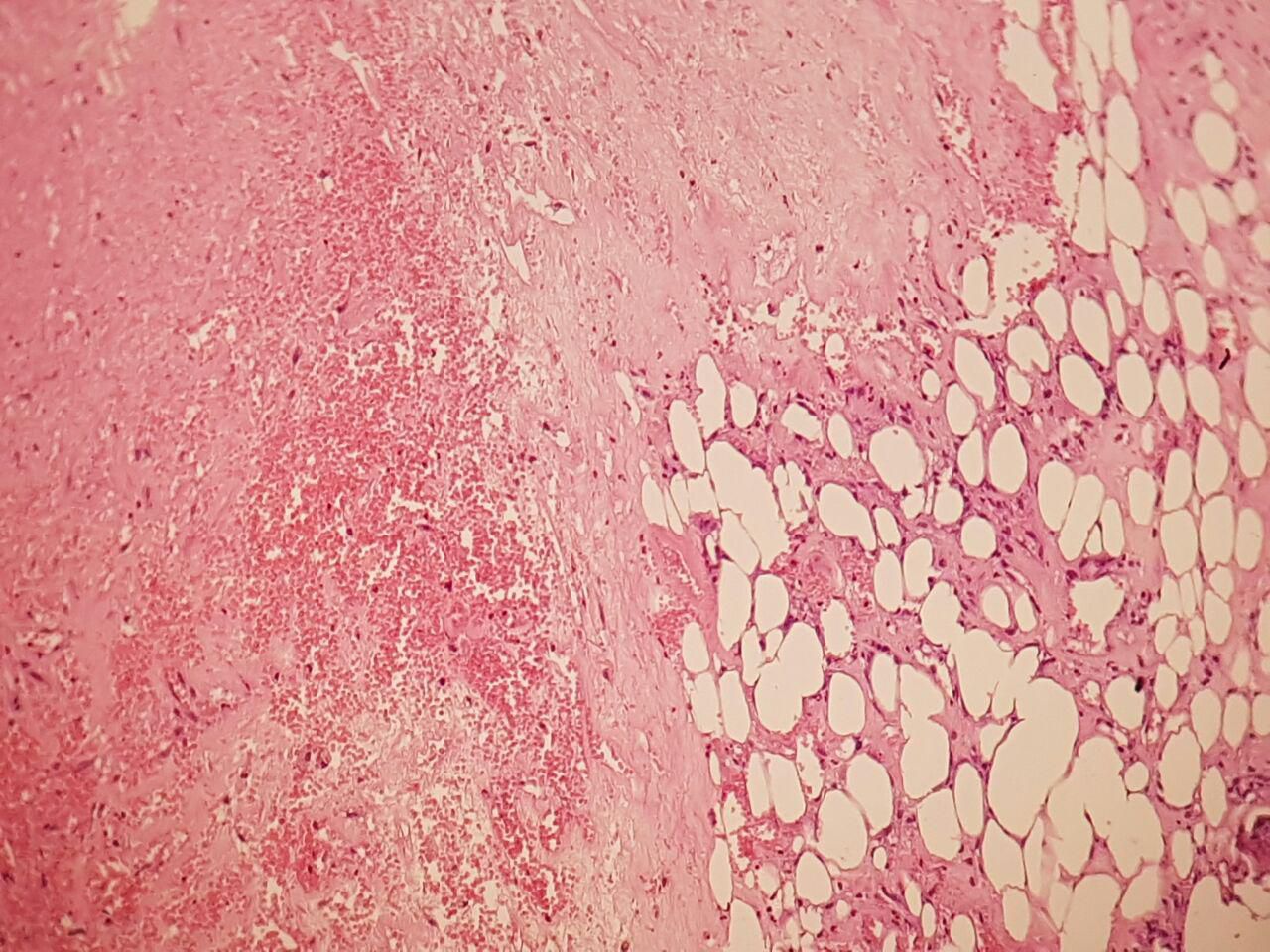
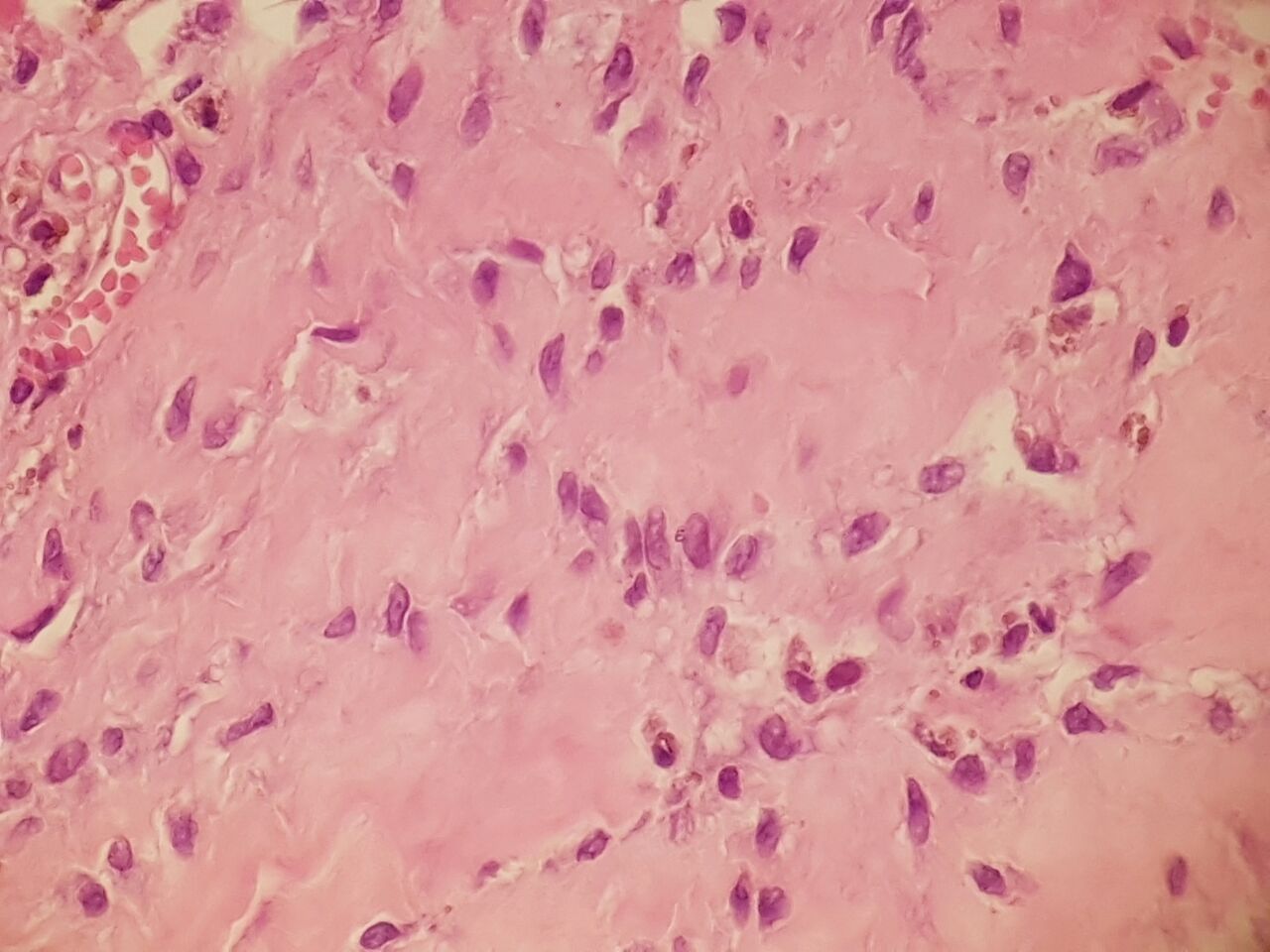
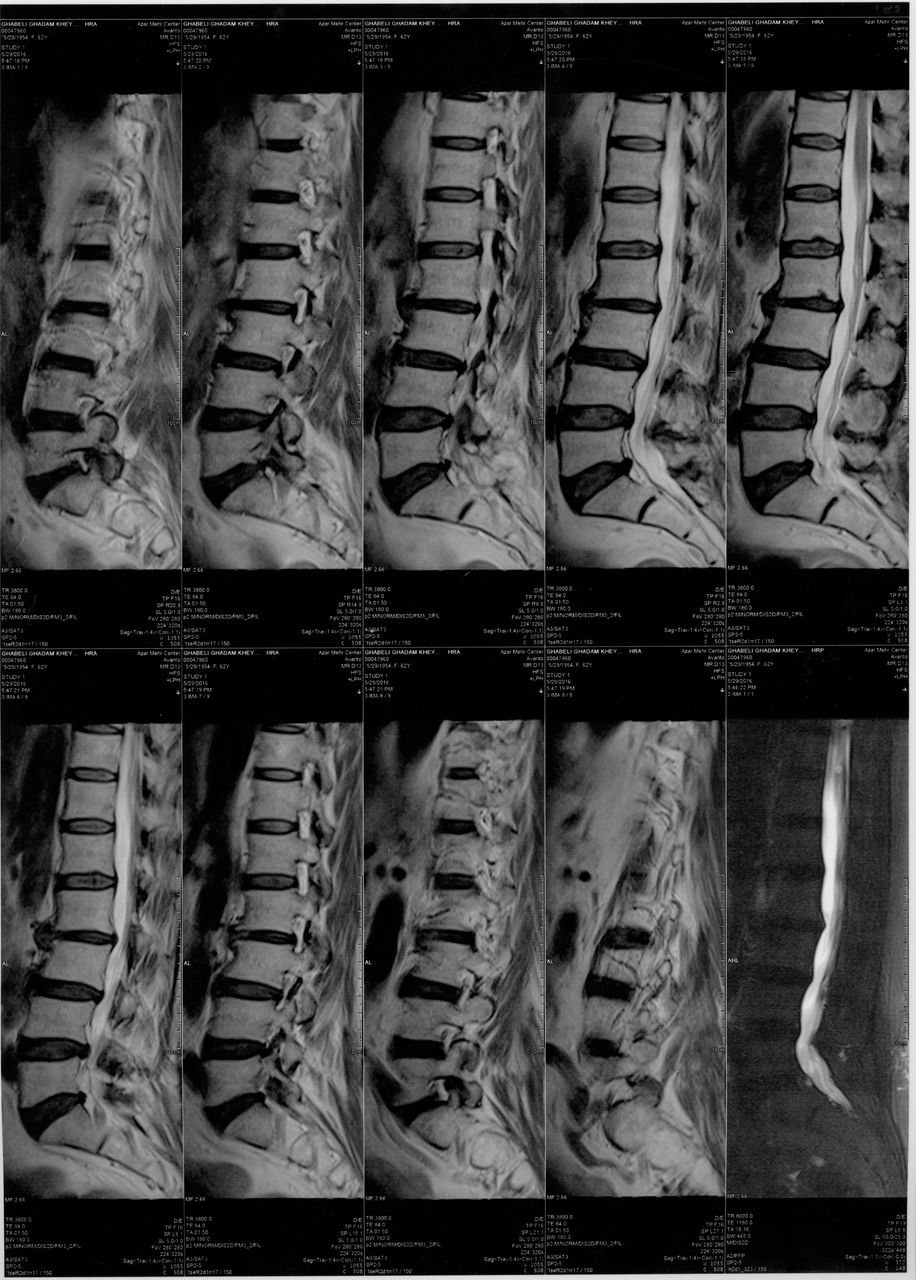
A 61-year-old woman with no past medical history who had been suffering from mild low back pain for 3 months presented with progression of symptoms and pain radiating to the right lower extremity for the past 4 weeks. She had no history of previous trauma, lumbar spine surgery, or anticoagulant therapy. She also had no medical illness, such as diabetes mellitus, hypertension, or other cardiac disease. All laboratory data, including coagulative tests, were normal and excluded bleeding tendency in the patient. On physical examination, she had tenderness in the paraspinal region at the level of the lower lumbar spine. Deep tendon reflexes in the lower extremities and bowel and bladder function were normal. The straight leg raising test was positive at 45 degrees on the right side. Also, neurological examination found four-fifths strength in the lower distal extremity of the right side and hyperesthesia in the right L4 and L5 sensory distributions. Lateral radiography of lumbar spine in flexion–extension showed no significant instability except mild spondylotic changes (Figure 1). Magnetic resonance imaging (MRI) revealed spinal cord compression at the L4-5 level caused by a postrolateral mass that was contiguous with the ligamentum flavum on the right side (Figure 2). Ligamentum flavum was obviously hypertrophic. The mass lesion appeared as an area of heterogeneous signal intensity on both T1-weighted and T2-weighted images. Contrast-enhanced MRI images were not obtained. Because of continuous low back and radicular pain, surgical treatment was indicated. The patient underwent a L4-5 laminectomy for decompression of the spinal canal and resection of the lesion. Easy aspiration of brownish fluid, suggesting an old hematoma, was done, and the remaining thickened ligamentum flavum was completely removed. The intraoperative diagnosis was LFH in the lumbar spine, and histological examination of the specimen confirmed our diagnosis (Figures 3 and 4). In the postoperative course, the patient's low back pain and radiculopathy resolved completely within a few days after the operation. Postoperation T2-weighted MRI confirmed that (Figure 5). She also experienced improvement in strength of the right lower extremity and increased sensitivity. The patient was discharged without any neurological deficit, and at 4 weeks after surgery follow-up, the patient remained asymptomatic.

Lateral radiography of lumbar spine in flexion–extension. There was no significant instability.

Magnetic resonance imaging shows spinal cord compression at the L4/L5 level and also ligamentum flavum on the right side.

Histological examination of the specimen confirms ligamentum flavum hematoma.
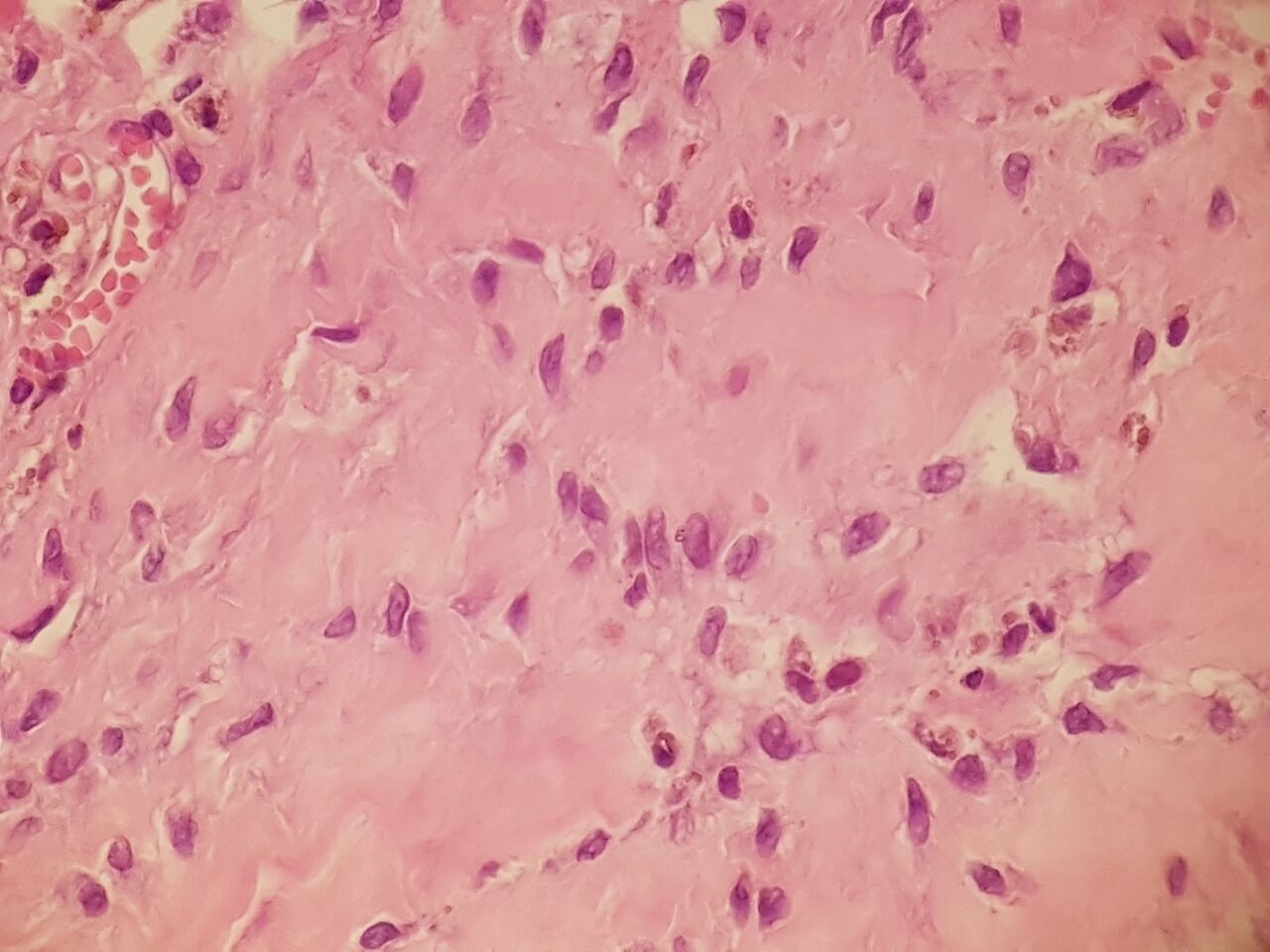
Histological examination of the specimen confirms ligamentum flavum hematoma.
Postoperation T2-weighted magnetic resonance imaging shows no sign.
DISCUSSION
Ligamentum flavum are long ligamentous structures in humans that are extended from the second cervical up to the lumbosacral vertebra. They consist of 80% elastic fibers and 20% collagen and have an assistive role in the maintenance of an erect posture. Ligamentum flavum are poorly vascularized, and only a few small vessels pass through it. Therefore, intraligamentous bleeding very rarely happens; distinguishing hematoma from other diseases, such as ganglion, synovial cyst, disk herniation, or neoplasm, can be difficult 5 For preoperative diagnosis of LFH, MRI imaging is the most preferred method, showing the heterogeneous intensity of the mass lesion continuous with ligamentum flavum. The mechanism of disease is still unclear, but vessel rupture within the ligamentum flavum or hemorrhage from the degenerative facet joint may be the cause of hematoma 4 Analysis of the previously reported cases of LFH showed these characteristics: The most commonly affected part in the spine is the lumbar area. The disease is caused mostly by minor trauma during normal activities. Most patients are middle aged or elderly males, and the disease commonly happens only at a single level, although involvement of more than one level has also been reported.4 In most patients, the clinical course progressively worsens. The treatment of choice for LFH is surgical removal of the lesion if progressive neurological symptoms occur. The analysis of reported cases also showed that total surgical resection of the mass lesion is an effective treatment for patients with LFH.2,3 Since LFH has no attachment to the facet joints, the stability of the lumbar spine can be regarded as intact, so simple microsurgical laminectomy provides an adequate operative view to remove the hematoma of ligamentum flavum, and in most cases additional fixation is unnecessary 6 We identified all the studies on LFH in patients with low back pain by a systematic search and hand search of the literature and electronic databases, including Google scholar, MEDLINE, and EMBASE for studies published until June 2016. The search term was “Ligament Flavum Hematoma” OR “LFH,” AND “Low back pain” OR “Lumbar spine.” The search resulted in 9 case reports of LFH with low back pain. Of the 13 cases of LFH who presented with low back pain, 9 were male, and 4 were female. The maximum age of presentation was 80 years, and the minimum age was 54 years.7–14 Table 1 shows the features of the described patient and the other cases of LFH with low back pain. This presented case of LFH in the lumbar spine was completely cured by total resection of the mass lesion through L4-5 laminectomy and relieved the patient's symptoms of low back pain and radiculopathy.
Features of the described patient and other cases of LFH with low back pain.
CONCLUSION
LFH is a rare cause of spinal root and canal compression that can be removed simply through surgery with excellent relief of symptoms. Low back pain occurs more in male in patients with LFH than in female patients. LFH is a rare differential diagnosis for cystic lesions in the lumbar spine.
- ©International Society for the Advancement of Spine Surgery
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.