


ABSTRACT
Background: The aim of our study was to identify factors that influence the occurrence of adjacent fractures in patients with cement-augmented pedicle screw instrumentation.
Methods: Data were retrospectively collected from medical charts and operative reports for every surgery in which cement-augmented instrumentation was used in our hospital of 4 consecutive years. A total of 93 operations were included and examined for gender, age, T-score, number of fused segments, number of implanted screws, broken screws, loosening of screws, leakage and distribution pattern of cement, pre- and postoperative kyphosis angle, revision surgery and adjacent fractures in follow-up. Categorical data were compared using the χ2 test or by Fisher's exact test, as appropriate. Continuous variables conforming to a normal distribution were compared using Student's t test. Otherwise the Mann-Whitney U test was applied. A P-value of <.05 was considered statistically significant. A trend was defined as a P < .2.
Results: The mean age was 68.1 years with a mean T-score of −3.12. Nineteen adjacent fractures occurred during follow-up and the median follow-up was 12 months (range, 1−27). Patients showed a higher risk for adjacent fractures following revision surgery (P = .016). Most fractures occurred superior to the instrumented level (P = .013) and in the first 12 months. Difference of T-score between the group “no adjacent fracture” and the group “adjacent fracture” was 0.7 (P = .138). Another trends were found in greater age (P = .119) and long instrumentations (P = .199).
Conclusions and Clinical Relevance: Revision surgeries are associated with a higher risk of adjacent fractures. In these cases, prophylactic kyphoplasty of the superior vertebra should be considered. This study is a retrospective, nonrandomized cohort/follow-up study.
Level of Evidence: 3.
INTRODUCTION
The proportion of elderly people is growing, particularly in industrialised countries.1–3 For this reason, there are a greater number of patients with reduced bone quality and consequent degenerative spine disease and osteoporotic fractures that require surgical treatment.1,2 In recent years, various surgical techniques have been developed to improve the fixation strength of implants in the osteoporotic spine, including supplemental laminar hooks, bicortical screw purchase, improved screw geometry and the augmentation of screws with bone cement.4 Cement-augmented pedicle screws are the most frequently used of these options in clinical practice.
Various cadaver studies have shown that fixation strength in osteoporotic bone is greater with cement-augmented screws than with noncement-augmented screws.5–7 Poly(methyl methacrylate) (PMMA) is the gold-standard cement for providing additional screw fixation. However, the use of cement carries its own risks, such as damage to neural structures, vascular injury, and pulmonary embolism caused by the leakage of cement out of the vertebral body. Furthermore, the biomechanical properties of the spine are altered when cement augmentation is used.1–3 In particular, there is greater stress on the vertebrae adjacent to the cement-augmented instrumentation, increasing the risk of subsequent fractures in these vertebrae.8,9
In this study, we examined the incidence of subsequent fractures in patients with decreased bone quality who received surgery involving cement-augmented pedicle screws. Herein, risk factors for the occurrence of subsequent fractures are identified.
MATERIALS AND METHODS
Patient Selection and Data Acquisition
This was a retrospective, single-center study. Between January 2010 and November 2013, a series of 87 patients with osteoporosis underwent 93 spinal instrumentation surgeries involving the application of high-viscosity PMMA cement (Confidence Spinal Cement System, DePuy Synthes, Indianapolis, Indiana) via a cannulated and perforated pedicle screw system (Viper 2, DePuy Synthes). These patients' demographic and clinical data were retrospectively collated from our institution's electronic record systems. Patients were clinically evaluated at each of the following time points after surgery: at 3, 6, 12, and 24 months. Postoperative bracing is not standard practice in our institution and none of the patients included in this study received a brace following surgery. In those patients who received bone grafts, local autologous bone was used.
The following variables were collected and included in analyses: patient age and sex, T-score, number of fused segments, number of implanted screws, number of broken screws, presence of screw loosening, particulars of the cement distribution pattern including any leakage, pre- and postoperative kyphosis angle, need for revision surgery, and occurrence of adjacent fracture during follow-up. The T-score was determined by preoperative quantitative computed tomography (QCT) of the first 3 lumbar vertebrae (L1 to L3). If any of these vertebrae were affected by pathology other than osteopenia or osteoporosis, the bone density of a neighboring vertebra was determined (eg, T12 or L4). Only patients with a T-score below −2.5 were included in this study. The kyphosis angle was ascertained from the midsagittal plane of a computed tomography (CT) scan. Here, the Cobb angle was determined between the endplates of the last instrumented (cranial and caudal) vertebral body. The degree of correction of kyphosis was determined as the difference between the preoperative kyphosis angle and the angle observed on the last radiological examination during the follow-up period.
Cement distribution and leakage pattern were analyzed on postoperative CT scans. The leakage pattern was classified as “prevertebral,” “paravertebral,” or “intraspinal.” The cement distribution was divided into the categories “concentrated” and “scattered.” Adjacent fractures were considered relevant only if they were both symptomatic and radiologically evident (on CT and/or magnetic resonance imaging scans).
Statistical Methods
SPSS Statistics for Windows version 22 (IBM, Armonk, New York) was used to perform statistical analyses. Variables were coded, depending on their characteristics, as nominal (eg, patient sex, presence of adjacent fracture, diagnosis), ordinal (eg, T-score) or metric (eg, body mass index, angular kyphosis, number of implanted screws). Discrete variables are expressed as counts (percentage) and continuous variables as means ± standard deviation (SD) or median and interquartile range (IQR) unless stated otherwise. Categorical data were compared using the χ2 test or by Fisher's exact test, as appropriate. Continuous variables conforming to a normal distribution were compared using Student's t-test. Otherwise the Mann-Whitney U test was applied. A P value of <.05 was considered statistically significant. A trend was defined as .05 < P < .2.
RESULTS
There were 41 males and 46 females in our cohort, with a mean patient age of 68.1 years (SD: 10.8 years; Table 1). Patients were followed postoperatively for a median of 12 months (range, 1–27 months). The most common indication for surgery was an unstable osteoporotic burst fracture (n = 42/87; 45.2%). A total of 513 cement-augmented screws were implanted (Figure 1). In most cases a screw was implanted in the second lumbar vertebra (n = 76/87). The mean T-score was −3.12. However, several patients in our cohort had a preexisting clinical diagnosis of osteoporosis; these patients (n = 9/87; 9.7%) did not receive a further QCT scan within the setting of the present study and they were not included in our calculation of the mean T-score for the cohort.
Patients characteristics with and without adjacent fractures.

Distribution of screw placement in the thoracic and lumbar spine.
Cement leakage was observed in 87/93 procedures (93.5%), relating to 236/515 screws (45.8%). Intradiscal cement leakage was observed in 2 cases; however, this leakage was not clinically relevant and the patients had no relevant signs or symptoms. A revision owing to cement leakage was necessary for one patient (n = 1/93; 1.1%); here a prevertebral cement leakage spread via the inferior vena cava into the right atrium and the patient underwent intervention at the hands of our institution's cardiac surgery team as a results.
In 78.5 % of all cases (n = 73/93) a concentrated cement distribution in the vertebral body was noted. Two screw cut-outs (n = 2/513; 0.38%) and 10 screw fractures (n = 10/513; 1.94%) were evident. In 3 of these 10 cases of screw fracture, pseudarthrosis was noted. Fifty percent (n = 6/12) of hardware failure occurred at the thoracolumbar junction. During the follow-up period, 19 adjacent fractures in 14 patients were observed (Table 2). Seventeen fractures (89%) were seen superior to the fused segments and 2 fractures occurred in an adjacent vertebra inferior to the fusion, which was a significant finding in bivariate analysis (P = .013). In cases in which an adjacent fracture was determined, there was a mean time to fracture occurrence of 8.5 months (range, 1–18 months). Most adjacent fractures appeared within the first 12 months following surgery (n = 15; 78.9%). Patients with an adjacent fracture had a mean T-score of −3.76 compared with −3.06 in patients without a fracture (Table 1). No statistically significant difference between these values was detected using the Mann-Whitney U test (P = .138).
Distribution of adjacent fractures.
In the subgroup of patients undergoing revision surgery, an adjacent fracture occurred in more than one third of cases (35.2%). Each of these patients was operated at least once before the revision surgery (median: 2; range, 1–4 times). In half of these cases (n = 7/14) a lumbar stenosis was the reason for the initial surgery. The first operation was a posterior lumbar interbody fusion in 10/14 cases (71.4%). Within this subgroup, there were a significantly higher number a fused segments (mean = 4.6; P = .001) and the patients were significantly older, by a mean of 4 years (67.5 vs. 71.8 years; P = .046). These results are presented in Table 3.
Comparison of the subgroups “revision surgery” and “no revision surgery.
There were no statistically significance differences in the rate or pattern of adjacent fractures when the cohort was analysed with respect to gender, number of implanted screws, broken screws, loosening of screws, cement distribution pattern and leakage, pre- and postoperative kyphosis angle, or the occurrence of adjacent fractures during follow-up. A trend was detected with respect to patient age (P = .119), T-score (P = .138) and number of fused segments (P = .199).
DISCUSSION
The augmentation of pedicle screws with cement is the gold standard for treatment of spinal pathologies requiring posterior pedicle screw instrumentation in patients with reduced bone quality. Various studies have demonstrated the advantages of cement-augmented stabilisation,4–6 which results in enhanced fixation of screws in the vertebral body. The frequency of adjacent fractures and risk factors for adjacent fracture have received little attention, despite it being self-evident that cement application to the operated vertebral body or bodies, and the fixation of 1 or more segments, may pose additional mechanical stress on adjacent vertebrae.
The aim of this study was to determine the characteristics of patients with cement-augmented pedicle screw instrumentation who developed an adjacent fracture during follow-up. Studies on this particular subject are rare and have incorporated only small patient cohorts.10–12 For this reason, we consulted previous clinical studies addressing adjacent fractures after vertebroplasty or kyphoplasty to assist us in identifying potential risk factors to investigate.
The pathogenesis of subsequent, adjacent fractures has primarily been attributed to the decreased bone density of adjacent vertebrae compared to the operated vertebrae. Phillips et al13 determined that the fusion of spinal segments in vertebroplasty and kyphoplasty surgery causes increased stress on the adjacent vertebrae. In addition, prolonged immobilisation is described as a risk factor for these fractures. There have been several studies investigating the occurrence of subsequent fractures following vertebroplasty or kyphoplasty, and rates of up to 52% are mentioned.14,15 In terms of risk factors, the application of a large volume of cement (more than 6 mL per vertebral body), intradiscal cement leakage, pronounced restoration of the vertebral body, greater age, fracture as the initial diagnosis, and reduced bone density are associated with the occurrence of adjacent fractures after vertebroplasty or kyphoplasty.16,17 In our study, we determined that clinically and radiologically apparent adjacent fractures occur following 15.1% of cement-augmented instrumentations. Several risk factors may be associated with the development of such adjacent fractures after cement-augmented instrumentation, which we now discuss.
Age
In our study, we found a slight difference in the age group (P = .119). Older patients had a higher risk of adjacent fracture. Similar results have been reported in the literature.13,14
Bone Density
Several studies have demonstrated that patients with decreased bone density have an increased risk of fracture after kyphoplasty.16,17 In our study, the T-score in the group with adjacent fractures was lower by a mean of 0.7 points compared to the group without a fracture. A trend was found (P = .137).
Patient Sex
We did not observe a sex-specific effect on the occurrence of subsequent fractures, in agreement with the preexisting literature. In a cohort of postmenopausal women, Etebar et al2 reported a high rate of adjacent segment degeneration after lumbar instrumentation without cement augmentation. Based on our retrospective data set, we were unable to determine what proportion of our cohort were postmenopausal women.
Correction of Kyphosis
In a case series examining outcomes after vertebroplasty, Rho et al16 found that a greater height restoration of the fractured vertebra is itself a risk factor for an adjacent fracture. In our study, we examined the difference between the pre- and postoperative kyphosis and compared this with the occurrence of subsequent fractures. There was no statistically significant difference in the degree of kyphosis correction between the “adjacent fracture” and “no adjacent fracture” groups.
Instrumented Level
In our study, subsequent fractures were significantly more likely to occur above the spinal fusion, equating to 85% of the fractures seen in our cohort. The findings of a cadaver study by Bastian et al,18 where the authors observed increased mobility and stress in the area above dorsal instrumentations, may provide a mechanistic basis for this finding. Increased mechanical stresses were less apparent in the level below the spondylodesis.
Cement Distribution
Hu et al19 investigated cement distribution around the screw tip after screw insertion into the vertebral body. They concluded that cement distribution (concentrated versus scattered) varies according to bone structure and density. In that study, the subgroup with scattered cement distribution had significantly higher rates of cement leakage.19 In our patient population, a scattered distribution was found in 22% of patients and we did not find a significant relationship between cement leakage and the occurrence of subsequent fracture.
Revision Spine Surgery and Long Instrumentation
We investigated whether patients undergoing revision surgery or complex, multisegment interventions were more likely to experience subsequent fracture. In our cohort, those undergoing revision surgeries did indeed experience a significantly greater number of subsequent fractures. These patients were, on average, 5 years older than those undergoing first surgery, and also had significantly more fused segments. These findings are in agreement with those of Phillips et al,13 who showed that patients with longer spinal instrumentations tended to develop subsequent fractures because of higher stress through the adjacent vertebrae.
Time of Occurrence
The vast majority of subsequent fractures, nearly 80%, were detected within the first 12 months following surgery (Figure 2), in accordance with previous literature.16 Based on this finding, it would seem sensible for patients to be monitored frequently in an outpatient setting during the first year.
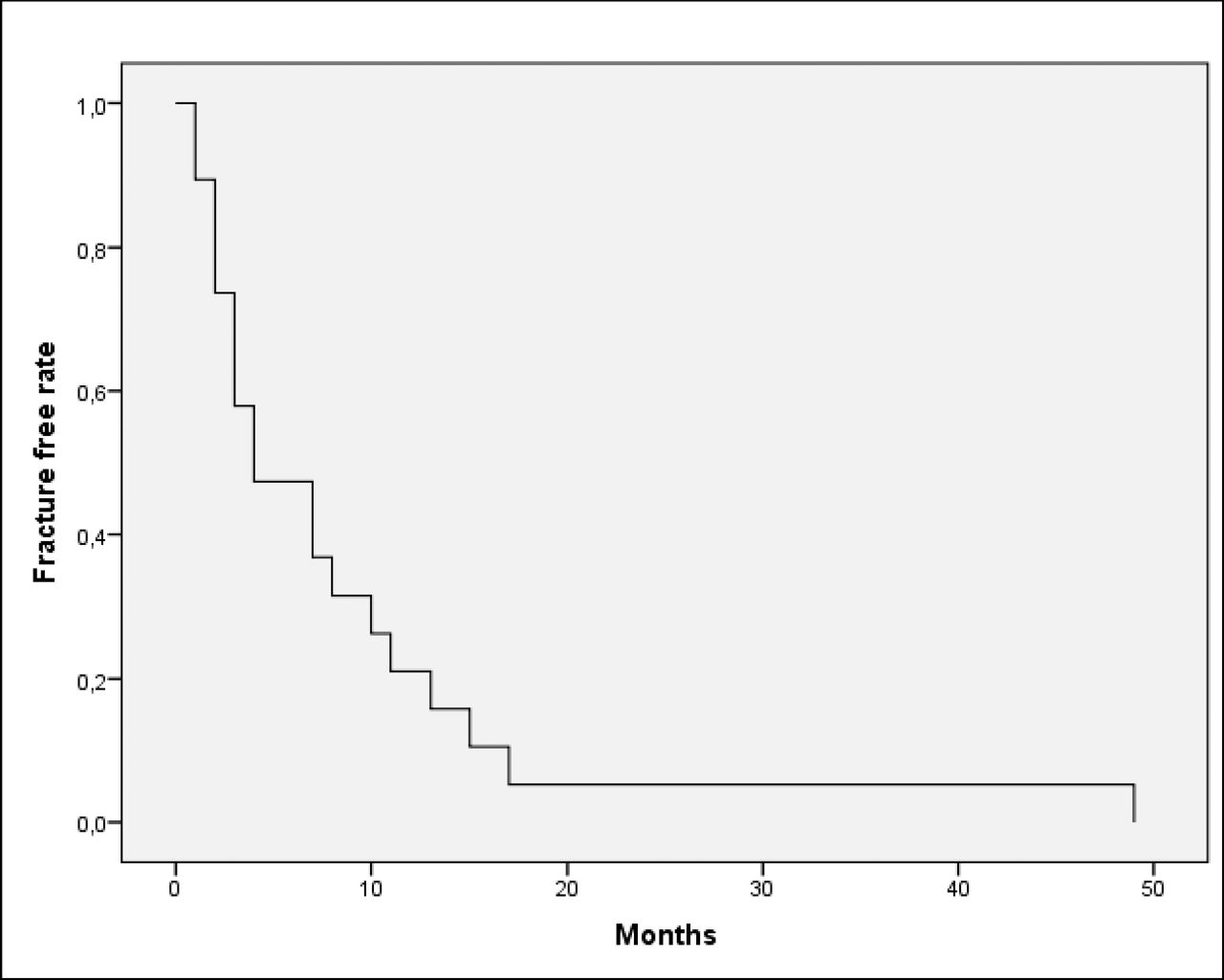
Kaplan-Meier fracture-free probability curve for patients in whom adjacent fractures occurred.
LIMITATIONS
This was a single-center and retrospective study and therefore has inherent limitations. In addition, the mean follow-up period of 12 months is relatively short. A proportion of patients were operated on in our tertiary-level, academic center, and then returned to smaller hospitals closer to their homes, leaving them lost to intensive follow-up. Another point of criticism is that the bone density was determined retrospectively and was not determinable for every patient in our study.
CONCLUSIONS
Our findings show that cement-augmented pedicle screw instrumentations have good fixation strength in patients with reduced bone density. Patients with a very low bone density, greater age, and long instrumentation showed a trend toward a higher frequency of occurrence of adjacent fractures. Revision surgery was a risk factor for adjacent fracture and most fractures occurred above the instrumentation. Patients should be followed up regularly in the first 12 postoperative months to enable early detection of potential adjacent fractures. Clinical and biomechanical studies suggest that the occurrence of subsequent fractures may be reduced by prophylactic kyphoplasty of the upper vertebra adjacent to a multilevel lumbar fusion.20–22 In conclusion, we propose that a kyphoplasty or vertebroplasty of the upper adjacent vertebral body to an instrumentation should be discussed in patients with revision surgery to reduce the rate of a subsequent fracture.
Footnotes
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2018 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.