


ABSTRACT
Background: Performing an adequate transforaminal lumbar interbody fusion (TLIF) discectomy requires numerous instrument passes, increasing surgical time and the risk of complications. The purpose of this study was to evaluate the efficacy and efficiency of discectomy and endplate preparation during TLIF using traditional manual instrumentation versus a novel suction discectomy curette. The direct economic benefit with use of the suction discectomy curette is calculated.
Methods: Three experienced, spine-fellowship-trained surgeons performed TLIF discectomies on 3 cadaveric specimens from T12 to S1 using either traditional manual discectomy instruments or CONCORDE Clear (Xtool) devices supplemented with manual discectomy instruments. For each level in which a discectomy was performed, the following were measured: elapsed time, number of instrument passes and the number of instrument exchanges, and estimated tissue volume.
Results: Transforaminal lumbar interbody fusion discectomy times improved on average 11:32 minutes per level, which equates to an estimated procedural time savings of 15:85 minutes, using 1.4 levels per TLIF, the average number of levels in a large series. Usage of the CONCORDE Clear significantly reduced instrument passes compared to traditional, with a mean of 62.0 for traditional versus 7.1 for CONCORDE Clear, an 8.7-fold improvement. Instrument exchanges showed a 5.9-fold improvement, with means of 26.8 and 4.6, respectively. Wet discectomy tissue volume was measured for each discectomy, with a mean of 5.4 cc for traditional versus 12.9 cc for CONCORDE Clear, a 2.4-fold improvement.
Conclusions: This study estimates that, in a typical TLIF procedure, over 15 minutes should be saved by using the CONCORDE Clear l device (a quarter of the time of a traditional discectomy), and by considering the direct cost-benefit associated with this time savings as well as reduced sterilization costs, it is estimated that a hospital could save approximately $1300 in operating room time and sterilization cost with the use of the CONCORDE Clear device in a typical 1-level TLIF procedure.
BACKGROUND
Several access techniques exist for performing lumbar interbody fusion. The anterior approach to the spine (anterior lumbar interbody fusion [ALIF]) is still considered the gold standard for having the highest rate of lumbar interbody fusion due to the most complete discectomy obtained secondary to disc access and direct visualization. Transforaminal lumbar interbody fusion (TLIF), which uses a posterior unilateral approach and avoids the morbidity of an anterior approach, is currently the most common type of lumbar interbody fusion in the US. Despite its popularity, the discectomy is technically more challenging and less complete, as access and visualization of the disc space is limited. In addition, today's various manual discectomy instruments have not changed over the last 20 years and require many instrument passes and exchanges to perform the discectomy. The discectomy is therefore time consuming, yet this is not documented well in the literature. A previous study was performed to quantitatively compare the traditional technique to a suction-curette discectomy (CONCORDE Clear MIS Discectomy Device/Xtool). This previous study succeeded in demonstrating a statistical improvement in the amount of disc removed (overall and by quadrant) and a reduction in the number of instrument passes (data reported in posters at Society for Minimally Invasive Spine Surgery 2013, American Academy of Orthopedic Surgeons 2014, and International Society for the Advancement of Spine Surgery 2014), yet this study failed to show a statistical improvement with regard to time. It is believed that true discectomy time in the operating room was not accurately simulated in this previous cadaveric study. Factors which were not accounted for which would affect discectomy time include: the number of instrument passes and exchanges to minimize endplate damage, the use of magnification, and better simulation of the operating room environment, including the use of the pace used on a live patient rather than that of a typical lab.
OBJECTIVE
This study is intended to assess the overall efficiency of traditional manual discectomies (“traditional” group) versus discectomies using a suction-curette (“CONCORDE Clear” group) using a TLIF approach as would be performed in patients, using human cadavers.
Primary Objective
Compare Discectomy Times (Operative Measurement)
Compare postannulotomy discectomy times for 2 fusion discectomy methods, traditional versus CONCORDE Clear. Additionally analyze any discectomy time savings in terms of economic impact for a hospital.
Secondary Objectives
Compare Discectomy Instrument Passes (Operative Measurement)
Compare discectomy instrument passes and exchanges (postannulotomy) for 2 fusion discectomy methods, traditional versus CONCORDE Clear.
Compare Volumes of Wet Discectomy Tissue (Postoperative Parameter)
Compare estimated wet discectomy tissue volumes for 2 fusion discectomy methods, traditional versus CONCORDE Clear. Additionally analyze and compare discectomy tissue volume removal per minute.
METHODS
Three experienced, spine-fellowship-trained surgeons performed TLIF discectomies on 3 cadaveric specimens from T12 to S1 (a maximum of 18 possible levels). Disc levels had discectomies performed using either traditional manual discectomy instruments (traditional) or CONCORDE Clear devices supplemented with manual discectomy instruments (CONCORDE Clear). Once the first specimen randomly received a discectomy from 1 group, all levels for the rest of the specimens were alternated for discectomy type (in sequence, moving up the lumbar spine).
The CONCORDE Clear discectomy device (DePuy Synthes) functions as a suction curette that simultaneously cuts and evacuates target disc tissue (Fig. 1). The device has a cutting tip with variable angles (15, 30, and 40°) with cutting edges that shear disc material from the endplates while the suction draws disc material into the tube. A tip guard distal to the cutter makes the tip blunt to impede penetration of the anterior annulus and minimize clogging of the tip (Fig. 1). Standard wall suction (300–600 mmHg) transports strips of cut disc tissue from the distal cannula near the cutter into a clear handle that collects tissue, similar to a suction canister.
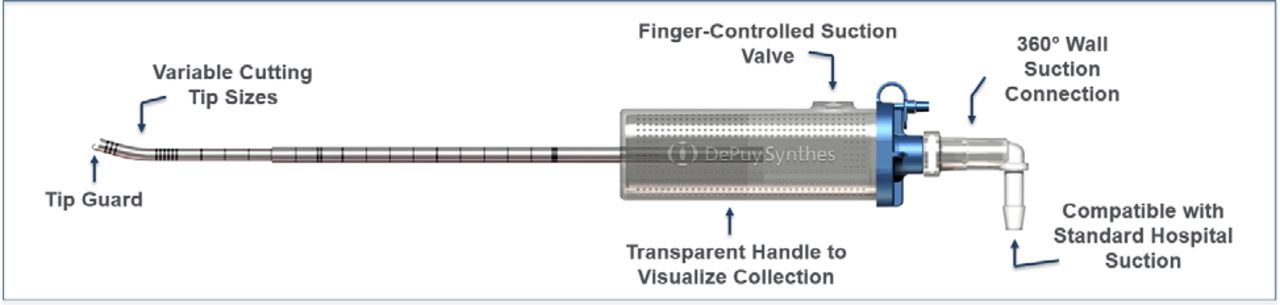
CONCORDE Clear MIS Discectomy Device (Xtool).
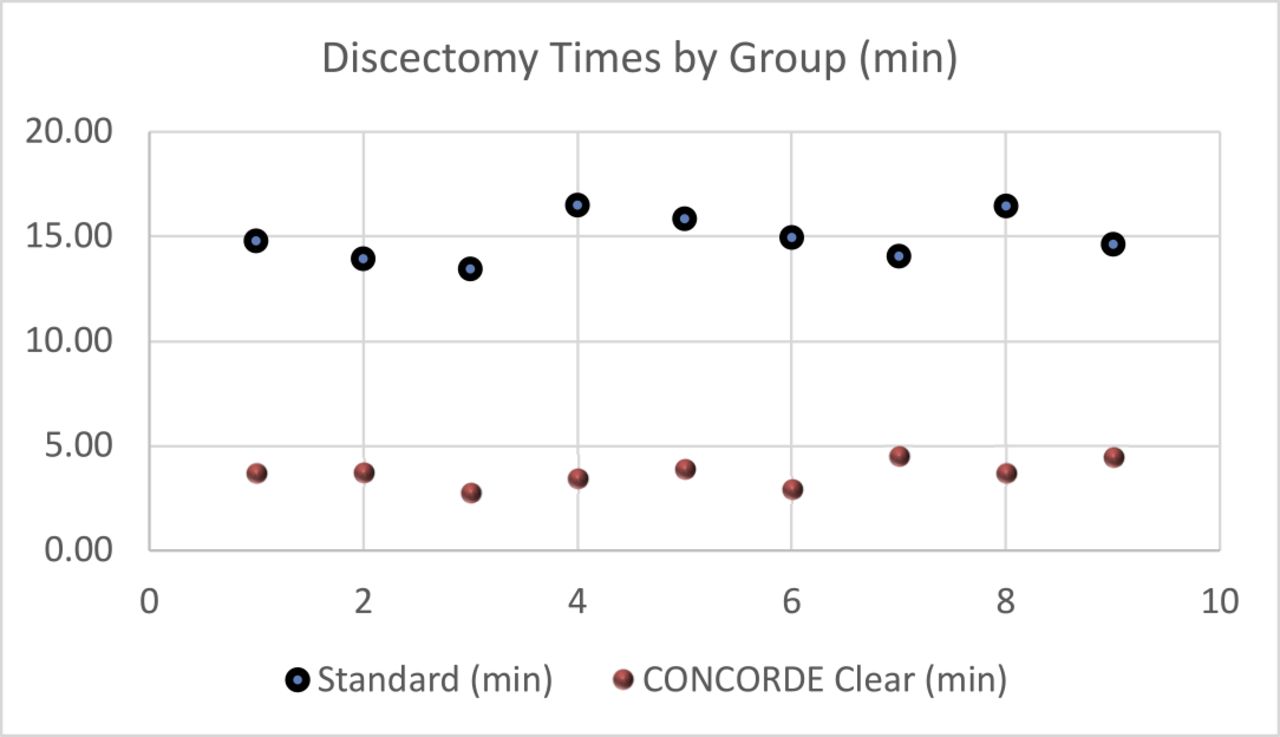
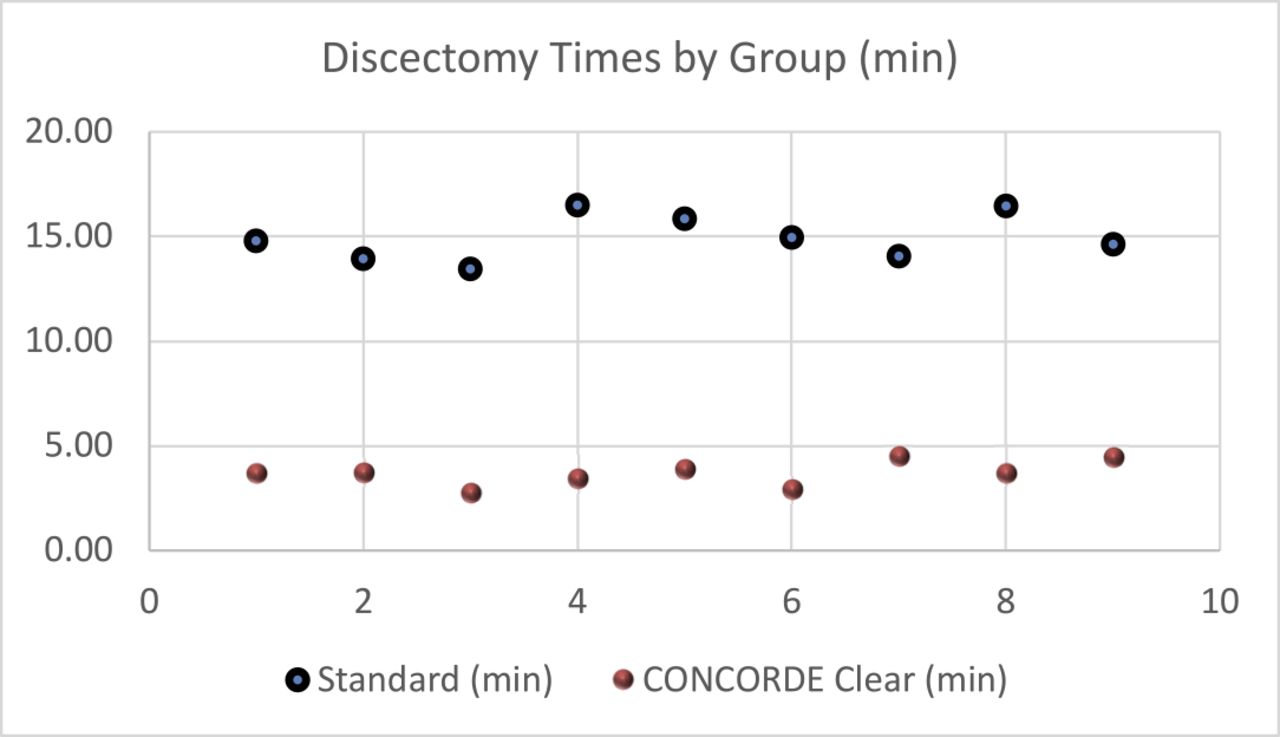
Chart of individual discectomy times (above).
Each surgeon performed 6 levels, using the same specimen for convenience. Collapsed, fused, and levels under 5 mm were excluded. All surgeons were experienced users of the CONCORDE Clear device. All surgeons were instructed to perform a thorough discectomy independent of the instruments used and stopped when they determined the discectomy was complete based on tactile and visual feedback, simulating the preparation of a disc in a live patient. The height of each disc was measured intraoperatively (using shaver or paddle distractor) to allow for retrospective analysis. A total of 18 discectomy levels were performed as there were no exclusions, with 9 in the traditional group, and 9 in the CONCORDE Clear group.
When performing the discectomy, the surgeons were asked to work at a pace that simulates an actual operation. The surgeon used either loops or a microscope, based on preference (and used the same for both groups). Besides discectomy instruments, a nerve root retractor and suction could be used.
For each level in which a discectomy was performed, the following were measured: (1) elapsed time (primary measurement), (2) number of instrument passes, (3) separately the number of instrument exchanges, and (4) estimated wet tissue volume (secondary measurements). Discectomy time was measured from postannulotomy until the surgeon announced the discectomy was complete. Instrument passes were counted, 1 for each time any instrument both entered and exited the surgical access incision site. Instrument exchanges were counted, 1 for each time any discectomy instrument was swapped for another discectomy instrument. Tissue collected for a single level for both the traditional groups (each wiped with gauze) and CONCORDE Clear groups (volume within the Xtool handle or other instrument wiped with gauze) was poured through a large diameter stainless steel filter with a 1 mm pore size to filter out fluid. To remove tissue from each piece of gauze, both manual and saline rinse techniques were used. Any tissue collected in the suction canister during the single-level discectomy was also poured through the filter. Collected tissue was both inspected and palpated for pieces of bone and hydrated with saline. Afterwards, the tissue was placed in a 30 cc syringe and compressed to measure volume (to the closest cc). (Note that the past CONCORDE Clear cadaveric study only measured CONCORDE Clear volume.) All data were recorded on a single datasheet per discectomy level (for either group).
For statistics, the method of comparison were t tests, with the probability of a Type 1 error set at 0.05. The standard error will be reported for all measurement means. Microsoft Excel was used for data analysis.
RESULTS AND ANALYSIS
Primary and secondary measures for each group of discectomy times, instrument passes and exchanges, and wet tissue volume, along with number of disc levels and average disc height, are listed in the table below.
Discectomy summary table by group (above).
As shown in the chart, traditional data points vary approximately 3 minutes, and CONCORDE Clear 2 minutes. The 2 groups have no overlap. Primary analysis: TLIF discectomy times improved on average 11:19 per level (P < .001), which equates to an estimated procedural time savings of 15:51, using 1.4 levels per TLIF, the average number of levels in a large series.1
Direct Economic Benefit
Both time and sterilization efficiency are expected to lead to a direct cost-benefit associated with the use of the CONCORDE Clear device. Related to time, it is difficult to arrive at an established operating room cost per minute. Watkins2 used $93 per minute in “cost savings” in a recent cost-effectiveness spine study. Average operating room fees, without surgeon or anesthesia fees, are an estimated $92 per minute (calculation based on time adjusting a 10-year old figure of $62 per minute,3 which was based on a 100-hospital national study, an increase from $20 in 1991). For the purposes of this analysis, as some sources use lower figures than cited, we use a reduced figure of $80 per minute. A separate direct hospital cost benefit is in reusable tray sterilization, where the average cost to prepare and sterilize a tray is $58.4 As the CONCORDE Clear device(s) becomes the primary discectomy instrument, as opposed to a broad range of discectomy instruments, and only a few added discectomy instruments are used (and added to ancillary tray), this obviates a dedicated discectomy tray. In summary, the direct cost-benefit associated with use of the presterilized, disposable CONCORDE Clear device(s) in a TLIF is an estimated $1300 (15.8 minutes × $80/minute + $58 = $1322).
Secondary Analysis
Usage of the CONCORDE Clear significantly reduced instrument passes compared to traditional, with a mean of 62.0 for traditional versus 7.1 for CONCORDE Clear, an 8.7-fold improvement (P < .001). Instrument exchanges showed a 5.9-fold improvement (P < .001), with means of 26.8 and 4.6, respectively. Wet discectomy tissue volume was measured for each discectomy, with a mean of 5.4 cc for traditional versus 12.9 cc for CONCORDE Clear, a 2.4-fold improvement (P < .001). Additionally, the mean wet tissue volume removal per minute was calculated, which was 0.4 cc/minute and 3.5 cc/minute, respectively, nearly a 10-fold difference (P < .001). Note that, for both groups, inspection and palpation of the excised disc tissues did not reveal any bone.
DISCUSSION
In today's health care environment with multiple constituents involved in health care purchasing decisions, it is important to not only study the clinical benefits of a new technology (previous study comparing traditional discectomy to discectomy with the CONCORDE Clear device), but also the economic benefits. This study estimates that, in a typical TLIF procedure, over 15 minutes should be saved by using the CONCORDE Clear device (a quarter of the time of a traditional discectomy), and by considering the direct cost-benefit associated with this time savings as well as reduced sterilization costs, it is estimated that a hospital would save approximately $1300 in operating room time and sterilization cost with the use of the CONCORDE Clear device in a typical 1-level TLIF procedure. Although the primary benefit associated with the use of the CONCORDE Clear device is a higher quality discectomy, which may lead to a higher rate of fusion, a significant time savings in a spinal procedure equates to an added clinical benefit.
Regarding instrument passes, the traditional discectomy group figure of 62.0 passes is similar to past discectomy technology studies. This figure is higher than the past cadaveric study assessing the CONCORDE Clear for the traditional group, which is believed to be due to efforts to more closely simulate the operating environment, which included loops or microscope, nerve root retractors and occasional suction use, and a safe pace which the surgeon felt matched that of a surgery on a live patient. (The mean traditional discectomy time of 14.96 minutes also seems to indicate the pace of a typical TLIF discectomy in the operating room.) In this study, the CONCORDE Clear group had less instrument passes compared to our previous cadaveric study.
This was likely because all surgeons in this case were experienced with the CONCORDE Clear. Overall, the significant difference in instrument passes and exchanges, over 8- and 5-fold, respectively, further highlights the efficiency gained with the CONCORDE Clear device. Additionally, each surgeon also commented there was less fatigue with the CONCORDE Clear device. Lastly, far fewer instrument passes relates to less risk of nerve root and dural injury, which not only adds to clinical safety, but can save on the costs of potential dural repair (eg, fine suture, dural patch, and fibrin glue) as well as a prolonged hospital stay and bedrest.
Wet discectomy tissue volume represents a new measurement, as it is not reported in the spinal fusion literature. However, 2 things can be fairly determined. One, the wet tissue volume for the CONCORDE Clear group is very similar to the past CONCORDE Clear cadaveric study, which likely means the discectomy was performed with similar thoroughness. Additionally, although the over 2-fold difference in the mean measurement for the CONCORDE Clear versus traditional groups is surprising, it can be interpreted to mean a more complete discectomy was performed using the CONCORDE Clear group, which concurs with the previous CONCORDE Clear study (using photographic analyses of excised discs). However, we do realize that overall disc volumes are not always consistent between cadavers and anatomic levels. Lastly, the calculated difference in wet discectomy tissue volume removal per minute for the 2 discectomy groups of nearly 10-fold highlights the efficiency brought with the CONCORDE Clear device.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2018 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.