


ABSTRACT
Background: Only a few cases of traumatic atlantoaxial fracture-dislocation have been reported, and neglected cases are seldom found because of the fatal nature of this condition.
Methods: We reported a neglected case of Jefferson fracture-dislocation associated with type II displaced odontoid peg fracture which was nonambulatory and myelopathic. A surgical plan involving posterior fossa decompression and laminectomy of the posterior arch of atlas following posterior spinal instrumentation was then conducted.
Results: Patient experienced marked neurologic recovery and was able to stand and walk with assistance during the early postoperative period.
Conclusions: This procedure may be an effective alternative treatment in neglected cases.
- neglected
- Jefferson fracture-dislocation
- odontoid peg fracture
- posterior fossa decompression
- occipitocervical fusion
INTRODUCTION
The presentation of concomitant atlantoaxial fracture dislocation and odontoid peg fracture is rare, with an estimated frequency of less than 2% among upper cervical spine injury cases. The resulting instability further increases the fatal nature of this injury.1 Atlantoaxial fracture-dislocation may cause cervical cord injury and death in the immediate postinjury period or in a delayed fashion.2,3 The survival rate of these cases can only be increased through early diagnosis, immediate immobilization, meticulous monitoring, and early reduction and fixation of the fracture.3
Neglected spinal injuries are frequently encountered in underdeveloped countries for many reasons, such as a patient's belief in medical treatment, poverty, unequal rights in health care access, delay in diagnosis, and inadequate medical facilities, but unfortunately, publised cases are seldom found.4 Such conditions cannot be treated with conventional surgical techniques and require a tailored surgical plan.5 Reports on neglected concomitant atlantoaxial fracture dislocation and odontoid peg fracture are infrequently published, and as such we would like to present our findings and treatment plan for this particular case.
CASE PRESENTATION
History
A 17-year-old male patient presented with neck pain, quadriparesis, and signs of myelopathy during the past 6 months. Bowel and bladder functions remained intact. The patient had a traumatic event when the motorcycle he was riding crashed into a tree. However, he was still able to walk with assistance during the immediate posttraumatic period, with only complaints of slight weakness and numbness at all 4 limbs and with moderate neck pain. He was then brought to a local health care facility but unfortunately refused further treatment and opted to be treated by a local “bone-setter.” The patient's condition soon deteriorated, and he had remained nonambulatory for the past 4 months after receiving numerous nonmedical treatments by a local “bone-setter” and refusing surgical referral by a neurologist who had found the spinal cord compression caused by the cervical fracture after performing magnetic resonance imaging (MRI). The patient was then willingly referred to a spine surgeon after exhausting all nonoperative measures.
Examination
The patient initially presented in our department with a hard collar on for support and was nonambulatory. Physical examination revealed a hump at the occiput region, with a slight torticollic posture of the neck. Neurologic evaluation revealed hypoesthesia at the C3 dermatomal level and below, with a motoric power at left-sided limbs of 3/5 and at right-sided limbs of 2/5 (American Spinal Injury Association [ASIA] Impairment Grade C). There was also spasticity and exaggerated deep tendon reflexes in all extremities. The clinical picture of the patient performing handgrip of the right hand prteoperatively was as depicted in Figure 1.

Clinical picture of maximum handgrip ability of the right hand.
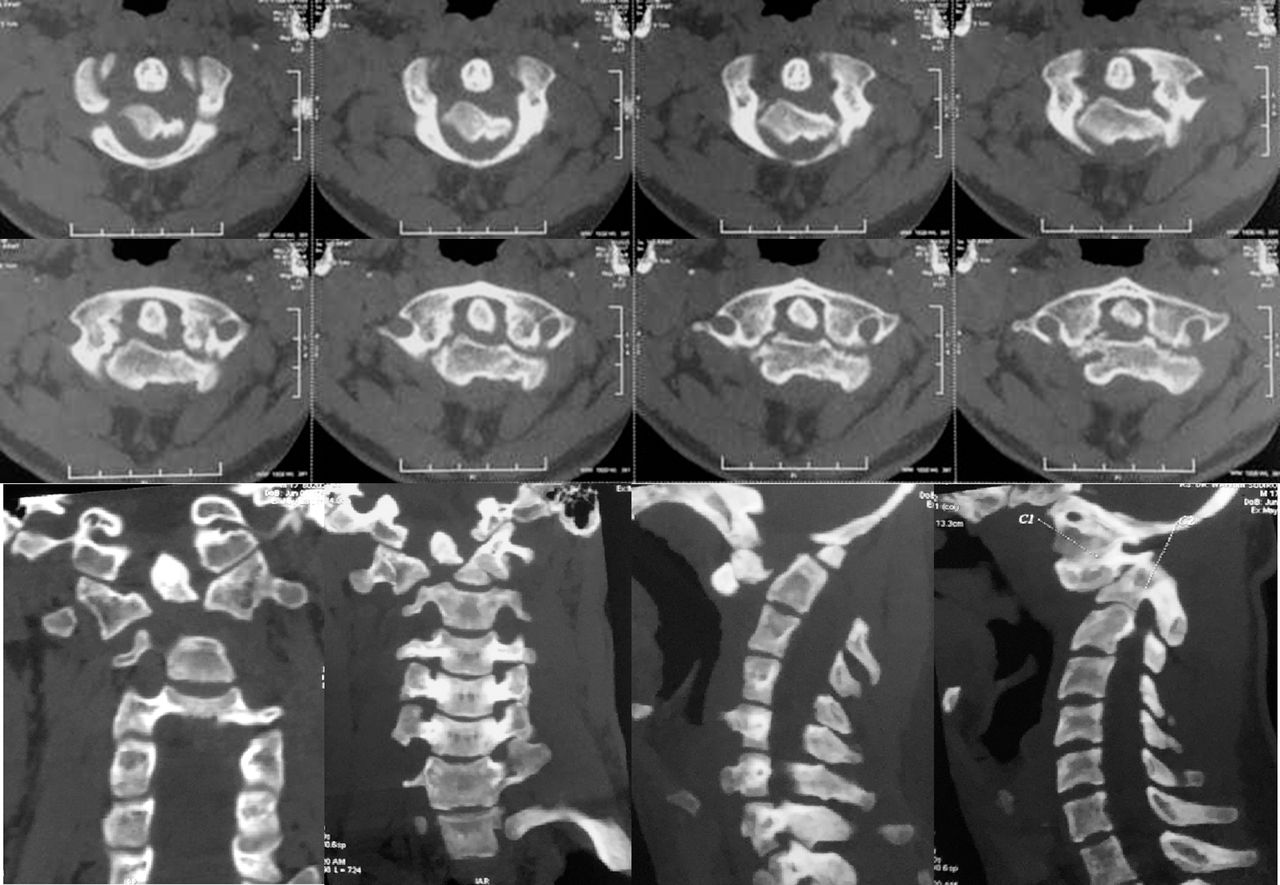
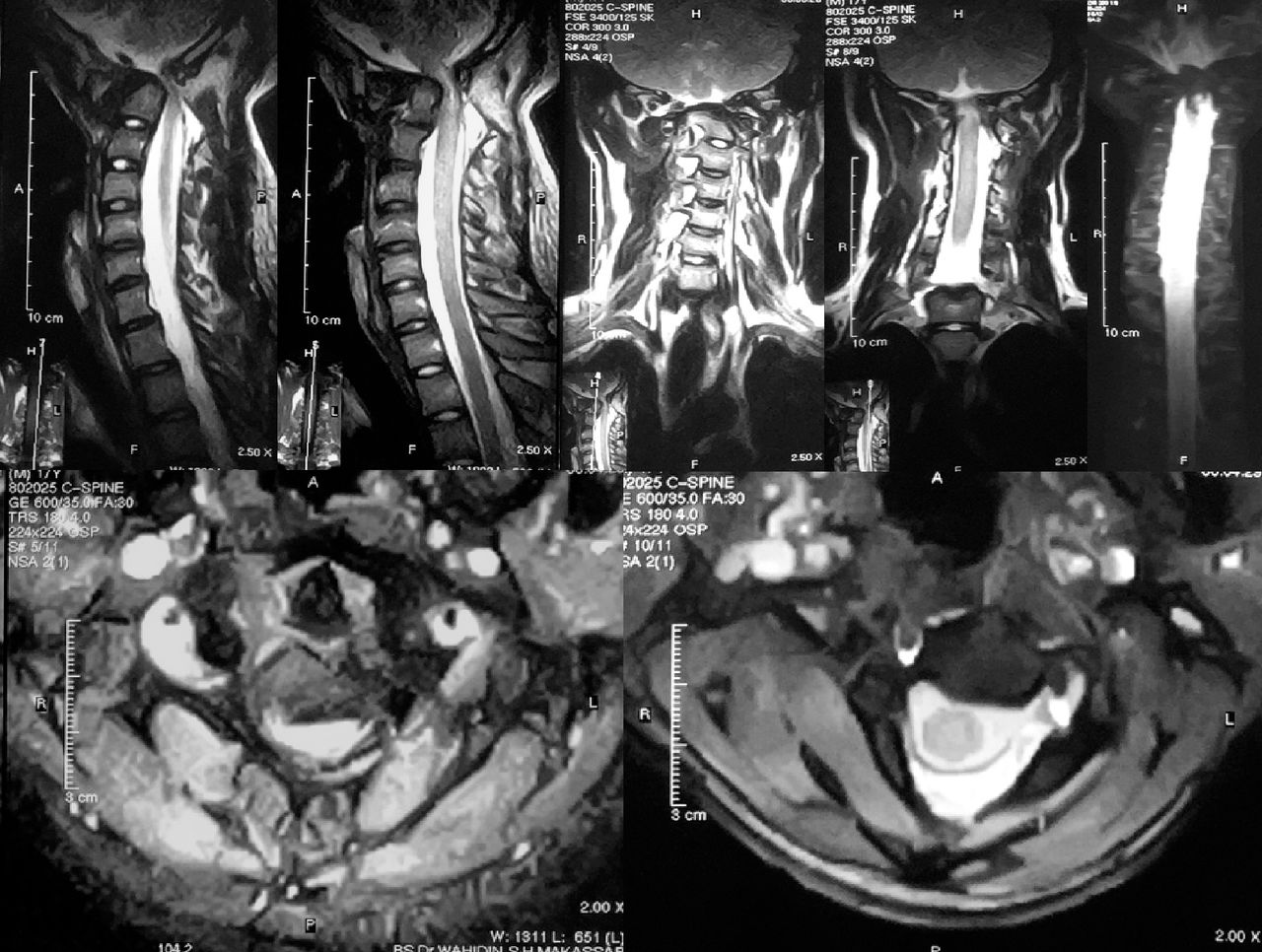
Cervical spine radiographs (Figure 2) and computed tomography (CT) scan (Figure 3) revealed Jefferson fracture-dislocation with anterior subluxation of atlas and odontoid process type II fracture (Anderson and D'Alonzo Classification).6 Overall, this combined injury produced angular flexion deformity of the upper cervical spine. The entire cervical spine showed osteopenia with marked compensatory lordosis. Some callus formation was also evident at the injury site. MRI revealed severe compression of the spinal cord, with myelomalacia at the craniovertebral segment of the cord (Figure 4).

Radiograph of the cervical spine: Antero-posterior, lateral, and open mouth position.
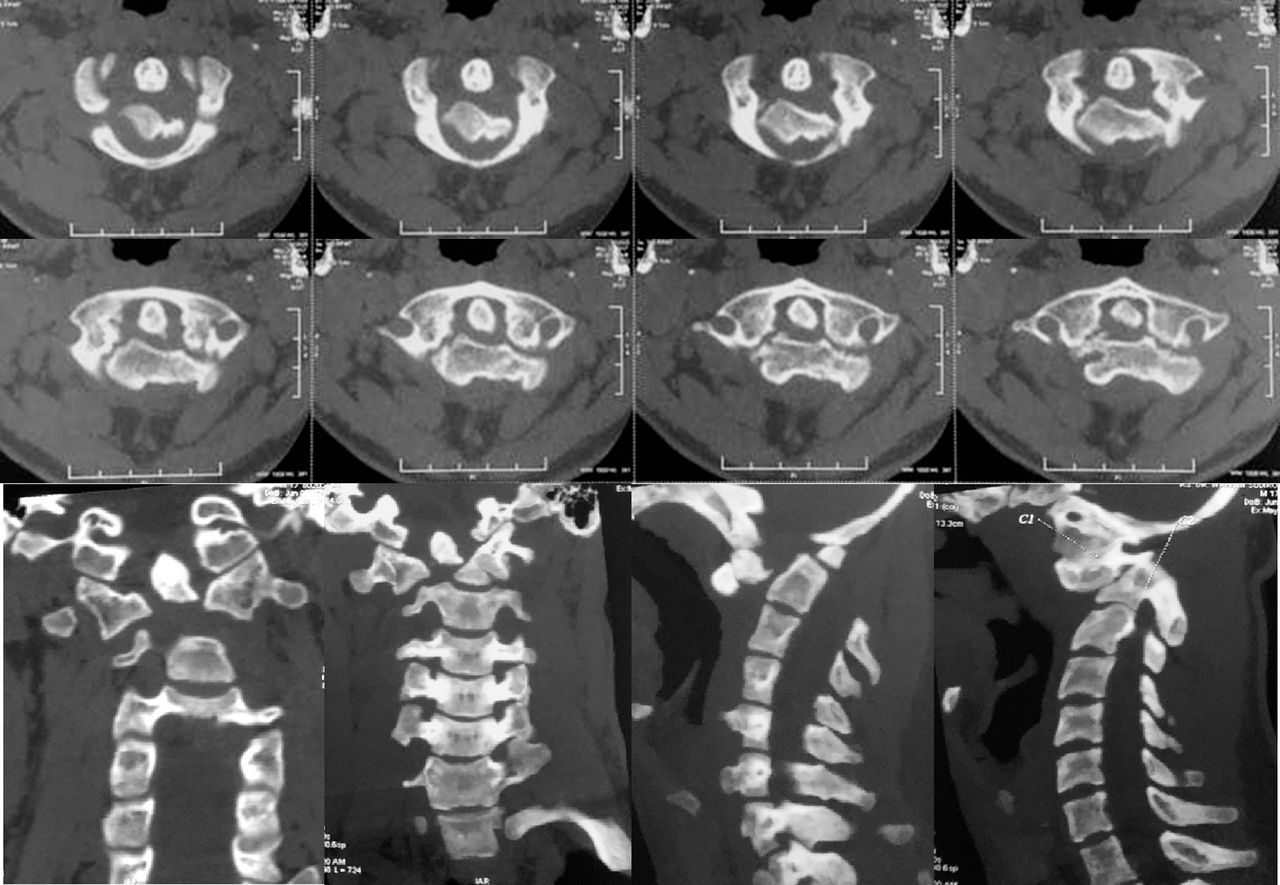
Computed tomography scan of the cervical spine: axial, coronal, and sagittal section.
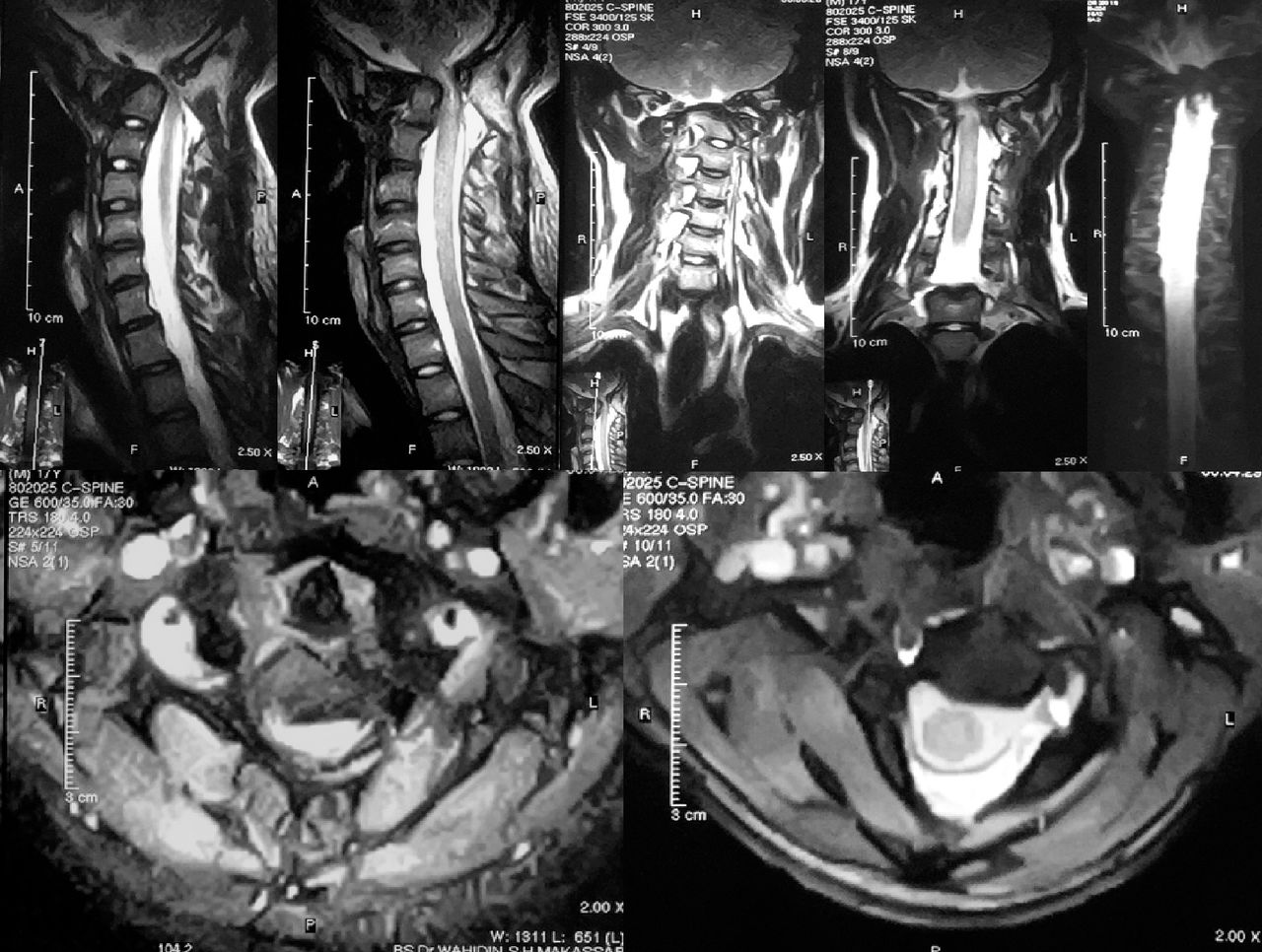
Magnetic resonance imaging of the cervical spine: reduced thickness of cord along with hyperintense signal on T2 in cord at the level C1-vertebra–myelomalacia.
Operative Findings
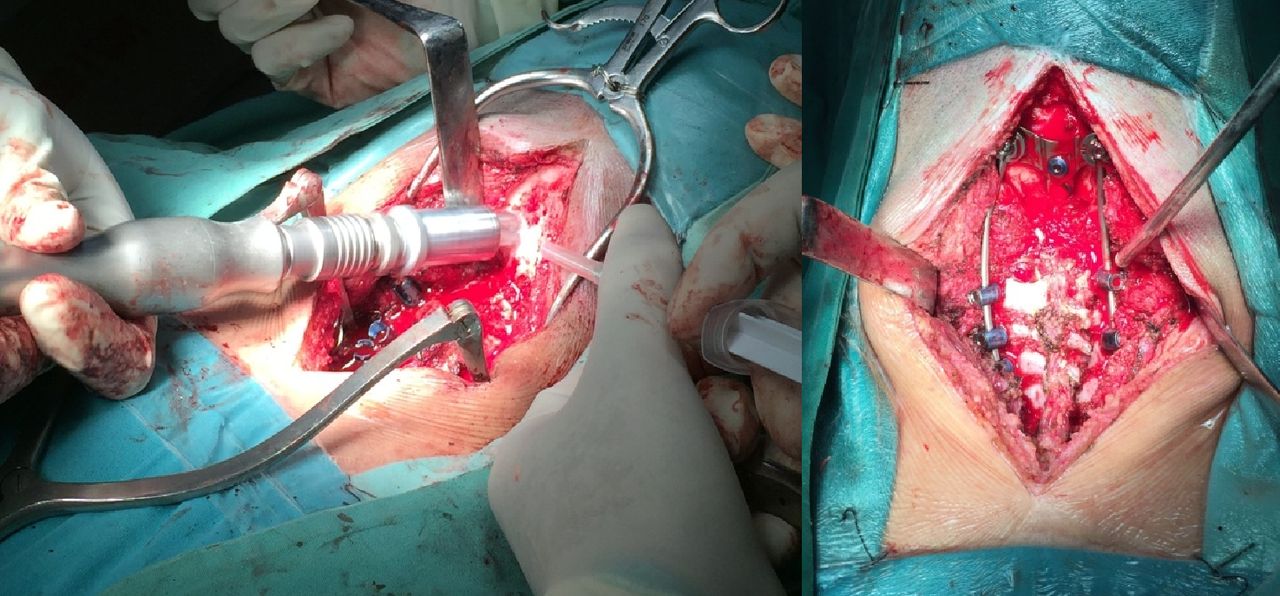
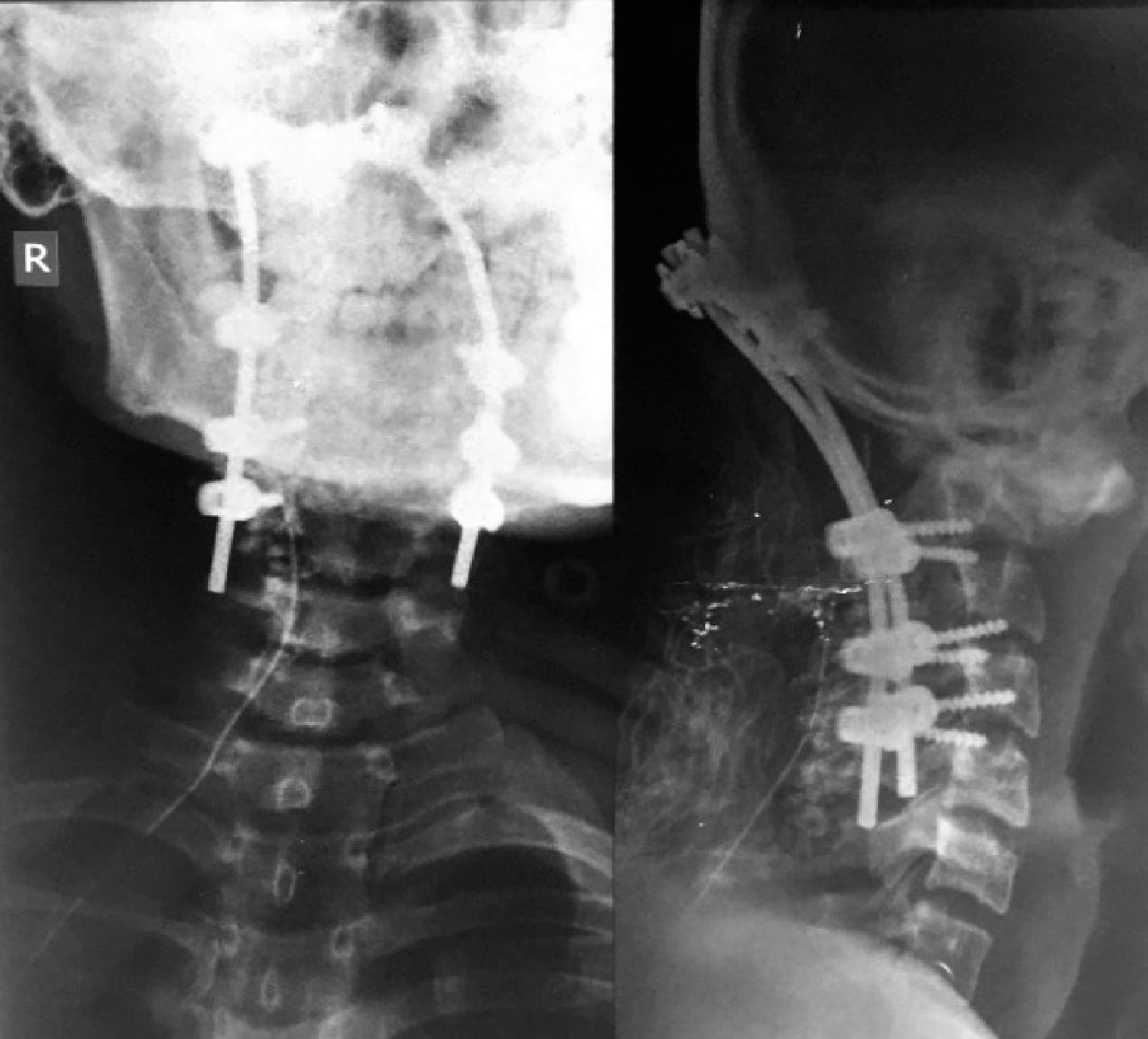
Surgery was performed using a posterior approach, with the midline incision made from the suboccipital area to the spinous process of C5. Posterior spinal instrumentation with occipitocervical fusion to the level of C4 was done using a combination of lateral mass and pedicle screws followed by posterior fossa decompression using a craniotome and laminectomy of C1. The patient was then placed on a Philadelphia collar neck postoperatively. Intraoperative findings are depicted in Figure 5, and postoperative radiograph is shown in Figure 6.

Intraoperative pictures showing suboccipital craniotomy using cranitome (right) followed by occipitocervical fusion and laminectomy of the atlas (left).

Radiograph of cervical spine after occipitocervical fusion.
Postoperative Period
There was progressive neurologic improvement during the early postoperative period. On day 5, the muscle strength of all 4 extremities had improved, especially on the right hand, with a motoric power of 3/5, and on day 10 the patient was able to sit independently and walk with assistance. Patient was discharged at day 14, with uneventful healing of the incision and minimal postoperative pain. At 2 months of follow-up, patient was able to walk and bathe independently, with motoric a power of 4/5 on all the extremities (ASIA Impairment Grade D). The neck range of motion, however, was markedly reduced. The clinical improvements were as depicted in Figure 7.

Ability to perform handgrip by day 5 (top); ability to sit independently with extended knee, and assisted walking (bottom) by day 10.
DISCUSSION
Neglected cases involving both Jefferson fracture-dislocation and odontoid peg fracture are rare. A large retrospective epidemiologic study conducted in 2000 for a period of 14 years revealed that 116 of 784 cases of cervical spinal injuries were upper cervical spinal injuries, and only 2 of them were a combination of these injuries.7 Most cases that are found are lethal, or the patient only survives for few hours,8 although successfully treated cases had also been documented.9 For the past 30 years, only 15 clinical cases have been described, with 7 cases presenting with no neurologic deficits and only 1 case with spastic tetraparesis.10
Odontoid process plays a vital role in maintaining the inherent stability of the C1 to C2 joint. Fracture of this anatomic structure often leads to nonunion or fibrous union due to the poor vascularity of this region because it is enveloped in synovium, or, in certain neglected cases, results in cervical cord compression with instability. Therefore, surgical intervention remains the most viable option in achieving fracture union.3,5 To date, there is still no known consensus for the treatment algorithm of Jefferson fracture-dislocation associated with an odontoid fracture, and thus several authors have employed different management protocol and surgical technique in handling these cases.11
In acute cases, closed reduction of the dislocation can be performed with skull traction followed by halo-vest immobilization. Surgery is only required if closed reduction attempts have failed.11,12 However, the treatment plan for neglected cases needs to be tailored according to several factors, including the patient's age, time lapse from initial injury, preexisting medical morbidity, severity of injury, stability of the C1 to C2 articulation, ease of reduction, and most importantly, the medical facility's capabilities, because these cases are frequently found in underdeveloped countries.13
Fracture reduction in delayed cases is often impossible because several changes have occurred since the initiating injury: (1) the anterior tissues over the craniovertebral area became contracted and shortened, (2) the C1 to C2 kyphotic deformity caused contracture of the muscles of the neck (such as longus colli and longus capitis) along with contracture of the joint capsules and the anterior longitudinal ligaments, and (3) the C1 to C2 articular surfaces gradually became arthritic and bony bridges eventually formed around the dens and body of the axis, further impeding the reduction maneuver.5
Traditionally, this irreducible condition was treated with transoral odontoidectomy followed by posterior fusion. This procedure, however, has the risk of incidental dural insult, which may lead to meningitis.14 Most surgeons preferred posterior fixation following anterior release, although other options, including posterior occipitocervical fusion and posterior transarticular fusion with C1 to C2 pedicle screws fixation, is still possible.5,10
We have opted to use the posterior approach because it has multiple advantages: (1) it allows access to the posterior joint when the dislocation is posterior and allows for screw fixation of C1 to C2, and (2) if intraoperative problems are encountered, occipitocervical fixation remains a viable option. This approach, however, does not provide good exposure of the articular processes, and muscle layers must be detached and reflected laterally, which further increases the risk of venous bleeding.1
Our surgical plan includes posterior fossa decompression and C1 arch laminectomy following posterior spinal instrumentation using a combination of pedicle and lateral mass screws. This management plan, which was usually used in cases of Chiari malformation,15 tumor decompression,16 and atlantoaxial subluxation of a chondroplastic patient with narrow foramen magnum,17 proved to be a good option in managing this particular combination of injury compared with the more complicated ventral procedures.18
With ease of access to the injury site and increased stability with maximum fixation, this operative technique may be a reasonable option in handling complicated neglected cases of combined Jefferson fracture dislocation and odontoid peg fracture.
Footnotes
Disclosures and COI: None of the authors received payments or other benefits or a commitment or agreement to provide such benefits from a commercial entity. No commercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation, educational institution, or other charitable or nonprofit organization with which the authors are affiliated or associated.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.