


Abstract
Background Endoscopic unilateral laminectomy for bilateral decompression (ULBD) is gaining attention as a minimally invasive procedure for treating spinal stenosis. However, comprehensive studies on its outcomes remain limited.
Purpose This study aims to evaluate the changes in radiologic parameters and clinical outcomes associated with endoscopic ULBD for treating spinal stenosis.
Methods A retrospective study was conducted on 53 patients with central lumbar spinal stenosis who underwent endoscopic ULBD decompression surgery. Pre- and postoperative visual analog scale and Oswestry Disability Index scores were collected to assess the impact on activities of daily living. Parameters such as operation time, intraoperative blood loss, postoperative drainage volumes (first and second day), total hospital stay, and postoperative hospital stay were recorded. Additionally, pre- and postoperative imaging changes were documented, and MacNab functional scores were evaluated at 6 months postoperatively to assess clinical efficacy.
Results No nerve injuries occurred during the operation. Two cases of cerebrospinal fluid leakage were successfully treated with pressure dressings, and no postoperative complications such as incision infection or dehiscence were observed. At 6-month follow-up, postoperative visual analog scale scores and Oswestry Disability Index showed significant improvement compared with preoperative levels (P < 0.05). Postoperative lumbar computed tomography images revealed a statistically significant enlargement in the anterior-posterior diameter of the spinal canal and the diameter of the bilateral lateral recesses (P < 0.05). All patients experienced either improvement or resolution of clinical symptoms. The MacNab functional scores at the 6-month follow-up indicated excellent outcomes in 37 cases, good in 15 cases, and fair in 1 case, resulting in an overall good rate of 98.11%.
Conclusions This study demonstrates that endoscopic ULBD can provide favorable outcomes for single-segment central lumbar spinal stenosis under local anesthesia at a relatively low cost.
Introduction
Lumbar spine stenosis (LSS) is a common clinical condition1 with various causes that lead to a reduction in the diameter of the lumbar spinal canal, resulting in compression of the dural sac, nerve roots, and other neurological dysfunctions.2 The main clinical symptoms include low back pain with radiating pain in the lower limbs, neurogenic intermittent claudication, and more, which severely affect the patient’s quality of life.3 Current treatments for LSS primarily include conservative treatment and surgical treatment,4 but surgical treatment should be considered for only those who are not satisfied with more than 3 months of conservative treatment or those who experience significant low back pain and require immediate relief.5 In the treatment of LSS, traditional spinal decompression surgery is effective. It is performed under direct vision to decompress the spinal canal, increasing the space for the dural sac and nerve roots and achieving satisfactory clinical outcomes.6 However, the incision is large, and the muscle tissue needs to be stripped layer by layer during the operation, which damages the posterior ligament complex of the vertebrae. Postoperative scar tissue hyperplasia often leads to persistent low back pain.
Traditional spinal canal decompression surgery or minimally invasive spinal canal decompression surgery, including microscopic and unilateral biportal endoscopic (UBE) discectomy,7 all require general anesthesia. With an aging population, the proportion of elderly patients visiting hospitals for spinal diseases is increasing.8 Many of these patients have comorbid conditions such as hypertension, diabetes, and heart disease (eg, postcoronary stent placement and postpacemaker placement), increasing anesthesia risk and requiring higher standards from the anesthesia team. However, endoscopic unilateral laminectomy for bilateral decompression (ULBD) can be performed under local anesthesia and mild sedation, which can not only reduce the damage caused by general anesthesia to the patient but also allow patients with poor cardiopulmonary function who cannot tolerate general anesthesia to reduce the discomfort caused by LSS through surgical treatment.
The miniaturization, visualization, and intelligence of medical technology have become the development trend of the future, with minimally invasive spinal endoscopy technology serving as the future trend in spinal medical treatment. With the current development of technology, endoscopic ULBD is gradually becoming 1 of the main treatment methods for LSS.9 The decompression process is completed under the endoscope, allowing precise control of range and depth. Tissue stripping is minimized compared with unilateral biportal spinal endoscopy, preserving median structures like the articular process joint and paraspinal muscles, thus preventing postoperative lumbar instability.10 The present study reviews and analyzes data from patients with LSS treated with endoscopic ULBD between August 2017 and August 2023 in our department. We sought to explore the clinical efficacy of endoscopic ULBD in treating LSS.
Materials and Methods
Patients
We performed a retrospective study of 53 consecutive patients who underwent bilateral decompression surgery for lumbar central spinal stenosis between January 2017 and December 2023. Patients with diagnosed LSS confirmed by clinical symptoms and radiographic examinations were included. Patients with severe comorbidities, prior spinal surgeries, or other spinal pathologies were excluded.
Informed consent was obtained from all patients participating in the study so that their data could be used for research purposes. In addition to indicating their consent by responding to the invitation, all participants provided written informed consent.
Surgical Techniques
The following methods were followed for endoscopic unilateral laminectomy for bilateral decompression in degenerative lumbar spinal stenosis:
Patient positioning: Patients were placed in a prone position with a split pad to elevate the chest and iliac crest.
Localization and marking: Under C-arm x-ray guidance, the responsible segment, upper and lower pedicles, as well as the median line of the spinous process were located and marked.
Preparation: The surgical field was disinfected, and a 3M skin film was applied to prevent the drapes from being soaked by irrigation fluids during surgery.
Anesthesia: Local anesthesia was administered at the puncture point with a mixture of 1% lidocaine and 10 mL: 20 mg ropivacaine diluted in half, using 2 to 3 mL for injection with a long needle, followed by the infiltration of anesthetic along the puncture path with 8 to 10 mL of mixed solution. For patients without contraindications, dexmedetomidine intravenous anesthesia was used to alleviate pain and reduce anxiety during the procedure.
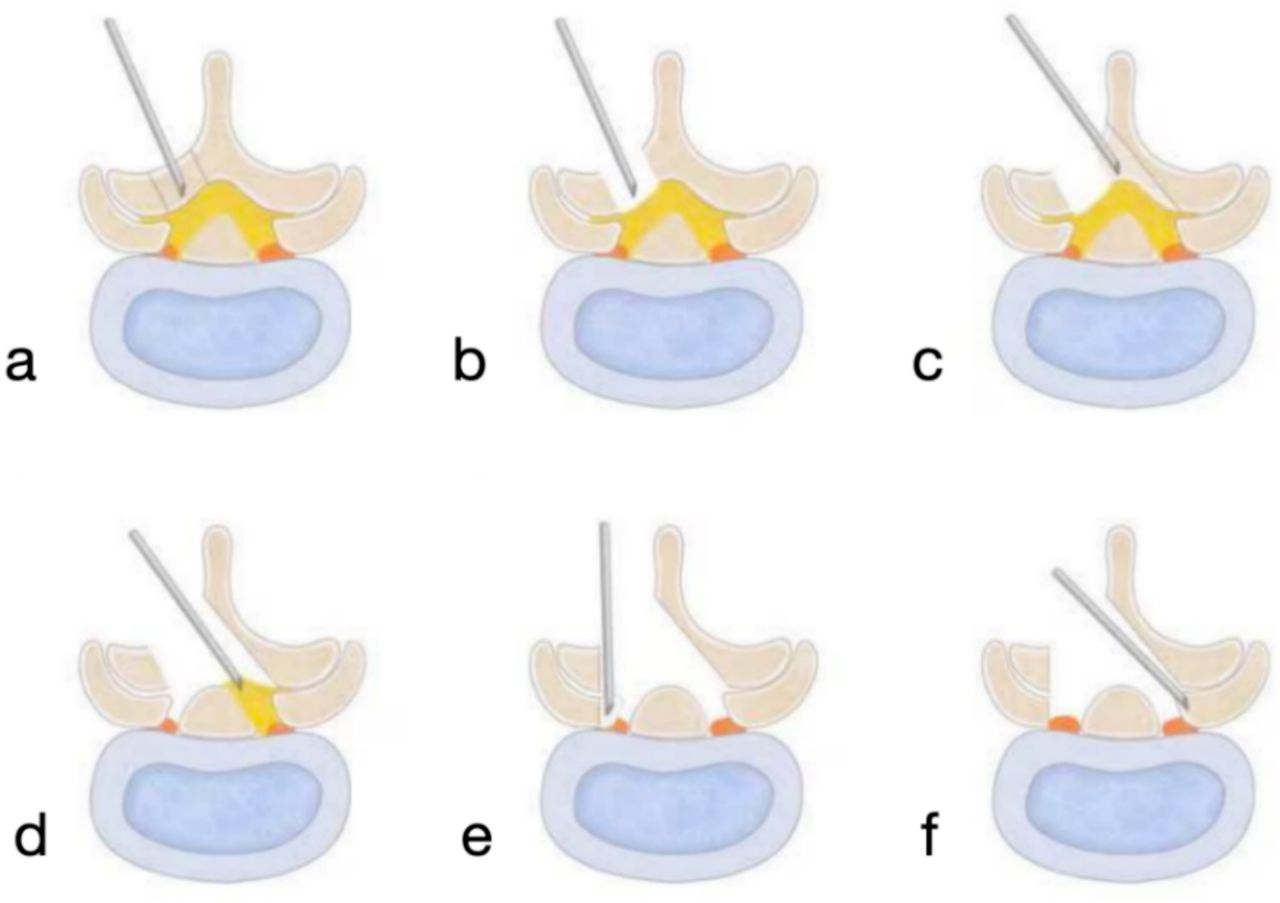
Channel implantation and lumbar laminar decompression: A 0.7-cm skin incision was made at the marked point to insert the working channel, maintaining preset lateral and craniocaudal angles according to preoperative lumbar CT. With soft tissue gaps expanded, a sequential dilator was used to create the working channel. Bipolar spherical radiofrequency ablation electrodes were employed to meticulously separate the soft tissues, thereby revealing the vertebral lamina. The decompression steps are shown in Figure 1. After confirming nerve root decompression and hemostasis, the working channel was removed. A negative pressure drainage tube was placed at the inferior aspect of the wound, which was then closed with sutures, and a pressure bandage was applied (Figures 2 and 3).

(a) C-arm-guided localization of the upper articular process of the affected lumbar segment. The working channel is positioned parallel to the intervertebral space and extends to the edge of the lamina. (b) Removal of the ipsilateral lamina up to the attachment of the ligamentum flavum using an endoscopic circular saw or osteotome. (c) Partial resection of the spinous process base, contralateral lamina, and the contralateral facet joint to fully expose the ligamentum flavum. (d) Bilateral removal of the ligamentum flavum, followed by exploration of the central spinal canal and both bilateral nerve roots. (e) Longitudinal resection of the medial aspect of the ipsilateral facet joint to decompress the lateral recess and the ipsilateral intervertebral foramen. (f) Decompression of the contralateral lateral recess up to the contralateral pedicle, allowing for the free exploration of the contralateral nerve root.

Case presentation of a 42-year-old woman with L5 to S1 lumbar spinal stenosis, presenting with a 3-month history of lower back pain and right lower limb radiculopathy, treated with endoscopic unilateral approach bilateral decompression. (a and b) Preoperative lumbar spine radiographs in anteroposterior and lateral views. (c and d) Preoperative dynamic lumbar spine radiographs in flexion and extension. (e and f) Preoperative magnetic resonance imaging demonstrating L5 to S1 lumbar spinal stenosis. (g and h) Preoperative computed tomography (CT) images confirm L5 to S1 lumbar spinal stenosis. (i) Postoperative lumbar spine CT image obtained 3 days after surgery.

Endoscopic unilateral approach bilateral decompression procedure. (a and b) C-arm guided placement of the working channel in anteroposterior and lateral views. (c) Hemostasis is achieved using a bipolar spherical radiofrequency ablation electrode. (d) Endoscopic lamina removal using a circular saw. (e) Endoscopic management of the lateral recess using an osteotome. (f) Further lamina removal using a Kerrison rongeur under endoscopic visualization. (g) Resection of the ligamentum flavum using specialized forceps. (h) Endoscopic view of the fully decompressed nerve root.
Radiographic Analysis
To minimize radiation exposure, standard posterior, anterior, and lateral view radiographs were used only when functional x-ray images were insufficient for study interpretation. Three-dimensional computed tomography (CT) images in the axial, sagittal, and coronal planes were obtained both preoperatively and at the 3-day and 6-month follow-up visits. Lumbar spine stability was measured on lumbar spine radiographs to determine the feasibility of simple decompression. The anteroposterior diameter of the spinal canal and the diameter of the lateral recesses at the surgical segment were measured on 3-dimensional CT images. All measurements were independently obtained by 2 experienced physicians on our team, and the final values were the average of the 2 measurements.
Statistical Analyses
Data were collected from electronic medical records and patient management questionnaires. Questionnaires were sent to patients along with a letter explaining the purpose of the study and the role of their participation. Data were collected from the preoperative period to 6 months postoperatively. The evaluation included the patient’s standing time and walking distance before and after surgery, pain and functional improvement, surgical duration, intraoperative blood loss, first and second postoperative day drainage volumes, total hospital stay, and postoperative hospital stay. Pre- and postoperative changes in lumbar CT imaging were recorded. Clinical outcomes were quantified using the visual analog scale (VAS; 0–10), Oswestry Disability Index (ODI; 0%–100%), and modified MacNab criteria (excellent, good, fair, and poor) at 3 days and 6 months postoperative follow-up. Statistical analysis was performed using χ 2 tests and independent sample t tests with STATA statistical software, with a P value of less than 0.05 considered statistically significant.
Results
All patients successfully completed the operation. The duration of the operation ranged from 65 to 295 minutes (mean 187.59 ± 10.51 minutes), and intraoperative blood loss ranged from 20 to 100 mL, averaging 47.27 ± 5.39 mL. The volume of negative pressure drainage on the first postoperative day ranged from 10 to 100 mL, averaging 44.55 ± 4.20 mL, while on the second postoperative day, it ranged from 5 to 30 mL, averaging 15.00 ± 1.71 mL. The total hospital stay ranged from 5 to 15 days, averaging 9.32 ± 0.54 days; the postoperative hospital stay ranged from 3 to 8 days, averaging 5.18 ± 0.28 days. None of the patients experienced cauda equina or nerve root injury during surgery, and although 2 cases of cerebrospinal fluid leakage occurred, they were well managed with bed rest positioning and pressure dressing, and no complications such as wound infection or dehiscence occurred. Postoperative follow-up from 6 to 12 months showed that the mean VAS score was 7.00 ± 0.35 before surgery, decreased to 4.32 ± 0.30 three days after surgery, and further decreased to 2.68 ± 0.24 six months after surgery. The mean ODI score was 50.91 ± 3.30 before surgery, dropped to 37.91 ± 2.04 three days after surgery, and further decreased to 30.95 ± 1.74 six months after surgery. Both VAS and ODI scores were significantly lower than before surgery (P < 0.05) (Table 1).
Patients underwent CT before and on the second day after surgery to measure the diameter of the anteroposterior and bilateral lateral recesses, assessing the improvement in imaging after lumbar spinal decompression surgery. The mean anteroposterior diameter of the spinal canal was 77.82 ± 7.82 mm before surgery and increased to 143.91 ± 8.25 mm after surgery; the diameter of the bilateral lateral recesses averaged 32.82 ± 3.94 mm before surgery and 52.91 ± 5.81 mm after surgery, indicating that the anteroposterior diameter of the spinal canal and the bilateral lateral recesses were enlarged (P < 0.05) (Table 2). The functional results of the lumbar MacNab score 6 months after surgery were excellent in 37 cases, good in 15 cases, and fair in 1 case, with a good and excellent rate of 98%.
Pre- and postoperative VAS and ODI comparisons.
Pre- and postoperative lumbar spinal canal diameter comparisons.
Discussion
LSS is a degenerative condition affecting the entire spinal motion segment and is 1 of the most prevalent spinal disorders.1 Prolonged weight-bearing and lumbar degenerative changes contribute to intervertebral disc degeneration, leading to spinal instability and increased pressure on the facet joints.11 The ligamentum flavum, attached to the lateral recess and joint capsule of the facet joints, can thicken significantly, potentially protruding into the lateral recess and compressing nerves.12 These phenomena, occurring individually or in combination, lead to LSS. This condition manifests as a reduction in spinal canal volume across all dimensions, resulting in nerve compression that causes low back pain, radiating limb pain, and intermittent claudication.2
Traditional lumbar decompression surgery removes the lamina and posterior spinal ligament complex (supraspinal ligament, interspinous ligament, ligamentum flavum, and joint capsule), increasing the risk of lumbar instability and degeneration.13 Spinal fusion surgery may result in epidural scar adhesions due to the close proximity of paravertebral soft tissue to the epidural space, potentially causing postoperative nerve root or cauda equina entrapment and related symptoms.14 Open surgery on obese patients requires deeper incisions due to adipose tissue accumulation, increasing tissue separation and muscle stripping, which may lead to postoperative complications like fat necrosis and impaired wound healing.15 Spinal endoscopy provides a broad field of view, minimizes trauma and blood loss, and significantly improves postoperative wound healing. This study included 53 patients, of whom 5 (9.43%) were obese (body mass index >3016). The MacNab functional scores at 6 months postoperatively were excellent, demonstrating good clinical efficacy, high efficiency, and high-quality treatment outcomes for LSS.
Studies have shown that traditional, microscopic, and endoscopic decompression surgeries effectively treat LSS with satisfactory outcomes.17 The trend toward minimally invasive and endoscopic spinal surgery has led to microscopic and endoscopic techniques gradually supplanting traditional open surgery. Microscopic decompression, while similar to minimally invasive traditional open surgery, utilizes air as a medium and requires a larger operating space for direct visualization. This approach has a more significant impact on the posterior paraspinal muscles. Microscopic surgery necessitates extensive removal of the ligamentum flavum and lamina, potentially compromising the biomechanical integrity of the vertebrae. This approach may lead to complications such as dural adhesions due to manipulation of the dura mater and associated nerve roots.18 Endoscopic techniques such as UBE combine the benefits of both microscopy and single-channel endoscopy, with a wide surgical field, large operating space, and high flexibility in the operation of decompression tools, and they have shown advantages in many medical centers.19 However, UBE relies on high-speed grinding drills to remove the vertebral plate under the microscope to achieve decompression, which is expensive. One hundred and eighty-one cases of lumbar spinal decompression under UBE were completed in our department in 2023 to 2024, with an average hospitalization cost of ¥38,712.35. However, the average hospitalization cost for the 53 patients in this study was only ¥12,753.74, only one-third of the UBE costs.
Both traditional and minimally invasive spinal canal decompression surgeries, including microscopic and UBE, typically require general anesthesia. The aging population has significantly increased the number of elderly patients requiring spinal surgery.7 In this study of 53 patients, 24 (45.28%) were older than 60 years, and 6 (11.32%) were older than 80 years. Due to decreased cardiopulmonary function and vascular elasticity with age, elderly patients have reduced regulatory function of blood pressure and heart rate during surgery, leading to a higher risk of hemodynamic fluctuations and greater demands on the anesthesia team.20 Age-related declines in cardiopulmonary function and vascular elasticity often present challenges during surgery for elderly patients. These factors reduce the regulation of blood pressure and heart rate, increasing hemodynamic fluctuation risks and requiring specialized anesthetic management. Spinal decompression surgery requires long periods of general or epidural anesthesia, and some patients cannot undergo surgery due to conditions preventing anesthesia tolerance. Chronic compression of lumbosacral nerve roots in spinal stenosis patients impairs nerve signal conduction, causing numbness and hyperalgesia in affected areas. Ropivacaine enables sensation separation from movement, facilitating endoscopic procedures under local anesthesia and mild sedation, with operators administering additional drugs as needed during surgery. Patients who are unable to tolerate general anesthesia in terms of cardiopulmonary function can also reduce the discomfort caused by LSS through the operation, which not only reduces the pain of the patients and contributes to the rapid recovery after the surgery. Intraoperative mechanical manipulation leads to nerve root injury, while prolonged high-pressure flushing results in neurological dysfunction including headache, palpitations, elevated blood pressure, and even a sense of imminent death. Spinal hypertension syndrome21 is a common complication of spinal endoscopy that cannot be ignored, and the patient in the waking state can communicate immediately with the operator, avoiding physical discomfort or nerves subjected to provocation, causing irreversible damage.
In 1997, Spetzger et al first introduced the ULBD technique and described clinical efficacy for the treatment of LSS in terms of lumbar spine anatomy, technical details, and clinical cases.22 Over the past 3 decades, the ULBD technique has been widely developed with a variety of minimally invasive tools, all of which have achieved good results in mid- and long-term follow-up.23 During microscopic surgery, the microscope and the patient’s position are constantly adjusted to obtain the field of view and operating space, the operation is performed under air media, the peripheral margin of the operation area is continuously oozing blood, the operation field is blurred, and the operation space under the spinous process is narrow, so it is difficult to reach the contralateral crypt with conventional open instruments to reach adequate decompression. UBE technique needs to be operated under the high-pressure water flow, and the ULBD technique needs to abrade the ipsilateral, contralateral, and spinous process, with a large number of plates. The ULBD technique requires the removal of a large number of vertebral plates ipsilaterally, contralaterally, and subacromial spine, which is a complex procedure with a long operative time and is prone to increased risk of hypothermia, metabolic disorders, and spinal cord hypertension-like syndrome.
Endoscopic ULBD utilizes a subcentimeter incision to access and remove the ipsilateral upper and lower vertebral plate bone. The technique involves obliquely cutting the bone at the spinous process root and addressing the contralateral side by removing the inner bone of the opposite vertebral plate, the lower articular process, and the hypertrophic upper articular process of the inferior vertebra. This approach exposes the inner edge of the contralateral vertebral arch, allowing for the removal of the ligamentum flavum and subsequent decompression of both the central and lateral spinal canal. The small incision accommodates an endoscope with a floating sheath, allowing for dynamic visualization. This approach provides a spatial perspective similar to traditional open surgery, offering a clear delineation of anatomical layers. Skillful use of a ring saw enables efficient bone resection and decompression, precisely addressing the area of spinal stenosis. This technique achieves bilateral decompression through a unilateral approach, expanding the spinal canal while preserving the integrity of select articular processes and the posterior spinal ligament complex, thereby maintaining spinal stability. This approach achieves comprehensive spinal canal decompression while preserving the posterior spinal structure’s stability. By avoiding iatrogenic secondary spinal instability, it eliminates the need for spinal fusion and internal fixation. Consequently, the efficacy of endoscopic ULBD may match or surpass that of traditional open surgery.
Conclusion
Endoscopic ULBD offers several advantages, including that it can be performed under local anesthesia and results in lower hospitalization costs, making it suitable for elderly patients with comorbidities who may not tolerate general anesthesia. The technique minimizes damage to the posterior spinal structure, reduces soft tissue separation and muscle stripping, and leads to less trauma, faster recovery, and favorable clinical outcomes. It is particularly beneficial for patients with moderate-to-severe single-segment central spinal stenosis, demonstrating positive mid-term follow-up results. However, it is important to note that this study’s limitations include a small sample size and a short follow-up period. Further long-term follow-up studies are required to definitively establish the technique’s long-term efficacy.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.