


ABSTRACT
Background: Cranial radiation exposure during instrumented spine surgery is not well documented. We set out to measure this risk to the patient, surgeon, surgical resident, and scrub technician during these procedures.
Methods: Forty-seven individuals were enrolled during a 1.5-year period between October 2014 and March 2016 at the University of New Mexico Department of Neurosurgery. Radiation doses were obtained through electronic dosimeters placed on the surgical cap over the temporal scalp (bilaterally on surgeon and resident assist, unilaterally on surgical scrub on the side facing radiation source) and on the midline of the patient's exposed cranium.
Results: Of the 47 procedures, 39 (83%) were open and 8 (17%) were minimally invasive or percutaneous instrumented procedures. A total of 91 motion segments were treated, with a mean of 1.9 levels per case (57% lumbosacral, 34% cervical, and 2.1% thoracic). Total fluoroscopic time was 12.9 minutes. Mean dose per case (mrem/case) was calculated for the spine surgeon (1.4), resident assist (1.4), surgical scrub (1.2), and the patient (3.6). All doses were within federal safety guidelines. A spine surgeon would need to perform more than 1400 cases per year to reach the current federal maximum permissible dose for head exposure.
Conclusions: There was no difference in cranial radiation exposure between operating room staff during spine surgeries. Moreover, the doses measured at the cranium were within national safety limits. Current protective technologies have significantly reduced the amount of ionizing radiation exposure during routine spine procedures; however, changes in behavior or equipment may further reduce radiation exposure to health care workers.
Clinical Relevance: Radiation exposure to patients and hospital staff remains a major concern in the practice of modern spine surgery. Cranial exposure remains the only established environmental risk factor for brain tumors, such as gliomas and meningiomas. Our study shows that all those exposed to radiation during spine surgery had cranial doses well within the national safety limits.
With the universal use of fluoroscopic guidance during spine procedures, concern for radiation exposure to patients and hospital personnel remains a major worry.1,2 Within the general context of radiation exposure, most workers exposed to man-made radiation are now medical personnel.3 Although scatter radiation exposure to the lens of the eye and regions below the neck have been quantified and minimized using a variety of personal protective equipment,4–10 not much literature is available on exposure to the forehead and skull.11–13
Cranial radiation exposure remains a major risk factor for the development of cataracts and brain tumors, including gliomas and meningiomas.11,14–22 According to federal safety guidelines from the Interventional Commission on Radiological Protection (ICRP), exposure to the lens of the eye (and extrapolated to head exposure) should be limited to 20 mSV (2000 mrem) per year.23 Our own data from the cranial angiography suite suggest considerable cranial radiation exposure to the operating interventionalist and circulating nurse.24
Currently, the literature on cranial radiation exposure in fluoroscopy-guided spine surgery has focused on exposure to the surgeon's torso,25–27 neck, or hand.26,28 However, there is little literature on cranial exposure to either the patient or operating room staff. Based on our previous observations during cranial angiography,24 we performed a prospective study evaluating radiation exposure to the cranium during spine procedures, where the use of fluoroscopy is universal.
METHODS
All patients older than 18 years, who underwent instrumented or noninstrumented spine procedures that required the use of intraoperative fluoroscopy at the Department of Neurosurgery, University of New Mexico Hospital, between February 2014 and June 2016, were prospectively enrolled in the study. Vulnerable populations, including minors, pregnant women, and incarcerated individuals, were excluded from the study. Patients were enrolled prospectively. Instadose, electronic direct ion storage dosimeter badges (Mirion Technologies, Irvine, California), certified by the National Voluntary Laboratory Accreditation Program, were worn by the primary operating surgeon, surgical resident, operating scrub technician, and the patient undergoing the surgical procedure. Institutional Review Board approval was completed through the University of New Mexico Institutional Review Board.
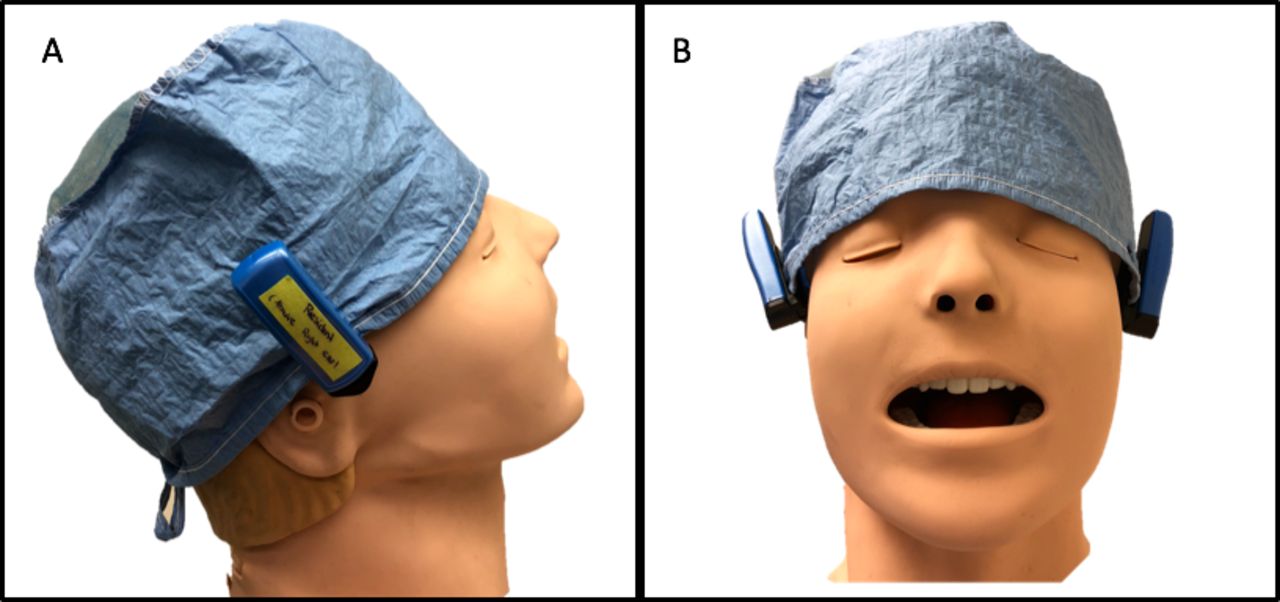
The primary surgeon and assistant wore two badges, one on each side over the temporal scalp, affixed to the surgical cap (Figure 1). The scrub technician wore one badge over the temporal scalp facing toward the source of ionizing radiation. The patient's badge was placed in the center of the forehead or occiput, facing upward for the entirety of the procedure (Figure 2). Because of low radiation doses overall, which were below the dosimeter detectable limit, 10 cases of cumulative radiation doses at a time were read from the dosimeters and subsequently averaged. Data were compiled and analyzed retrospectively using Microsoft Excel, 2016 (Microsoft Corp, Redmond, Washington).

Placement of dosimeter badges on the outside of the scrub cap for both primary surgeon and resident assistant on each temporal scalp area. (A) Lateral view. (B) Profile view.

Operating room setup. Black upward arrow represents the dosimeter badge.
RESULTS
A total of 47 patients were prospectively enrolled in the study. Of these, 39 (83%) were treated with an open approach, and 8 (17%) were minimally invasive (MIS) or percutaneous procedures. No significant difference in radiation delivered via fluoroscopy machine (C-arm) was noted for MIS versus open approaches (P = .79 using Student 2-tailed t-test). A total of 91 motion segments were treated, with a mean of 1.9 levels per case (57% lumbosacral, 34% cervical, and 2.1% thoracic). Radiation dose received at the dosimeters per case was averaged for the spine surgeon (1.4 mrem), resident assistant (1.4 mrem), surgical scrub technician (1.2 mrem), and the patient (3.6 mrem; Table). A spine surgeon would need to perform more than 1400 cases per year to reach the current federal maximum permissible head exposure dose and more than 3500 cases per year to reach the whole-body deep permissible dose.
Dosimetry measurements in vivo and extrapolated annual exposure.
DISCUSSION
Radiation exposure to patients and hospital staff remains a major concern in the practice of modern spine surgery.1,2 The majority of man-made sources of radiation exposure is to medical personnel.3 Moreover, cranial exposure remains the only established environmental risk factor for brain tumors, such as gliomas and meningiomas.11,14–22
In 1929, what is now the National Committee on Radiation Protection and Measurements was established to provide the public with recommendations on radiation safety.29 This need arose from the developments of atomic and nuclear weapons during World War II. Although no dose is considered without risk, the ICRP has established 20mSV (2000 mrem) per year as the head exposure limit.23
A study by Mariscalco et al30 compared radiation exposure to a surgeon's thyroid/eye, chest, and hand in open discectomy cases versus minimally invasive lumbar microdiscectomy cases. They demonstrated that a surgeon would have to perform only 1623 minimally invasive microdiscectomies in their lifetime to surpass the amount of whole-body radiation of 5000 mrem deemed safe for occupational exposure.30 Another study by Amoretti et al13 measured the amount of radiation exposed to the left orbit of the operating surgeon during computed tomography (CT)–guided and fluoroscopy-guided percutaneous vertebroplasty to be a cumulative irradiation dose of 0.14 mSV. An in vivo study by Mulconrey25 placed unprotected dosimeters on the surgeon's and first assistant's chests, and they estimated that they could be exposed to a maximum of 453 minutes of radiation to remain below the yearly permissible dose.
Available literature on radiation exposure in fluoroscopy-guided spine surgery is focused on exposure to the surgeon's torso, neck, or hand, whereas studies on cranial exposure remain scarce.4–6,8,12,13,17,28,30,31 We therefore sought to determine cranial radiation exposure to the patient, surgeon, and operating room personnel during spine surgeries requiring fluoroscopic guidance.
The ICRP guidelines limit exposure to the lens of the eye, and therefore the head, to 20 mSV (20 000 mrem) during a 5-year period.23 A head CT scan is 2.0 mSV (2000 mrem), whereas the average radiation dose received by the spine surgeon, resident assistant, surgical scrub technician, and patient is a fraction of that amount.32
In addition, our results demonstrated that there was no statistical difference in cranial radiation among operating room staff during fluoroscopic spinal surgeries. The patient's dosage, however, was 3 times that of the staff. Even with these differences, all those exposed to the radiation were well within the national safety limits, according to the ICRP.23 Therefore, a spine surgeon would need to perform more than 1400 cases per year to reach the current federal maximum permissible head exposure dose.
The strength of the study is that the dosimeters are placed directly over the skull caps of the operating room personnel and on both sides of the scalp of the operating surgeon and resident. Previous studies have placed dosimeter badges on the chest and extrapolated radiation doses to the cranium.25 Limitations of our study included the quality of the dosimeters themselves. The accuracy of the dosimeters is found to have a 25% to 35% error rate. Even with that margin of error, the detectable dose is so low that the current radiation exposure is still found to be minimal. Our study suggests that the current fluoroscopic radiation exposure is well below the federal maximum permissible dose for operating surgeons, residents, scrub technicians, and the patient.
CONCLUSIONS
In summary, the current study is the first of its kind to directly study cranial radiation exposure during spine surgeries. We found no difference in cranial radiation exposure between operating room staff during spine surgeries. Moreover, the doses measured at the cranium were within national safety limits. Current protective technologies have significantly reduced the amount of ionizing radiation exposure during routine spine procedures; however, changes in behavior or equipment may further reduce radiation exposure to health care workers.
Acknowledgments
The authors wish to acknowledge the efforts of Dr Howard Yonas, chair of the Department of Neurosurgery at the University of New Mexico, in support of this research.
Footnotes
Disclosures and COI: The authors report no conflict of interest or financial disclosures concerning the information presented or the findings specified.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.