


Abstract
Background Surgical management of severe thoracolumbar kyphosis (TLK) is challenging due to the necessity of achieving adequate sagittal realignment without increasing operative risk or compromising hardware integrity. Performing large corrective maneuvers during deformity correction may increase the risk of neurological complications, especially when correcting hyperkyphosis in the distal thoracolumbar spine. The present article describes the first use of a custom-made articulating rod to manipulate a patient’s severe TLK into extension in combination with the expandable lateral interbody device to achieve circumferential deformity correction.
Clinical Presentation A 38-year-old woman with a history of spinal trauma 10 years ago developed severe TLK (<70° angulation) after failed posterior spinal stabilization. Due to her debilitating neurological symptoms and profound sagittal deformity, we performed a T9 to L2 navigation-assisted posterolateral fusion followed by a circumferential kyphotic correction utilizing a custom-made articulating rod (Globus Medical, Inc., Audubon, PA) with an expandable device placed in prone-lateral position at T11 to T12. The use of an articulating rod enabled us to safely manipulate the thoracolumbar spine into extension prior to permanent rod fixation. We were able to achieve approximately 40° of thoracolumbar correction. No immediate or late (at 2-year follow-up) postoperative medical or hardware-related complications were reported.
Conclusion The use of an articulating rod with prone-lateral placement of an expandable interbody device allowed for a high degree of circumferential thoracolumbar deformity correction in a patient with severe post-traumatic TLK. Our results indicated the technical feasibility and success of utilizing this treatment strategy for high-grade TLK without medical- or hardware-related failure.
Clinical Relevance The use of an articulating rod for correction of complex TLKs may benefit patient outcomes and improve safety.
Level of evidence 4.
Introduction
Thoracolumbar kyphosis (TLK) represents a significant source of functional, neurological, and cosmetic morbidity.1,2 Surgical management of severe TLK is challenging due to the necessity of achieving adequate realignment without increasing operative risk. However, in performing the necessary corrective maneuvers, the rate of neurological complication can be exceptionally high.3–5 Etiology of neurological complications can range from blood flow and pressure aberrations, compression/traction of neural elements, or osteotomy-related injury.6 Therefore, various techniques are employed to maximize corrective ability while decreasing operative risks, such as multistaged surgeries, implementation of nontraditional approaches, and use of novel technologies for controlled spinal reduction to prevent neural injury.4
In the current article, we present a technical report of our patient undergoing circumferential correction of severe TLK (>70°) by combining a custom-made articulating rod to control compression/distraction forces on the neural elements and an expandable lateral interbody device. The articulating rod acts by capitalizing on a central pivot point that allows for dynamic maneuvers of the spinal alignment not possible with static rods and in situ benders. We believe that the collective use of such devices can allow for safe, durable, and significant thoracolumbar correction, particularly in highly sensitive spinal segments.
Clinical Presentation
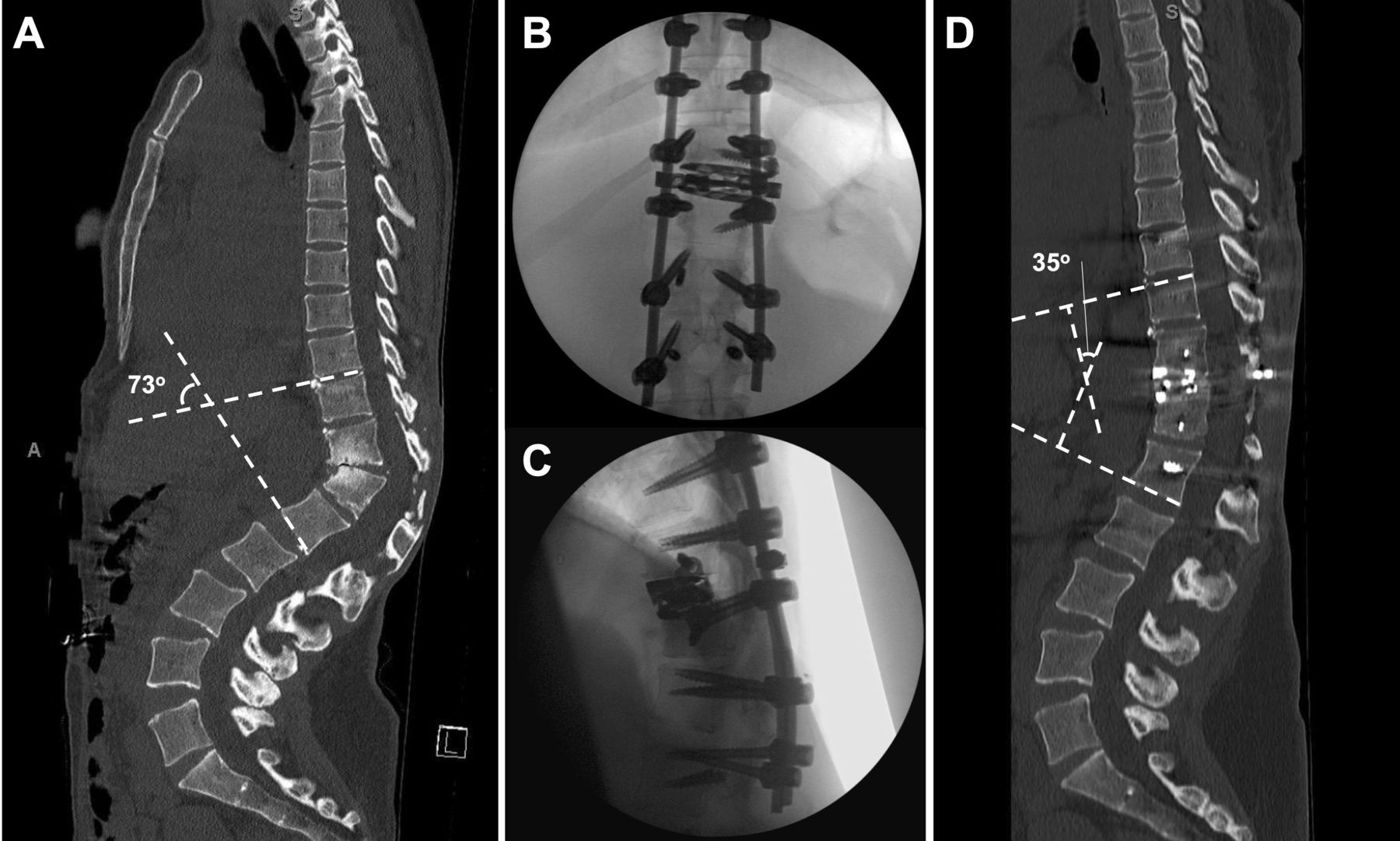
A 38-year-old woman with a history of spinal trauma requiring previous lumbar fusion 10 years prior presented with complaints of severe positive sagittal deformity contributing to neurogenic claudication, back pain, and radiculopathy into the anterior thigh and knee bilaterally. Past medical history was significant for hypertension and obesity. While she was neurologically full strength and had no sensory deficits on physical examination, she exhibited a forward-leaning station and profoundly antalgic gait. Medications included gabapentin, methocarbamol, and buprenorphine. Conservative management including physical therapy, and chiropractic care was trialed without benefit. Computerized tomography and magnetic resonance imaging indicated a severe TLK with apex at T11 to T12 and a Cobb angle between T10 and L1 of 73° (Figure 1A). Evidence of prior failed fusion was noted with fracture and retained pedicle screw fragments at L2. Otherwise, available neuraxial imaging was benign.

(A) Preoperative computerized tomography (CT) shows a severe thoracolumbar kyphosis due to wedge deformity causing posterior canal stenosis and a Cobb angle of 73° at the T11 to 12 apex. (B and C) Anteroposterior and lateral intraoperative fluoroscopy images showing posterolateral instrumented fusion with a left-sided approach lateral interbody device at T11 to T12 with integrated fixation. (D) Postoperative follow-up CT at 2 years with nearly 40° correction. No hardware issues were noted.
Operative Plan
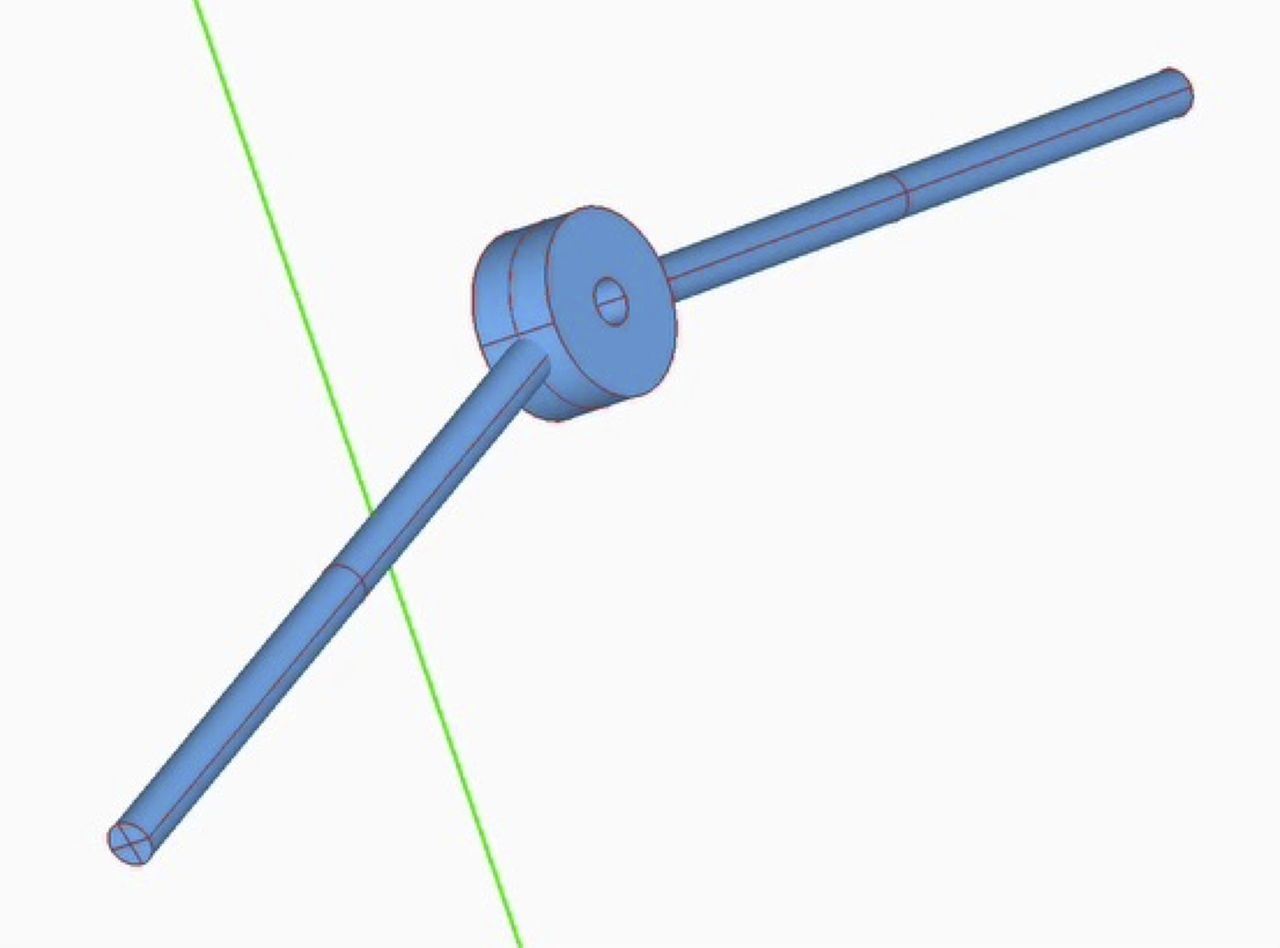
Given the degree of symptomatic kyphotic deformity and failure of conservative therapy, surgical intervention was recommended by way of T10 to L1 laminectomy, Ponte osteotomies at T11 to T12, placement of expandable lateral interbody device (Globus Medical Inc., PA, USA) at T11 to 12 in prone-lateral position, and T9 to L2 navigation-assisted posterior pedicle screw fixation. Considering the need to achieve significant sagittal deformity correction, we opted to use a custom-made articulating rod (Globus Medical Inc., PA, USA) to allow for controlled distraction and extension during reduction maneuvers (Figure 2, Supplemental Video 1). The risks and benefits were discussed with the patient, and informed consent was obtained for operative management. The patient provided consent to use of their deidentified clinical information for publication. No institutional review board approval was necessary per institutional case report policy.

Schematic of an articulating rod using a commercially available 3-dimensional software used to create the device.
Surgical Management
Instrumentation and decompression with Schwab Grade 2 posterior osteotomies were performed. A standard superficial left-sided lateral approach was then utilized at the T11 to T12 level, tailored to the severity and anatomical presentation of the deformity. An anterior column release was performed in the lateral position using an anterior column blade to precisely transect the anterior longitudinal ligament, with surrounding structures protected throughout the procedure using a spec retractor. Due to the anatomical presentation of the deformity, the mobilization of the diaphragm and pleura was not required, and a retropleural approach was unnecessary. Segmental vessels were carefully ligated using bipolar cautery to prevent bleeding.
The articulating rod was then introduced and secured into the pedicle screws to sequentially expand the T11 to T12 disc space. This allowed for the placement of an expandable interbody device, inserted in the prone-lateral position. Once adequate expansion was achieved, the articulating rod was adjusted into a slight extension, and the T12 to L2 screw caps were tightened. Reduction towers were placed on the top T9 to T11 screws to further correct the thoracolumbar deformity. No intraoperative neuromonitoring (IONM) changes were noted during these maneuvers.
After achieving the desired correction, the final rod was placed on the contralateral side of the articulating rod and securely tightened. The articulating rod was then removed and replaced with a second rod, augmented with a cross-connector over the T11 to T12 space for added stability. A chest tube was placed, and appropriate postoperative imaging was obtained to evaluate for pneumothorax. The patient was then closed in a standard fashion. IONM remained stable throughout the case. The total operative time was 478 minutes, with an estimated blood loss of 750 cc.
Postoperative Outcome
Thoracolumbar kyphotic angle was 35°, showing a 40° improvement from preoperative measurements. Anteroposterior and lateral intraoperative films showed adequate placement of hardware (Figure 1B and C). The patient was observed in our standard step-down unit until postoperative day 10, after which she was transferred to inpatient rehabilitation. No postoperative medical complications were noted, and our patient did not require a blood transfusion. Of note, due to the patient’s significant preoperative opioid necessity, our acute pain management service was consulted for the comanagement of postoperative pain.
Follow-Up
At a 2-year postoperative evaluation, the patient had significant improvement in back and lower extremity pain, sagittal deformity, and claudication symptoms. No hardware issues were noted on follow-up imaging, and preservation of immediate postoperative correction was maintained (Figure 1D).
Discussion
Advancements in surgical technique and spinal technologies have allowed for high degrees of correction in sagittal deformity of various etiologies. In our patient who presented with delayed posttraumatic TLK, her severe (>70°) focal kyphosis necessitated extreme focal correction to allow for the return of sagittal alignment. The greatest concern for any deformity correction, especially in cases of hyperkyphosis of the distal thoracic spine, includes injury to neural elements due to cord distraction/compression during the corrective maneuvers.6 In addition, we believed that the use of pedicle subtraction osteotomy (PSO), while they may have provided the necessary degrees of correction, would have increased the overall risk profile with minimal gain considering her deformity was not rigid.7
Therefore, we opted to provide anterior support with a lateral interbody device, maximize lordotic potential with an anterior column release, and minimize the osteotomy necessary to achieve the necessary correction. However, the concern still remained of neurological compromise during the maneuver to distract the disc space open to allow for the interbody device to be introduced in a highly collapsed space and the maneuver to compress the thoracolumbar spine into the proper alignment. Here, the articulating rod was used in conjunction with IONM to safely achieve the planned correction. Depending on the points of fixation, we are able to directly control compression and distraction of the spine with rod holders on the articulating rod without the need for in situ benders. Additionally, any IONM changes can be detected instantaneously and can thereby be reversed quickly.
The intraoperative video shows the active use of the articulating rod (Supplemental Video 1). By placing the articulating rod with the central pivot hinge over the kyphotic point and finally tightening it with set caps, we can distract the disc space safely (Figure 3A). This allowed us to safely introduce our lateral interbody device (Supplemental Video 2). When we fix the articulating rod to the pedicle screws at the caudal end of the construct without final tightening set caps at the proximal end, we are able to compress the spine. With downward pressure, the articulating rod slides within the tulip heads (Figure 3B). We combined this maneuver with the expansion of the interbody device to achieve an adequate correction—approximately 40° comparable to a standard PSO.8

Illustration of placed articulating rod. (A) With the articulating rod in place within the pedicle screw tulip and all set caps finally tightened, downward pressure utilizing heavy rod holders allows for distraction of the disc space immediately inferior to the central pivot point. This allows for increased space to introduce an expandable lateral interbody device safely. (B) The cranial set caps are then loosened. When downward pressure is applied now, it allows for compression. With the sequential expansion of the interbody device with a continued downward force vector, the construct and spine can be placed in mild extension. Intraoperative neuromonitoring during these maneuvers is critical.
Limitations
While this is the first reported use of an articulating rod in literature for complex thoracolumbar correction of sagittal deformity, the applicability of this technology will need to be determined with additional trials. However, its inaugural use without complication, even at 2-year follow-up, is encouraging. Future reports should include long-term functional outcomes to provide a more complete patient assessment.
Conclusion
Our use of a custom-made articulating rod allowed for the safe placement of an expandable lateral interbody device and controlled compression and distraction during a severe TLK correction case. We were able to achieve a 40° correction without the need for multilevel PSOs or a vertebral column resection, which we believe contributed to reduced risk and ultimate operative success. While more trials are necessary prior to further implementation, the use of articulating rods in select patients requiring extensive kyphotic corrections is technically feasible and may offer benefits in risk reduction during corrective maneuvers.
Supplementary material
Supplemental Video 1.
The mechanism of action for the articulating rod is seen after midline exposure, posterolateral pedicle screw fixation, and posterior element release are completed. Downward vector causes the articulating rod to pivot on its central lever proportional to the force applied. The exposed spinal cord can be seen adjacent to the central pivot.Supplemental Video 2.
This sequence demonstrates the technique to induce distraction in order to safely introduce the lateral interbody device into the collapsed space. The set caps are tightened at all points, fixing the articulating rod to the pedicle screws. Rod holders are used to apply downward force, which opens the disc space (see Figure 2A) so that the lateral interbody device can be introduced. Intraoperative C-arm fluoroscopy confirms adequate placement, and the interbody device is expanded in the lateral plane.Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Statement No Institutional Review Board approval was necessary per institutional policy. Consent for use of de-identified clinical information for publication was obtained.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.