


Abstract
Background Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly prescribed for postoperative pain management after spinal fusion surgeries, but their potential impact on fusion outcomes and wound healing remains controversial.
Objective To use a national database and consistent selection criteria to compare the postoperative outcomes of patients who first received NSAIDs ≤ 72 hours, 72 hours to 90 days, and 90 days to 1 year after posterior lumbar fusion (PLF) surgery, to those who never received NSAIDs within the first year of surgery.
Methods Using the Merative Marketscan Research Databases, we analyzed PLF patients aged 18 to 90 years who underwent either single- and multilevel fusions. A subanalysis focused specifically on single-level fusions. Using the inverse probability of treatment weighting to adjust for confounders, we compared the outcomes of patients first administered NSAIDs at 3 different postoperative timeframes (≤72 hours, 72 hours to 90 days, and 90 days to 1 year) to patients who did not receive NSAIDs within 1 year of surgery. The outcomes evaluated included 30-day readmissions, length of stay, pseudoarthrosis, hardware failure, and wound complications up to 1 year after surgery.
Results Single- and multilevel PLF patients who received >90-day courses of NSAIDs 72 hours to 1 year postoperatively had greater odds of pseudoarthrosis, with those receiving short, ≤30-day courses of NSAIDs 72 hours to 90 days postoperatively additionally having greater odds of wound complications. Meanwhile, patients who started≤30-day courses of NSAIDs within 72 hours of surgery experienced reduced length of stay and lower rates of wound complications.
Conclusion Administration of long courses of NSAIDs >72 hours to 1 year after PLF surgery is associated with higher odds of pseudoarthrosis, while short courses of NSAIDs administered 72 hours to 90 days of surgery are additionally associated with higher odds of wound complications. Conversely, patients who received NSAIDs within 72hours of surgery may experience a slightly reduced length of hospital stay, with short courses of NSAIDs protecting against wound complications.
Clinical Relevance This study suggests that the timing and duration of postoperative NSAID use after posterior lumbar fusion can significantly affect outcomes, particularly fusion integrity and wound healing. These findings may help guide pain management protocols to balance effective analgesia with minimizing surgical complications.
Level of Evidence 3.
- posterior lumbar fusion (PLF)
- non-steroidal anti-inflammatory drugs (NSAIDs)
- pseudoarthrosis
- hardware failure
- wound complications
- readmissions
Introduction
Spinal fusion surgeries, such as posterior lumbar fusion (PLF), are vital interventions for a spectrum of spinal pathologies, including degenerative disc disease, scoliosis, spinal tumors, and trauma.1,2 Elective PLF, particularly for degenerative conditions, has seen a remarkable increase, surging by 62% in the United States from 2004 to 2015.2 This upsurge has placed PLF among the most frequently performed surgeries in the country. However, the complexity of PLF surgeries brings about considerable risks and the potential for various postoperative complications that contribute to increased health care costs.2–4 Given the prevalence of PLF surgeries, it is crucial for health care providers and patients alike to be well informed about the factors influencing adverse postoperative outcomes associated with PLF to ensure better prognostic outcomes and optimized care delivery.
Among these factors, nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used for pain control, yet their use after spine surgery remains controversial. These medications inhibit cyclooxygenase, preventing the synthesis of prostaglandins, thromboxanes, and prostacyclins, thereby potentially impacting wound and bone healing processes crucial for recovery.5–7 Research on the relationship between NSAID use and postoperative outcomes has yielded conflicting findings. Some studies have suggested unfavorable effects, such as reduced fracture healing rates leading to delayed union or nonunion.8–11 In the context of wound healing, the NSAIDs-mediated suppression of PGE2 may enhance scar formation and lead to antiproliferation of blood vessels and skin, conceivably resulting in delayed healing.6,7 However, other studies have failed to establish a clear connection between NSAIDs and delayed wound or bone healing.12–14 These discrepancies between findings could be attributed to differences in study designs, including different NSAID dosages, administration timing, limited number of drugs, and uncontrolled confounding variables or patient characteristics. These studies have also typically explored outcomes within varying postoperative timeframes, posing challenges for direct comparisons and impacting the generalizability of results.
In the present study, we aimed to address some of these inconsistencies by leveraging a national database and maintaining uniform patient selection criteria to compare the postoperative outcomes across 3 different NSAID administration windows following PLF surgery. In addition to the commonly reported outcomes in the literature, such as nonunion, we additionally evaluated wound complications, hardware failure, 30-day readmissions, and length of stay (LOS). By doing so, we aimed to build on the current literature and provide an understanding of how NSAIDs used at different time windows after surgery are associated with different patient outcomes. To do this, we controlled for confounding patient comorbidities, such as diabetes and other baseline health conditions, to minimize bias and ensure a more accurate assessment of the associations observed. Additionally, we performed subanalyses to evaluate how these associations may differ between patients undergoing multilevel vs single-level fusions. We purposefully used a patient database that included individuals taking a wide variety of NSAIDs to gain a collective understanding of the drug class as a whole, rather than focusing on the effects of individual medications. This approach allowed us to isolate the potential effects of NSAID timing on postoperative outcomes.
Methods
Data Source
The study utilized the Merative Marketscan Research Databases, a deidentified national database that spans a wide array of health care settings and recorded data from >250 million patients, for a query on patients who underwent PLF between 2007 and 2022.15 Due to the deidentified nature of Marketscan, the study was deemed exempt from requiring approval by the Institutional Review Board of our university.
Cohort Selection
Patients aged 18 to 90 years who underwent PLF, defined with an arthrodesis current procedural terminology (CPT) code of 22612 or 22633 and an instrumentation code (i.e., 22840 or 22842 or 22843 or 22844), were selected. To qualify for the study and minimize attrition bias via inverse probability of treatment weighting (IPTW), subjects had to have ≥1 year of medical history with ≥1-year follow-up. We excluded patients with a 1-year history of anterior arthrodesis (CPT 2258). Depending on whether variables were binary or continuous, missing data were addressed by assigning a zero for missing binary entries, signifying no diagnosis, while omissions in continuous variables were left out of the dataset. A subcohort analysis evaluated PLF patients undergoing uncomplicated, single-level fusions, excluding those with CPT codes 22842 and 22843.
Treatment Groups for Comparison
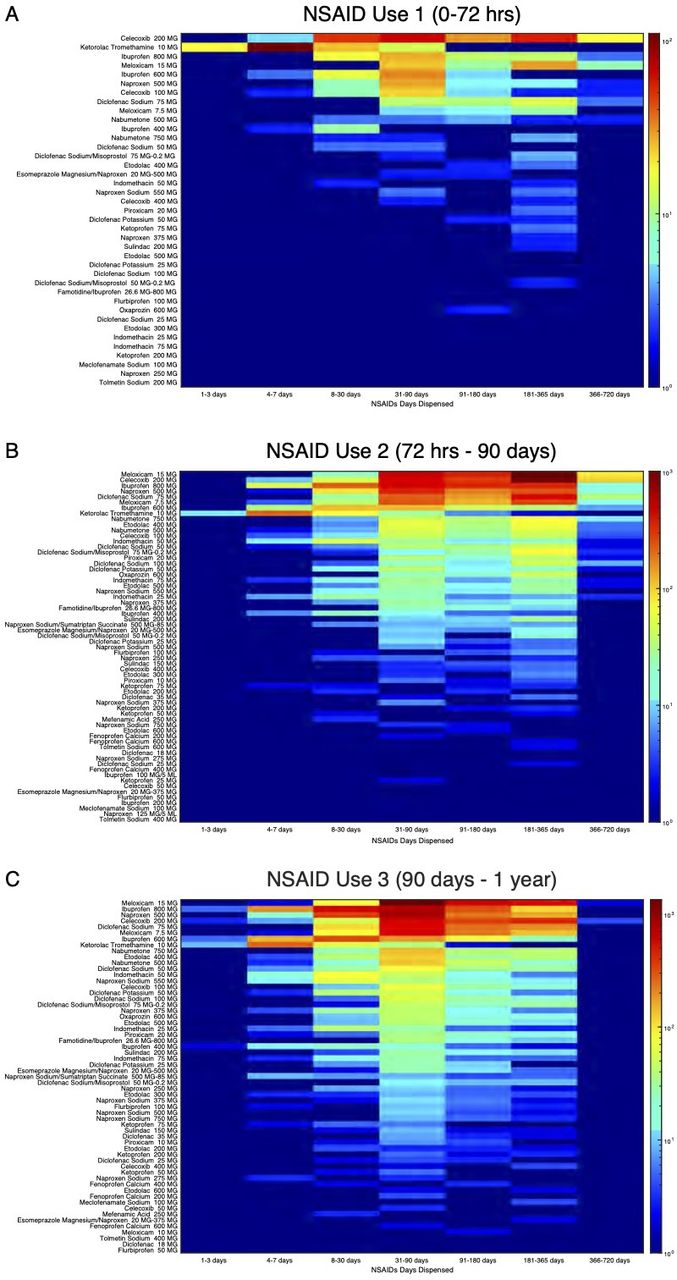
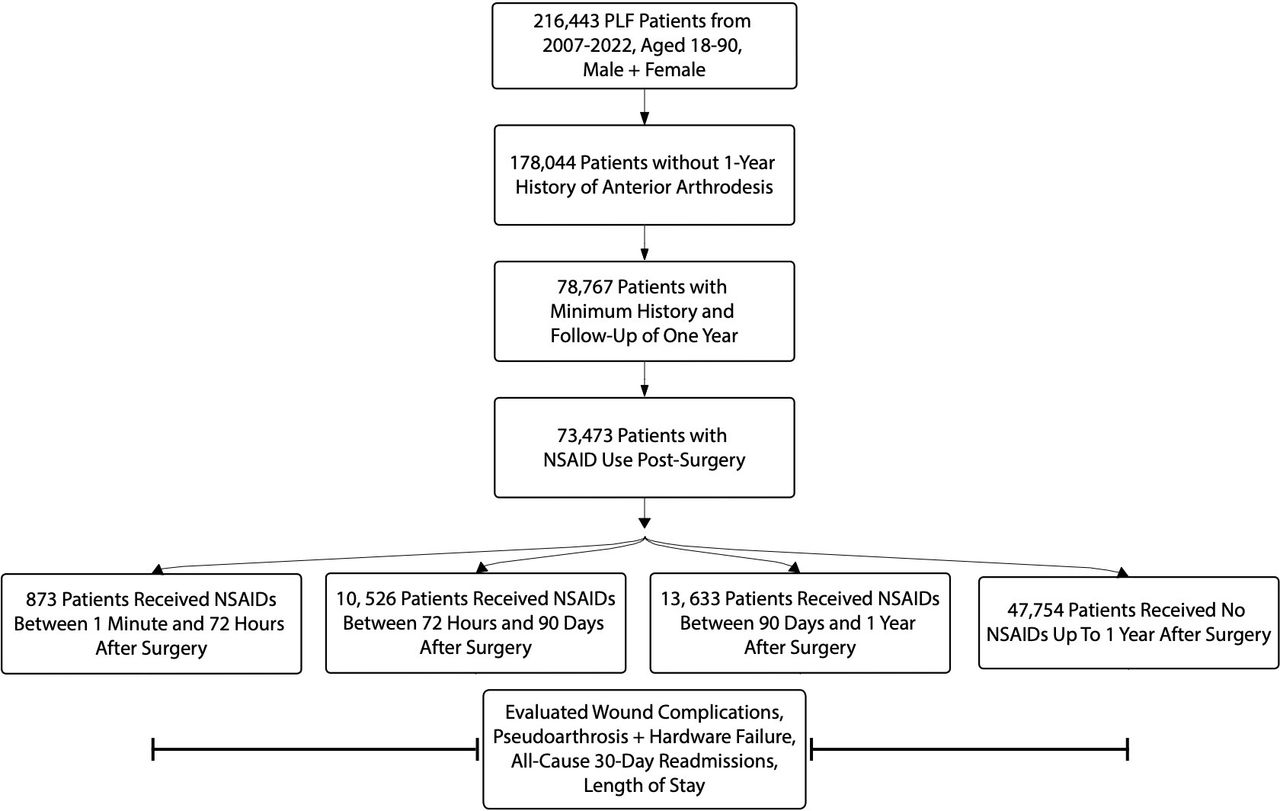
Patients were grouped based on NSAID administration during 3 postoperative periods: ≤72 hours after surgery, 72 hours to 90 days, and 90 days to 1 year postoperatively—all compared with patients who did not receive NSAIDs ≤1 year after surgery. NSAIDs were administered orally, with the exception of IV NSAIDs provided ≤72 hours postoperatively. Additionally, we analyzed how the length of NSAIDs courses (1–30, 31–90, 91–180, 181–365, and 366–720 days) impacted the postoperative outcomes measured, comparing these dispensation intervals within each NSAIDs administration group to the no NSAIDs control group. Figure 1 shows the frequency of NSAIDs types and the specific dosages prescribed during different length courses across the 3 postoperative timeframes, highlighting commonly used NSAIDs, such as meloxicam and Celecoxib, and how their usage patterns varied with both dosage and duration. Furthermore, Figure 2 provides a detailed overview of the cohort selection process, including the exclusion criteria and grouping of patients based on NSAID administration timing.

Distribution of nonsteroidal anti-inflammatory drug (NSAID) dispensation across postsurgical time intervals based on the timing of NSAID initiation. Heatmaps represent the distribution of NSAIDs dispensation across various time intervals postsurgery for different cohorts based on the timing of NSAIDs initiation. (A) NSAIDs started between 0 and 72 h of surgery with various day supply prescribed. (B) As in (A), but for patients who began NSAIDs between 72 h and 90 d postsurgery. (C) As in (A), but for patients who began NSAIDs between 90 d and 1 y postsurgery. The color intensity reflects the number of patients, with warmer colors indicating higher patient frequency and cooler colors indicating lower frequency. The x-axis shows the NSAIDs dispensation intervals (1–3 d, 4–7 d, 8–30 d, 31–90 d, 91–180 d, 181–365 d, 366–720 d), and the y-axis lists the specific NSAIDs and their dosages administered.

Selection criteria flow chart for the posterior lumbar fusion (PLF) cohort depicting the selection inclusion and exclusion criteria for the final PLF patients in the study.
Patient Characteristics
The burden of comorbidities within this patient cohort was evaluated by providing the prevalence and percentages of specific Charlson Comorbidity Index disorders within the NSAIDs or control groups. We defined gender as a binary variable and expressed it in terms of counts and percentages (ie, number and percentage of women). Age was treated as a continuous metric, expressed using mean and SD and also categorized by age groups to report patient counts and percentages. When the standardized mean differences (SMD) between the NSAIDs and the control group exceeded 0.25,16 patient characteristics, such as gender and age, were considered significantly different.
Postoperative Outcomes
Postoperative outcomes ≤1 year after surgery were analyzed, including all-cause, 30-day readmissions, LOS, pseudoarthrosis/nonunion, hardware failure, and wound complications—such as hemorrhage, hematoma, infection, and dehiscence. To ensure accurate outcome assessment, each was identified using a coding system consisting of CPT, ICD-9, and ICD-10 codes.
Statistical Analysis
Incidence rates of outcomes for treated vs control groups were compared through odds ratios and 95% confidence intervals from logistic regression using MATLAB software (v9.13.0 [R2023b], Natick, MA, USA). For the LOS in days, which are discrete counts, we utilized incidence rate ratios obtained from hurdle negative binomial regression. To maintain rigor in our statistical analysis, we accounted for multiple comparisons and outcomes assessed by using a Bonferroni-corrected P ≤ 0.01.17–20
Confounder Adjustment
To adjust for confounders, we used the IPTW approach, which is underpinned by high-dimensional propensity scores (hdPS) derived from baseline variables such as pretreatment diagnostic, procedure, and medication codes, as per the protocol detailed in Schneeweiss et al.21 The hdPS was designed to balance the baseline characteristics between our study’s control and treatment groups, with each participant’s weight being the inverse of their probability of receiving the treatment, thus fostering a balanced pseudopopulation and controlling for cofounders. Specifically, we adjusted for patient demographics (eg, age and gender) and a comprehensive range of comorbidities, including congestive heart failure, diabetes, chronic pulmonary disease, tumors, peripheral vascular disease, peptic ulcer disease, stroke, renal disease, dementia, liver disease, paralysis, rheumatoid arthritis, human immunodeficiency virus, and myocardial infarction. Logistic regression was utilized to fit a propensity score model incorporating these hdPS covariates, applying the Least Absolute Shrinkage and Selection Operator method to prune less significant variables. The fine-tuning of the Least Absolute Shrinkage and Selection Operator model, specifically the lambda hyperparameter, was accomplished through 5-fold crossvalidation based on the 1-standard error principle, aiming to forge a more parsimonious model without overfitting, as discussed in the literature.22
Results
Study Population Characteristics
In this study, 47,754 patients who were not administered NSAIDs were contrasted with those who were: 873 treated ≤72 hours, 10,526 within 72 hours to 90 days, and 13,633 between 90 days to 1 year after surgery. Baseline demographics and clinical profiles were similar among the groups: control, 54.12% women aged 52.01 ± 9.32 years; ≤72 hours group, 54.17% women aged 52.00 ± 9.32 years; 72 hours to 90 days group, 55.33% women aged 52.31 ± 9.15 years; 90 days to 1 year group 55.59% women aged 52.04 ± 9.25 years (Table 1). Diabetes was the most prevalent comorbidity among all 3 NSAIDs groups (control, 21.72%; ≤72 hours, 21.74%; 72 hours to 90 days, 22.41%; 90 days to 1 year, 21.72%). The most common administration course length was 31 to 365 days, with meloxicam 15 mg, celecoxib 200 mg, ibuprofen 800 mg, and naproxen 500 mg being the most commonly prescribed NSAIDs (Figure 1).
Demographics and clinical characteristics of PLF patients with NSAIDs use ≤ 72 h, 72 h to 90 d, or 90 d to 1 y after surgery.
In a subanalysis of uncomplicated, single-level PLF patients, 27,101 patients did not receive NSAIDs, compared with 542 treated ≤72 hours, 5823 72 hours to 90 days and 7725 90 days to 1 year after surgery (Table 2). Baseline characteristics were similar to those of the combined single- and multilevel PLF cohort; control, 56.04% women aged 51.57 ± 9.31 years; ≤72 hours, 56.12% women aged 51.57 ± 9.31 years; 72 hours to 90 days, 57.19% women aged 51.84 ± 9.15 years; 90 days to 1 year 57.40% women aged 51.53 ± 9.28 years. The most prevalent comorbidity in this cohort was also diabetes (control, 20.64%; ≤72 hours, 20.66%; 72 hours to 90 days, 21.36%; 90 days to 1 year, 20.65%).
Demographics of patients who received NSAIDs after uncomplicated, single-level PLF surgery at 3 different time windows.
Propensity Score–Matched Analysis
The balance achieved between the control and NSAIDs groups post-IPTW matching was evidenced by many SMD values falling below 0.25, across sex, age, and baseline comorbidities, suggesting the efficacy of IPTW in neutralizing a variety of confounders (Table 1) and further bolstered by using a Bonferroni-adjusted P value ≤ 0.01(Table 3).
Complication rates in PLF patients after NSAIDs use.
Control vs ≤72 Hours NSAIDs
Compared with the control group, PLF patients who received NSAIDs ≤72 hours postoperatively did not have significantly different 30-day readmissions (0.883 [0.631, 1.237], P = 0.470) or pseudoarthrosis/hardware failure outcomes (1.198 [1.020, 1.408], P = 0.028), at the Bonferroni-adjusted P value of 0.01. However, these patients did have lower associations with wound complications (0.692 [0.538, 0.889], P = 0.004), especially when prescribed ≤30-day course of NSAIDs (0.571 [0.391, 0.832], P = 0.004; Table 4), and shorter LOS (0.736 [0.706, 0.768], P < 0.001). Findings were similar in patients who underwent uncomplicated, single-level PLF: no significant associations were found in readmissions (0.836 [0.506, 1.380], P = 0.483), pseudoarthrosis/hardware failure (1.068 [0.882, 1.294], P = 0.500), or with wound complications (0.839 [0.599, 1.175], P = 0.308; Table 5). However, this group did have significantly shorter LOS (0.757 [0.715, 0.801], P < 0.001).
Complication rates in PLF patients starting NSAIDs use <72 h with different dispensing intervals.
Complication rates in uncomplicated, single-level PLF patients after NSAIDs use.
Control vs 72 Hours to 90 Days NSAIDs
Patients who started NSAIDs use 72 hours to 90 days postoperatively did not have significant differences in 30-day readmissions (1.011 [0.962, 1.063], P = 0.666). However, these patients did have increased associations with wound complications (1.069 [1.035, 1.105], P < 0.001), especially when provided with short, ≤30-day NSAIDs course (1.427, [1.286, 1.583], P < 0.001), and pseudoarthrosis/hardware failure (1.042 [1.017, 1.068], P = 0.001), particularly with longer, >180 NSAIDs courses (1.212 [1.114, 1.317], P < 0.001; Table 6). Similarly, while the uncomplicated, single-level PLF cohort did not show a significant association with readmissions (1.029 [0.954, 1.109], P = 0.462; Table 5), pseudoarthrosis/hardware failure was significantly associated with NSAIDs use (1.048 [1.015, 1.082], P = 0.004), as were wound complications (1.150 [1.097, 1.206], P < 0.001).
Complication rates in PLF patients starting NSAIDs use 72 h to 90 d with different dispensing intervals.
Control vs 90 Days to 1 Year NSAIDs
While there was a notable association between NSAIDs use and pseudoarthrosis/hardware failure (1.024 [1.009, 1.039], P = 0.002), particularly when prescribed up to 90 (1.096 [1.009, 1.190], P = 0.030) or 180 days (1.154 [1.035, 1.287], P = 0.010) of NSAIDs, there was no association found with the rest of the tested outcomes (Table 7). Similarly, there was no significant association with readmissions (1.032 [0.987, 1.078], P = 0.167) or wound complications (1.020 [0.989, 1.052], P = 0.202) in patients who underwent single-level PLFs, but an association was found with pseudoarthrosis/hardware failure (1.038 [1.019, 1.058], P < 0.001; Table 5).
Complication rates in PLF patients starting NSAIDs use 90 d to 1 y with different dispensing intervals.
Discussion
In this study, we utilized a national database to compare the outcomes of various postoperative NSAID administration windows in PLF patients. We analyzed a total of 47,754 patients and divided the cohort into those who received NSAIDs ≤72 hours after surgery, 72 hours to 90 days, or 90 days to 1 year—all compared with patients who did not receive NSAIDs. While we measured an association between NSAIDs 72 hours to 90 days and 90 days to 1 year postoperatively with increased pseudoarthrosis/hardware failure, the effect size was the largest in the 72 hours to 90 days timeframe. Interestingly, receiving NSAIDs ≤72 hours after surgery was associated with decreased wound complications—particularly, when patients received short, ≤30-day courses—as well as shorter LOS. Meanwhile, those who received NSAIDs 72 hours to 90 days after surgery had greater instances of wound complications, particularly when administered for ≤30 days. These findings were broadly similar in PLF patients who underwent uncomplicated, single-level fusions. Our results build upon existing literature by (1) comparing 3 timeframes within a single, confounder-adjusted cohort under consistent selection criteria, (2) extending beyond the commonly reported postoperative metric of nonunion by evaluating various outcomes, including wound complications, (3) analyzing the postoperative outcomes of various NSAIDs, (4) considering the effect of varying NSAIDs administration course lengths, and (5) subanalyzing how associations may differ in a cohort of uncomplicated, single-level PLF patients.
To the best of our knowledge, there are only a few studies that have evaluated the impact of short-term postoperative NSAID administration (≤72 hours) on pseudoarthrosis outcomes.23–26 These studies have a limited focus on specific NSAIDs and exclusively measure the rates of pseudoarthrosis. To further complicate the interpretation of these studies, the results across them are mixed: 3 found no association between ketorolac use ≤48 to 72 hours of surgery and pseudoarthrosis,23,24,26 while another study reported an increased association with pseudoarthrosis when ketorolac or fentanyl was administered ≤72 hours postoperatively.25 The differences observed between these studies may result from variations in study populations and size, differently defined pseudoarthrosis, and the specific types and dosages of NSAIDs analyzed. NSAIDs administered 72 hours after surgery were associated with pseudoarthrosis in several studies.27–31 Our findings agree, further supporting the deleterious effects of long, ≥180-day courses of NSAIDs when administered primarily 72 hours to 90 days after surgery, as shorter courses were not associated with these outcomes. To a much lesser extent, ≥90-day NSAID courses started 90 days to 1 year after surgery were associated with pseudoarthrosis/hardware failure; however, the increased odds ratio was comparatively smaller, suggesting a reduced risk for these complications as the postoperative period lengthens.
Interestingly, we found decreased associations with wound complications and shorter LOS if NSAIDs were administered ≤72 hours after surgery, particularly, when administered ≤30-day NSAIDs course, as longer medication courses were not associated with decreased wound complications or shorter LOS. This result aligns with prior studies; for instance, immediate postoperative ibuprofen does not increase bleeding in soft tissue surgeries;32 short, 4.5 to 13.5 days NSAIDs use following extremity wounds was associated with superior wound healing;33 and aspirin had beneficial effects in treating chronic wounds by inhibiting cytokine release.34 These studies, along with ours, suggest that in specific circumstances—particularly with short-term administrations—NSAIDs might not only fail to impede wound healing but could potentially enhance the process, especially in wounds that are prone to excessive inflammation.
While immediate postoperative administration might be associated with minimal or even beneficial effects on wound healing, NSAIDs used at other time points could lead to wound complications. For instance, Vadivelu et al found that prolonged NSAID use leads to impaired wound healing, especially in surgical patients,35 and Schafer et al highlighted the risk of bleeding complications associated with long-term NSAID use, particularly in patients with coagulopathies or during perioperative period.36 Our findings agree with these studies: patients who received NSAIDs 72 hours to 90 days postoperatively had a greater association with wound complications, even when only prescribed short, ≤30-day medication courses. However, unlike these previous studies that identify associations between NSAID use and wound complications within a specific time snapshot, our approach allows for a more nuanced understanding of how the timing and medication course lengths influence outcomes.
Clinical Implications
In light of these findings, clinicians should consider integrating the timing of NSAID administration into their perioperative management plans by evaluating the potential risks and benefits for individual patients. For both single- and multilevel fusion patients, administering NSAIDs within the first 72 hours after surgery may be safe and even beneficial for wound healing while also reducing hospital stays. LOS is influenced by hospital resources, workflows, therapy plans, patient compliance, and administrative processes;37–43 therefore, immediate, postoperative NSAID use may lead to reduced LOS by managing postoperative pain, improving mobility, expediating the start of physical therapy, and improving patient compliance—all of which are key in reducing complications, accelerating discharge, and efficiently utilizing health care resources. After 72 hours but before 90 days, caution is warranted, as both short and long courses of NSAIDs can negatively impact wound and bone healing. However, another safe window for NSAID use maybe after 90 days, as only the longest courses of NSAIDs were associated with pseudoarthrosis.
Limitations
While our study provides valuable insights into the effects of NSAID administration at various postoperative intervals on patient outcomes, there are limitations inherent to our analysis. These include the inability to control for all variables that might influence LOS and 30-day readmissions, such as hospital resource allocation, efficiency of care delivery, care transition planning, and insurance or administrative hurdles. Additionally, the reliance on administrative claims data limits our ability to establish causality, as the observed relationships are associative rather than causal. For example, NSAIDs may have been prescribed reactively to patients with higher baseline risks of complications, such as elevated pain or inflammation, suggesting the possibility of reverse causality. Our analysis also did not adjust for NSAID use prior to surgery nor could it differentiate the effects of various NSAID dosages due to dataset limitations. Future investigations should leverage institutional data sources, which could provide more control over such patient-specific factors, as well as prospective designs, including randomized controlled trials, to better evaluate causal relationships and refine our understanding of NSAID use on postoperative outcomes. Despite the limitations of this study, most of which are inherent to the use of large patient databases, our research provides an initial exploration into the impacts of NSAID timing on postoperative outcomes in PLF patients.
Conclusions
Our study leverages a national payer’s database to evaluate the impact of NSAID administration at different postoperative intervals in PLF patients. It identifies a link between long, ≥180-day NSAID courses and increased pseudoarthrosis/hardware failure when administered 72 hours to 90 days—and to a lesser extent, 90 days to 1 year—after surgery. Patients who received NSAIDs ≤72 hours postoperatively, however, had lower associations with wound complications and decreased LOS. In contrast, those who received even short, ≤30-day NSAID courses 72 hours to 90 days after surgery had a greater association with wound complications. These findings suggest that the timing of NSAID administration is crucial and warrants careful consideration in perioperative patient management. By analyzing a single patient population with consistent selection criteria across 3 distinct NSAID administration windows, our study facilitates a cross-comparison of postoperative outcomes as a function of time.
Acknowledgments
Data for this project were accessed using the Stanford Center for Population Health Sciences Data Core. The PHS Data Core is supported by a National Institutes of Health National Center for Advancing Translational Science Clinical and Translational Science Award (UL1TR003142) and from Internal Stanford funding. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Footnotes
Funding This study was conducted without any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests The authors declare no conflicts of interest related to this work. They have no financial, personal, or institutional relationships that could be perceived as influencing the content of this manuscript.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.