


Abstract
Background Lumbar interbody fusion is commonly performed to improve spinal stability in the context of degenerative, traumatic, and deformity-related pathologies. The axial lumbar interbody fusion (AxiaLIF) technique, also known as presacral interbody arthrodesis, is the only presacral interbody fusion technique approved by the US Food and Drug Administration. It is a rarely utilized approach to interbody fusion that aims to achieve fusion across L4 to L5 and/or L5 to S1 levels, which are the most susceptible to pseudoarthrosis and hardware failure. This case series describes the utility of the AxiaLIF procedure as a salvage approach when traditional interbody fusion techniques pose significant risks or are not feasible due to rare patient-specific factors.
Methods All identifiable cases of the AxiaLIF procedure performed at a single, academic medical center were reviewed. Operative data were collected and each case presentation is described in detail.
Results Six patients underwent AxiaLIF between July 2010 and May 2022. Indications for AxiaLIF as a salvage approach included hardware failure with a significant risk of recurrence with traditional revision techniques; a lack of segmental fixation at the distal end of the spinal construct; avoiding extensive tissue disruption in the setting of staged realignment surgery or previously compromised tissue; and comorbidities such as muscular dystrophy, abdominal hernias, and severe obesity. Two patients were fused solely across the L5 to S1 level, and 4 patients were fused from L4 to S1. The mean operative time, estimated blood loss, time under fluoroscopy, complications, and follow-up were noted.
Conclusion This case series introduces the utility of AxiaLIF as a salvage approach. We believe the AxiaLIF procedure may be a valuable alternative to traditional lumbar interbody fusion in salvage situations when traditional techniques are not feasible or pose significant risk to the patient. In such situations, surgeon awareness of this approach has the potential to improve patient outcomes and safety.
Clinical Relevance AxiaLIF, as a salvage approach, has the potential to improve patient outcomes safely when other surgical options pose significant risk or are not feasible.
Level of Evidence 4.
- Axial lumbar interbody fusion (AxiaLIF)
- salvage situation
- complex spine surgery
- lumbosacral fixation
- anterior column support
- interbody fusion
- presacral fusion
Introduction
Lumbar interbody fusion (LIF) is a well-established surgical intervention for various degenerative, traumatic, and deformity-related pathologies. LIF involves the removal of an intervertebral disc with subsequent insertion of an implant designed to promote fusion of adjacent vertebrae, enhance stabilization by providing intervertebral support, and restore disc height. Traditional open approaches include standard posterior lateral instrumentation, anterior lumbar interbody fusion (ALIF), transforaminal lumber interbody fusion (TLIF), and posterior lumbar interbody fusion (PLIF).1 Recently, minimally invasive techniques, including lateral LIF and oblique LIF, have gained popularity.1 Each technique achieves the insertion of an implant through its respective anatomical pathway.
The axial lumbar interbody fusion (AxiaLIF) technique, presacral interbody arthrodesis, is the only presacral interbody fusion technique approved by the US Food and Drug Administration (CPT22586). AxiaLIF is a minimally invasive technique first described by Cragg et al in 2004,2 utilizing a presacral pathway, defined posteriorly by the parietal fascia covering the sacrum, anteriorly by the visceral fascia of the mesorectum, and laterally by the internal iliac vessel to access the L4 to L5 and L5 to S1 vertebrae and disc spaces.2,3 Compared with traditional techniques, AxiaLIF reduces tissue insult, minimizes disruptive dissection and risk to adjacent structures, and may improve spinal stabilization by preserving the outer annular disc and the anterior and posterior longitudinal ligaments.2,4–6
At our institution, AxiaLIF is utilized when specific patient risk factors preclude traditional techniques. In such “salvage situations,” it is often the most appropriate choice. In the present report, we describe the AxiaLIF surgical technique and present a case series of unique complex spine surgeries demonstrating the utility of AxiaLIF. To our knowledge, this report is the first to describe the unique application of AxiaLIF as a “salvage approach.”
Methods
We retrospectively reviewed all identifiable cases of AxiaLIF performed by the senior author at our institution from July 2010 to May 2022. Six cases were identified and are subsequently described. Inclusion criteria consisted of any patient who underwent this procedure for any indication. The Institutional Review Board at our institution declared this case series exempt from Institutional Review Board approval.
Operative Technique
A 2-cm incision is made lateral to the paracoccygeal notch on either side. Finger and blunt dissection are performed to expose the anterior base of the sacrum and establish a presacral passageway. Malleable ribbon retractors are utilized to gently retract the rectum away from the sacrum. Guidewire is then placed under biplanar C-arm guidance into the sacrum at the appropriate trajectory, followed by the placement of dilators. The sacrum is then drilled through to the disc space. Disc preparation is accomplished by removing the disc material and endplate cartilage with custom curettes and shavers, followed by the placement of a bone graft. The process of guide pin advancement, drilling, disc space preparation, and bone graft placement is repeated for procedures that include the L4 to L5 level. Finally, the threaded interbody device is inserted via screw technique across the appropriate disc spaces and into the vertebral bodies. Biplanar C-arm views are utilized throughout the procedure for evaluation and implant positioning.
Clinical Presentations
Failure of Interbody Cage in the Setting of Compromised Soft Tissues
Patient A was a 54-year-old man with a medical history of type 2 diabetes mellitus managed with an insulin pump, obesity, multilevel lumbar stenosis, and multiple abdominal surgeries from a boating accident propeller strike to his flank and back. Despite significant soft tissue defects and scarring around the operative site, he underwent posterior lumbar decompression and instrumented fusion from L2 to S1 with interbody cage placement at the L5 to S1 level (Figures 1 and 2). Imaging 2 weeks postoperatively demonstrated dorsal extrusion of the cage into the spinal canal, placing him at significant risk for neurological sequelae and necessitating revision surgery. During cage removal, gross loosening of the left-sided S1 screw was noted, and the screw was removed and upsized. This screw loosening raised concern regarding the integrity of segmental fixation and potential risk for repeat cage dislodgment following a revision posterior interbody cage. Given his medical history and preserved disc space height at L5 to S1, anterior column support was desired to reduce the risk of hardware failure and pseudoarthrosis. ALIF was contraindicated due to his significant intra-abdominal scarring and surgical interventions that required skin grafting across the abdomen and flank. AxiaLIF was deemed the best approach to achieve spinal stability while minimizing the risk of failure and avoiding dangers of an anterior approach.

(A and B) Patient A presented following a recent posterior lumbar decompression, instrumentation, and fusion of L2 to S1. (C and D) Preoperative x-ray images reveal dorsal extrusion of the interbody cage. (E and F) Postoperative x-ray images at 12-month follow-up.

Clinical image depicting the soft tissue damage from Patient A’s boating accident, with scarring crossing the subsequent incision site. Extensive scarring across anterior abdomen precluded traditional anterior retroperitoneal approaches.
Five days after cage removal, AxiaLIF was performed at the L5 to S1 level. An elongated implant was utilized to enhance purchase and fixation (Table). Two weeks postoperatively, he developed a surgical site infection involving the posterior lumbar and paracoccygeal incisions, which resolved with incision and drainage, wound vacuum-assisted closure device therapy, and antibiotic treatment. At follow-up, beyond 1 year postoperatively, it appears fusion was achieved as the implant remains stable radiographically, and lumbar mechanical pain has dissipated.
Operative summary of case presentations of AxiaLIF procedures.
Adherent Iliac Vessels and Hardware Failure
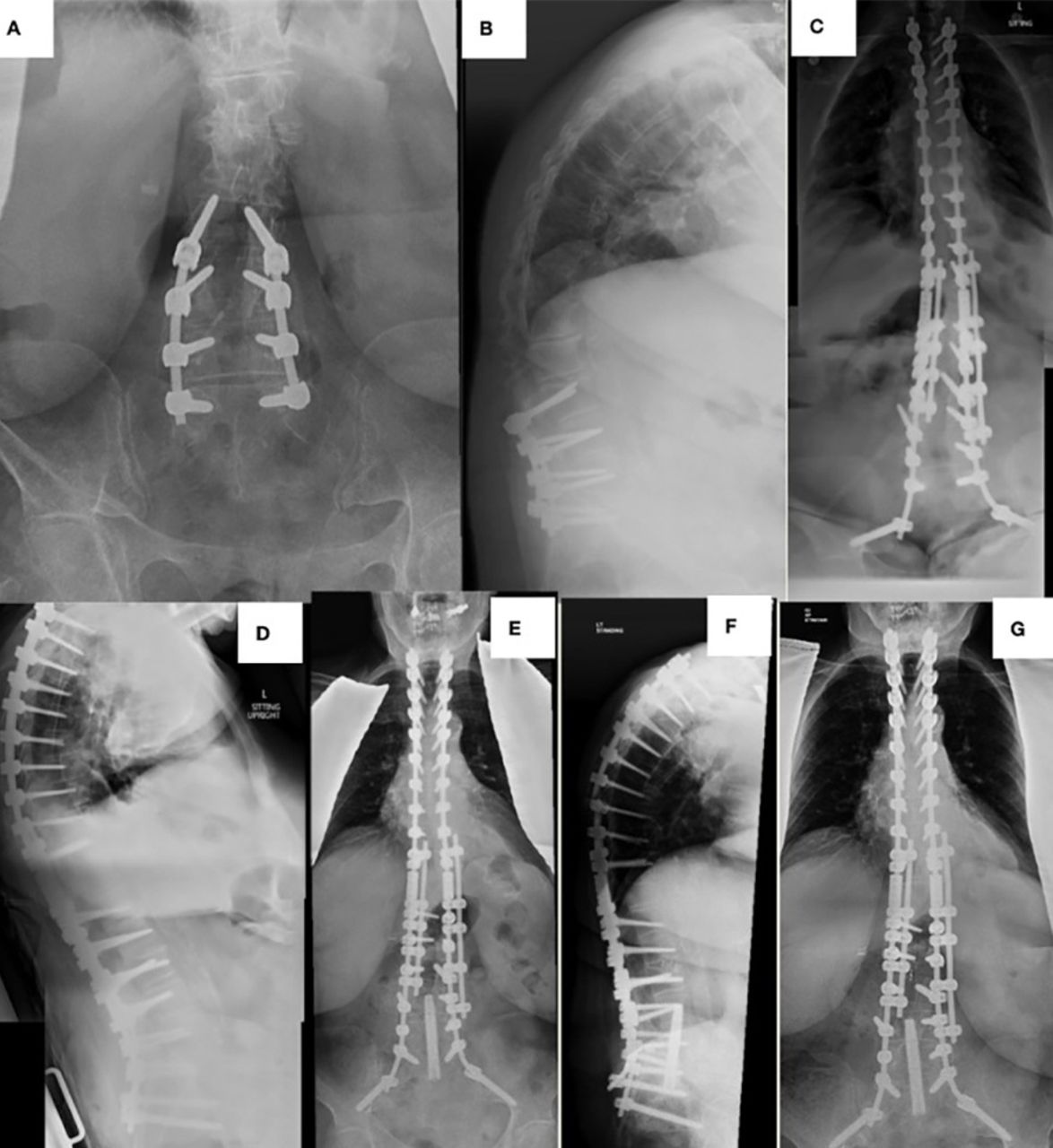
Patient B was a 48-year-old woman with a surgical history that included T10 to L5 posterior lumbar instrumented fusion with subsequent development of distal junctional failure and fracture of the L5 vertebral body addressed with L5 screw removal and extension of the construct to the ilium bilaterally (Figure 3). Approximately 8 months postoperatively, she presented with bilateral rod fracture between L4 and S1 and pseudarthrosis at L4 to L5 and L5 to S1. Additional surgical intervention was recommended, including posterior exploration of the fusion, revision of hardware at the lumbosacral junction, and L5 corpectomy with anterior fusion. Intraoperatively, hardware failure was identified below the L4 screw bilaterally. S1 and ilium screws were removed and upsized. Following the revision of hardware, she was repositioned supine for L5 corpectomy and anterior fusion. Then, it was determined that the iliac vessels were adherent to the L5 vertebral body, and corpectomy or limited discectomy from an anterior approach could not be achieved due to the high potential for vascular injury. A vascular surgeon corroborated injury concerns with an anterior surgical intervention, and the procedure was aborted.

(A) Patient B presented with distal junctional failure following T10 to L5 fusion. (B and C) Her fusion was extended to the ilium, which subsequently progressed to pseudoarthrosis and rod fracture. (D and E) Postoperative x-ray images following the axiaLIF procedure. (F and G) Most recent x-ray images more than 4 years postoperatively.
Due to previous pseudoarthrosis, hardware failure, and lack of segmental fixation at the distal aspect of the construct, she was considered to be at high risk for recurrent failure with posterior-only instrumentation. Anterior column support was desired. One day after the aborted ALIF, she underwent a recommended L4 to S1 AxiaLIF with no intraoperative complications (Table). At the most recent follow-up, 13 years postoperatively, hardware has remained intact across the lumbosacral junction.
Muscular Dystrophy and Abdominal Hernia
Patient C was a 75-year-old man with a history of large abdominal hernia, muscular dystrophy, and multilevel lumbar lateral recess and neuroforaminal stenosis from L4 to S1 with neurogenic claudication and lumbar radiculopathy. His muscular dystrophy, violating the posterior musculature for a posterior decompression and instrumented fusion, carried a significant risk of excessive surgical insult and compromise to his weak posterior musculature. Additionally, the large abdominal hernia prevented safe access to the spine precluding ALIF. We recommended AxiaLIF, with a distraction screw, to provide indirect decompression while preserving his posterior musculature and avoiding potential complications associated with an anterior approach (Figure 4).

(A) Patient C preoperative x-ray image. (B and C) Postoperative x-ray images following the axial lumbar interbody fusion procedure. (D) X-ray image at 6-month follow-up.
Intraoperatively, a presacral arthrodesis screw with a distracting component for indirect decompression was placed after removing the disc material at L4 to L5 and L5 to S1. Percutaneous screws and rods were then placed at L4 and S1 bilaterally (Table). The patient recovered without complication and has benefited from the procedure at the latest follow-up.
Maintaining Deformity Correction After Hardware Failure
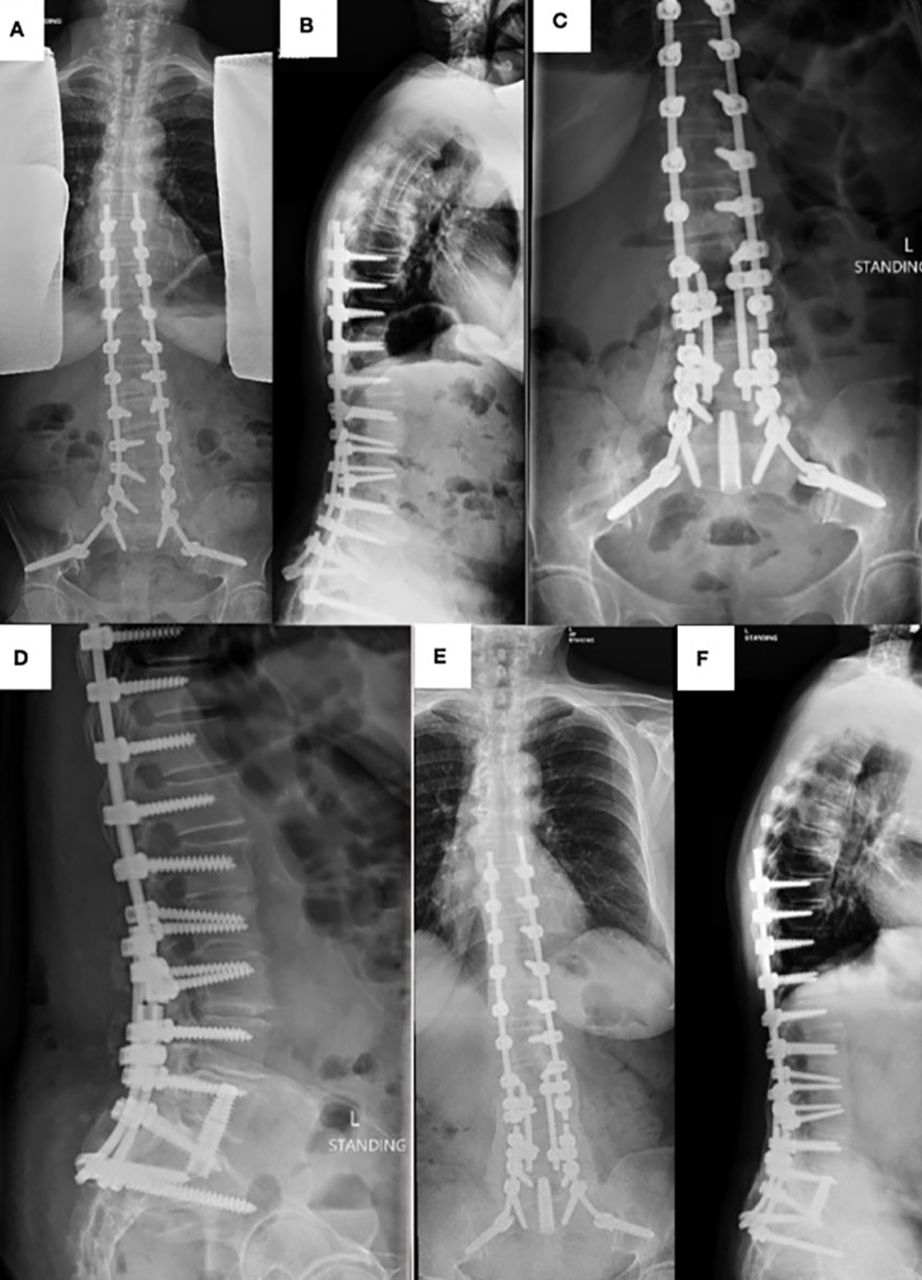
Patient D was a 67-year-old woman with a history of extreme obesity (body mass index = 53), severe kyphoscoliosis with sagittal imbalance greater than 16 cm, previous C3 to C6 laminoplasty, and previous L3 to S1 lumbar decompression and instrumented fusion performed elsewhere with subsequent development of pseudoarthrosis and adjacent segment disease (Figure 5). She developed an inability to maintain a horizontal gaze due to a severe positive sagittal imbalance of greater than 25 cm and reported a rapidly deteriorating quality of life. Given her severely comorbid state, spine surgery carried significant complication risks (>65%), and she desired to proceed with staged realignment/reconstructive surgery. The first stage included posterior decompression L1 to L3, revision decompression L3 to L4, T2-ilium instrumented fusion with revision of pedicle screws L3 to S1, and a Ponte osteotomy at L2 to L3 to correct significant sagittal imbalance. Due to significant physiological insult and blood loss, further intervention was postponed with a future option for lateral interbody at the L2 to L3 Ponte osteotomy site and presacral interbody at L4 to S1.

(A and B) Patient D presented with significant kyphoscoliosis and a history of L3 to S1 lumbar decompression and fusion. (C and D) Postoperative x-ray images following the first stage of realignment/reconstructive surgery. (E and F) Postoperative x-ray images following axial lumbar interbody fusion procedure. (G) X-ray image at 15-month follow-up.
Approximately 1 month postoperatively, she was optimized for further surgical intervention. In the interim, screw loosening/lateral cut-out on the right side at L4 was identified, raising concern for pseudoarthrosis and hardware failure without interbody support. ALIF was precluded due to previous abdominal surgeries and her large pannus, and TLIF was thought unlikely to provide sufficient support. We recommended AxiaLIF to provide anterior column support and reduce the risk of failure. Intraoperatively, the AxiaLIF implant was placed across the L5 to S1 and L4 to L5 disc spaces into respective vertebral bodies (Table). Two weeks postoperatively, she developed wound dehiscence of the paracoccygeal incision due to her extreme obesity and significant comorbid state, resolving with local debridement, wet-to-dry dressing changes, and wound vacuum-assisted closure. Eight months postoperatively, she underwent lateral interbody fusion at L2 to L3 without complication. At 15-month follow-up, she showed no evidence of hardware failure or loosening.
Hardware Failure and History of Abdominal Adhesions
Patient E was a 68-year-old woman with a history of prior hysterectomy, back pain, and previous lumbar decompression at L1 to S1 and instrumented fusion from T8-ilium (Figure 6). She developed persistent back pain, and imaging revealed rod fracture and pseudoarthrosis at the L5 to S1 level bilaterally. Following nonoperative management, revision surgery to address hardware failure and pseudoarthrosis was recommended. An anterior surgical approach carried significant risk due to adhesions from her prior abdominal surgery. Additionally, PLIF/TLIF, requiring revision decompression prior to cage placement, carried unnecessary risk for dural injury and neurological sequela. AxiaLIF was selected to provide anterior column support at L5 to S1 in conjunction with revision instrumented fusion from L2-ilium.

(A) Patient E presented with a history of decompression with instrumented fusion from T8-ilium. (B) Lateral preoperative x-ray image showing rod fracture and pseudarthrosis at the L5 to S1 level. (C and D) Postoperative x-ray images following the axial lumbar interbody fusion procedure. (E and F) X-ray images at 3-year follow-up.
Intraoperatively, the AxiaLIF implant was placed across the L5 to S1 disc space. Revision posterior instrumentation was then completed. There were no intra- or postoperative complications (Table). At 3 years postoperatively, she showed no evidence of hardware failure or adjacent segment changes.
Hardware Failure and a High Risk of Cage Subsidence
Patient F was a 66-year-old man with a prior surgical history including C4 to C7 anterior cervical discectomy and fusion, C3 to C5 posterior instrumented fusion, and posterior decompression and instrumented fusion from T10 to L1 performed elsewhere (Figure 7). Due to severe neurogenic claudication secondary to adjacent segment disease and multilevel lumbar stenosis, he underwent posterior lumbar decompression L1 to L5 and extension of instrumented fusion from T10 to L5. One year postoperatively, his symptoms persisted, and imaging revealed L4 to L5 pseudoarthrosis with bilateral L5 screw loosening and adjacent segment disease at L5 to S1 resulting in significant stenosis. He underwent revision decompression L4 to S1 with the extension of the construct to the ilium. Segmental fixation at L5 could not be achieved due to significant haloing about the screws leading to compromise of the L5 vertebral body and endplates. Due to the lack of segmental fixation, PLIF/TLIF was deemed inappropriate because of the risk of cage dislodgment. Anterior column support was desired to reduce the risk of pseudoarthrosis and hardware failure over the L4 to S1 span. Due to the compromise of the L5 vertebral endplates, it was thought that ALIF carried a high risk of subsidence. AxiaLIF was selected to achieve fusion through fixation in its vertical trajectory. One month after the failed revison decompression, he underwent AxiaLIF.

(A) Patient F presented with a history of a T10 to L1 fusion. (B) Postoperative x-ray image following the extension of fusion to L5. (C) Postoperative x-ray image after extension of fusion to the ilium. (D and E) Postoperative x-ray images following axial lumbar interbody fusion procedure. (F) X-ray image at 5-year follow-up.
Intraoperatively, a presacral pathway was created to access the L4 to S1 disc spaces with minimal tissue disruption, allowing for subsequent implant placement. No intra- or postoperative complications occurred (Table). At the most recent follow-up, 5 years postoperatively, the AxiaLIF implant appeared in proper position without evidence of failure or loosening.
Discussion
This case series introduces the utility of the AxiaLIF procedure as a “salvage approach” when traditional interbody fusion techniques pose significant risks due to patient-specific comorbidities or extensive prior surgical intervention. AxiaLIF was used selectively in salvage situations: hardware failure with a significant risk of recurrence with traditional revision techniques; lack of segmental fixation at the distal end of spinal constructs; avoidance of extensive tissue disruption in the setting of staged realignment surgery or previously compromised tissue; and comorbidities. AxiaLIF may also be considered when anterior approaches pose an increased risk to patient safety (extensive scarring and adhesions or herniations).
Addressing the anterior column is paramount during spinal fusion, as a lack of anterior column support places patients at increased risk for pseudoarthrosis and hardware failure. Developed in the 1930s, ALIF was the first interbody fusion technique to successfully achieve spinal fusion and preceded many contemporary techniques (PLIF, TLIF, oblique LIF, and lateral LIF).7 AxiaLIF can be used as an alternative at the L4 to S1 levels providing anterior column stabilization of the lumbosacral spine while reducing physiological insult. This approach may further enhance spine stability through the preservation of the annulus fibrosis and the threaded nature of the implant.5,8,9
Biomechanical testing in bovine specimens and preliminary studies of AxiaLIF has delivered promising results.8,10,11 Biomechanical testing of the AxiaLIF construct in both 1- and 2-level trans-sacral rod placement demonstrated a significant decrease in range of motion, further augmented by the placement of facet and pedicle screws.9,12 Subsequent studies with long-term follow-up provided evidence that AxiaLIF decreased postoperative visual analog scale and Oswestry Disability Index scores, improved back pain and function, and carried relatively low complication rates in both 1- and 2-level procedures.13–19 In a systematic review, Schroeder et al found a 90.5% fusion rate at the lumbosacral junction following axial interbody fusion.20 A multicenter review of 96 patients found no significant difference in fusion rates between traditional ALIF and AxiaLIF.21
Relative contraindications for AxiaLIF include severe degeneration, adhesions obstructing the anatomical pathway of the procedure, and a history of retroperitoneal surgery in the operative area.11,19 Perioperative risks of the procedure include iatrogenic bowel perforation, infection, pseudoarthrosis, pelvic hematoma, sacral fracture, ureter injury, and transient nerve root irritation.14,22,23 The complication risk is low with Gundana et al reporting a complication rate of 1.3%.24 Our patients experienced no intraoperative complications. Postoperatively, 1 patient, with sacral wound dehiscence due to extreme obesity, was treated successfully with secondary intention healing; also, 1 patient had an infection of the paracoccygeal incision due to poorly controlled diabetes, but the infection resolved with incision and drainage and conservative measures. These complications were not unexpected. As previously stated, AxiaLIF, at our institution, is solely for highly complex spine surgeries in patients with significant comorbidities. There were no long-term complications from this procedure.
Conclusions
Our cases demonstrate the utility of AxiaLIF in uncommon and challenging patient presentations. At our institution, posterior interbody fusion approaches were precluded in instances of muscular dystrophy, cases with major risk of further physiological insult, and an increased risk of repeat hardware failure in patients with poor bone quality and inadequate fixation at the distal portion of their constructs. The anterior intervention is contraindicated in patients with a history of significant abdominal surgery, extreme obesity, abdominal hernias, and adherent iliac vessels. AxiaLIF allowed for the fusion of the L4 to L5 and L5 to S1 levels and anterior column stabilization of the lumbosacral spine in these unique situations. Our experiences demonstrate that AxiaLIF can be utilized as a “salvage approach” to lumbosacral fusion when encountering rare patient presentations. When traditional techniques are not feasible or pose significant risks, surgeon awareness of this approach has the potential to improve patient outcomes and safety.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors declare no conflicts of interests with this manuscript.
Disclosures William Lavelle is a paid consultant, paid presenter, and has stock or stock options for 4-Web, research grants for Abryx, AO Foundation, Cerapedics, Empirical Spine, Medtronic, Spinal Kinetics, Inc., 3 Spine; is a paid consultant for DePuy Spine; has stock or stock options for Expanding Innovations; and serves on advisory boards for Vertiflex, TruSpine, and Innovasis. Richard Tallarico is a paid consultant for Stryker Spine and has received research grants for Vertiflex, Spinal Kinetics, Inc., Cervitech, Inc., Stryker; 3 Spine. The remaining authors have nothing to disclose.
IRB Approval The Institutional Review Board (IRB) at our institution declared this case series exempt from IRB approval.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.