


Abstract
Background Cervical myelopathy caused by pseudarthroses is rare, with the exact pathophysiology of its occurrence unclear and reports scarce. To the best of our knowledge, only a few cases have been reported so far. We present a case of cervical myelopathy secondary to bilateral pseudoarticulations in rheumatoid arthritis and discuss possible pathomechanisms with reference to previously published reports.
Case Presentation A 61-year-old woman with rheumatoid arthritis and previous C1 to C2 laminectomy suffered from cervical myelopathy. On preoperative imaging as well as surgical exploration, large osteophytes from bilateral pseudoarticulations between the posterior arches of the atlas and axis were seen to be causing severe compression of the spinal cord.
Case Management Posterior instrumented C1 to C2 fusion with patient-specific pedicle screws and surgical planning was performed. The patient had significant clinical improvement after fusion.
Conclusions Ligamentous laxity in rheumatoid arthritis can lead to the development of pseudoarticulations, with dynamic forces of neck motion causing osteophytic bony spurs and cord compression. Posterior decompression and fusion was effective in this case of bilateral pseudoarticulations, which produced a posterolateral or “lateral recess” pattern of cord compression refractory to previous central decompression alone.
Level of Evidence 5.
Introduction
Pseudoarticulations refer to a “false joint” of the spine and were first reported by Baastrup in 1933 to involve spinous processes of lumbar vertebrae.1 Pseudoarticulations of the cervical spine, however, are rare, with few reported cases.2,3 These anatomical anomalies do not typically cause cervical myelopathy with few reported cases in the literature in congenital states4–7 such as Klippel-Feil syndrome,8 malignancies such as osteochondroma,9 and degenerative states such as diffuse idiopathic skeletal hyperostosis.10 We report a rare case of bilateral posterolateral atlantoaxial pseudoarticulations in rheumatoid arthritis.
Case Report
A 61-year-old woman with rheumatoid disease presented with a 4-month history of worsening cervicogenic headaches associated with bilateral upper limb paresthesia, distal sensory loss, and loss of hand dexterity. Over this time, her gait had become unsteady with worsening balance (Nurick grades 3–4). On questioning, the patient admitted to occasional Lhermitte’s phenomenon and intermittent incontinence. In the years leading up to her presentation, she had failed trials of physiotherapy, periradicular injections, nonsteroidal anti-inflammatory agents, and neuropathic analgesics.
She had undergone a C1 laminectomy more than 10 years prior to the current presentation for cord compression, for which she had initially experienced marked improvements in myelopathy. Her rheumatoid arthritis was well controlled with disease-modifying antirheumatoid drugs (methotrexate) as well as monoclonal antibody therapy (abatacept weekly injections). Her other medical history included osteoporosis, type 2 diabetes mellitus, hypercholesterolemia, nonalcoholic fatty liver disease, hypertension, and hypercholesterolemia.
Examination showed upper limb weakness including 4/5 hand intrinsics with bilaterally positive Hoffman’s sign as well as slowed hand clap. Lower limb power was also reduced, particularly right hip flexion (4/5) with slowed foot clap. Her gait showed positive tandem ataxia with reflexes that were generally brisk (3+). Magnetic resonance imaging showed C1/C2 canal stenosis with progressive T2 signal cord changes, which were present posteriorly and extending 9 mm in length (Figure 1). The anteroposterior canal diameter was reduced to 5 mm. There was also cord atrophy with posterior bow stringing due to bony spurring from bilateral pseudoarticulations (Figure 2). There was no dynamic instability on flexion and extension films.

Preoperative magnetic resonance imaging sequences of the patient’s cervical spine demonstrating cervical myelopathy due to posterolateral cord compression related to bilateral pseudoarticulations. (A) T2-weighted sagittal view. (B) T2-weighted axial view.

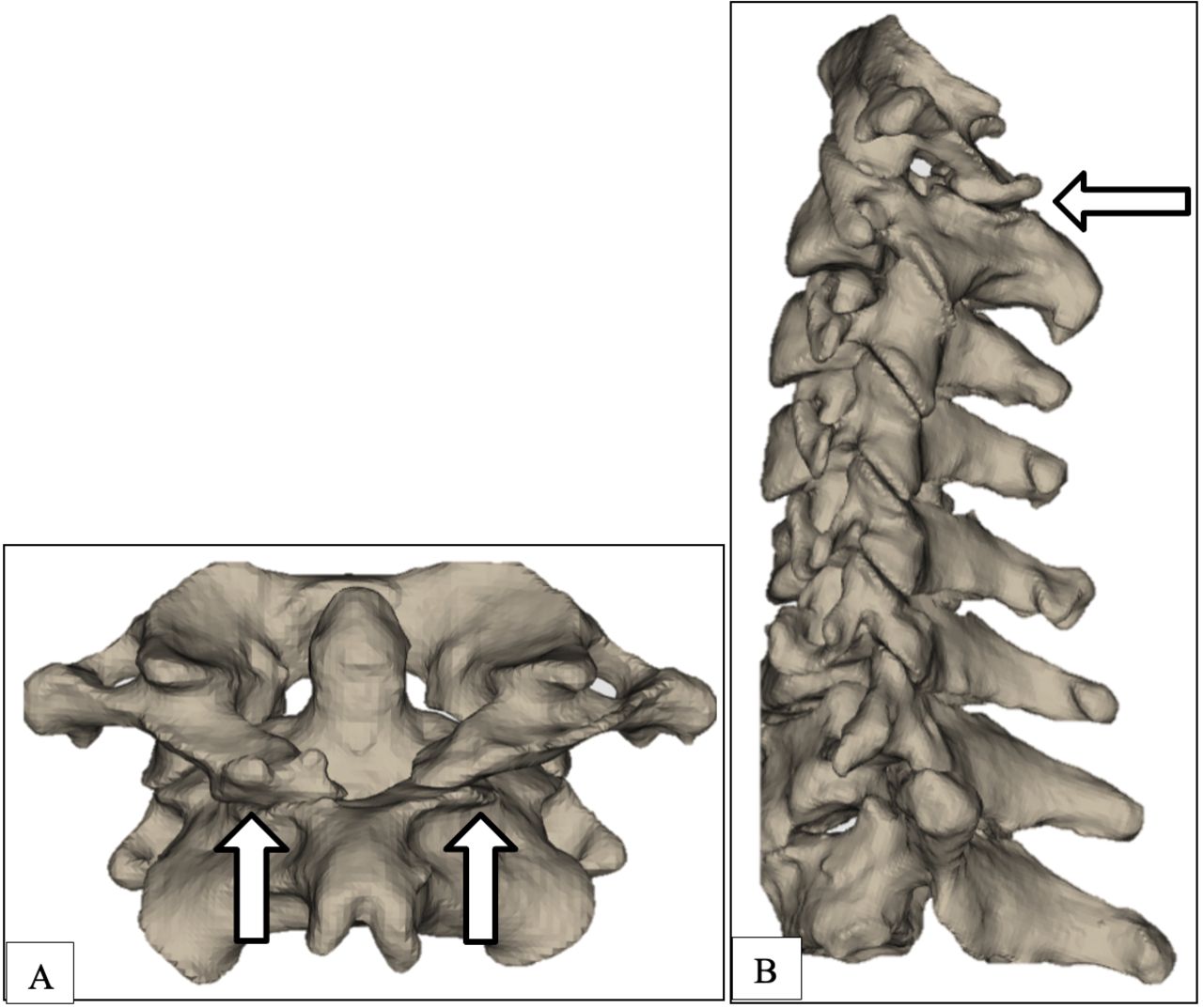
Preoperative 3-dimensional reconstruction computed tomography (CT) images demonstrating bilateral pseudoarticulations (white arrows). (A) CT dorsal view of C1 to C2 vertebrae. (B) Sagittal view of C1 to C7 vertebra. Images reproduced with permission from Medacta Australia.
Following surgical planning, the decision was made for direct decompression by resection of these pseudoarticulations medially until the lateral turn of the thecal sac, followed by C1 to C2 fusion. Following a midline craniocervical incision, a subperiosteal dissection was performed in the midline avascular plane from occiput to C2 to allow visualization of these pseudoarticulations (Figure 3). The C1/C2 posterior pseudoarticulation was drilled bilaterally with dissection above the C2 nerve root to expose lateral masses. Three-dimensional–printed patient-specific guides (MySpine, Medacta International, Strada Regina 6874 Castel San Pietro, Switzerland) were fitted prior to insertion of C2 pedicle screws (Medacta M.U.S.T Mini Posterior Cervical Screw System) with pilot holes (16 mm on left and 18 mm on right). Entry points were also drilled onto the undersides of the lateral masses to allow insertion of C1 screws (2 × 30 mm). Fixation rods were sited and secured with set screws and bone grafts were applied to posterolateral gutters.

(A) Intraoperative findings of bilateral C2 pseudoarticulations with occiput superiorly (star) and C2 spinous process inferiorly (blue arrow). (B) Close-up view demonstrating the presence of synovial membranes as well as synovial fluid adjacent to inferior and superior pseudoarticulations bilaterally (green triangle). The majority of the C1 posterior arch was removed in previous laminectomy surgery.
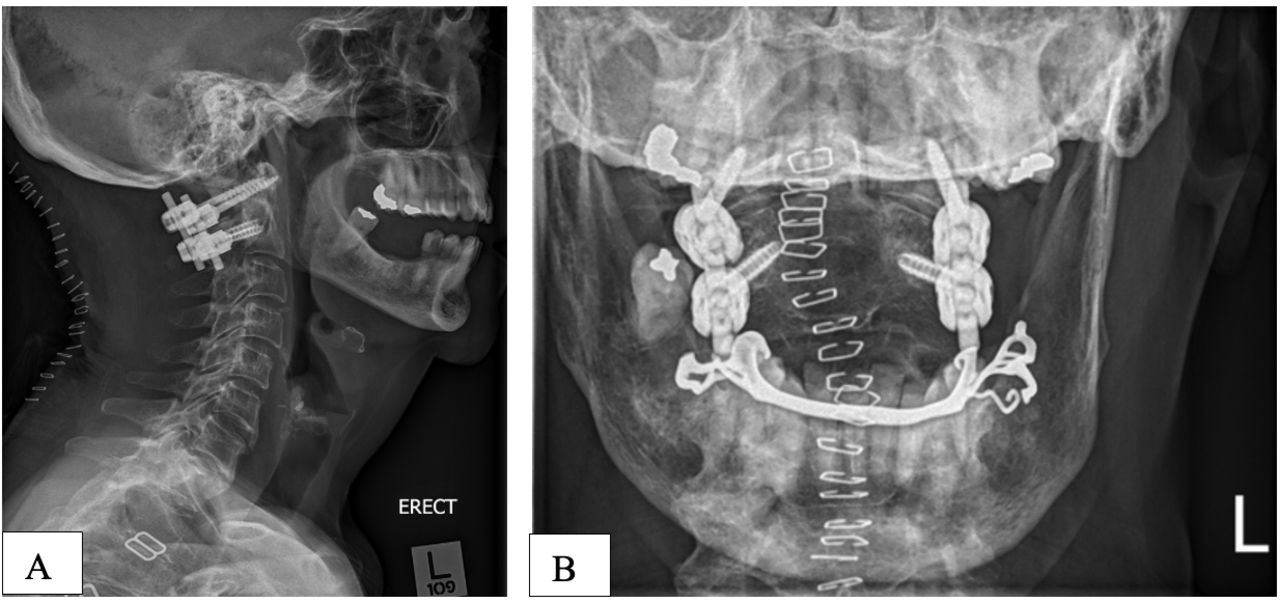
Following surgery, our patient had an uneventful recovery with adequate fixation at 1-week postoperative erect x-rays imaging (Figure 4). Six-week follow-up computed tomography imaging showed stable posterior fixation with normal alignment. At 6-month follow-up, there was complete clinical resolution of neurological symptoms with maturing fusion on computed tomography.

Day 7 postoperative erect x-ray images. (A) Lateral erect view. (B) Odontoid view.
Discussion
Atlantoaxial pseudoarticulations were previously reported by Viallet et al2 and Kremser et al11 in the 1950s, describing a cervical localization of Baastrup disease of the lumbar spine, in which spinous processes contact each other closely.1 However, there are few reports of these cervical myelopathy due to pseudoarticulations in the cervical spine. There have been reports of at least 2 patients with diffuse idiopathic skeletal hyperostosis in which osteophytes were formed at the C1/C2 pseudoarticulation site causing cervical myelopathy.10 There has also been a report of progressive myelopathy due to pseudoarticulations between an osteochondroma of the atlas and lamina of the axis.9 Other reports of C1/C2 pseudoarticulations in the second,5 third,6 and fourth4,7 decades of life have implicated underlying genetic aberrations and abnormal segmentation of the cervical sclerotomes. These pseudoarticulations may therefore be associated with Klippel-Feil syndrome where there is a complete failure of segmentation in the embryological period and fusion of 2 or more cervical vertebrae. These may develop with or without key elements of a true joint such as smooth articular cartilage, synovial capsule, or synovial membrane.
Presentation in the sixth decade of life in our patient suggests a likely degenerative etiology secondary to rheumatoid arthritis. A “true joint” allows smooth articulation between opposing skeletal elements and transmits biomechanical loads through the structure. This is achieved by the articular cartilage, the lubricating action of synovial fluid, and capsular ligaments and fibrous tissue that bind and protect the skeletal elements from dynamic motion. However, “false joints” are pathological and can lack these key structures (or if present can develop in a pathological fashion) resulting in poor distribution of dynamic load and accelerated development of osteophytic bony spurs, as occurred in the patient described in the present report. These osteophytic changes, if sufficiently large, can cause cord compression and myelopathy, as in our patient. C1 to C2 pseudoarticulations can arise with hyperlordosis of the cervical spine in clinical presentations such as rheumatoid arthritis. The recurrence of clinical myelopathy in our patient postlaminectomy suggests that these bilateral pseudoarticulations can lead to recurrent stenosis due to instability, much like what is often seen in the lumbar spine. Failure to recognize the presence of these pseudoarticulations can lead to persistent “subarticular” lateral stenosis if only central decompression of the canal is performed.
Conclusion
Ligamentous laxity and synovial inflammation in rheumatoid arthritis can lead to abnormal load distributions in the atlantoaxial complex and the development of pseudoarticulations, osteophytic bony spurs, and cord compression. The pathophysiology of synovial membrane and capsular development in noncongenital states remains unclear with potential links to underlying inflammatory processes or genetic predispositions. Posterior decompression and fusion were effective in this case of bilateral pseudoarticulations, which produced a posterolateral or “lateral recess” pattern of cord compression, which was refractory to central decompression alone.
Acknowledgments
Medacta Australia paid the article processing charge for this article.
Footnotes
Funding The authors received no financial support for the research or authorship of this article. Medacta Australia paid the article processing charge for publication.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval Informed (written and verbal) consent was obtained from the patient for publication of this manuscript and the accompanying images.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.