


ABSTRACT
Background: Bone morphogenetic protein–2 (BMP-2) is an available bone graft option in spinal fusion surgery. The purpose of this study is to investigate the trends of BMP-2 utilization in adult spinal deformity (ASD) surgery.
Methods: The Nationwide Inpatient Sample database from 2002 to 2011 was reviewed. Inclusion criteria were patients over 18 years of age who underwent spinal fusion for ASD. Trends of BMP-2 use were examined over time, as well as stratified based on patient and surgical characteristics. All analyses were done after application of discharge weights to produce national estimates.
Results: There were 54 054 patients who met inclusion criteria and were included in this study. The overall rate of BMP-2 use was 39.7% (95% confidence interval 35.0%- 44.3%). Overall, there was steady increase in its use over time, with the highest peak in 2009 (55.3% of all cases used BMP-2), and then a decrease up to 37.9% in 2011 (P < .001). The rate of BMP-2 use was significantly higher for patients older than 54 years of age (compared to patients <54, P < .001). It was also higher in females (P = .009), Caucasian patients (P = .006), and Medicare patients (P = .006). Its use was 28.6% in the Northeast, 38.1% in the South, 45.2% in the Midwest, and 48.2% in the West (P = .035). Circumferential procedures had the highest rate of BMP-2 use (44.3%, P = .045). Average total hospital charges were $152,403 ± 117,454 for patients who did not receive BMP-2 and $205,426 ± 137,561 for patients who did (P < .001).
Conclusion After analysis of a large nationwide database, it was found that the rate of BMP-2 use in ASD surgery is approximately 40%. There was a significant increase in use from 2002 to 2009, and a decrease thereafter. The highest rates of use were found in older patients, female patients, white patients, Medicare patients, circumferential approaches, and patients undergoing surgery in the Midwest and West regions.
INTRODUCTION
First discovered in 1965, bone morphogenetic protein–2 (BMP-2) is a protein that functions as a differentiation factor and acts on mesenchymal stem cells to produce bone formation.1 Although only approved by the US Food and Drug Administration (FDA) for anterior lumbar interbody fusion with a cage,2 the off-label use in spinal fusion surgery has tremendously increased in the past decade.3 However, BMP-2 use has been associated, among others, with complications such as seroma, hematoma, and ectopic bone formation, which led the FDA to announce a public health notification in 2008 regarding potential hazards of its use.4
Adult spinal deformity is known to affect up to 70% of the elderly patients, though only a small percentage ultimately require surgical intervention. Long-segment fusions are commonly used for scoliosis correction, but nonunion may affect approximately 17% of patients.5 BMP-2 has been promoted as a potential factor in decreasing the rate of pseudoarthrosis.6 Ruofeng et al2 found in a 2015 study that the rate of BMP-2 use in patients over 65 years of age who underwent scoliosis surgery was 35.5%.
The purpose of our study is to analyze the trends in BMP-2 use for scoliosis surgery in patients over 21 years of age over a 10-year period, using a large nationwide inpatient database. Trends in BMP-2 use based on patient and operative characteristics are also reported, as well as factors associated with its use.
METHODS
Study Sample
The study sample for this investigation derived from the Nationwide Inpatient Sample (NIS) database for the years 2002 to 2011. This database is a government-sponsored inpatient database of all admissions from a 20% sample of nonfederal hospitals in the country. Given that all admissions from these hospitals are captured, the sample is designed to be nationally representative, and allows for calculation of national estimates using discharge weights (DISCWTs). Over 400 inpatient variables pertaining to demographic data, diagnoses, procedures, hospital charges, and others are captured and allow for analyses of large patient samples. Diagnoses and procedures are encoded in the form of International Classification of Disease 9th Edition (ICD-9) codes.7
For this study, patients with a principal diagnosis of spinal deformity were first identified (ICD-9 codes 737.10, 737.12, 737.19, 737.20, 737.21, 737.20, 737.21, 737.22, 737.29, 737.30, 737.32, 737.34, 737.39, 737.40, 737.41, and 737.42). Subsequently, patients who underwent primary or revision fusion procedures were also identified via use of codes 81.00 to 81.09 and 81.31 to 81.39. Patients younger than 21 years of age and nonelective admissions were excluded. This resulted in 11 043 identified cases, which after application of DISCWTs corresponded to 54 054 patients.
Collected Data
Reviewed demographic data included patient age, sex, race, insurance status, estimated median household income, hospital teaching status, and hospital region. Reviewed surgical data included use of BMP-2, revision status (primary versus refusion), use of osteotomy, approach, and number of levels fused. Other reviewed data included total adjusted hospital charges (excluding professional fees) expressed in 2016 US dollars and hospital length of stay.
Statistical Analysis
All analyses were performed in Stata SE 12 (StataCorp, College Station, Texas) after application of DISCWTs. The survey command in Stata was used for these analyses. Trends over time were analyzed using linear regression. Trends were also analyzed stratified by each of the following: age groups (21-54, 55-64, 65-74, and 75 and older), sex (male versus female), race (white, black, or Hispanic/other), insurance status (Medicare, Medicaid, versus private), hospital region (Northeast, Midwest, South, and West), hospital teaching status (teaching versus nonteaching), type of surgery (primary versus revision), technique (osteotomy versus no osteotomy), and number of levels fused (less than 8 versus 8 or more). Statistical significance was defined as P < .05.
RESULTS
A total of 54 054 patients who underwent adult spinal deformity (ASD) surgery between 2002 and 2011 were identified (Table 1). Average age at surgery was 59 ± 15 years; 27% of patients were male and 73% were female. Almost half of patients had Medicare as insurance (45.1%) and the other half had private insurance (46.9%). Almost half of patients had surgery in a Southern hospital (41.8%), followed by the Midwest region (27.6%). Over two-thirds of procedures were performed in teaching hospitals (63.1%), 11.6% were spinal refusion procedures, osteotomy was performed in 6.6% of cases, and fusion of 8 or more spinal segments was performed in 21.7% of all cases.
Characteristics of patients who underwent adult spinal deformity surgery.
The overall rate of BMP-2 use was 39.7% (95% confidence interval 35.0%-44.3%). Based on age groups, the overall rate of BMP-2 use was 34.5% for patients aged 21 to 54, 42.6% for patients aged 55 to 64, 42.0% for patients aged 65 to 74, and 41.7% for patients aged 75 or older (P < .001). The rate of BMP-2 use was 40.5% for females and 37.6% for males (P = .009), 41.4% for white patients, 29.5% for black patients, and 36.4% for Hispanic/others (P = .006). When stratified by insurance status, BMP-2 use was 42.7% for Medicare, 31.8% for Medicaid, 37.9% for private insurance, and 34.4% for others (P = .006); its use was 28.6% in the Northeast, 45.2% in the Midwest, 38.1% in the South, and 48.2% in the West (P = .035). Teaching hospitals and nonteaching hospitals had similar rates of BMP-2 use (38.1% versus 42.6%, P = .388). Its use in primary fusion procedures was 39.3% versus 42.3% in revision procedures (P = .129); 39.7% in nonosteotomy procedures and 38.9% in osteotomy procedures (P = .785); 39.0% in posterior-only procedures, 33.6% in anterior-only procedures, and 44.3% in circumferential procedures (P = .045); and 42.4% in 1- to 7-segment fusions and 47.3% in 8+ level fusion procedures (P = .190). Average total hospital charges were $152,403 ± 117,454 for patients who did not receive BMP-2 and $205,426 ± 137,561 for patients who did (P < .001); this corresponded to a $53,023 difference.
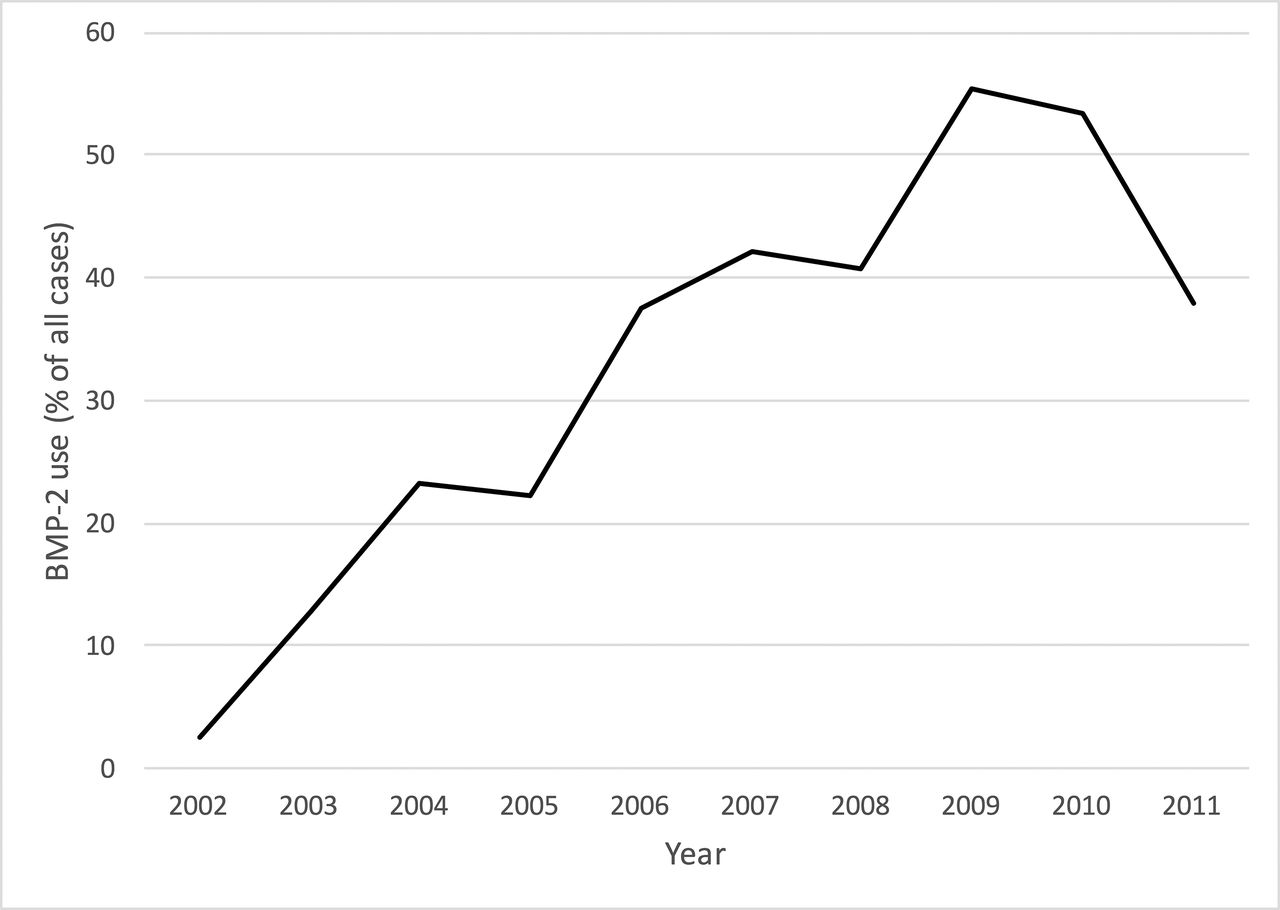
Overall, there was a significant change in the rate of BMP-2 use over time (Figure 1). Figure 2, A to F, depicts rates of BMP-2 use stratified by age group (A), sex (B), race (C), insurance (D), hospital region (E), and hospital teaching status (F). On the other hand, Figure 3, A to C, depicts rates of BMP-2 use stratified by primary versus revision status (A), use of osteotomy (B), and number of levels fused (C). All changes over time were found to be statistically significant (all P < .001).
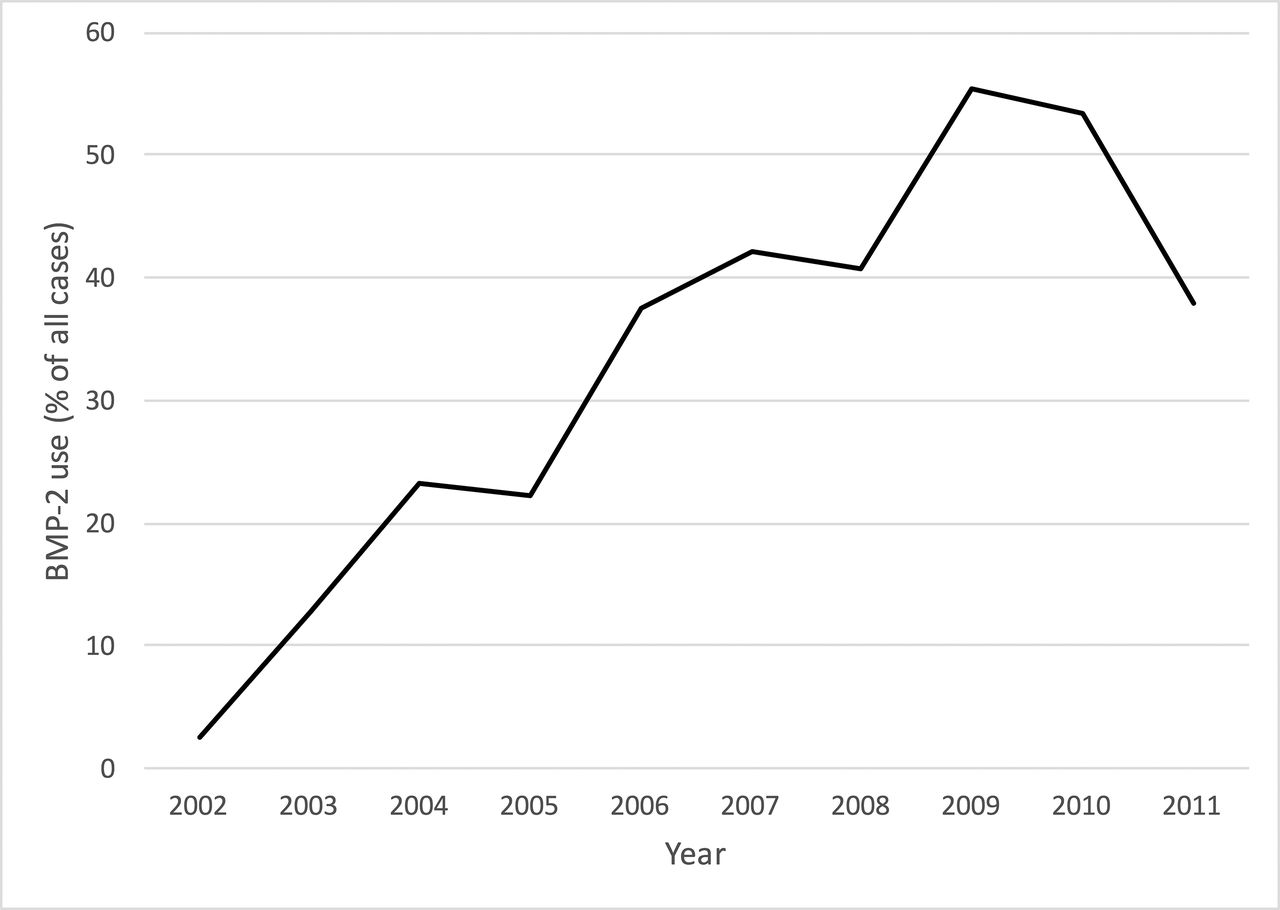
Rate of BMP-2 use over time (P < .001).
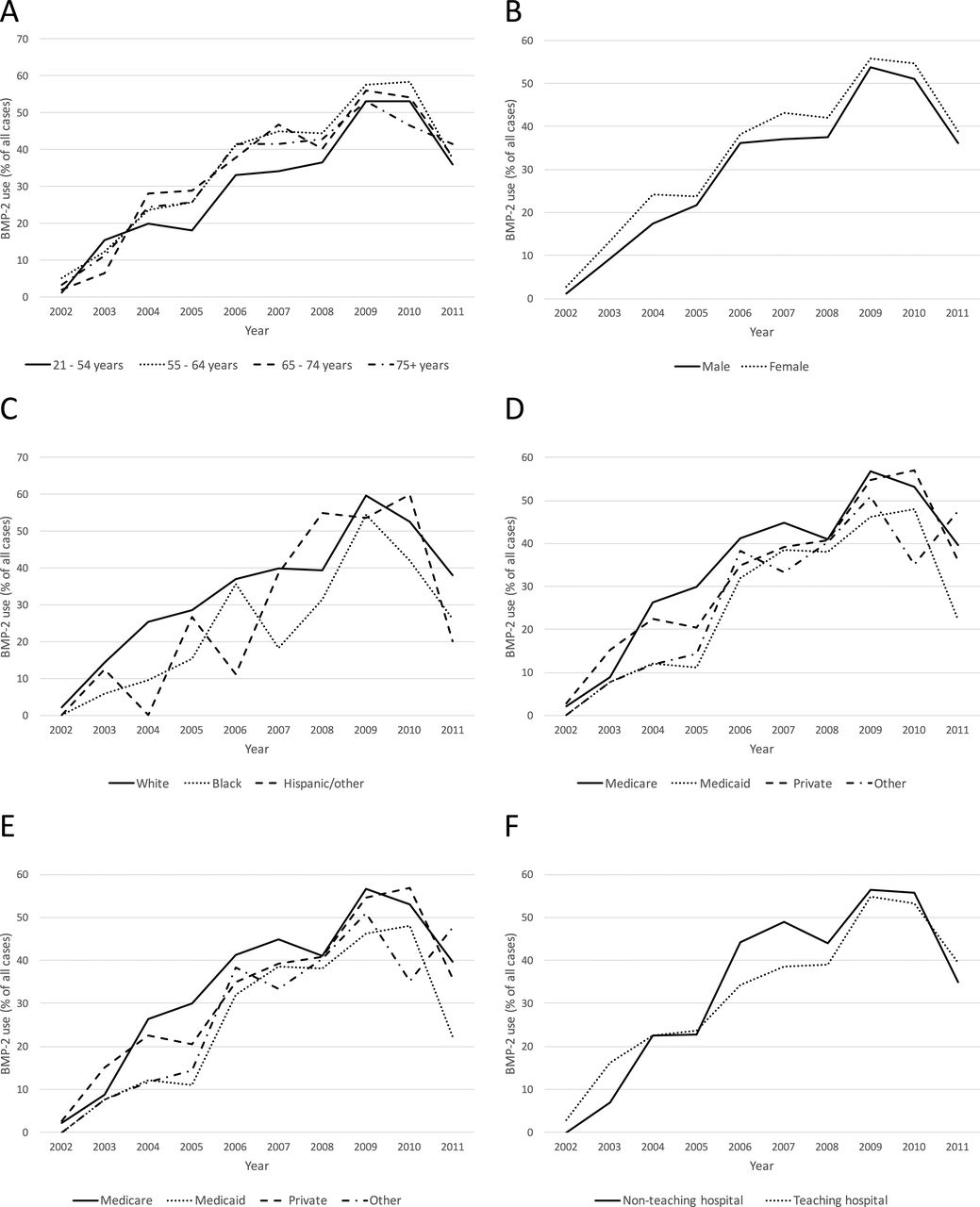
Rates of BMP-2 use stratified by (A) age group, (B) sex, (C) race, (D) insurance, (E) hospital region, and (F) hospital teaching status. All changes over time were found to be statistically significant (all P < .001).

Rates of BMP-2 use stratified by (A) primary versus revision status, (B) use of osteotomy, and (C) number of levels fused. All changes over time were found to be statistically significant (all P < .001).
DISCUSSION
Although initially approved only for anterior lumbar interbody fusion, BMP-2 has been used for posterior lumbar fusion, posterior thoracic fusion, anterior cervical fusion, and posterior cervical fusion; for ASD patients, rates of BMP-2 use are approximately 35.5% to 61.6%.2,8 In this study, we found a similar rate of 39.7%, with a steady increase in its use up to 2009 and then a decrease thereafter up to 2011.
Ruofeng et al2 reported similar findings in their study of 29 787 patients over the age of 65 who underwent posterior long-segment fusion for scoliosis; the rate of BMP-2 use decreased also after 2009. However, Ruofeng et al2 reported an increase after 2010, which is different from our findings. One of the possible explanations for this is that Ruofeng et al2 only looked at posterior instrumentations, whereas our present study also included anterior and circumferential fusions. In fact, the highest rate of BMP-2 use was in patients who underwent anterior-posterior fusion (44.3%). Similarly, Martin et al3 reported a rapid increase in BMP-2 use for cervical and lumbar fusion operations (degenerative conditions) up to 2008 (involving up to 45.2% of lumbar and 13.5% of cervical operations); there was an average annual decrease of 11.7% thereafter. However, in our current study there was an increase between 2008 and 2009, which likely reflects different practices when using BMP-2 in degenerative conditions (as in the investigation by Martin et al3) versus deformity. The decrease in the use of BMP-2 after 2008/2009 is most likely the result of the FDA warning in 2008, which stated that the use of the osteoinductive agent for cervical spine operations was associated with serious and potentially life-threatening complications such as breathing/swallowing difficulty.2 Likewise, McKie et al9 noted a decrease, albeit small, in the use of BMP-2 for anterior cervical fusion after the 2008 warning (5% decrease compared to the preadvisory era). Although the warning was issued primarily for cervical spine surgery, it is interesting that the use of BMP-2 use also decreased in lumbar degenerative disease and adult deformity surgery.
Nonetheless, the use of BMP-2 in adult scoliosis surgery has not been associated with a significant risk of complications in other investigations. In a report of 279 ASD patients from the International Spine Study Group, authors noted 172 patients (61.6%) in whom BMP-2 use was used.8 Although patients who received BMP had higher rates of total complications (1.4 versus 0.6 complications per patient) and minor complications (0.9 versus 0.2), BMP did not increase the risk for acute major, neurological, or wound complications.8 Furthermore, the use of BMP-2 has been associated with a significantly decreased risk of reoperation due to pseudoarthrosis after ASD surgery (5.0% versus 33.9% for patients in whom BMP-2 was not used).6
When looking at factors associated with BMP-2 use, we found that the use of BMP was higher in patients above 55 years of age, higher in females, white patients, and Medicare patients, and in the Midwest and West regions. Interestingly, the rate of use was not different for primary versus revision procedures, osteotomy versus no osteotomy, or fusion procedures involving less than 8 versus 8 or more segments. These findings suggest that there are certain patient/regional discrepancies in the use of BMP, but the exact cause is unknown and warrants further investigation.
Interestingly, the impact of BMP-2 use in hospital charges was significant, increasing the total charges on average by $53,023. While it has been shown that its use significantly decreases the need for further revision surgery due to pseudoarthrosis,6 a 2007 systematic review on BMP-2 use concluded that there is limited evidence to support greater improvement in clinical outcome for patients who use this agent, and that “the use of BMP for spinal fusion is unlikely to be cost-effective” given the high cost of this product.10 Although revision fusion procedures have been found to significantly increase the cost of surgery compared to primary procedures ($176,809 versus $161,791 in fusion procedures with 4+ levels),11 no formal cost-effectiveness analysis in the ASD population has been performed yet, and this may be the next step in evaluating the long-term efficacy of BMP-2 use in scoliosis surgery. Specifically, it would be interesting to evaluate whether utilizing BMP and potentially preventing need for further revision surgery is more cost effective than not utilizing BMP and potentially increasing the risk for pseudoarthrosis/instrumentation failure.
Limitations
Although this study provides a large picture of trends of BMP-2 use for ASD surgery over time in the United States, it has several limitations. The use of ICD-9 codes for identification of diagnoses and procedures has risk of miscoding, though the NIS undergoes quality control measures and multiple studies have used this database to examine trends and outcomes in spine surgery.3,9,12–17 Another important limitation is that the NIS database is not specific for spine surgery, so variables such as global spinal alignment, radiographic parameters, specifics of implants utilized, and others are unfortunately not available for review.
CONCLUSION
After analysis of a large nationwide database, it was found that the rate of BMP-2 use in ASD surgery is approximately 40%. There was a significant increase in use from 2002 to 2009, and a decrease thereafter. The highest rates of use were found in older patients, female patients, white patients, Medicare patients, circumferential procedures, and patients undergoing surgery in the Midwest and West regions.
Footnotes
Disclosures and COI: The manuscript submitted does not contain information about medical device(s)/drug(s). No funds were received in support of this work. The authors have no conflicts of interest.
- ©International Society for the Advancement of Spine Surgery
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.