


Abstract
Objectives Lumbar lateral transpsoas interbody fusion is a powerful technique for addressing various spinal pathologies, enabling effective anterior column reconstruction. A critical decision in performing this procedure is selecting the appropriate side for the approach to the lumbar spine, whether in the prone or lateral decubitus position. This article outlines a decision-making framework to assist surgeons in deciding the optimal approach for direct lateral surgery to achieve the desired surgical outcome.
Study Design Technical note for lateral spinal fusion approaches.
Methods The article explores anatomical considerations, surgical indications, and patient-specific factors relevant to the choice of approach in lateral lumbar transpsoas fusions. Through case examples, various factors influencing side selection are discussed.
Results While many traditionally learn and perform direct transpsoas fusions through left-sided approaches, it is essential to consider pertinent anatomical features or variations, surgical pathologies, and patient-specific symptoms. The optimal side of the approach may vary based on these factors and remain key considerations for a holistic decision.
Conclusions A thoughtful assessment of the factors highlighted here can significantly improve the likelihood of a successful prone or lateral transpsoas fusions. Although comprehensive studies are needed to better guide decisions between right- and left-sided approaches, surgeons currently rely on their clinical judgment and expertise to navigate these choices to maximize safety and efficacy for each patient.
Clinical Relevance This study highlights minimizing surgical risk through holistic patient-centered decision-making.
Level of Evidence 4.
- lateral interbody fusion
- left-sided approach
- right-sided approach
- single-position interbody fusion
- transpsoas technique
Introduction
Spinal fusion techniques can address a range of spinal pathologies, including trauma, spinal instability, deformity, degenerative changes, neural compression, and neoplastic pathologies.1,2 In these instances, surgeons can access the anterior spinal column from various approaches to achieve solid interbody fusion: posterior, transforaminal, anterior, oblique, and direct lateral transpsoas methods. Direct lateral approaches to the lumbar spine, whether in the lateral decubitus or prone position, have increased in popularity amongst spine surgeons for various reasons. These include its minimally invasive nature through the preservation of posterior paraspinal structures, reduced risk of subsidence from large footprint cages, and the ability to achieve indirect neurological decompression by restoration of disc height and concurrently address spinal sagittal balance.3,4 In formulating a surgical plan, a fundamental question for surgeons is determining the optimal side of approach for direct lateral interbody fusion. For spine surgeons developing these skills, it is one of the most common questions they must address to position the patient and perform the surgery appropriately.
The present article presents a decision-making framework to assist surgeons in selecting the optimal approach for direct lateral spinal surgery and achieving the desired clinical outcomes. The prone lateral spinal fusion technique is emphasized as the preferred approach in the case examples provided. This technique enhances operative efficiency by leveraging the prone position, which naturally accommodates spinal lordosis, and facilitates pedicle screw placement without the need to reposition the patient for posterior column decompressions or access to other spinal levels.4
The main issues to consider when determining right- vs left-sided approaches are which side offers a favorable safety profile from an anatomical standpoint, whether one side provides more favorable ease of access, and whether symptoms are predominant to one side. Other surgical indications to potentially guide a side of approach are discussed below.
Key Surgical Considerations for Decision-Making
Anatomical Considerations
The detailed anatomy for access to the retroperitoneal space and relevant psoas muscle, lumbar plexus, visceral, and vasculature anatomy are described elsewhere. Here, we summarize pertinent anatomy to consider in direct lateral fusions.
Psoas Anatomy and Nerve Position
The lateral interbody fusion technique uses the transpsoas method to guide the placement of an interbody cage. The psoas muscle, a prominent hip flexor, arises from the anterolateral aspect of the lumbar vertebral bodies, adjacent intervertebral discs, and transverse processes of L1 to L5.5 It contains a superficial and deep segment within which the formation of lumbar plexus occurs. Multiple anatomical cadaveric and imaging studies have described the course of the psoas muscle caudally through the lumbar levels and the relevant neural structures within.6–9
While the muscle is usually thin over the upper lumbar levels, the presence of psoas muscle, particularly over the L3/4 and L4/5, is a prerequisite for a direct lateral approach. It is pertinent to consider psoas anatomy at the level of interest to establish a safe working zone with real-time image-guided access and neuromonitoring to minimize the risk of nerve injuries. The safe working zone in the caudal lumbar levels is narrowed to the midpoint of the disc in the dorsoventral plane at L4/5.
The most common issue at L4/5 is when the psoas muscle is anterior to the disc space. These “Mickey Mouse Ears” psoas denote their relative ventral migration. Although some studies show that the position of the psoas will change to some degree depending on positioning,10–12 particularly with hip flexion and extension, this will not compensate for this anatomical appearance.
An anteriorly located psoas muscle at L4/5 is often seen in cases of transitional anatomy and is usually bilateral in nature.13 However, there are instances of variation at L4/5 between the left and right sides where the location of the psoas may be more favorable on one side (Figure 1). Given the protection it affords to the lumbar plexus, this should be a high consideration in the preoperative decision-making at L4/5.

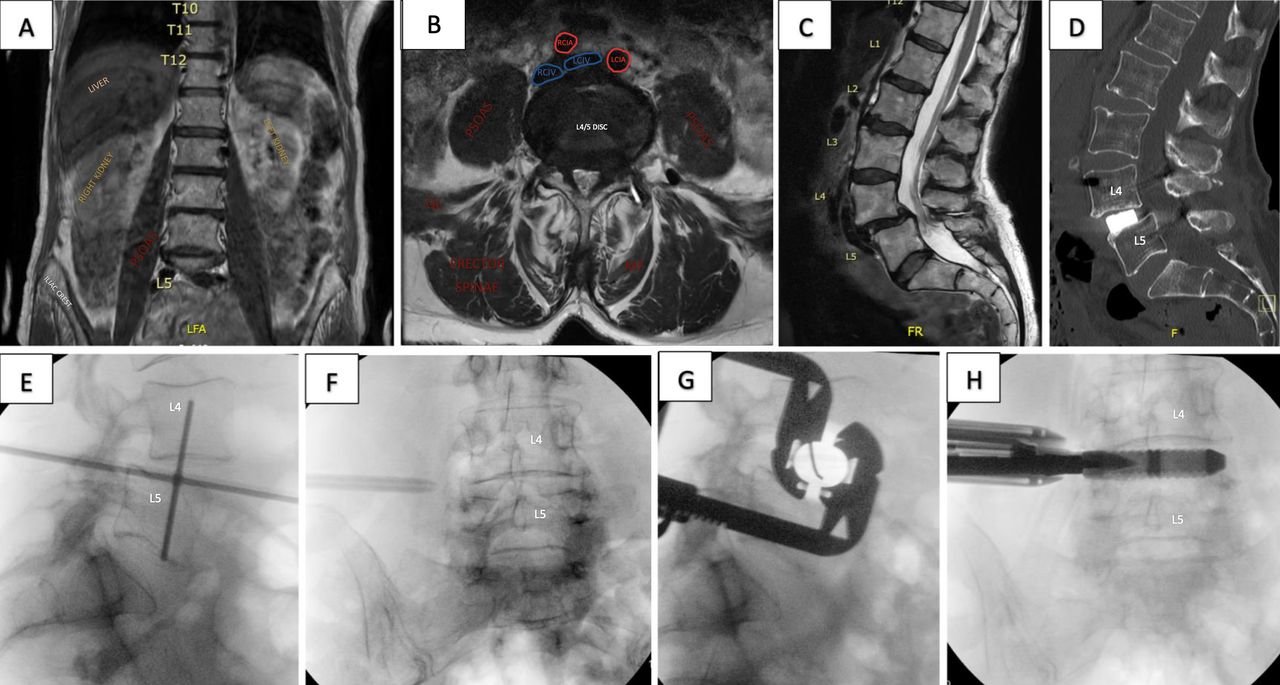
Case Example 1: A 72-year-old woman presented with neurogenic claudication symptoms and bilateral lower limb symptoms. Preoperative magnetic resonance imaging coronal (A) illustrates coronal deformity and asymmetry of iliac crests, with ease of access likely through the right. Preoperative sagittal (B) with grade 1 anterolisthesis of L4/5 and L5/S1 and associated canal stenosis. Preoperative axial (C) of L4/5 with severe canal stenosis, asymmetry of psoas—left psoas resembling “Mickey Mouse Ear”—favoring right-sided approach. However, the vascular anatomy—the right common iliac vein trajectory—encroaching on the right anterior disc space is noted. She underwent an uncomplicated right-sided L4/5 prone lateral interbody fusion with a posterior approach for L5/S1 level and L4 to S1 pedicle screws. Intraoperative radiography (D) showing fluoroscopy targeting and final implant position in anteroposterior view (E) and lateral view (F) with a decrease in spondylolisthesis at L4/5 through a right-sided approach. RCIA, right common iliac artery; LCIA, left common iliac artery; RCIV, right common iliac vein; LCIV, left common iliac vein.
Vessel Position
The great vessels run anterior to the lumbar vertebral bodies, which need to be carefully inspected on patient imaging before selecting the side of the approach. While some advocate for a left-sided approach due to the relatively anterior and right migration of the inferior vena cava and right common iliac vein (RCIV),14 we emphasize that careful consideration of a range of patient-related factors should be analyzed when choosing the side of the approach.
One of the most significant potential complications in lateral transpsoas approaches is an injury to a major vessel, usually the inferior vena cava or common iliac veins. While major vascular complications are infrequent, inspecting the preoperative images is crucial to knowing all major vessels’ locations and trajectories across the disc spaces. Hu et al8 demonstrate that the safe zones in the right-sided approach are narrowed at the caudal lumbar levels through their magnetic resonance imaging (MRI) study. In contrast, another MRI study by Deukmedjian et al15 illustrates that the RCIV trends posteriorly at the L4/5 level and into the surgical corridor in the right lateral decubitus position, arguing in favor of a right-sided approach with the patient in left lateral decubitus position. More recently, Joiner et al16 illustrate the positional variances of the great vessel in their MRI study comparing supine, right, and left lateral decubitus positions, recommending left-sided approaches for safe surgical access. The RCIV may encroach across the anterior margin of the disc space on the right side, narrowing the safe target area for docking. This is one of the reasons why some surgeons prefer a left-sided approach.
From our experience, direct visualization of the anterior margin of the vertebrae and anterior longitudinal ligament with an anterior retractor, using a 3-bladed lateral retractor, allows the vessels to be retracted (Figure 1). Still, it must be done carefully to minimize the risk of injury to the RCIV. For the 2-bladed retractor systems, direct visualization of the disc space and maintaining orthogonality are essential, particularly when placing an anterior shim. Apart from anatomical variants and excessive encroachment of the common iliac vein on the right at L4/5, the vessels are usually a secondary consideration in determining the side of the approach. The discrepancy in literature identifies the gaps in knowledge and the need for further studies with a significant population to enable robust statistical analysis for conclusions. In the interim, however, surgeons must be guided by their clinical expertise and judgment when deciding their approach to lateral transpsoas fusions.
Organ/Viscus Position
In assessing the preoperative scans, surgeons should consider the location of major visceral structures such as the kidney, ureter, and colon. The kidneys are located between the 12th thoracic vertebrae and the third to fourth lumbar vertebrae, typically located more caudally on the right due to the presence of the liver.17 The ureters travel adjacent to the psoas muscle, migrating on a sagittal plane from the dorsal third aspect of the vertebral bodies to the ventral third portion as they course caudally through the lumbar levels.18 The ascending and descending colon can be encountered when accessing the L2/3 to L4/5 from the right- and left-sided approaches, respectively.19 In the prone or lateral decubitus position, these structures are typically easily dissected away from the posterior wall of the retroperitoneal space to allow access into the lateral aspect of the psoas muscle.
When deciding on the side of the approach, a previous nephrectomy or solitary kidney on the side of the exposure should be considered. Minimizing risk to the kidney by choosing the contralateral side is suggested. In revision surgeries, surgeons should consider the side of previous retroperitoneal approaches for direct lateral fusions, given the increased likelihood of adhesions or scarring that may limit access to the psoas.
In underweight patients, the retroperitoneal space may appear thin, and the visceral structures may appear as an obstacle to a lateral approach (Figure 2). However, this is rarely the case with careful dissection of the retroperitoneal space, during which these structures are often palpated and swept away from the surgical corridor. In these circumstances, using a second incision is an added safety measure to carefully access and expand the retroperitoneal space just lateral to the quadratus lumborum.

Case Example 2: An 81-year-old woman with a body mass index of 18 presented with severe back pain, neurogenic claudication symptoms, and intermittent bilateral lower limb paresthesia on a background of rheumatoid arthritis. Preoperative magnetic resonance imaging coronal (A) with visceral structures, axial (B) with canal stenosis, psoas and vascular anatomy, and sagittal (C) with grade 1 anterolisthesis of L4/5 highlights approachability from either side of the spine. She underwent an uncomplicated right-sided L4/5 prone lateral interbody fusion with posterior percutaneous pedicle screws. Postoperative sagittal (D) with realignment at L4/5 and final implant position. Intraoperative radiography (E–H) showing fluoroscopy targeting, through 2-blade retractor system. RCIA, right common iliac artery; LCIA, left common iliac artery; RCIV, right common iliac vein; LCIV, left common iliac vein; MF, multifidus; QL, quadratus lumborum.
Level-Specific Considerations
Direct lateral interbody fusions have been successfully performed across the lumbar levels, with case reports of its expanded use rostrally and caudally at the thoracolumbar and lumbosacral junction, respectively. The anatomical feasibility of direct lateral spinal fusion has been investigated through MRI and cadaveric studies. Multiple studies indexing the neurovascular structures at risk across the intervertebral lumbar levels illustrate that this risk is highest at the L4/5 level.6,9 Kepler et al14 quantify neurovascular structures at risk in left-sided lateral approaches, 2.3% at L1/2, 7.0% at L2/3, 4.7% at L3/4, and 20.9% at L4/5 levels. The same study shows an increased risk in right-sided approaches, 7.0% at L1 to L2, 7.0% at L2 to L3, 9.3% at L3 to L4, and 44.2% at L4 to L5 due to vascular structures.14 Another study showed that persistent motor deficits following interbody fusion at L4/5 were 2.5% compared with 0.4% at the other rostral levels.20
Nonetheless, studies have shown the feasibility of lateral lumbar interbody fusions at L4/5 with acceptable sensorimotor neurological complication rates.21 Interestingly, a multicenter study of 172 lateral lumbar interbody fusion procedures shows a higher number of degraded femoral nerve evoked potentials at L3/4 compared with L4/5, further challenging the dogma of transpsoas approach feasibility of L3/4 over L4/5 levels.22 Again, this highlights the variability in anatomy concerning the lumbar plexus, and a detailed study of the patient’s imaging is a prerequisite to deciding procedures. However, in such cases of unfavorable anatomy, surgeons should consider an alternative approach to the spine.
L1/2 Level Considerations
The L1/2 level may challenge the lateral approach due to the floating ribs overlying the direct lateral corridor. However, it is rare for the L1/2 level to be targeted in isolation. In multilevel lateral fusions, whereby the retroperitoneal space has been entered for the lower lumbar levels, the L1/2 level can be approached by gentle retraction of the floating ribs (Figure 3). It is common to use angled instruments for L1/2, which is further discussed below when considering the L4/5 level.

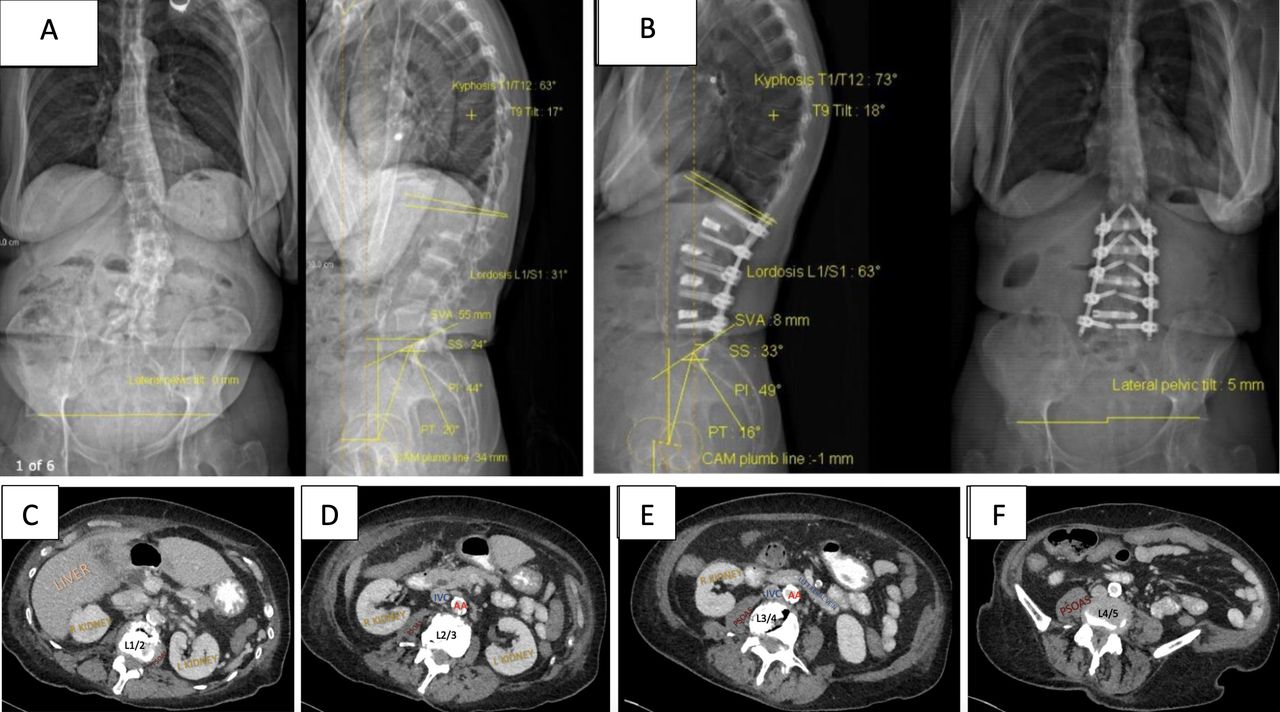
Case Example 3: A 78-year-old woman presented with severe back pain limiting mobility, neurogenic claudication symptoms, and L4 radiculopathy with imaging findings of degenerative scoliosis. EOS images preoperatively (A) with sagittal vertical axis (SVA) of 55 mm, lumbar lordosis of 31°, and postoperatively (B) with SVA of 8 mm, lumbar lordosis of 63°. Preoperative axial images at L1/2 (C), L2/3 (D), L3/4 (3), and L4/5 (F) with relevant vascular and visceral anatomy. A right-sided approach at the side of the concavity was selected, and she underwent an uncomplicated L1/2, L2/3, L3/4, and L4/5 prone lateral interbody fusion with L1 to L5 posterior percutaneous pedicle screws and L2 to L4 decompression. IVC, inferior vena cava; AA, abdominal aorta.
An additional consideration for L1/2 is the presence of the liver on the right, which may restrict access. However, in our experience, this does not preclude safe access and would only be a consideration in situations of significant hepatomegaly.
Coronal Asymmetry at the Disc Space
In some cases, particularly those with asymmetrical disc degeneration, collapse, osteophyte complex, or coronal deformities, one side may be a more straightforward approach due to the disc’s angle in the coronal plane. Furthermore, the L4/5 level may present a challenge for the lateral approach, mainly due to the position of the iliac crest relative to the disc space. The angle of the disc relative to the iliac crest can be assessed on plain films but is best assessed on a coronal magnetic resonance sequence. The position of the iliac crest is an important consideration but rarely an absolute contraindication, given the ability to use angled instruments in those approaches. In addition, using specific patient bolsters or tables to allow lateral bending may improve the angle of approach to the L4/5 level, shifting the iliac crest inferiorly. In most cases where the iliac crest is very high, the psoas muscle position is also unfavorable, which may be contraindicated. This level often represents a transitional level rather than a true L4/5 disc.
Side of Symptoms
The direct transpsoas approach commonly produces temporary psoas-related discomfort or pain on hip flexion, sometimes with inhibition of the hip flexion. If present, it usually passes within days or, in more severe cases, a few weeks, as shown in a recent long-term follow-up study highlighting largely transient weakness. 23 In most cases, where the preoperative symptoms are pain rather than weakness, either side can be considered for the approach, and the decision on the side of the approach should be based on ease of access, anatomy, and surgical pathology.
For patients with existing unilateral neurological deficits, particularly weakness of the quadriceps such as an L4 radiculopathy, the risk of injury to the lumbar plexus on the contralateral side, while small, should be avoided wherever possible.
Surgical Indications and Pathologies
Unilateral Foraminal Stenosis
In unilateral foraminal or lateral recess stenosis cases, lateral approaches are particularly effective for restoring disc height and achieving indirect decompression. Accessing the disc from the contralateral side allows for more straightforward navigation to the affected level, facilitating optimal restoration of both disc and foraminal height, as demonstrated through successive trials and cage implantation. This contralateral approach is especially advantageous in cases of asymmetric collapse, where osteophyte complexes may be present (Figure 4).

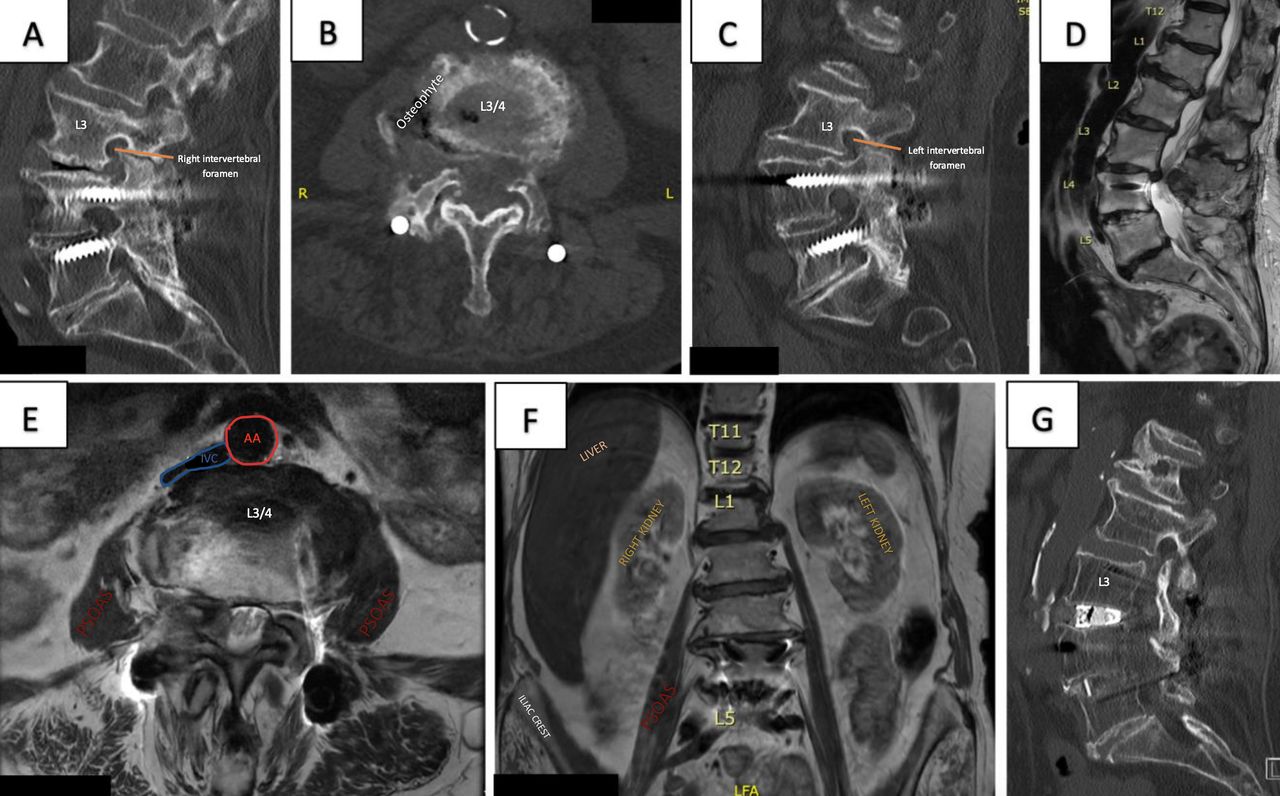
Case Example 4: An 86-year-old woman presented with severe lower limb pain and claudication due to spinal stenosis at L3/4 and adjacent segment disease on the background of an L4/5 posterior lumbar interbody fusion. Preoperative computed tomography L-spine sagittal (A) of vacuum phenomena of L3/4 disc space and right intervertebral foramen, axial (B) at L3/4 with a right-sided osteophyte complex, and sagittal (C) left intervertebral foramen. Preoperative magnetic resonance images are sagittal (D), axial at L3/4 disc and right-sided unilateral stenosis (E), and coronal (F). A left-sided approach was chosen, contralateral to the osteophyte, for ease of access and hepatomegaly evident on the right. She underwent an uncomplicated left L3/4 prone lateral interbody fusion with the extension of L4/5 posterior fusion and L3/4 laminectomy. IVC, inferior vena cava; AA, abdominal aorta.
When there is no significant neurological deficit on the affected side, a contralateral approach generally provides more straightforward access, provided anatomy allows for it. Furthermore, in situations where segmental deformity exhibits flexibility, patient positioning devices can effectively open intervertebral levels, allowing for optimal access from the desired side.
Bilateral Foraminal Stenosis/Central Stenosis
In cases of single-level bilateral foraminal stenosis and/or lumbar canal stenosis, the side that provides the safest anatomical route and ease of access should be used when symptoms are bilateral. Otherwise, if symptoms are unilateral or predominantly on 1 side, that side would typically be the preferred side of the approach.
Spondylolisthesis
Spondylolisthesis, particularly grade I to II, is a common pathology that frequently requires decompression and stabilization. The target area for docking in a lateral approach is the disc area where there is an overlap between the end plates of the vertebrae above and below. Spondylolisthesis may reduce the target area available for docking in a lateral approach. However, lateral approaches are commonly used for fusion procedures in spondylolisthesis and often achieve excellent clinical outcomes through indirect decompression (Figures 1 and 2).
Sometimes, a rotatory component to the spondylolisthesis may result in greater anterolisthesis on 1 side. The side of less anterolisthesis potentially provides a greater target area for docking and access to the disc. Close assessment of the vascular structures is also imperative in these cases. The common iliac vessels may be inadvertently pulled more posteriorly due to the slippage, resulting in a narrower, safer target area for docking.
One technique to increase the safe target area for docking is to place the pedicle screws before performing a lateral approach. This method can be a particular advantage of the prone lateral approach. Placement of the pedicle screws and partial reduction without tightening the cranial set screws may be beneficial in cases with higher degree of spondylolisthesis.
Multilevel Cases
When performing lateral surgery at multiple levels, assessment of the anatomy and safety is again paramount. However, the ideal approach is to plan the side and level to allow access to all levels needed through a single incision (Figure 5).

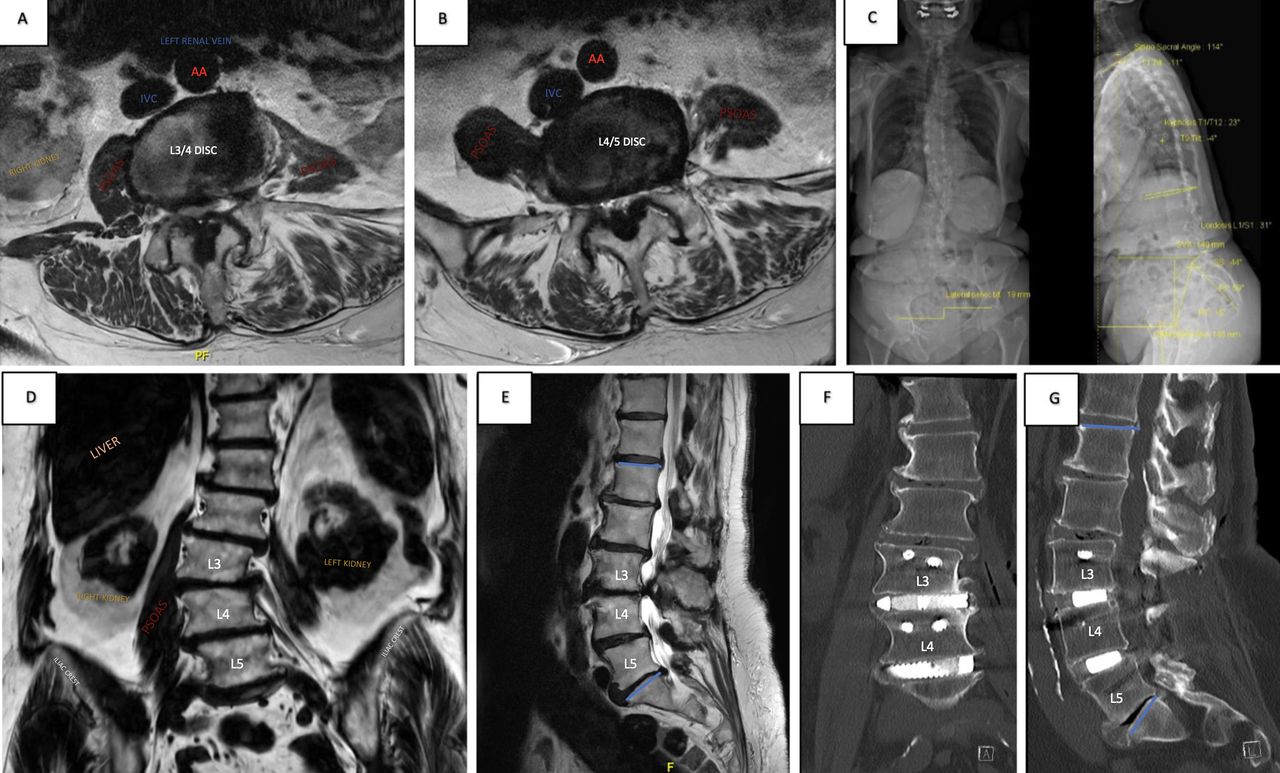
Case Example 5: An 83-year-old woman presented with neurogenic claudication, bilateral lower limb paresthesia, and difficulty walking in an upright posture. Preoperative magnetic resonance imaging axial L3/4 (A) with severe canal stenosis and axial L4/5 (B), coronal (D) with asymmetry of psoas and scoliosis convex right and sagittal (E). EOS (C) with sagittal vertical axis 149 mm. A left-sided approach was selected due to concavity to the left, plus the right psoas location is more anterior to the disc space at L4/5. She underwent a left-sided L3/4 and L4/5 prone lateral interbody fusion with L3 to L5 posterior percutaneous pedicle screws and L3 to L5 laminectomy. Postoperative computed tomography L-spine of coronal (F) and sagittal (G) with final implant positions. IVC, inferior vena cava: AA, abdominal aorta.
In the absence of a coronal deformity and when either side can be accessed, planning should be primarily driven by the issues identified above: symptomatology and surgical indication.
Coronal Deformity
Multiple levels can often be more accessible when a coronal deformity is present. In this situation, the psoas will usually present laxity on the side of the concavity, and the ideal angle for access at each level will pass through a common site on the lateral side.
One potential disadvantage is that the most collapsed side of the disc space will be within the concavity, and there may frequently be osteophytes present that hinder docking on the lateral aspect of the disc and advancement of a K-wire. Surgeons can overcome this challenge by removing the osteophyte, placing the shim, and sequentially trialing to expand the disc space.
When performing multilevel lateral approaches for coronal correction, there are various options for the order in which the levels should be approached—some advocate simply starting most caudally and then working progressively in a cranial direction. However, when planning surgery, the impacts of both coronal correction and rotational correction should be considered in the surgical plan. In some cases, working from “outside in” may provide the advantage of maintaining ease of access to all levels as the deformity is progressively corrected. For example, if 3 levels from L2/3 to L4/5 are to be addressed, the order might be L4/5, L2/3, and finally L3/4 (Figure 6).

Case Example 6: A 74-year-old man presented with significant lower back pain, limiting mobility on a background of renal impairment and cardiac issues. His imaging showed degenerative scoliosis and loss of lumbar lordosis. Preoperative axial L2/3 (A), L3/4 (B), L4/5 (C), sagittal (D), and coronal (E) with scoliosis convex left and kidney abnormalities. After medical work-up and preoperative optimization, a right-sided approach was chosen due to coronal concavity to the right. He underwent a right-sided L2/3, L3/4, and L4/5 prone lateral interbody fusion plus L5/S1 posterior lumbar interbody fusion with L2 to S1 posterior pedicle screws and S2-iliac screws. Intraoperative radiography shows fluoroscopic targeting of L4/5 (F) and trialing (G) prior to other rostral levels. Postoperative coronal (H) and sagittal (I) with final implant positions through a single incision right-sided approach for L2 to L5 prone lateral fusion. IVC, inferior vena cava; AA, abdominal aorta; RU, right ureter; LU, left ureter; LCIA, left common iliac artery; RCIV, right common iliac vein; LCIV, left common iliac vein.
More complex spinal curves and challenging surgical anatomy have occasionally necessitated bilateral approaches. While these scenarios are relatively uncommon, when the anatomy allows, this represents an advantage of prone lateral interbody fusion. This technique facilitates simultaneous access to both right- and left-sided approaches and posterior approaches, enhancing the surgeon’s ability to address multifaceted anatomical challenges efficiently in a single position.
Adjacent Segment Disease
The transpsoas approach, especially in prone position, is ideal for the surgical management of adjacent segment disease (Figure 7). This is due to the ability to achieve stabilization with restoration of lumbar lordosis and decompression, whether direct or indirect. In addition, the placement of pedicle screws and extension of the previous fusion with the replacement of existing rods and set screws can all be performed in 1 position. Advocates for single-position lateral decubitus surgery will also access the posterior column in the lateral position; however, the revision of existing constructs is more tedious with greater complexity, particularly for the inferior screws. The comments about other surgical indications are equally applicable to the decision-making regarding the side of the approach when performing surgery for adjacent segment disease.

Case Example 7: A 78-year-old woman presented with claudication symptoms secondary to adjacent segment disease on a background of L4/5 and L5/S1 interbody fusion. Preoperative axial at L3/4 (A) with severe canal stenosis and vascular, visceral and psoas anatomy, coronal (B) highlighting left-sided collapse, and sagittal (C) with canal stenosis and previous fusion. A right-sided approach was chosen for ease of access at disc space given overhang and collapse on the left. The patient underwent an uncomplicated right-sided L3/4 prone lateral interbody fusion with lateral plate and L3/4 laminectomy. Postoperative sagittal (D) with final implant position. IVC, inferior vena cava; AA, abdominal aorta; MF, multifidus; QL, quadratus lumborum.
This study emphasizes the advantages of accessing the lateral spine from either side, in contrast to the traditional left-sided approach. Specifically, the right-sided transpsoas approach is recommended in instances of asymmetry involving the psoas, intervertebral discs, or iliac crest when access is more favorable on the right (Figures 1 and 6). Additionally, it is beneficial in cases of coronal deformity with a left-sided convexity (Figure 3), as it allows for the treatment of all operative levels through a single incision. This approach can be indicated in patients with pre-existing weakness or pathology localized to the right side, as it reduces the risk of compromising the contralateral plexus. However, careful evaluation of vascular and visceral anatomy is essential to identify any anatomical variations that might contraindicate right-sided access. This comprehensive assessment ensures optimal surgical planning to minimize the potential for complications.
Operating Room Set-Up
The set-up for lateral approaches to the spine, whether prone or lateral decubitus, is essential for efficient workflow. Usually, the image intensifier enters from the contralateral side, opposite the sterile set-up. In most operating theaters, the design dictates which side of the patient this will be. The patient’s head may then need to be at one end or the other, depending on the side of the approach. Changes to the location of the anaesthetic machine can be avoided by using extended tubing. Importantly, the anaesthetist’s preferences regarding access to the patient’s head and airway may influence the approach taken, when either side is acceptable.
Conclusion
Minimally invasive spinal fusions offer versatility in addressing a range of spinal pathologies. Direct lateral interbody fusion through the transpsoas approach allows surgeons to access the intervertebral space through a unilateral retroperitoneal approach to stabilize and reconstruct the anterior spinal column. Surgeons undertaking this procedure must decide on the appropriate side of approach to position patients for surgery. In the present article, we discuss a range of factors to aid in the decision-making of left- vs right-sided approaches. The case examples illustrate the procedure’s feasibility from either side and the nuanced decision-making skills that surgeons must develop. Optimizing the side of the approach should not be overlooked, and surgeons should challenge the completeness of their decision with patient-specific anatomy. The knowledge gaps highlighted above emphasize the need for studies investigating intraoperative outcomes of right- vs left-sided direct lateral fusions and help guide the approach.
Footnotes
Funding VSR is funded as a Research Fellow at O SPINE through ATEC Research Grant; BO holds consultancy positions with Globus Medical and ATEC; YYW holds consultancy position with ATEC.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures B.O. holds consultancy positions with Globus Medical and ATEC; Y.Y.W. holds a consultancy position with ATEC.
Ethics Approval Multicenter study approval was obtained through Human Research Ethics Committee through National Health and Medical Research Council of Australia (ID: VR00025, Project ID: 2024-007).
Author Contributions Conception and design: B.O.; administrative support: B.O. and Y.Y.W.; provision of study materials or patients: B.O.; collection and assembly of data: V.S.R.; data analysis and interpretation: V.S.R.; manuscript writing: all authors. Final approval of manuscript: All authors have read and agreed to the published version of the manuscript.
Data Availability Statement The authors agree to the journal’s data sharing policy
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.