


Abstract
Background Uniportal spine endoscopy is a minimally invasive technique gaining widespread popularity, but fluid insufflation during the procedure poses risks of neurological deterioration. The present study examines these risks through a case series and literature review.
Methods A review of the literature was conducted to identify reported complications related to fluid insufflation. Additionally, we present a case series of 3 patients who experienced neurological deterioration associated with irrigation pressures.
Results Key findings from the literature include complications such as raised intracranial pressure, seizures, durotomy-induced injuries, and unintended fluid migration. This case series describes novel complications, including transient ipsilateral weakness and lumbosacral plexopathy, linked to high irrigation pressures.
Conclusion Neurological deterioration, though rare, is a significant risk in uniportal spine endoscopy. Future research should focus on defining optimal irrigation parameters and pressure management strategies.
Clinical Relevance
By understanding the mechanisms in which fluid insufflation may cause neurological deterioration and by consequently adopting preventive strategies, surgeons can reduce complications and improve patient outcomes.
Level of Evidence 4.
Introduction
In recent decades, minimally invasive surgical treatments have gained popularity as an alternative to their open counterparts. While the primary goal of any surgical procedure is to treat the underlying disease process, there has become an increasing focus on secondary outcomes including reduced postoperative pain, shorter hospital stays, and faster return to daily activities. Since Kambin and Hijikata first described their respective endoscopic spinal procedures,1,2 significant advancements have been made in this field as endoscopic procedures have evolved, and their clinical indications have grown. Compared with open spinal procedures, endoscopic spine surgery has been shown to have reduced postoperative back pain and shorter hospital stays with comparable long-term outcomes.3,4 This is likely due to the shorter duration of muscle retraction with smaller skin and fascia incisions and reduced soft tissue and bony resection required.5
The standard endoscopic spinal surgical technique has been referred to as full-endoscopic, percutaneous endoscopic, or uniportal endoscopic spine surgery. This method utilizes an endoscope with its portal and optics included in the same device, the introduction of the endoscopic device via percutaneous access, and the use of a uniportal approach under continuous saline irrigation.6 This differs from biportal endoscopic spine surgery, which involves a separate optic and working portal,7 though both methods have been shown to have similar clinical outcomes.8
Many minimally invasive surgical procedures require the use of gas to create pneumoperitoneum to create a space to view the surgical field through the endoscope. However, in the bladder and joint cavities, fluid is more commonly used as a distention and irrigation media.9 In endoscopic spine surgery, low-pressure irrigation allows the control of epidural bleeding as well as maintaining visibility within the potential working space.10
Although there are many advantages of endoscopic approaches compared with traditional open spinal surgery, endoscopic techniques are not without their risks. In 1 recent systematic review, the complication rate was 9.26% for uniportal endoscopic spine surgery, with most complications occurring in the perioperative period. The most common complications identified from endoscopic spine surgery include intraoperative durotomy, transient neurological deficit, dysesthesia, radicular pain, and early recurrence of disc herniation or canal stenosis.11 Additionally, irrigation during endoscopic spine surgery can lead to postoperative headache, seizures, visual impairment, and autonomic dysreflexia, especially after incidental durotomy.12,13 Fluid insufflation may also lead to extravasation or intravasation of fluid. Extravasation of fluid can result in tissue edema, while intravasation of fluid into the patient’s circulation can result in electrolyte disturbances and cardiopulmonary complications.9
While there have been some reports of complications of endoscopic spine surgery due to fluid insufflation, there is a paucity of data on this topic. The purpose of this review is to catalog published complications due to fluid insufflation in uniportal spine endoscopy, present a case series of complications from a single-surgeon experience, and provide risk mitigation strategies to optimize patient safety when performing such procedures.
Methods
This literature review aimed to identify and synthesize existing literature on the occurrence and mechanisms of neurological deterioration associated with fluid insufflation in endoscopic spinal surgery. The review focused on identifying the risks and pathophysiological mechanisms of neurological impairment specifically related to fluid management in spinal endoscopic procedures.
A comprehensive search of peer-reviewed articles was conducted across multiple databases, including PubMed, Embase, and Web of Science. Keywords and Medical Subject Heading terms included “neurological deterioration,” “complications,” “fluid insufflation,” “irrigation,” and “endoscopic spine surgery.” Boolean operators were used to broaden the search. Articles were screened based on their relevance and study quality. The review included case studies, cohort studies, randomized controlled trials, and systematic reviews that reported on neurological complications associated with fluid insufflation in spine endoscopy. Excluded were articles without specific mention of complications, studies involving animals, or unrelated articles. A qualitative synthesis was conducted to analyze patterns and common findings. Statistical meta-analysis was not conducted due to variability in study design, and outcome measures across included studies. Findings were grouped thematically based on complications and mechanisms of injury.
In addition to the review of literature, we conducted a retrospective case series of all cases of endoscopic spinal surgery performed at a single Neurosurgical center in Sydney, Australia, between January 2015 and November 2024. All cases within this period were reviewed for instances of neurological deterioration associated with fluid insufflation. Patients were included if they underwent endoscopic spinal surgery and experienced a postoperative neurological deterioration potentially associated with fluid insufflation. All patients provided informed consent for their data to be included in this study. Clinical data were extracted from their medical records, including demographic information, surgical details, pre- and postoperative neurological outcomes, and postoperative management and imaging. Neurological deterioration was defined as a documented new or worsened neurological deficit following the procedure.
Case Series
Case 1
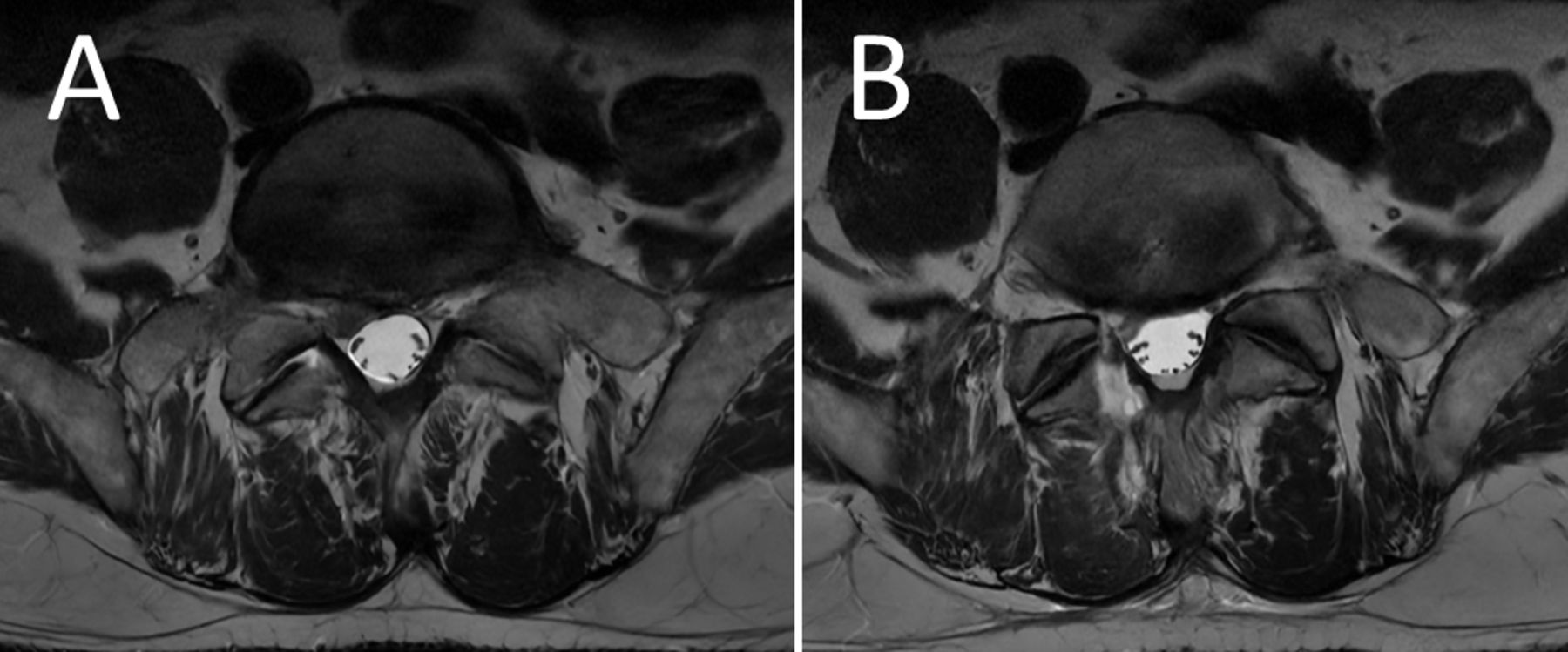
A 57-year-old man with lower back pain and right-sided S1 radiculopathy, presenting with mild ankle plantar flexion weakness (Medical Research Council [MRC] grade 4+), underwent a right-sided L5/S1 microdiscectomy for a paracentral disc herniation. During surgery, an interlaminar endoscopic system (Elliquence, USA) was used, and fluid irrigation pressures exceeded 50 mm Hg due to preoperative aspirin use and increased bleeding. Postoperatively, the patient developed transient worsening of ankle plantarflexion weakness (MRC grade 3). Magnetic resonance imaging (MRI) revealed paraspinal muscle signal changes (Figure 1) attributed to high intraoperative fluid pressure, with good decompression of the S1 nerve root. By postoperative day 2, his weakness had resolved, and at the 6-week follow-up, he reported no complications.

(A) Magnetic resonance image (MRI) of the lumbar spine (axial) demonstrating right L5/S1 paracentral disc herniation contacting the right S1 nerve root. (B) MRI of the lumbar spine (axial) 24 hours after the operation demonstrating signal change within paraspinal musculature.
Case 2
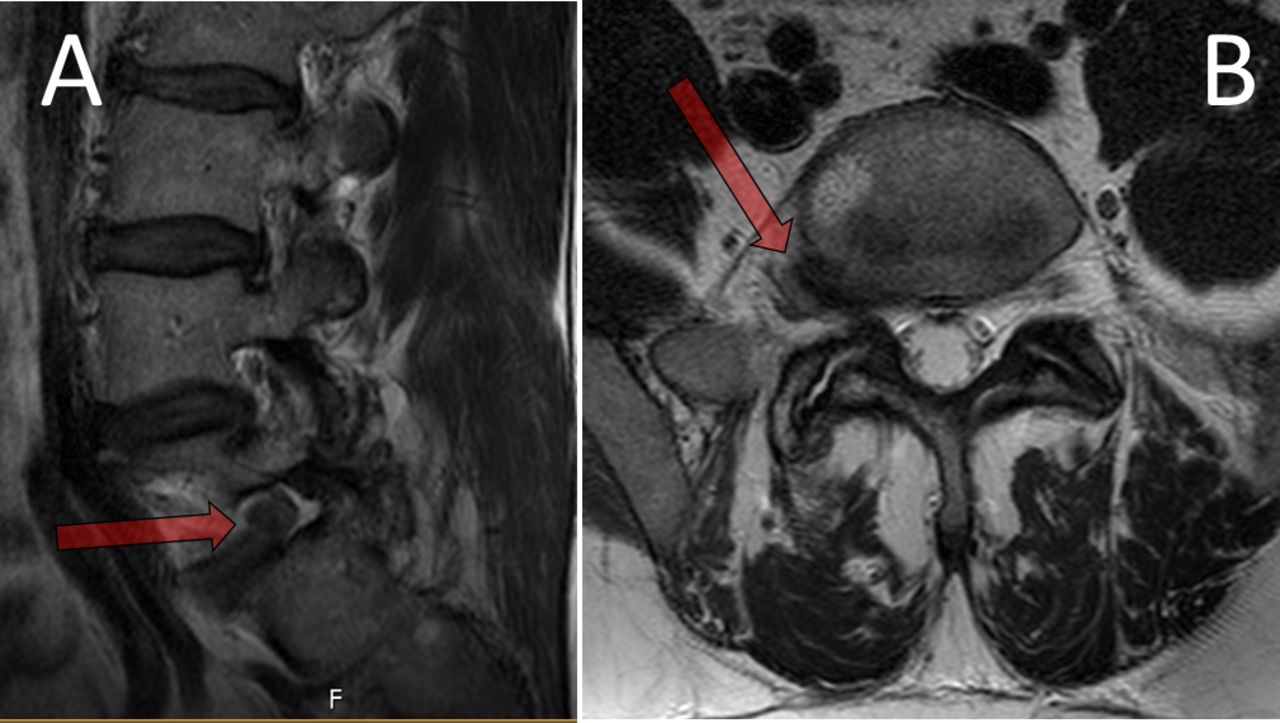
A 78-year-old man with lower back pain and right-sided L5 radiculopathy, presenting with mild ankle dorsiflexion weakness (MRC grade 4+), underwent a right-sided L5/S1 microdiscectomy for a foraminal disc herniation compressing the L5 nerve root (Figure 2) via the transforaminal corridor. During surgery, a transforaminal endoscope system (Matrix Endoscopy, Australia) was used to remove a large disc fragment. Postoperatively, the patient developed transient lumbosacral plexus palsy with weakness in knee extension, ankle movements, and dorsiflexion/plantarflexion. Imaging showed no acute pathology, and decompression of the L5 nerve root was satisfactory. His weakness was resolved by postoperative day 2, and at the 6-week follow-up, he reported no complications. Sustained high irrigation pressures were deemed to be the causative agent of the transient weakness as no other cause could be found.

(A) Magnetic resonance image (MRI) of the lumbar spine (sagittal) demonstrating L5/S1 foraminal disc herniation (red arrow) compressing the exiting L5 nerve root. (B) MRI of the lumbar spine (axial) demonstrating the same right-sided L5/S1 foraminal disc herniation (red arrow).
Case 3
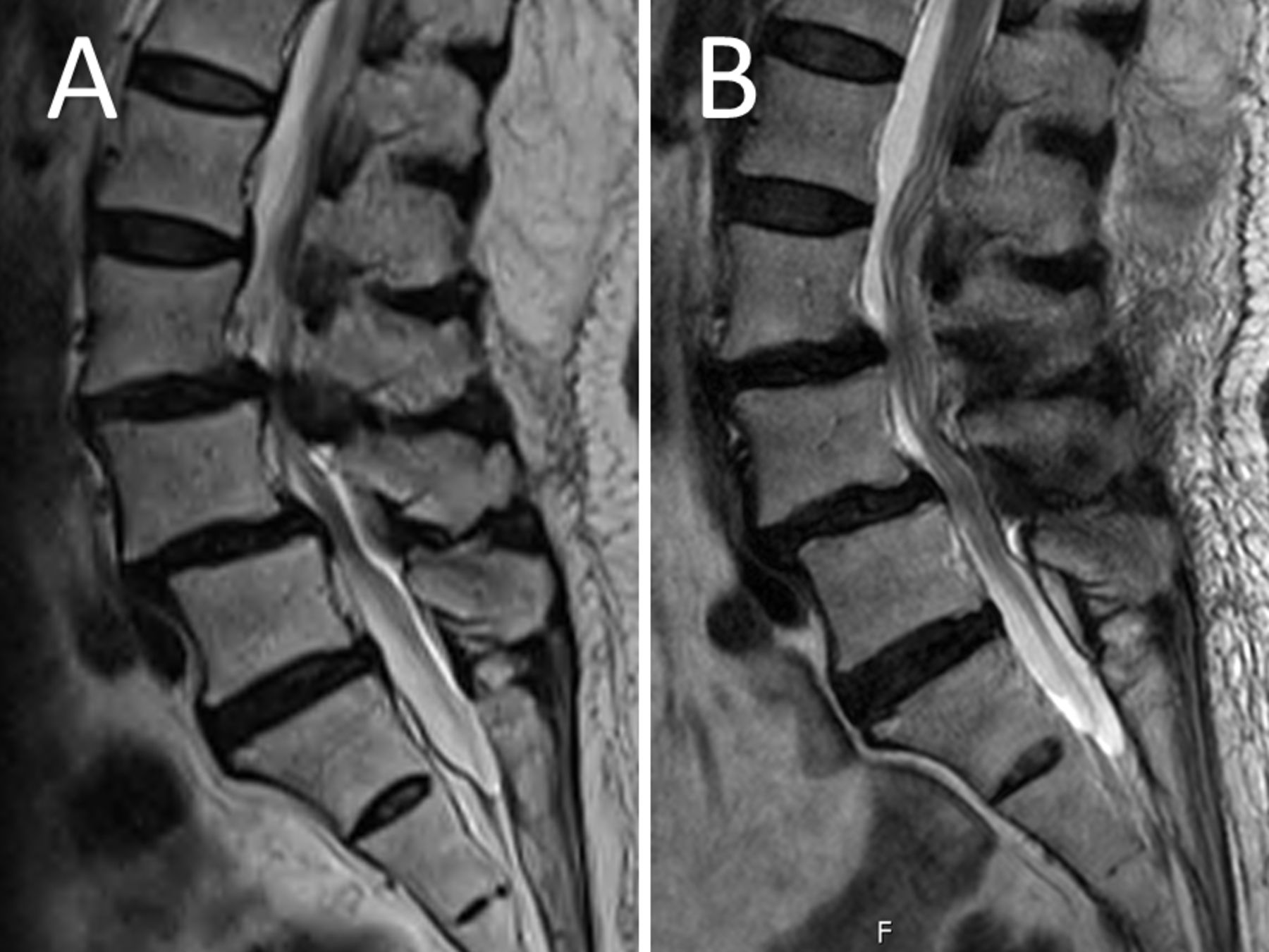
A 76-year-old woman presented with neurogenic claudication. MRI of the lumbar spine demonstrated significant spinal canal stenosis at L3/4 and L4/5 secondary to hypertrophy of the ligamentum flavum, facet joints, and disc bulging (Figure 3). An endoscopic right-sided hemi laminotomy (Matrix Endoscopy, 8.4 mm stenosis scope) with bilateral decompression was performed. A right-sided hemilaminotomy and medial facetectomy were performed with contralateral decompression. Postoperatively, the patient developed a right-sided foot drop (MRC 3). An MRI of the lumbar spine was performed on postoperative day 1 and did not demonstrate an identifiable structural cause for her ankle dorsiflexion weakness. There was satisfactory decompression of the L3/4 and L4/5 spinal canal and lateral recesses (Figure 3). She was examined by the primary surgeon (R.J.M.) at 6-week postoperative follow-up, where she had partial recovery of her right-sided ankle dorsiflexion weakness (MRC 4+).

(A) Preoperative magnetic resonance image (MRI) of the lumbar spine (sagittal) demonstrating canal stenosis at L3/4 and L4/5 with grade 1 anterolisthesis of L4 on L5. (B) Postoperative MRI of the lumbar spine (sagittal) demonstrating decompression of the spinal canal at L3/4 and L4/5 without an identifiable structural cause for her foot drop. High irrigation pressures (sustained >50 mm Hg) were deemed to be the cause of the neurological deterioration.
Mechanisms and Pathophysiology
Uniportal spine endoscopy requires continuous fluid insufflation to provide irrigation to control epidural bleeding and wash out debris, while also allowing distention of the potential space to maintain visibility of the surgical field.9,10 Irrigation also reduces the risk of electrocautery burns and infection.14 However, irrigation pressures during endoscopic spine surgery have been postulated to lead to postoperative headache, seizures, visual impairment, and autonomic dysreflexia, especially after incidental durotomy.12,13
Despite the increasing popularity of spinal endoscopic surgery, there remains a limited understanding of the fluid dynamics and pressure changes that occur as a result of continuous irrigation. Factors that may be involved include high pump pressures, high irrigation flow, dural tears, saline outflow obstruction, surgical duration, and anesthetic strategies. Higher body mass index has also been shown to have higher levels of tissue resistance and lead to higher fluid pressures.14
Saline outflow obstruction has been shown to cause significant increases in pressure in both intradural and extradural compartments at all levels of the neural axis, thus acting as a potential mechanism for irrigation-related neurological complications. Farshad et al conducted a human cadaveric study to measure intradural and extradural pressures at various levels of the neural axis.15 They found that backflow occlusion of the irrigation system led to a uniform increase in pressures across both intradural and extradural compartments at each level of the spine of around 30 to 40 mm Hg, including cervical extradural pressures. Furthermore, when a durotomy is present, irrigation may enter the intradural space and cause direct increases in pressures within the intradural compartment.15 Hong et al studied water dynamics during in vivo endoscopic spine surgery and found that proper placement of a rigid cannula was the primary factor in ensuring meaningful and regular distribution of water pressure as it maintained patency of water, decreased water pressure, and reduced infiltration to surrounding tissues.14 Additionally, increasing the pump pressure was linearly proportional to the increase in compartment pressures. Interestingly, the authors found that there was no difference in baseline pressures between interlaminar and transforaminal approaches.15
Despite this, the mechanism behind raised pressures and neurological deterioration remains poorly understood. When Soliman first described the technique termed “irrigation endoscopic decompressive laminotomy,” he paused the procedure for 3 minutes every 30 minutes to avoid prolonged fluid irrigation. Their theory was that prolonged irrigation fluid pressure could result in neurapraxia, in keeping with the same principle as tourniquet palsy in upper and lower limb surgeries.10 Neural tissue is particularly vulnerable, and excessive pressure may cause damage to surrounding neural structures.16 Separately, Amato et al theorized that neurological symptoms may be attributed to raised intracranial pressure (ICP) due to continuous saline infusion into the extradural space. The authors used swine models to measure ICP during endoscopic spinal surgery and found that occlusion of saline outflow channels led to a rapid rise in ICP.17 Postoperative raised ICP may then lead to headaches, seizures, and visual impairment.7,18 Higher irrigation pressures have also been theorized to cause meningeal irritation, leading to postoperative headache and neck pain.19,20 Other authors have postulated that the rates of incidental durotomies are higher than most surgeons report because many go unrecognized. They believe that neurological deterioration following irrigation is due to unrecognized durotomy, and the observed adverse events are due to the intradural spread of irrigation fluid, blood, and air.12,13
Review of the Literature
This literature review has revealed a range of neurological complications associated with fluid insufflation in endoscopic spine surgery.
Raised ICP
Raised ICP and subsequent neurological deterioration, including seizures, are a potential complication associated with fluid irrigation. Given that spinal cerebrospinal fluid (CSF) communicates freely with intracranial CSF, an increase in spinal extradural pressures from fluid insufflation compresses the thecal sac and shifts the CSF volume cranially, causing raised ICP.21 Additionally, the collapse of extradural spinal veins from fluid irrigation pressures increases intracranial blood flow, leading to raised ICP.22 Choi et al reported a 0.02% incidence of intraoperative seizures in a large cohort of 16,725 patients undergoing endoscopic spine surgery. Though rare, these seizures were often preceded by neck pain, which the authors suggested could be a prodromal sign due to its correlation with increased cervical epidural pressure and hence ICP.23 Raised ICP has also been associated with headaches, neck stiffness, gait disturbances, distal extremity paresthesia, and low back pain.24 Neck stiffness was the most prevalent symptom and, in the context of endoscopic lumbar surgery, was associated with increased cervical extradural pressure generated by continuous fluid infusion.25 Wu et al documented a case where raised ICP after transforaminal endoscopic lumbar spine surgery led to seizures and a lacunar infarct.26 Furthermore, a global survey by Vargas et al found that among 766 surgeons, 38% reported irrigation-related complications, with a subset observing seizures, nerve root injury, cauda equina syndrome, and autonomic dysreflexia due to the noxious stimulus of escaped irrigation fluid that migrated from the decompression site in the spinal canal.13 These findings collectively underscore the effect of fluid insufflation on raised ICP and subsequent neurological deterioration.
Durotomy-Related Complications
A durotomy represents a significant risk factor for severe neurological complications when coupled with fluid irrigation as the positive pressure can lead to the migration of fluid, air, or blood through the dural defect and into the subarachnoid space. Vargas et al reported 3 cases where durotomy-related complications led to subarachnoid hemorrhage, hydrocephalus, and diplopia. In 1 case, an incidental durotomy and the subsequent inflow of blood into the subarachnoid space led to blood within multiple intracranial compartments. The postoperative computed tomographic image was characteristic in the appearance of an arterial Fisher grade IV subarachnoid hemorrhage. Additionally, 2 other patients reportedly suffered intraoperative seizures, and 1 experienced cardiac arrest.13,27 The mechanism of cardiac arrest may be related to a durotomy-induced intradural spread of irrigation fluid, which elevates ICP, subsequently affecting the vagus nerve and its ability to innervate the heart.27 In Lewandrowski et al’s survey of 64,470 lumbar endoscopic surgeries, surgeons reported neurological complications of severe radiculopathy with dysesthesia, sensory loss, and motor weakness associated with incidental durotomy.12 Sandon et al described a case of a durotomy during endoscopic thoracic discectomy causing an intraoperative spinal fluid fistula, leading to raised ICP and subsequently an abducens nerve palsy.28 However, similar cases of neurological deterioration have arisen without a dural tear, as Zhang et al reported a case of non-aneurysmal subarachnoid hemorrhage without durotomy after an endoscopic transforaminal lumbar interbody fusion. The authors postulated that continuous extradural pressure from irrigation fluid increases the pressure of the extradural and intracranial veins, leading to the rupture of an intracranial vessel and causing subarachnoid hemorrhage. The raised ICP could also cause dilation and congestion of cerebral vessels, causing blood cell exudation, which results in intracranial hemorrhage.29
Spinal Subdural Hematoma
Although less common, spinal subdural hematomas due to high-pressure fluid irrigation have been documented, indicating another potential risk associated with fluid insufflation. Walbridge et al and Bae et al separately each presented a case in which a spinal subdural hematoma developed following high-pressure fluid irrigation during endoscopic spinal surgery. The authors postulated that their higher pressures of irrigation fluid could have led to accumulation of fluid within the subdural space. The pressure may have also contributed to injury of the bridging vessels between the dural and arachnoid membranes, leading to hematoma formation.30,31
Nonspecific Neurological Deficits
A range of nonspecific neurological complications following endoscopic spinal surgery has also been observed, with symptoms that may or may not be directly related to the pressure of irrigation fluid. In the survey conducted by Vargas et al, headaches, neck pain, and a broad array of other neurological symptoms were reported by 9.4% of surgeons using irrigation pumps.13 Compagnone et al conducted a detailed systematic review of complications associated with endoscopic spinal surgery and found that the incidence of neurological deficit and dysesthesia was 0.4% and 2%, respectively. However, the authors did not assess the potential mechanisms underlying such neurological deterioration.11
Discussion
There are limited reports of neurological complications due to fluid insufflation during endoscopic spinal surgery in the literature. Our current understanding regarding risks, potential complications, and pathophysiological mechanisms is limited to several theories without definitive evidence of their accuracy. Our literature review has shown that fluid insufflation has been associated with raised ICP and an increased risk of seizures.13,23–26 When continued to be used with an incidental durotomy, fluid insufflation can lead to the migration of fluid, air, or blood into the subarachnoid space, causing subarachnoid hemorrhage, hydrocephalus, and other focal neurological deficits.12,13,27,28
We describe 2 cases of transient weakness that resolved within 48 hours postoperatively, with 1 affecting the ipsilateral isolated nerve root and the other affecting the ipsilateral lumbosacral plexus. The third case represented a case of ipsilateral postoperative foot drop with partial resolution at the 6-week follow-up review. To the best of the author’s knowledge, such adverse events related to fluid insufflation affecting individual nerve roots or the lumbosacral plexus have not been documented in the literature. Although Compagnone et al’s systematic review described cases of postoperative neurological deficit, the authors do not provide detailed descriptions regarding the type of deficit, whether it was transient or permanent, or possible underlying mechanisms.11 Additionally, Walbridge et al and Bae et al each described a case of postoperative neurological deficit though this was associated with a spinal subdural hematoma.30,31 Similarly, other documented cases of neurological deterioration and deficit have all been associated with unintended durotomy or a structural cause identifiable on neuroimaging.
In the absence of an identifiable structural cause, there are several possible mechanisms that may lead to neurological deficits. Soliman believed that fluid irrigation could result in neurapraxia due to prolonged pressure on the nerve root, in a similar mechanism to the tourniquet palsy seen in limb surgery.10 It is possible that prolonged fluid insufflation at higher pressures in our cases may have caused transient axonal damage and hence postoperative weakness. Additionally, higher irrigation pressures may also cause microvascular damage to the small capillaries innervating the underlying neural structures, causing transient ischemic injury. This mechanism would be similar to the mechanism of subdural hematoma formation as described by Walbridge et al and Bae et al.30,31 A less likely explanation for the neurological deterioration seen in our cases may be related to incidental durotomy, as postulated by Lewandrowski et al. The authors suggested that the rates of incidental durotomies are higher than most surgeons report because many go unrecognized, and subsequent neurological complications may be a result of unrecognized small durotomy.12
Clinical Implications and Recommendations
Our analysis underscores the need for careful intraoperative monitoring of irrigation pressures and vigilant observation for early signs of neurological compromise. Standardized guidelines for pressure limits could help reduce the incidence of these complications. Although such guidelines are yet to be established, several authors have suggested that irrigation pressures be maintained below 30 mm Hg during surgery.7,10,32,33
Additionally, surgeons should ensure an adequate distribution and outflow of irrigation fluid to avoid raised irrigation pressures. Hong et al reported that proper placement of a rigid cannula was the primary factor in ensuring the effective distribution of fluid pressure and reduced infiltration to surrounding tissues.14 When backflow occlusion of the irrigation system occurs, Farshad et al found this led to a uniform increase in pressures across both intradural and extradural compartments at each level of the spine of around 30 to 40 mm Hg, including cervical extradural pressures.15 Kim et al proposed a technique where, rather than increasing the infusion pressure to obtain a clearer view, the authors attempted to facilitate fluid outflow by applying an extension or crosscut of the fascia incision through the working portal. A clear visual field obtained through smooth continuous irrigation can prevent the need for increased irrigation pressures.34
Surgeons should also aim to reduce the length of irrigation as much as practically possible. Joh et al suggested that shorter lengths of fluid insufflation could reduce the rate of irrigation-related complications. The authors postulate that the longer the irrigation time, the higher the probability of the epidural space filling with fluid, which would lead to decreased extradural compliance.25 Furthermore, surgeons should approach highly vascular areas such as the extradural space with additional care to reduce the incidence of unnecessary bleeding. Bleeding reduces visibility through the endoscope and requires higher irrigation pressures to achieve hemostasis and improve visibility.23 Therefore, avoiding unnecessary bleeding can assist in reducing irrigation pressures.
Limitations
This study’s primary limitation is its design as a case series, involving a small sample size, which restricts the generalizability of the findings. Additionally, the literature surrounding complications related to elevated fluid pressures in uniportal spine endoscopy is sparse. This gap underscores the challenge of establishing robust comparisons or context for the reported outcomes. Furthermore, while the study incorporates a literature review to explore the phenomenon, it lacks the comprehensive and methodologically rigorous approach characteristic of a systematic review, potentially leading to an incomplete synthesis of available evidence.
Future research directions should aim to address these limitations and advance the field. A deeper investigation into the impact of higher irrigation pressures on nerve root dysfunction is crucial for understanding the neurological implications of fluid insufflation. This could include studies exploring how specific pressure thresholds influence nerve viability or recovery. Additionally, developing strategies to minimize pressure accumulation during procedures, such as optimizing surgical techniques or refining equipment design, would be instrumental in enhancing safety. Research into defining optimal irrigation parameters, including flow rates and pressure thresholds, can assist in establishing standardized practices that mitigate the risk of pressure-related complications.
Conclusion
This review underscores that neurological deterioration, though uncommon, is a significant risk associated with fluid insufflation during spine endoscopy, with elevated ICP, durotomy-related injuries, and unintended fluid migration identified as primary risk factors. Our case series introduces additional complications not previously reported in the literature, including ipsilateral weakness and lumbosacral plexopathy linked to fluid irrigation pressures. Awareness of the potential impact of insufflation fluid pressure is critical, and surgeons should consider reducing these pressures when bleeding is minimal during endoscopic spine procedures. By understanding these mechanisms and incorporating preventive strategies, clinicians can mitigate risks and improve patient outcomes.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Research Ethics All patients provided written informed consent for their data to be included in this study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.