


ABSTRACT
Background: The study aimed to characterize trends in incidence, etiology, fracture types, surgical procedures, complications, and concurrent injuries associated with traumatic pediatric cervical fracture using a nationwide database.
Methods: The Kids' Inpatient Database (KID) was queried. Trauma cases from 2003 to 2012 were identified, and cervical fracture patients were isolated. Demographics, etiologies, fracture levels, procedures, complications, and concurrent injuries were assessed. The t-tests elucidated significance for continuous variables, and χ2 for categoric values. Logistic regressions identified predictors of spinal cord injury (SCI), surgery, any complication, and mortality. Level of significance was P < .05.
Results: A total of 11 196 fracture patients were isolated (age, 16.63 years; male, 65.7%; white, 65.4%; adolescent, 55.4%). Incidence significantly increased since 2003 (2003 vs 2012, 2.39% vs 3.12%, respectively), as did Charlson Comorbidity Index (CCI; 2003 vs 2012, 0.2012 vs 0.4408, respectively). Most common etiology was motor vehicle accidents (50.5%). Infants and children frequently fractured at C2 (closed: 43.1%, 32.9%); adolescents and young adults frequently fractured at C7 (closed: 23.9%, 26.5%). Upper cervical SCI was less common (5.8%) than lower cervical SCI (10.9%). Lower cervical unspecified-SCI, anterior cord syndrome, and other specified SCIs significantly decreased since 2003. Complications were common (acute respiratory distress syndrome, 7.8%; anemia, 6.7%; shock, 3.0%; and mortality, 4.2%), with bowel complications, cauda equina, anemia, and shock rates significantly increasing since 2003. Concurrent injuries were common (15.2% ribs; 14.4% skull; 7.1% pelvis) and have significantly increased since 2003. Predictors of SCI included sports injury and CCI. Predictors of surgery included falls, sports injuries, CCI, length of stay, and SCI. CCI, SCIs, and concurrent injuries were predictors of any complication and mortality, all (P < .001).
Conclusions: Since 2003, incidence, complications, concurrent injuries, and fusions have increased. CCI, SCI, falls, and sports injuries were significant predictors of surgical intervention. Decreased mortality and SCI rates may indicate improving emergency medical services and management guidelines.
Level of Evidence: III
Clinical Relevance: Clinicians should be aware of increased case complexity in the onset of added perioperative complications and concurrent injuries. Cervical fractures resultant of sports injuries should be scrutinized for concurrent SCIs.
INTRODUCTION
Cervical fracture in pediatric patients is rare but is frequently associated with significant morbidity and mortality. The mortality rate of pediatric patients with cervical spine trauma has been reported in ranges of 16% to 18%, with a higher rate in patients with upper cervical spine injury.1,2 Pediatric patients have been identified to be more susceptible to cervical trauma than adults; up to 80% of pediatric vertebral injuries occur within the cervical spine, whereas cervical injury in adults accounts for only 30% to 40% of spine trauma.3
Recently there has been an increased societal awareness for the prevention of traumatic injuries.4,5 However, despite being a significant traumatic injury, cervical fractures have not been thoroughly studied. A previous study used the Longitudinal Health Insurance Database (LHID 2000) to assess the incidence and risk factors of skull, neck, and trunk fractures in a cohort of ADHD children, with unclear generalizability for a general population.6 The National Electronic Injury Surveillance System, a database that only records consumer product–related injuries, was analyzed to quantify the amount of golf cart–related head and neck injuries in children, a similarly narrow scope.7 Another study attempting to characterize the incidence and characteristics of cervical, thoracic, and lumbar injuries of polytraumatized children uses a level 1 trauma center's database in which only 28 patients were included.8 Understanding the changing epidemiologic patterns in pediatric cervical injury on a larger and more generalizable scale is an important step in local and national efforts of injury prevention.
Our study aims to describe trends and overall rates in the incidence of cervical fractures, and the prevalence of various etiologies, concurrent injuries, complications, and surgical procedures during a 10-year period. Our study also looks to quantify the amount and location of associated spinal cord injuries (SCIs). An analysis of the Healthcare Cost and Utilization Project's Kids' Inpatient Database (KID) inpatient sample was performed for the years of 2003, 2006, 2009, and 2012.
METHODS
Data Source
The Agency for Healthcare Research and Quality's Healthcare Cost and Utilization Project created the KID to make national estimates of health care use, access, charges, quality, and outcomes in a pediatric setting. The KID represents the largest all-payer pediatric (age <21 years at admission) inpatient health care database in the United States. The KID samples various pediatric inpatient procedures from more than 1000 hospitals. The KID does not draw data from every hospital in the United States, resulting in a possible sampling bias that may create a skewed population. Weighted files help compensate for potential bias. The KID contains 107 data elements, including diagnoses and procedures conveyed by the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) format. Released every third year and containing more than 3 million hospital stays per database, year and hospital weights allow accurate calculation of incidences of diagnoses, in-hospital outcomes, and complications. (https://www.hcup-us.ahrq.gov/kidoverview.jsp).
Each institution in this study obtained approval from its local Institutional Review Board, in which this study was deemed exempt because of the deidentified nature of the data.
Inclusion Criteria
The KID was queried for pediatric trauma cases coded in the years 2003, 2006, 2009, and 2012, using ICD-9 External Cause of Injury codes (E-codes). E-codes are secondary codes used to describe external causes of injury and are primarily used for research purposes. Trauma cases isolated used E-codes for various blunt and penetrating trauma types, such as cut/pierce, fall, firearm, machinery, motor vehicle accidents (MVAs), motorcycle, bicycle, pedestrian, pedal cyclist (other), pedestrian (other), miscellaneous transport (other; railcar, snow craft, water craft, airplane, animal-drawn vehicle), assault, and sport. From the trauma cohort, patients with cervical spine fractures were extracted for analysis. Patients with neuromuscular conditions and Down syndrome were excluded from analysis. All ICD-9-CM and E-codes used in this study can be seen in the supplementary material appendix A.
Data Collection/Study Design
Patients were stratified by year of discharge. Patients were then further stratified by age: infantile (ages 0–2 years), child (ages 3–10 years), adolescent (ages 11–18 years), and young adults (ages 19–20 years) based on World Health Organization suggested age groupings (http://archives.who.int/eml/expcom/children/Items/PositionPaperAgeGroups.pdf). Demographics included incidence, mean length of stay (in days), mean Charlson Comorbidity Index (CCI), mean age, mean age of the age stratified groups, and prevalence of sex (male/female), race, and age stratifications. Etiologies were queried using E-codes. Fracture types (closed/open) and cervical spine levels for varying years and age groups, surgical procedures, and surgical procedures for varying fracture levels were queried using ICD-9 codes. SCIs were queried and assessed according to upper (C1-C4) and lower (C5-C7) cervical spine levels. Complications and concurrent injury rates were queried with ICD-9 codes.
Statistical Analysis
Descriptive analyses delineated demographics, incidence, prevalence of trauma types, surgical procedures, fracture types/levels, SCIs, complications, and concurrent injuries. Chi-square analysis determined significant yearly variation of categoric variables, such as sex, race, surgical procedures, fracture levels, SCIs, complications, and concurrent injuries. Student t-tests and 1-way analysis of variance determined significant variation for continuous variables, such as length of stay, CCI, mean age, and mean age of stratified subgroups. Level of significance was set at P < .05. Controlled logistic regression models identified predictors of SCIs, any surgical procedure, any complication, and mortality. Significant predictors were reported after multiple model adjustments. Incidence of traumatic cervical fracture was determined using hospital- and year-adjusted trend weights, and dividing the frequency of cervical fractures by the overall number of trauma cases occurring that year.9 IBM SPSS Statistics version 23.0 (IBM Corp, Armonk, New York) performed all statistical analyses.
RESULTS
Demographics
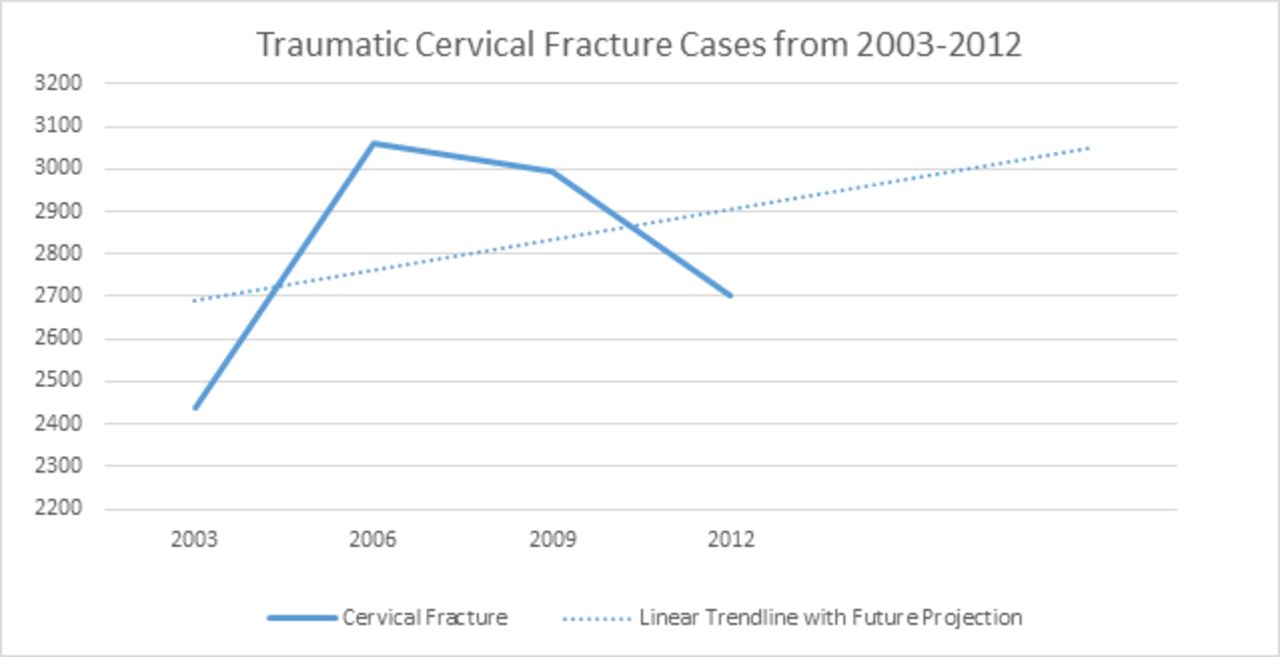
A total of 385 353 pediatric trauma discharges were identified, of which 11 196 were coded as having cervical fractures. The incidence of cervical fracture has increased since 2003 (2003 vs 2012, 2.39% vs 3.12%, respectively; P < .001), with an overall incidence of 2.91% (Figure 1 and Table 1). The overall average age of the cohort was 16.63 years, with a male predominance (65.7%). Average length of stay (LOS) was 8.98 days. There was insignificant yearly variation in age, sex, and LOS. CCI significantly increased since 2003 (2003 vs 2012, 0.2012 vs 0.4408, respectively; P < .001) The most common race was white (65.4%), followed by Hispanic (14.3%) and black (13.3%; P < .05). Adolescents (mean age, 16.26 years) had the highest proportion of cervical fractures (55.39%), followed by young adults (mean age, 19.45 years; 36.14%) and children (mean age, 6.41 years; 5.29%; Table 1).

Traumatic cervical fracture cases from 2003 to 2012. Number of cases is represented along the y-axis. A linear trend line with an extrapolated future projection is plotted alongside cases of traumatic cervical fracture per year.
Demographics of traumatic cervical fractures from 2003 to 2012.a
Prevalence of Trauma Types
MVAs were the most prevalent etiology, with MVAs responsible for 50.5% of cervical trauma, followed by falls (10.1%), and miscellaneous transport vehicles (5.3%; Table 2). MVAs have declined from 52.2% in 2006 to 49.3% in 2012, whereas the prevalence of falls has increased from 9.6% in 2003 to 10.8% in 2012. Sports injuries have increased since 2003 (2003, 3.4%; 2012, 5.5%; P < .001).
Traumatic causes of cervical fracture from 2003 to 2012.a
Fracture Types, Levels, and Surgical Procedures
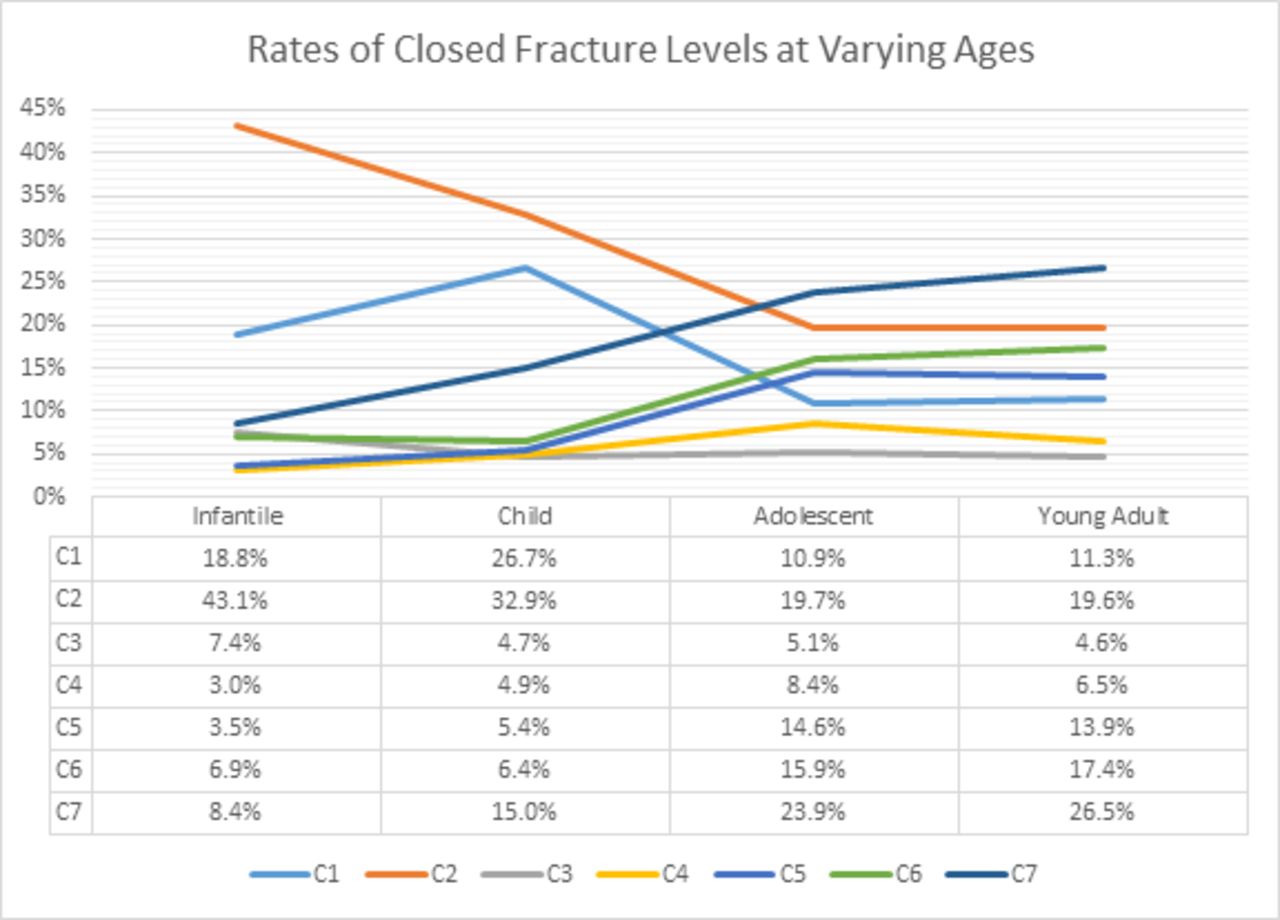
The most common levels of fracture for infants and children, respectively, were closed fractures at C2 (43.2%, 32.9%), followed by C1 (18.8%, 26.7%) and C7 (8.4%, 15.0%). The most common fractures for adolescents and young adults, respectively, were closed fractures at C7 (23.9%, 26.5%), followed by C2 (19.7%, 19.6%) and C6 (15.9%, 17.4%). Closed fractures at all levels were more common than open fractures at all levels. Closed fracture rates at the C1 and C2 levels showed a pronounced decrease in adolescents and young adults (Figure 2).

Rates of closed cervical fracture levels across age groups. Fracture rate trends of varying cervical spine levels are plotted across age groups. Exact rates for each level are shown via the incorporated data table.
Of the entire cervical fracture cohort, closed fractures were most frequent, and they usually occurred at the C2 (20.8%) or C7 (24.1%) level. Open fractures occurred most frequently at C1 (0.47%) and C7 (0.27%) levels (Table 3). Closed fractures at the C6 and C7 levels showed increased prevalence since 2003 (2003 vs 2012, respectively: C6, 13.2% vs 15.7%; C7, 19.9% vs 24.1%). For all closed fracture levels, halo insertions and simple anterior fusions were the most common procedures, usually followed by decompression only or complex posterior fusions (Table 3).
Prevalence of varying fracture levels with most common surgical procedures.a
Overall fusion rates of cervical trauma increased from 5.1% in 2003 to 16.2% in 2012 (P < .001). Halo device insertions decreased from 17.6% in 2003 to 12.4% in 2012 (P < .05). The most common cervical procedure was simple fusions (12.9%), followed by halo insertion (12.4%) and decompressions only (3.1%). Both simple fusions (2003, 2.3%; 2012, 12.9%; P < .001) and complex fusion rates (2003, 1.4%; 2012, 4.7%; P < .001) increased over time, whereas decompression only rates decreased (2003, 9.7%; 2012, 1.1%; P < .001; Table 4).
Rates of varying surgical procedures from 2003 to 2012.a
Prevalence of SCIs Within the Cervical Fracture Cohort
Upper cervical SCI was less common (upper, 5.8%; lower, 10.9%). Unspecified SCI was the most prevalent type of cord injury, particularly in the lower cervical spine (C5-C7, 4.0%; C1-C4, 2.3%). Unspecified SCIs at the lower C5-C7 levels have decreased in prevalence since 2003 (2003, 5.4%; 2012, 3.8%; P < .001). Complete lesions to the spinal cord were the second most common SCI, which occurred at 3.0% of lower-level (C5-C7) fractures and in 1.6% of upper-level (C1-C4) fractures. Unspecified SCIs and anterior cord syndrome rates at lower cervical levels have decreased since 2003 (P < .05). Other SCIs have increased in prevalence at lower C5-C7 levels since 2003 (2003, 3.2%; 2012, 3.5%; Table 5).
Spinal cord injury types and rates.a
In-Hospital Outcomes
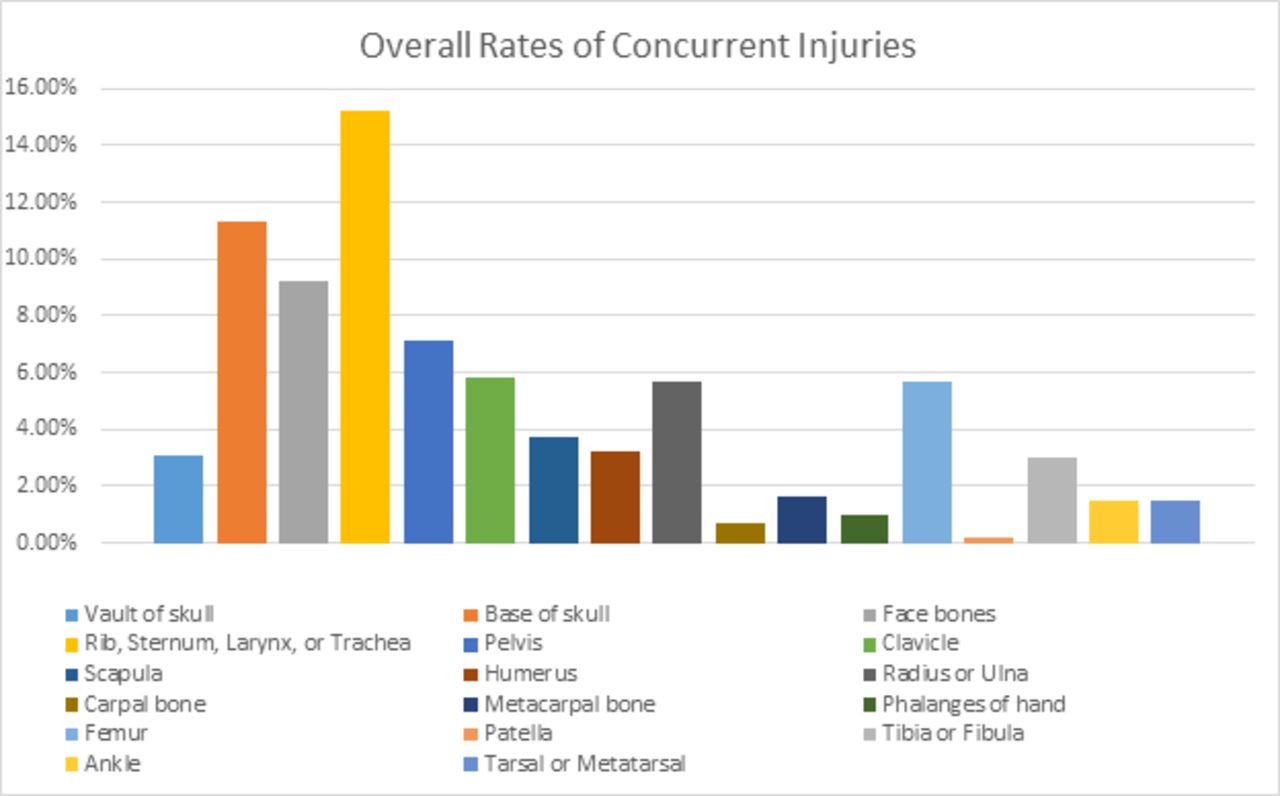
Overall mortality rate was 4.2%. The most common complications were acute respiratory distress syndrome (7.8%), anemia (6.7%), bowel complications (3.8%), shock (3.0%), quadriplegia (2.3%), and bladder complications (1.5%). Bowel complications, cauda equine, anemia, and shock rates all increased since 2003 (P < .001). Dysphagia and pulmonary complications have decreased since 2003 (P < .001; Figure 3 and Table 6).
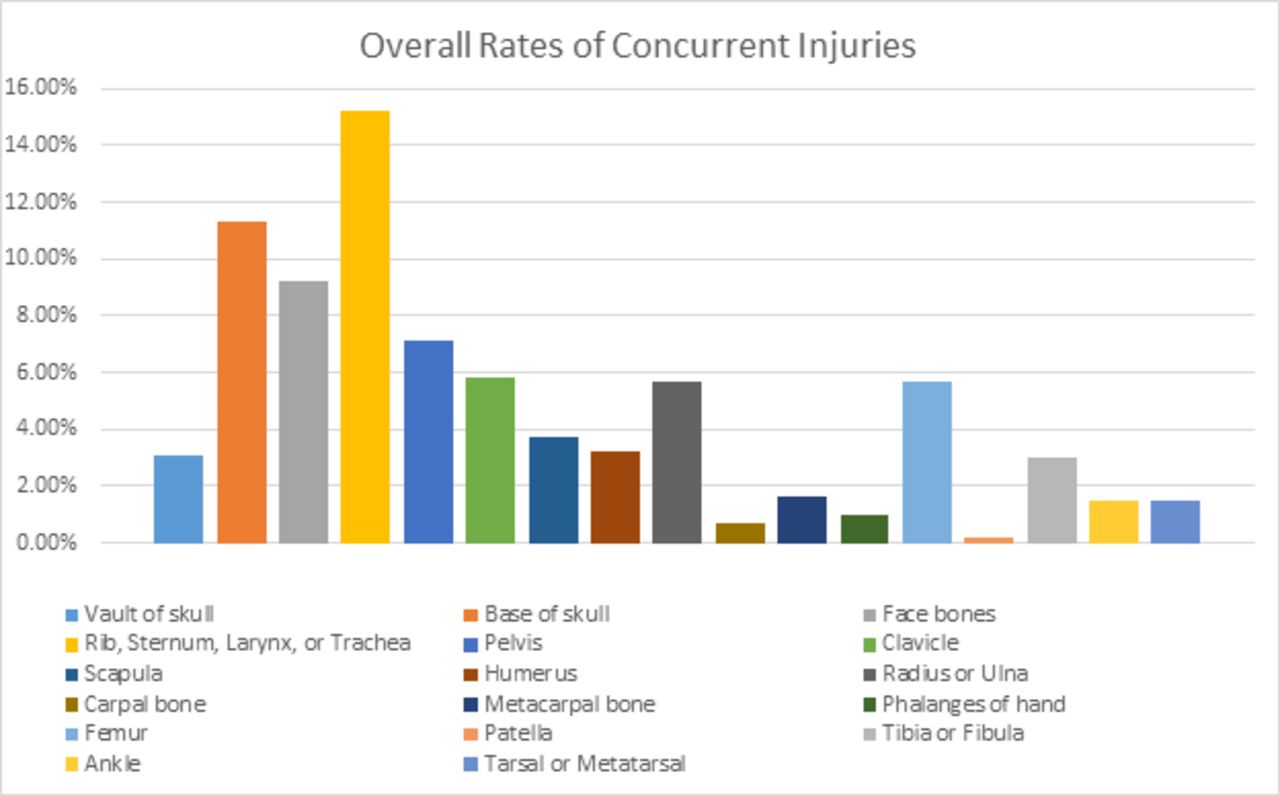
Overall rates of concurrent injuries. Represents percentage of patients for each x-axis concurrent injury, in relation to total cervical spine fracture cases.
Inpatient complications.
In addition to cervical fracture, concurrent fractures of the ribs, sternum, larynx, and trachea were highest in prevalence (15.2%), followed by fracture to the base of the skull (11.3%), the face (9.2%), and the pelvis (7.1%). Fractures at the base of the skull, in facial bones, of the rib/sternum/larynx/trachea, of the scapula, humerus, metacarpal bone, and tibia/fibula have all increased since 2003 (P < .001; Table 7).
Concurrent injury rates.a
Regression Analysis
Significant positive predictors of SCI were determined to be sports trauma (odds ratio [OR], 2.642), CCI (OR, 2.863), and black racial status (OR, 1.448). Significant positive predictors of any surgical procedure were fall traumas (OR, 1.417), sports trauma (OR, 2.259), CCI (OR, 1.116), LOS (OR, 1.024), and SCI (OR, 4.565). Significant positive predictors of any complication were CCI (OR, 4.796), LOS (OR, 1.024), SCI (OR, 4.565), fractures to the base of the skull (OR, 2.039), rib/sternum/larynx/trachea (OR, 1.276), and pelvis (OR, 1.714). Significant positive predictors of mortality were being an infant (OR, 4.561), motorcycle trauma (OR, 1.912), pedestrian accidents (OR, 1.266), CCI (OR, 1.453), SCI (OR, 5.228), fracture to the base of the skull (OR, 4.459), rib/sternum/larynx/trachea (OR, 1.366), and pelvis (OR, 2.799; Table 8).
Significant predictors of spinal cord injury (SCI), surgery, any complication, and mortality.a
DISCUSSION
Among all isolated trauma cases, this study reports a 2.39% incidence of cervical fracture in 2003, which increased to 3.08% in 2006 and has since plateaued. Patients on average were 16.6 years old, and they were more likely to be white male adolescents. Mortality rate and LOS have remained stable over time, whereas CCI has increased since 2003. MVAs have remained the most common cause of trauma, whereas the prevalence of falls, sports injuries, and pedestrian injuries have all increased since 2003. Infants displayed extraordinarily high rates of closed C2 level fractures, and children displayed markedly high rates of closed C1 fractures, both of which declined with increasing age and were surpassed by C7 fracture rates. Of the entire cohort, closed fractures at the C2 and C7 levels were the most common types of fractures. Simple cervical fusions and halo insertions were typically the most common procedures performed at varying fracture levels. Since 2003, overall halo rates have decreased, whereas fusion rates, complications, and concurrent injuries have all increased. SCIs, most prevalent as unspecified injury or complete lesion, have typically remained stable in upper cervical levels, and have decreased at lower cervical levels.
The KID inpatient sample was also used by Shin et al10 to analyze cases of traumatic pediatric cervical spine injuries (nonfracture, fracture, SCI without radiographic abnormality, and dislocation). Although this study has a design similar to ours, our study focuses solely on traumatic fractures of the cervical spine and is mainly stratified by year of discharge. Shin et al10 stratify all of their data by varying age groups. The authors also do not study concurrent injuries, surgical procedure data, complications, or in-depth details regarding SCIs. Shin et al10 determined the incidence of traumatic cervical spine injuries to be 2.07%, the average age to be 15.86 years, the total percentage of females to be 33.15%, and overall mortality rate to be 4.87%. These results are consistent with our calculated 2.9% for traumatic cervical spine fractures, mean age of 16.63 years, female prevalence of 34.3%, and overall mortality rate of 4.2%. The consistency of our results strengthens our methodology and study design. The slight variations between the results from Shin et al10 and our study are likely due to differences in inclusion criteria.
Shin et al10 also report approximately 80% of total pediatric cervical spine injuries occurring in adolescents and young adults, with a higher prevalence of cervical fracture and lower-level cervical spine injury (C5-C7) in adolescents and young adults. This is consistent with our reported 91.53% of traumatic cervical fractures occurring in adolescents and young adults, as well as our trends showing higher rates of lower cervical fracture (C5-C7) in adolescents and young adults. Traffic accidents were reported as the most frequent cause of cervical spine injury (57.51%), followed by falls and sports injuries. This supports our findings of traffic accidents (MVA + motorcycle) accounting for 53.6% of cervical spine fractures, followed by pedestrian accidents, falls, and sports injuries. Shin et al10 reported a 3.84-day average LOS, which is palpably lower than our reported 8.98-day average LOS. This is also most likely due to differences in inclusion criteria. Shin et al10 include nonfracture, SCI without radiographic abnormality, and dislocation, which could result in a reduced average LOS by nature of the injury.
Patel et al11 conducted a similar study looking at the National Pediatric Trauma Registry, a database of 75 172 injured children, during a consecutive 10-year period from 1988 to 1998, another of the few large database studies for pediatric cervical spine injuries.12 This study identified 1098 discharges with cervical spine injury, reporting an overall incidence of 1.5%, similar to the findings of Shin et al10 and our study. The most common reported etiology was MVAs at 61%, with 14% of those injuries as pedestrians, followed by falls and sports injuries as the second and third most common injuries, respectively. These findings also support our reported MVA rates, followed by pedestrians, falls, and sports injuries.
Patel et al11 reported that upper spine injuries were nearly twice as frequent as lower spine injuries (C1-C4, 52%; C5-C7, 28%), with fractures of the upper cervical spine more frequent in comparison with the lower cervical spine (302 vs 210 pediatric patients). The findings from our study, as well as the findings from Shin et al,10 contradict this report. Our findings show a substantial overall increased rate of lower-level (C5-C7) cervical spine fractures (54.1%) in comparison with upper-level (C1-C4) cervical spine fractures (45.3%). This is most likely attributable to our larger study population, resulting in a higher proportion of adolescents and young adults with cervical spine fracture. Although Patel et al11 do note an increased prevalence of lower cervical spine injuries in older children (age ≥8 years, 85%), the study lacks the required power to give an accurate representation of the proportion of traumatic injuries occurring in adolescents and adults in comparison with infants and children. This can also explain the reported overall mortality rate of 17.0% by Patel et al,11 in that younger children are described by Patel et al11 and Shin et al10 as having a much higher mortality rate in comparison with adolescents and adults. Younger children are most likely prone to upper cervical spine injuries, simply as a function of developmental anatomy. The proportionately larger heads of infants and children, combined with increased ligament laxity and practically horizontal facet joints in the upper cervical vertebrae, result in high torques and shear forces applied to upper cervical spine levels, specifically C1 and C2.13–16
Regarding management for pediatric cervical trauma patients, approximately 25% to 30% of cervical spine injuries require surgery.17,18 The goal of surgery is to improve the stability of the vertebral column and protect the spinal cord, while limiting risks, repeated procedures, and morbidity.19 It is important to consider the growth potential of the pediatric spine and perform an assessment of whether the size of the spine is adequate to accept hardware.19 Eleraky et al17 conducted a study of 102 pediatric patients who had experienced cervical trauma and reported that 30% of the patients were treated surgically. Of those patients, 18% were treated with an anterior cervical approach and 12% underwent a posterior fusion. This is similar to our reported findings of the anterior approach generally being used more in comparison with the posterior approach.
Given that trauma patients who die before entering the hospital are not included in the KID, and the decline of trauma cases since 2003, the increased incidence of cervical fractures witnessed in our data set may be a result of improved emergency medical services, management, and treatment strategies. Our finding that various concurrent injuries and complications have increased since 2003 would help support the claim that more patients with traumatic cervical fractures, in relatively worse condition, are generally making it to the hospital alive. In earlier years with potentially worse emergency medical services and injury management strategies, only patients in generally better condition would have made it to the hospital alive and been included in the KID. The steady annual rates of upper cervical SCI and decreasing rates of lower cervical SCI shown by our data also may support the idea of improving emergency spine stabilization strategies.
Assessment of potential spine injuries is considered controversial, with insufficient evidence to support diagnostic standards, treatment standards, and guidelines.20,21 Lee et al22 in 2003 attempted to address the issue of assessing and managing cervical trauma in children. Strict guidelines were created and used for cervical spine injury identification, immobilization, and clearance criteria. The study found that a multidisciplinary team with standards for spine immobilization, assessment, and morbidity/concurrent injury recognition had decreased the average time to patient clearance. Further research is needed to gauge the epidemiologic impact of bolstered emergency medical services and standardized management/treatment guidelines on traumatic cervical fractures.
LIMITATION
The KID gives rise to this study's principal limitations. The information coded in the database is limited by the accuracy of the coders. Moreover, the database is an inpatient database, lacking longitudinal value (follow-up reports, long-term outcomes) and limiting our ability to strengthen associations between variables. The use of ICD-9-CM coding itself is a limitation. Codes are subject to change over time, and we can only determine that patients were coded for a specific injury or complication during their hospital stay, lacking temporal aspects warranted for causation. Determining the true incidence of the traumatic pediatric cervical fracture is limited because incidence is dependent upon individuals of a healthy population (persons at risk for injury). The KID only contains hospital admissions, excluding the vast majority of the at-risk population, as well as patients who died before entering the hospital. Furthermore, the database lacks specificity regarding complex cases and procedures, such as surgical indications or disease severity, which would further understanding of concurrent injury and operative data.
CONCLUSION
This study characterizes the etiologies and epidemiology of traumatic pediatric cervical spine fractures. The incidence of traumatic cervical fracture has increased since 2003. Patient case complexity has increased in the onset of higher comorbidity, complication, and concurrent injury rates. Fusion procedures seem to increasingly be the top compensatory surgical treatment, with CCI, SCI, falls, and sports injuries being significant predictors of surgical intervention. Future trends of traumatic pediatric cervical fractures should be monitored in order to gain a better understanding of improving emergency medical services' and management strategies' influence on epidemiologic trends.
Footnotes
Disclosures and COI: Dr Gerling received personal consulting fees for Paradigm Spine and speaking/teaching fees for Stryker Spine. Dr Passias received personal consulting fees for Spinewave and Medicrea. The other authors received no funding for this study and report no conflicts of interest.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}