


Abstract
Background Despite its clinical importance, osteoporosis remains underdiagnosed, particularly in spinal surgery patients, where bone quality affects surgical outcomes. Existing screening methods are often costly or inaccessible, highlighting the need for a simpler alternative.
Objective The purpose of the present study was to assess the canal bone ratio (CBR) as a predictive tool for bone mineral density (BMD) in patients with lumbar degenerative diseases and establish a specific cutoff value for diagnosing osteoporosis.
Methods A retrospective analysis was conducted of 102 patients older than 50 years who underwent lumbar spine surgery at our institution from 2016 to 2024. Eligible patients underwent dual-energy x-ray absorptiometry (DXA), full-spine x-ray imaging, and computed tomography within 3 months before their surgery. CBR measurements were obtained by analyzing x-ray images for the inner and outer diameters of the femoral shaft 7 cm below the lesser trochanter. The Youden index based on T score thresholds from DXA scans determined the optimal cutoff value for diagnosing osteoporosis using CBR.
Results The cutoff value for CBR was 0.501, which was identified by analyzing BMD data from the lumbar spine and femoral neck regions. This cutoff demonstrated a strong correlation with low BMD scores, exhibiting a sensitivity of 0.656 and a specificity of 0.671 for identifying osteoporosis among the included patients. Additionally, CBR values negatively correlated with T scores and computed tomography-based Hounsfield units values obtained from lumbar and femoral regions, reinforcing its validity as a screening tool.
Conclusion CBR correlates with T scores from DXA and Hounsfield units values, establishing itself as a feasible and practical screening tool for osteoporosis in patients with lumbar degenerative disease.
Clinical Relevance CBR facilitates early intervention and improves management in populations at high risk for bone fragility.
Level of Evidence 3.
Introduction
In recent decades, the growing elderly population has increasingly required surgical interventions for spinal disorders.1 A major issue within this demographic is osteoporosis, a condition that remains underdiagnosed and undertreated. Despite the known risks, osteoporosis often goes unnoticed due to factors such as low health literacy, socioeconomic challenges,2,3 and, notably, insufficient proactive screening by health care professionals.4 For instance, a survey of 349 orthopedic and neurosurgeons revealed that only about one-fifth regularly assessed bone density in their patients, highlighting a statistical gap in standard care practices.5
In response to these challenges, opportunistic screening has emerged as a promising solution. This method utilizes routine spinal imaging, such as computed tomography (CT)-based Hounsfield units (HU)6 and magnetic resonance imaging (MRI)-based vertebral body quality scores,7 before spine surgery to improve osteoporosis screening rates. Moreover, dual-energy x-ray absorptiometry (DXA) remains the criterion standard.8,9 However, none of these options can be easily used for simple screening due to the high cost of the medical equipment involved. Typically, the diagnosis and treatment of spinal degenerative diseases require spinal x-ray imaging and CT/MRI.10 However, considering the limited availability of CT and MRI in low- and middle-income countries and the need for practical screening tools that do not increase radiation exposure or costs, this study focuses on the utility of the canal bone ratio (CBR) in diagnosing osteoporosis. The CBR, an x-ray–based measure, holds potential as a cost-effective alternative, offering comparative benefits in cost, accessibility, and diagnostic effectiveness.11,12 Full-length anterior-posterior and lateral x-ray imaging are essential for assessing alignment.13 Additionally, spine surgeons measure spinal and pelvic parameters to evaluate compensation of the pelvis and lower limbs, typically including the proximal femur. Preliminary evidence suggests that CBR provides an alternative to DXA for quick and accurate bone mineral density (BMD) measurements.
The present study aims to rigorously evaluate the predictive performance of CBR for bone density in patients with lumbar degenerative disease (LDD). We hypothesized that CBR can serve as a reliable indicator of bone density, potentially replacing DXA in clinical settings where it is unavailable. Our research seeks to establish specific cutoff values for CBR that correlate with osteoporosis, thereby enhancing the screening process and supporting better management of osteoporosis in spinal surgery patients.
Materials and Methods
Included Patients
We collected data from patients preparing for lumbar spine surgery at our institution between April 2016 and April 2024 who had undergone CT, MRI, and DXA. Eligible participants were those aged 50 years or older with lumbar spine imaging performed within 3 months before their surgery. We excluded individuals who had previous lumbar spine surgeries (such as posterior fusion or balloon kyphoplasty), those with spinal conditions (including tumors such as multiple myeloma and metastatic cancers, inflammatory diseases such as ankylosing spondylitis and tuberculosis, or significant scoliosis or deformities with a coronal Cobb angle greater than 30°), or those with severe vertebral fractures that hindered assessment. Basic demographic and clinical information, including age, gender, height, weight, body mass index (BMI), and the type of lumbar spinal disorder, was recorded.
Canal Bone Ratio
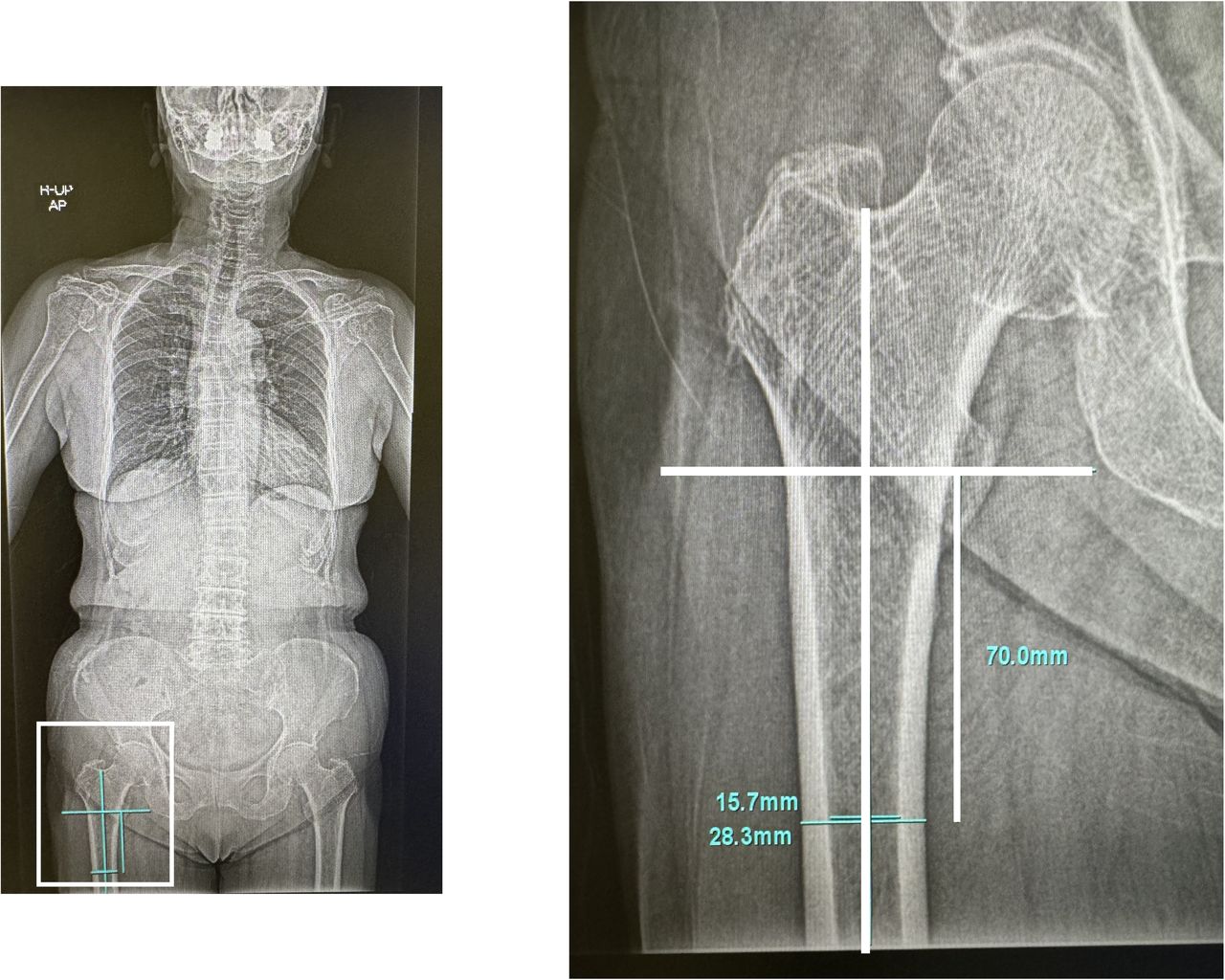
On whole-spine x-ray images, we marked a reference line perpendicular to the femoral shaft running through the center of the lesser trochanter. Lines were then measured 7 cm below this reference. At this height, the medulla-cortical ratio was measured as the canal-bone ratio CBR (inner diameter of the femoral shaft/outer diameter of the femoral shaft; Figure 1).14,15 Two spine surgeons measured CBR. They were blinded to BMD results during measurements. One of the surveyors repeatedly measured radiographs in random order after a 2-week interval to assess the intraobserver variance. Moreover, the interobserver variance among the 2 surveyors was also assessed by the intraclass correlation coefficient (ICC).

Method for measuring canal bone ratio (CBR). This figure illustrates the measurement of CBR using the femoral shaft, with an inner diameter of 15.7 mm and an outer diameter of 28.3 mm. The calculated CBR is 0.554 (CBR = inner diameter/outer diameter).
Dual-Energy X-Ray Absorptiometry
Our research group followed the manufacturer’s recommendations and performed standard analysis procedures for the spine and hip on all patients. We used DXA to measure the BMD of the lumbar spine (L1–L4) and the left hip. BMD is defined as bone mineral content (BMC) divided by the projected area of the scanned image, ie, BMD = BMC/area (g/cm²). Patients lie on their backs on the DXA table, with their legs elevated for lumbar spine measurements and their feet placed in a brace for hip measurements. A low-dose x-ray beam is passed through the bones, and BMD is measured by calculating BMC divided by the bone area. The entire procedure takes approximately 10 min.
Using the Horizon W system (Hologic, Inc.), DXA scans provided BMD scores expressed as T scores for the lumbar spine and femoral neck. A specialist radiologic technologist and the automated densitometry software determined these scores. T scores were used to classify bone status into osteoporosis (T score < −2.5), osteopenia (T score < −1.0), and normal (T score ≥ −1.0).16
In this study, we divided patients into 2 groups—an osteoporosis group and a normal group—based on a T score of −2.5 to measure the CBR cutoff value.
Measurements of HU Value
HU values were derived from presurgery CT scans of the L1 to L4 vertebrae using established methods from earlier studies. Scans were performed on 1 of 4 types of Siemens helical CT scanners.9,17 Parameters included a 120 kVp tube voltage, 280 mA current, and a slice thickness of 3.0 mm at intervals of the same width. We focused on 3 specific areas per vertebra: immediately below the superior endplate, the vertebral body’s center, and just above the inferior endplate. The most distinct cancellous and cortical bone areas were targeted for region of interest selection. After standardizing the placement of the region of interest to exclude cortical bone, the average HU values were calculated using the picture archiving and communication system.
Statistical Analysis
Data are presented as mean ± SD or as number (%) of patients. The Kolmogorov-Smirnov test confirmed the normal distribution of the continuous variables. To establish intra- and interrater reliability, the ICC was calculated for the CBR measurements using a 1-way random effects model and absolute agreement type. We used the χ 2 test to assess the associations between categorical variables across different groups. We employed t tests and the Mann-Whitney U test to analyze continuous variables. Although the Kolmogorov-Smirnov test confirmed a normal distribution, the correlation between variables was investigated using Spearman’s rank correlation coefficient (r) instead of Pearson’s correlation. This decision was made due to potential outliers and the ordinal nature of some variables, which may not fully meet the assumptions of Pearson’s correlation. The area under the curve (AUC) was evaluated using receiver operating characteristic (ROC) analysis. Furthermore, the cut-off value for CBR corresponding to a T score of −2.5 SD for diagnosing osteoporosis was determined based on the Youden index. Data were analyzed using IBM SPSS Statistics software (version 23.0, IBM Corp., Armonk, NY, USA). A P value of <0.05 was considered statistically significant.
Results
We studied 102 patients (49 men and 53 women) with an mean age of 73.3 years. The mean height was 157.2 cm, weight was 60.0 kg, and the mean BMI was 24.2 kg/m². Bone density measurements indicated a lumbar BMD of 0.978 and a femoral neck BMD of 0.652. The average T scores for the lumbar and femoral neck regions were 0 and −1.6, respectively. Based on T scores, 30 patients had normal bone density, 40 had osteopenia, and 32 had osteoporosis. Measurements of the femoral shaft revealed an inner diameter of 14.1 cm and an outer diameter of 28.7 cm, resulting in a CBR of 0.491 (Table 1). In CBR, the intra- and interrater reliability, as measured by the average ICC, were statistically significant, with values of 0.933 (0.806–0.977, P < 0.001) and 0.955 (0.856–0.985, P < 0.001), respectively.
Baseline characteristics of patients (N = 102).
Table 2 presents the Spearman correlation matrix between CBR and HU at lumbar levels L1 through L4. Significant negative correlations were found at all individual levels (L1–L4), with correlation coefficients ranging from −0.290 to −0.385, indicating that lower bone density is associated with higher CBR values. Strong positive correlations were observed among HU measurements across the lumbar levels, particularly between L1 and L2 (r = 0.867) and L2 and L4 composite (r = 0.905), suggesting consistent density patterns across these segments. All reported correlations were statistically significant, with P values less than 0.05.
Spearman product-moment correlation matrix between HU at L1−L4 and VBQ scores.
Table 3 outlines the Spearman correlation matrix among CBR and T scores at different anatomical sites. There are significant negative correlations between CBR and lumbar T score (r = −0.425), femoral neck T score (r = −0.338), and low T score (r = −0.361), indicating that higher CBR is associated with lower bone density scores. Although a correlation was observed between CBR and T score, no statistically significant difference was found between CBR and age (Figure 2).

Correlation graphs between (A) CBR and low T score and (B) CBR and age. Although a correlation was observed between CBR and T score (r = −0.361, P < 0.001), there was no correlation between CBR and age (r = 0.164, P = 0.100). Abbreviation: CBR, canal bone ratio.
Spearman product-moment correlation matrix between lumbar T score, femoral neck T score, low T score, and HU values.
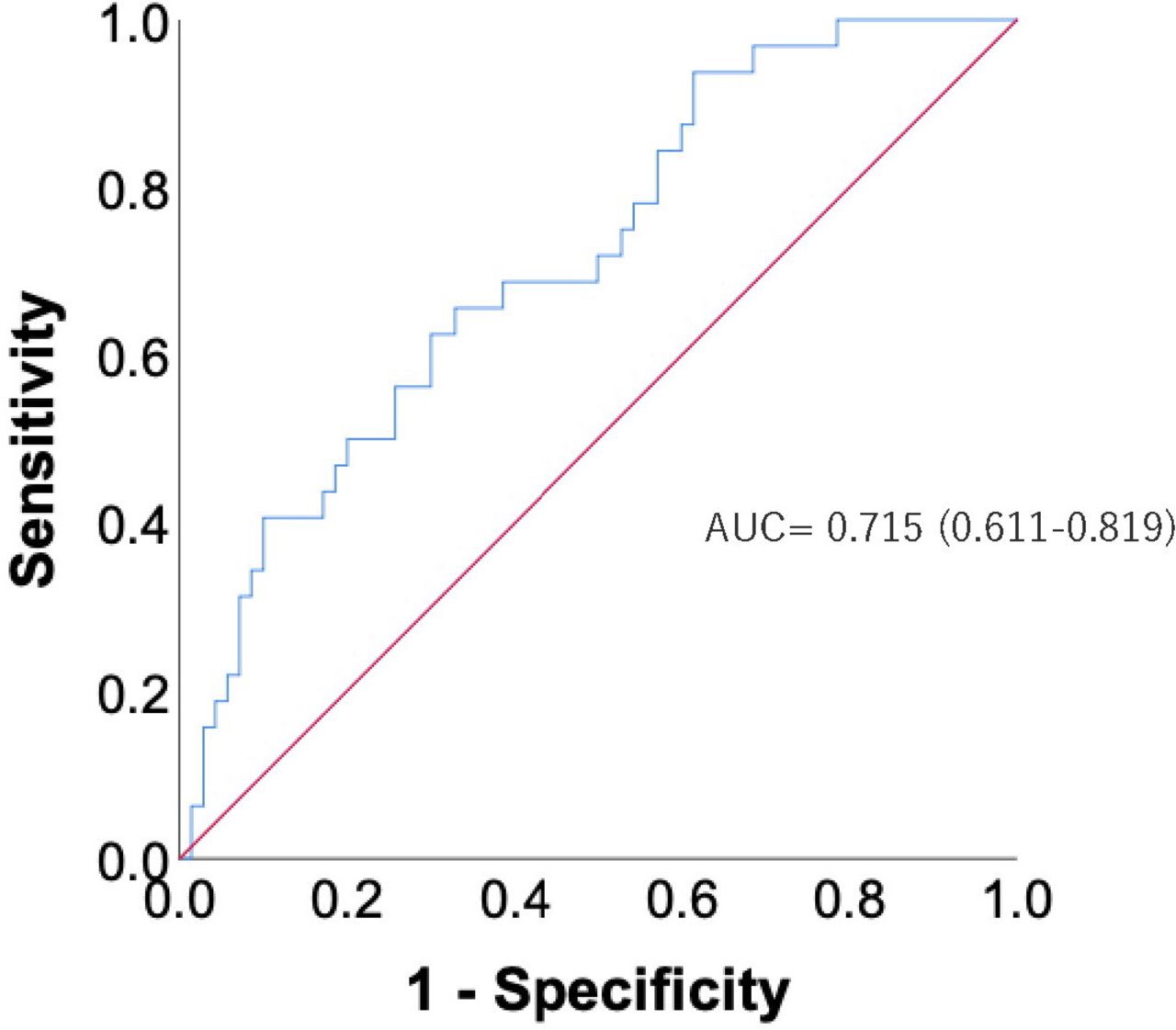
Patients were classified as osteoporotic if their T score was −2.5 or lower and nonosteoporotic if it was higher. Table 4 compares the clinical outcomes between these 2 groups. Significant differences were observed in several parameters, including age, sex distribution, height, body weight, BMI, and BMD measurements at both lumbar and femoral neck sites. Osteoporotic patients were generally older, shorter, lighter, and had significantly lower BMD and T scores. Additionally, osteoporotic patients had higher CBR. Figure 3 shows the AUC of CBR in the presence and absence of osteoporosis determined by receiver operating characteristic curve analysis.

ROC curve for osteoporosis in patients with lumbar degenerative disease. The results of the ROC curve analysis and the AUC of CBR-7 for the proximal femora are shown. Abbreviations: AUC, area under the curve; CBR, canal bone ratio; ROC, receiver operating characteristic.
Comparison of clinical outcomes in osteoporotic vs nonosteoporotic patients.
Table 5 presents the CBR cutoff values for distinguishing osteoporotic from nonosteoporotic patients based on their BMD. A CBR cutoff of 0.501 was evaluated, showing an AUC of 0.715, with a confidence interval (95% CI) ranging from 0.611 to 0.819. This cutoff demonstrated a sensitivity of 0.656, specificity of 0.671, accuracy of 0.667, recall of 0.656, and precision of 0.477. The distribution of patients above and below this cutoff indicated that 21 osteoporotic patients had a CBR greater than 0.501 (Table 6). In comparison, 47 nonosteoporotic patients had a CBR less than 0.501, illustrating the effectiveness of this threshold in clinical assessment.
Cutoff values for CBR: sensitivity, specificity, accuracy, recall, precision, and AUC with 95% CI.
Osteoporotic and nonosteoporotic patients by CBR.
Discussion
This study represents 1 of the first to evaluate femoral radiographic parameters, specifically the CBR, for assessing bone density in patients with LDD. Building on the pioneering work of Ellis Barnett et al,18 who utilized proximal femoral cortical bone thickness on x-ray images to evaluate bone density, our findings indicate a strong correlation between CBR and bone density measures, confirming the clinical utility of radiographic parameters beyond traditional sites to include the spine, particularly for patients with LDD. An easily accessible screening tool for osteopenia or osteoporosis using plain radiographs is of great importance for spine surgeons to mitigate potential surgical risks during spinal fusion surgery due to osteopenia and osteoporosis. In our preoperative evaluation of patients with LDD using DXA, 31% of patients had osteoporosis and 29% had normal bone density. Patients with osteoporosis are at a higher risk of complications related to spinal instrumentation, with reports indicating that half of the osteoporotic patients surgically treated face surgery-related complications after spinal operations, compared with less than a quarter of patients with healthy bone quality.19 In patients with reduced bone density, complications reported include pedicle screw loosening, pseudarthrosis, proximal junctional kyphosis, and higher rates of implant failure.20–22
Considering the routine use of whole spine, lumbar, and hip x-ray imaging in clinics and hospitals, CBR provides a practical and cost-effective approach to osteoporosis screening. Liu et al showed that measurements of the CBR at 7 cm (CBR-7) and 10 cm (CBR-10) below the lesser trochanter in 216 patients (aged 18 years or oder) who underwent total hip arthroplasty (THA) are effective screening tools for osteoporosis.15 Liu et al also reported that the measurement of CBR-7 and CBR-10 was similarly valid as a screening tool for osteoporosis in 81 pre-THA patients.14 However, it is important to note that the presence of hip implants, such as those found in patients who have undergone THA, may significantly impact the accuracy of CBR measurements. Implants can alter the radiographic appearance of the femur, potentially leading to inaccurate CBR values. Therefore, the use of CBR in patients with hip replacements should be approached with caution, and alternative methods of assessing bone density may be necessary for these individuals.
This study utilized whole spine x-ray imaging instead of the standard anteroposterior (AP) hip view for several reasons. First, whole spine x-ray images are more commonly taken in patients with LDD as part of their routine evaluation. Utilizing these existing images allows for opportunistic screening for osteoporosis without subjecting the patient to additional radiation exposure. Second, whole spine x-ray images provide a broader view, including the proximal femur and other relevant anatomical structures. This can be valuable in comprehensive patient assessments, particularly in spinal surgery planning. Although the standard AP hip view is traditionally used for evaluating hip bone density, whole spine x-ray images offer a practical alternative in scenarios where additional imaging is not feasible or desirable.
Wang et al conducted a study involving 102 adult spinal deformity patients (mean age 63.3 years) and demonstrated the effectiveness of measuring CBR-7 for osteoporosis screening. This metric showed a strong negative correlation with bone density.23 In our study, we conducted evaluations using CBR-7. because whole spine x-ray images often did not capture up to 10 cm below the lesser trochanter, preventing assessment with CBR-10. Our analysis found the cutoff value for diagnosing osteoporosis with CBR-7 to be 0.501. Rohe et al also reported that the cutoff values for CBR-7 or CBR-10 were 0.49 or 0.47 for osteopenia and 0.51 or 0.50 for osteoporosis.15 The determination of the CBR cutoff value at 0.501 aligns with the findings from similar studies and offers novel insights into the clinical applicability of CBR in diagnosing osteoporosis. This cutoff value demonstrated a sensitivity of 0.656 and a specificity of 0.671, indicating its practical utility in clinical settings. DXA, CT, and MRI have been reported as useful tools to assess BMD, but cost and accessibility may be limiting factors, especially in resource-limited settings. However, the primary objective of employing CBR is not to replace these advanced imaging techniques but to provide a supplemental tool that allows for the early identification of osteoporosis. Early diagnosis and treatment of osteoporosis are crucial, as they can significantly reduce the risk of complications later, particularly in patients who may not have immediate access to MRI or CT. This early intervention is essential, as it focuses on preventing osteoporosis progression rather than diagnosing the condition only when surgery is imminent. Moreover, after spinal fusion surgery, accurately assessing bone density using DXA or HU becomes challenging due to interference from inserted implants. However, the CBR can be evaluated using x-ray imaging, making it feasible for routine clinical use to monitor the progression of osteoporosis. The clinical significance of this cutoff value lies in its potential to facilitate early intervention and targeted treatment in patients at high risk for osteoporosis, thereby potentially reducing the incidence of implant-related complications after spinal fusion surgery.
Despite its strengths, this study has several limitations. The sample size was relatively small, which may have limited the generalizability of the findings. The retrospective design could have introduced selection biases and restricted the ability to establish causality between CBR values and bone density outcomes. Additionally, the study relied on x-ray image measurements for CBR, which, while practical, might not have captured the nuanced details of bone quality that more advanced imaging techniques could provide. Also, using a single center for data collection may have reflected specific demographic and clinical practices not applicable to other settings. Furthermore, as mentioned earlier, the presence of hip implants can interfere with the accuracy of CBR measurements, limiting its applicability in patients with hip replacements. This factor is crucial as it underscores the need for careful consideration and potentially the development of alternative screening tools or methods for this specific patient population. Finally, the cutoff values for CBR used in this study were derived from the study population, which might not be directly transferable to other populations without further validation. As with any opportunistic screening tool, CBR should be seen as a preliminary indicator that warranted further investigation through more definitive diagnostic approaches. It is essential to recognize that opportunistic screening is not a substitute for a comprehensive evaluation, particularly in complex cases where multiple factors influence bone health.
Conclusion
CBR was a significant predictor of BMD in patients with spinal disorders. We established a cutoff value of 0.501 for diagnosing osteoporosis using CBR, which can enhance the screening process for this condition and is a valuable tool for early intervention and management in high-risk populations due to bone fragility. Furthermore, CBR may serve as a practical diagnostic screening alternative to DXA following spinal fixation surgeries, offering a method for monitoring bone density changes postoperatively. Future research should validate these findings through large-scale prospective studies and explore the integration of CBR into routine clinical practice to optimize the management of osteoporosis in patients with spinal disorders. Additionally, focusing on the changes in CBR values after spinal fixation surgeries may also be necessary to understand the impact of surgery on bone health.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This study was conducted by ethical standards and received approval from the Ethics Committee and the Profit Reciprocity Committee (reference number 24R-022).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.