


ABSTRACT
Background: Transpedicular screw insertion has become widely accepted for the correction of spinal deformity as well as degenerative and traumatic injury, but adoption of this technique has remained less widespread in the thoracic compared to the lumbar spine. This is thought to be associated with the relative technical difficulty of screw insertion into the narrower widths of the thoracic pedicles and the neurologic and mechanical risks associated with breach of the pedicle wall. The surgical decision making involves determining the appropriate sized screw for maximum fixation strength while simultaneously respecting the structural integrity of the vertebral pedicles to prevent a breach and provide better fixation. This paper presents a systematic review of criteria for thoracic pedicle screw diameter (SD) selection in order to orient inexperienced surgeons on the impact of this selection on pedicle breaching and fixation strength.
Methods: We performed a systematic literature review focused on studies reporting SD selection in relation to pedicle dimensions, measures of fixation strength, and breach rate.
Results: Twenty-nine articles that measured fixation strength, breach rate, and/or provided SD in relation to pedicle width were selected for inclusion.
Conclusions: A commonly accepted criteria for pedicle SD selection has not yet been proposed. Screw diameters approximately 80% of the pedicle width have been adopted, but this proportion is rarely reported in the midthoracic vertebrae for which smaller pedicles and inadequate hardware specificity result in higher breach rates. Depending upon the insertion technique adopted, greater specificity in diameter selection by vertebral level should be pursued in order to maximally target cortical bone purchase.
Clinical Relevance: Based on this review of the literature, we believe that proper selection of the SD for individual vertebral level directly affects the insertion technique and the potential breach.
INTRODUCTION
Transpedicular screw insertion has become the gold standard for spinal fixation used in the correction of spinal deformity1–3 and trauma.4–7 It is focused on achieving long-lasting fixation and strength and providing the scaffolding for a bony fusion. Despite the increased use of pedicle screw constructs, the insertion of pedicle screws in the thoracic spine represents unique challenges as compared to the earlier adopted instrumentation of lumbar segments. These challenges mainly stem from the increased technical difficulty in placing thoracic pedicle screws due to smaller sized pedicles and the proximity to neural, visceral, and vascular structures of the thorax.8,9 Screw misplacement (see Figure 1) can alter the pullout strength (POS)10 and can cause various complications such as intraoperative pedicle fracture, loosening, dural laceration, and transient neurologic injury.11 The accuracy of screw insertion has been analyzed extensively, and full containment within the cortical walls of the pedicle is achieved 69–94% of the time using the free-hand technique, with an increased range of 89–100% of attempts when utilizing computer tomography (CT) navigation across all vertebral levels.12 Additionally, a 2007 meta-analysis reporting on 130 studies representing 37 337 total screws reports an overall accuracy rate of 91.3% throughout the spine, with decreased accuracy at thoracic levels.13
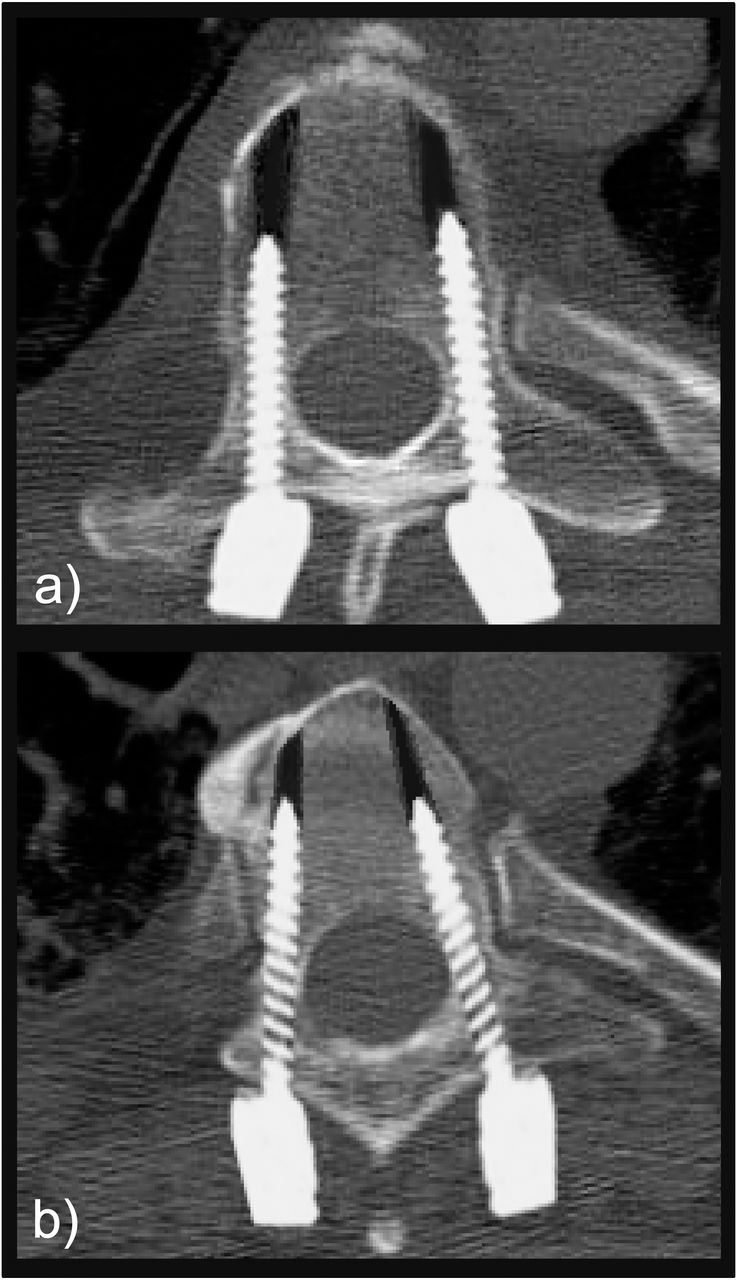
Pedicle screw insertion on computer generated images of (a) successfully placed screws and (b) misplaced screws: laterally for the right pedicle and medially for the left pedicle.
It has been shown that, when using currently accepted insertional techniques, malposition is strongly reduced with surgeon experience.14 Chen et al15 demonstrated that, using free-hand placement, an apprentice surgeon dangerously misplaced screws at a rate of 26.7%, in contrast to just 9.1% obtained by the chief surgeon. Furthermore, a minimum of 60 supervised screw placements were found to be necessary before the apprentice could accurately execute the free-hand technique independently. Additionally, in a 14-month period, Samdani et al16 reported a dangerous misplacement rate of 15.5% for a surgeon's first 181 implanted screws, which was reduced to 10.6% for the next 189 and 8.7% for the final 183 attempts. The selection of appropriate screw dimensions by vertebral level is key for successful insertion. As such, screw length is precisely pre-operatively and intraoperatively evaluated,17,18 but SD selection is left up to the experience of the surgeon.19 The tolerance for avoiding pedicle wall perforation has been theoretically proven to be reduced with increased SDs,20 while in actual placement, the screw is selected as the largest possible17,19 to achieve greater stability.21,22 These measures are reported, often in separate studies, as experiments measuring either pullout/fixation strength or breach rate of screws inserted in vitro or in cadaveric models. The resultant compromise between safety and stability that must be weighed for SD selection remains an important area of research which the current study will review.
This study aims to build a comprehensive systematic review of thoracic pedicle SD selection in order to summarize currently suggested selection criteria and demonstrate the impact that this decision can have on pedicle breaching and fixation strength. We hope these findings will be of particular interest to inexperienced surgeons for whom the breach rate in relation to SD has been shown to be significantly higher.
MATERIALS AND METHODS
Search Strategy
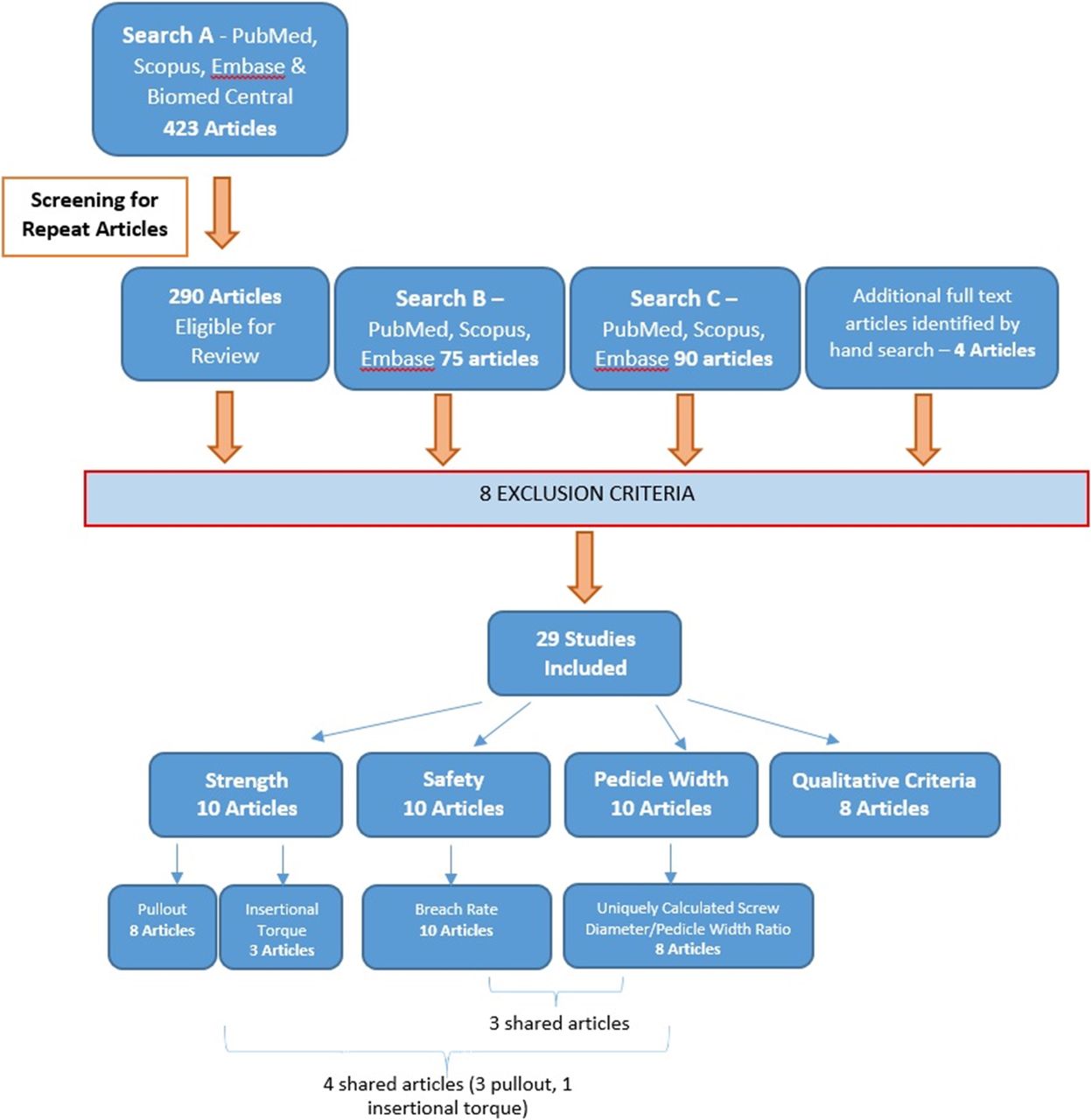
A systematic literature search was conducted in PubMed, Scopus, EMBASE and Biomed Central online databases using the syntax: (((thoracic) AND pedicle) AND screw) AND diameter. Of the 423 articles identified by this strategy, duplicates were removed, yielding 290 articles eligible for review. Following this initial search, we conducted 2 additional searches with the keywords “size” and “width” in place of “diameter.” After review, if articles were deemed worthy of inclusion, they were then checked against prior inclusions across all previous searches, and repeats were discarded. An additional 4 articles were also identified by hand search of the reference sections of articles identified by the review process.
Article Selection
Articles were selected for inclusion based on their contribution to 1 or more of 3 topics which we deemed relevant to our objective. These topics included (1) recommendations for appropriate SD selection including concurrent reporting of utilized SD and transverse pedicle dimension by vertebral level, (2) quantitative data on POS or insertional torque of pedicle screws of defined diameter, and (3) quantitative data on breach rate of inserted pedicle screws of defined diameter. Studies meeting inclusion criteria (2–3) are all linked by the reporting of SD across defined vertebral level(s), allowing for useful comparison between groups. Studies were excluded during the review process for meeting 1 or more of our 8 exclusion criteria: (1) full text article was unavailable, (2) article was not available in English, (3) morphometric study without actual screw placement or description of ideal screw dimension, (4) article contained no significant/sufficient discussion of 1 or more keywords, (5) article consisted of analysis irrelevant to the topic, (6) article discussed cervical or lumbar spinal segments rather than thoracic, (7) article detailed a nonhuman study, and/or (8) studies related to bicortical screw placements. Extraction of relevant data by 2 independent observers followed the review process, and any discrepancies were resolved by the lead author. Given the heterogeneity of the studies involved in this systematic review, we determined early on that it would not be feasible to combine data across studies for use in a quantitative meta-analysis. Instead, we set out to individually examine each study in order to extract the relevant information about the relationships between diameter, strength, and safety, while considering the unique strengths and limitations of each study.
Screw Diameter Selection in Relation to Pedicle Widths
In an attempt to uniform the reported diameters to the documented pedicle dimensions, since pedicles are mostly evaluated in CT axial slices through their transverse width, we calculated the ratios of SD to pedicle width (PW) in studies where both values were reported. In order to compute these ratios, the standard deviations were dropped from the reported values and are thus to be considered as approximations. Average ratios were computed with standard deviations, representing the average ratio of SD to PW by vertebral level across studies. Additionally, we calculated the average breach rate by level as documented in literature, and using 3 of the most referenced morphological studies on the pedicle dimensions, we correlated the breach rate to the PWs and to the adopted SD/PW ratio performing linear regression in Microsoft Excel software (Microsoft Corp., Redmond, Washington).
RESULTS
Search Results
We identified 29 unique articles for inclusion in this review (see Figure 2). Among these studies, 18 provided information for SD selection in relationship to pedicle dimension, 10 reported quantifiable measures of fixation strength, and 10 reported values of breach rate. Studies providing recommendations for screw selection were often morphologic in nature and did not report data on safety/fixation strength of screw insertion. Of these, we reported the provided recommendations, and where possible, we calculated the SD to PW ratio, a measure that has been calculated in prior studies.23,24 Articles reporting fixation strength were further divided between those reporting POS of inserted screws and those reporting maximal insertional torque. Carmouche et al21 provided data on both of these measures of fixational strength and is thus listed twice in the summarizing table. There were 5 articles reporting measures of strength as well as PW22,25–28 and 4 articles reporting breach rate as well as PW.29–32

Systematic review procedure: the exclusion criteria allowed the narrowing to a limited number of papers with detailed information on pedicle width, breach rate, and fixation strength.
Disclosed Criteria for Screw Diameter Selection
Articles which provided explicit recommendations for SD in relation to pedicle dimensions were highly variable (Table 1) and either consisted of a defined SD to PW ratio, a “pedicle fill” model,33 or discussed the clearance necessary between the diameters of the screw and pedicle.
Studies which offered recommendations for screw diameter (SD) in relation to pedicle width (PW): recommendations are reported with their relevant demographic to facilitate comparison across studies.
Suggested diameter values ranged from 80%23 to no more than 125% of PW.24 Two morphometric analyses of PW in different patient populations state that a 0.5 mm margin of cortical bone should be left on both the lateral and medial margins of the screw for safe fixation with both straightforward and anatomical insertion techniques.16,34
An additional study by Christodoulou et al,35 in which the insertion technique is not indicated, simply suggests that SD should be matched as closely as possible to the internal cortical diameter of the pedicle without ever exceeding the outer cortical width. Furthermore, when these studies are grouped by the age of their relevant patient population, only those dealing at least in part with a pediatric population offered recommendations for SD wider than the pedicle.24,36,37 These studies, based on both insertion techniques, define the upper limits for pediatric SD/PW between 1.15 and 1.25.
Of the 10 studies that concurrently reported PW and SD (Table 2), 5 also included measures of fixation strength, and 4 also include measures of breach rate. In an experimental study aimed at identifying criteria for safe diameter selection, Fujimoto et al,32 without specifying the insertion technique adopted, utilized SDs ranging from 4.0 to 6.5 mm and suggested that SDs should be 0.5 mm smaller than the PW. Helgeson et al25 defined the optimal screw size as the screw size equal to, or the first size smaller than, the PW but did not achieve this size in all the tested specimens that were instrumented with the straightforward technique.
Summary of data from studies concurrently reporting screw diameter and pedicle width.
Fixation Strength
Eight studies reported POS in relation to SD,10,22,25–27,38 3 studies reported maximum insertional torque, and 1 study by Carmouche et al21 offered both measures (Table 3). Due to the heterogeneity of the patient populations (age, bone mineral density [BMD], living versus cadaveric, etc), screw insertion techniques, and testing methods, it is not possible to concurrently analyze results across studies. Screw diameters and POSs were often reported as an average across multiple levels, in some cases across the entire thoracic spine, making meaningful comparisons between vertebral level and/or screw sizes impractical across studies. In 4 pullout studies, however, we see a clear intrastudy relationship between increased SD and increased POS.21,22,25,39 A similar relationship is observed in the 3 studies of maximal insertional torque wherein Carmouche et al21 and Mishiro et al40 report increases of 0.43 and 0.033 Nm of torque, respectively, with increasing SDs. The values reported by Matsukawa et al28 appear to break this trend, but this can be accounted for by their use of a novel insertion trajectory that achieved greater cortical bone purchase with a smaller 5.5 mm screw as opposed to a 6.5 mm screw inserted in the standard straightforward technique. The influence of insertion technique on POS has been revealed by studies instrumenting the lower thoracic segments with SDs of about 5.5 mm that have shown higher pullout loads when inserted in the straightforward technique25,38 than in the anatomical trajectory.27
Summary of data from studies which reported screw diameter in relation to a measure of fixation strength.
Breach Ratio
Of the studies that reported breach rates in relation to SD, screw sizes ranged from 3.5 to 7.9 mm, and breach rates ranged from 100% at T3 with a 4.0 mm screw, to 0% at multiple levels with varying SDs (Table 4). Breach was defined differently by multiple studies. In Koktekir et al,41 greater than 25% of the outer SD needed to reside outside the pedicle wall in order to count as breach, whereas Fujimoto et al32 stated that a screw was either contained fully within the pedicle or was counted as breach. Most studies appear to follow the latter model of recording any perforation of the pedicle wall, and Payer et al5 states that, in their analysis, cases of questionable cortical integrity were counted as breach. Furthermore, Belmont et al42 states that medial perforations are safe up to 2 mm, while lateral perforations are safe up to 6 mm. Similarly, Chan et al29 defines safe perforations as less than 2 mm. In the 5 studies that defined the safety of their breaches, only 10 of the 310 cumulative perforations, just 3.23%, were deemed unsafe.
Summary of data from studies which reported screw diameter in relation to breach rate.
Holly et al30 reported breaches mainly in the segments T4–8, where screws 4 mm in diameter were placed in PWs ranging from 4.1 to 4.4 mm. Hart et al31 detailed PW values as well as breach rates. He used 4.0 and 4.5 mm screws and found lateral breach of 100% for 2.99 mm pedicles, which is reduced to 61% for PWs of 4.0 to 4.99 mm, and a minimal breach rate of 13% for PWs of 9.0 to 9.99 mm. Lastly, Fujimoto et al32 divided their specimens into 2 groups which warranted separate reporting in the table. Group 1 screws had a diameter less than the inner PW (ie, the transverse diameter of the inner cortical walls of the pedicle), while Group 2 screws had a diameter greater than the inner PW. According to the findings of Fujimoto et al,32 when SD is selected to be larger than the inner PW, the average breach rate can be as high as 54.5% but can be reduced to 6.3% for screws smaller than the inner PW.
Most of the studies reporting on breach rate did not provide any indication of the insertion technique adopted.43,44 However, a comparison can be made for a 4.5 mm SD inserted into the upper thoracic segments, for which the straightforward technique5 has shown higher breach rates than the anatomical trajectory.30,45
Screw Diameter Selection in Relation to Pedicle Width
Of the 10 studies that concurrently reported PW and SD, Holly et al30 and Liljenqvist et al22 were not included in SD/PW calculations because they reported nonspecific SDs across vertebral levels, making it impossible to calculate meaningful ratios by vertebral level. This left 8 studies with SD/PW ratios to report. In relation to PW, screws inserted with the straightforward technique25 were smaller than screws adopted with the anatomical technique.27,46,47 Xie et al46 provided their own SD/PW ratios with calculated standard deviations, so these were reported without additional calculation and can be considered exact.
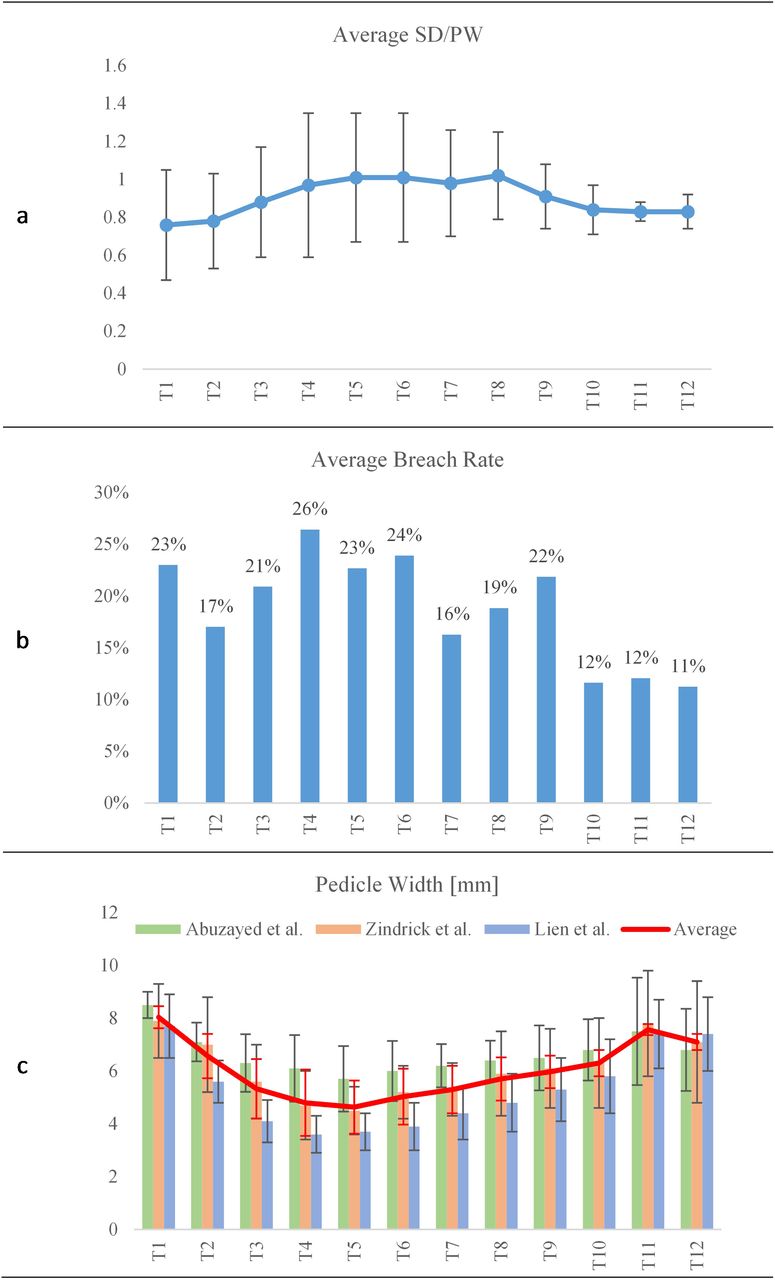
Regardless of the insertion technique adopted, when we calculated the average SD/PW for each vertebral level, we found the lowest value at T1 with a ratio of 0.76 ± 0.29 (see Figure 3), which increased through the midthoracic vertebrae to a peak of 1.02 ± 0.23 at T8 before decreasing towards T12 with a ratio of 0.83 ± 0.09 (Table 5).
Average values calculated for screw diameter (SD) to pedicle width (PW), breach rate, and PW.
Screw diameter (SD) to pedicle width (PW) ratios calculated in the current study (□ indicates studies also reporting on fixation strength and ⋄ indicates studies also reporting on breach rate).
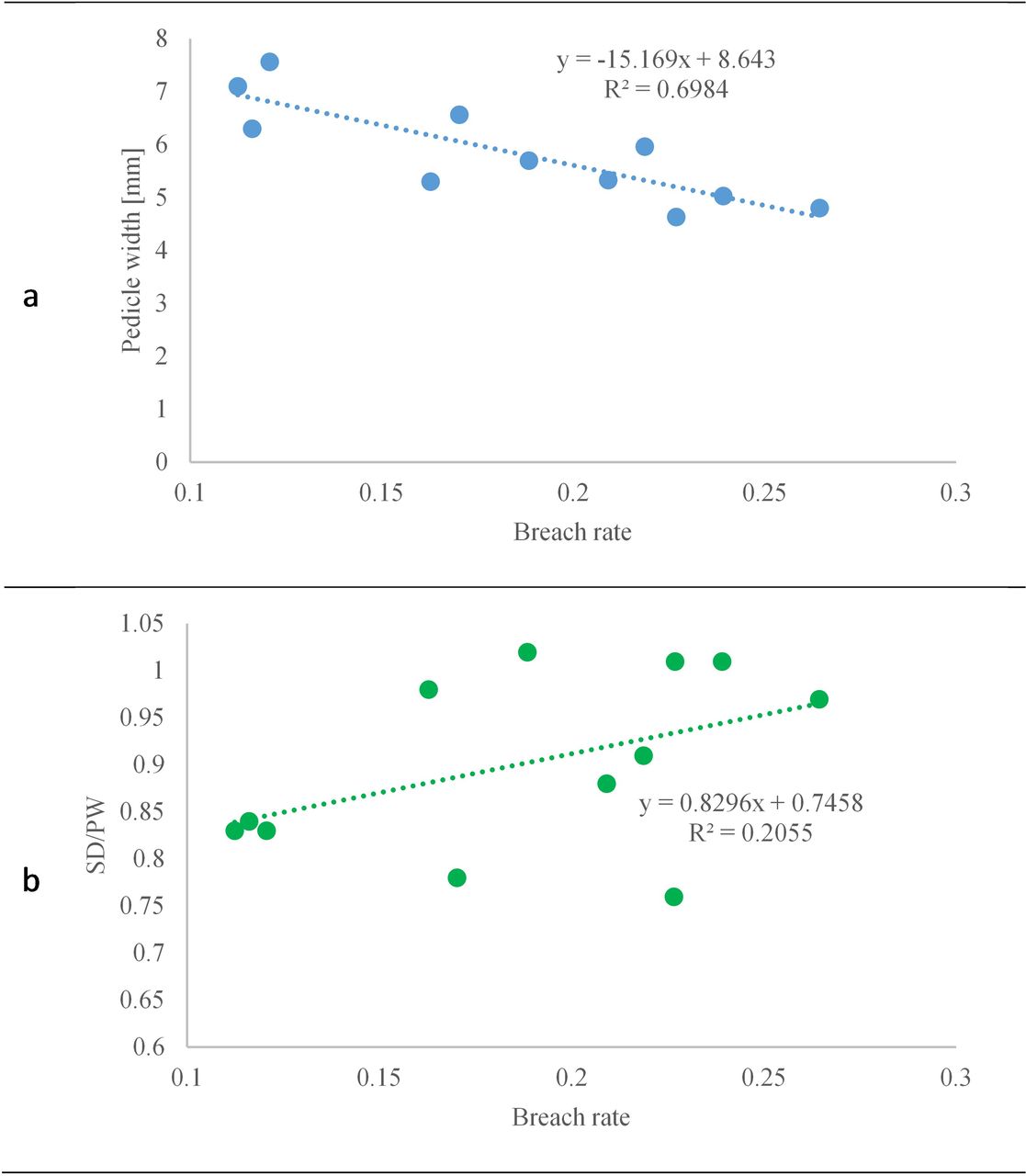
The breach rate has been evaluated as being inversely proportional to the PW, with a coefficient of determination of 0.7 (see Figure 4). The smallest value of breach rate is associated with pedicles of 7.1 mm in width. Considering the entire thoracic spine, a weak correlation (R2 = 0.20) has been found between the breach rate and the SD/PW ratio; however, the smallest values of breach rate are associated with the lower vertebrae T10–12, where very similar ratios within the range of 0.83 ± 0.05 to 0.84 ± 0.13 are used.

Breach rate correlation with (a) pedicle width and (b) screw diameter to pedicle width ratio.
DISCUSSION
The data collected in this review allowed for an overview of SD selection in relation to vertebral level and insertion technique adopted. Despite our best efforts, there are some limitations of this review that should be mentioned. Gender of cadaveric and human subjects was rarely reported in the included studies, even though pedicle diameter has been clearly demonstrated to differ between men and women. As such, we were unable to consider the effect of this variation in our study. Additionally, screw design is clearly an important variable, especially for measures of fixation strength. Screw design and manufacturer were reported where available; however, many studies did not report on screw type. The variability of results among studies is almost certainly due in part to differences in screw design such as thread crest and pitch, which were rarely reported, much less discussed by the included studies.
Furthermore, the SD in relation to PW is meaningless when insertion technique is not disclosed. For example, Helgeson et al,25 using the straightforward technique, reports a mean POS of 877.9 ± 235.2 N with a calculated SD/PW of 0.82, while Hongo et al,27 using the anatomical technique, reports a mean POS of 672 ± 412 N with a calculated SD/PW of 0.86. In addition, Helgeson et al25 reported an average BMD of 0.6 ± 0.07g/cm2, while Hongo et al27 reported an average BMD of 0.8 ± 0.28g/cm2, with the commonly accepted cutoff for osteoporosis stated as density less than 0.9g/cm2. In cases of osteoporosis, BMD has been shown to strongly correlate with POS,38 and the large difference in reported POS between Gayet et al39 and Carmouche et al21 with similar sized screws is likely due to the parallel difference in the BMD of their specimens. Studies such as Carmouche et al,21 cited in this review, have clearly demonstrated the correlation between increased insertional torque and increased pullout resistance in osteoporotic bone. This is likely due to the advantage it provides in achieving greater bony purchase of cortical bone, which can be highly variable between patients due to age,48 as well as demonstrated differences between men and women.34 In recent biomechanical studies, it has been demonstrated that the density of the bone in contact with the screw threads is strongly correlated with POS.49,50 As a result, the variable of SD can be seen as a means of achieving increased cortical bone purchase.
Breach rate peaked among found studies from T4–6 (see Figure 3b), which can be predicted by many studies which characterize T3–7 as having the smallest pedicles, with T5 often reported as the smallest overall.29,35,51 To confirm these relationships, we combined data from 3 frequently cited morphological studies of PW (see Figure 3c), which showed a minimum of 4.63 mm at T5 and a maximum of 7.57 mm at T11.52–54 A direct comparison of average breach rate by vertebral level with the average morphologic values of PW shows a clear inverse relationship between PW and breach rate (see Figure 4a). Considering the entire thoracic spine, a weak correlation (R2 = 0.20) has been found between the breach rate and the SD/PW ratio (see Figure 4b), as seen in previous studies.29,31,32 Despite the poor correlation, breach rates associated with an SD/PW ratio of around 0.8 are consistently among the lowest overall. A ratio of 0.8 then can be reasonably suggested as a conservative starting point for SD selection for the inexperienced surgeon. When we consider the average SD/PW ratios calculated by vertebral level, we see an increase in ratio from T1 to T4 through T8 and a decrease in the lower thoracic spine towards T12. This can be accounted for by the fact that most studies do not make SD selections by individual segment, but rather utilize 1 or 2 SDs over multiple segments, or sometimes over the entire thoracic spine.25,38,55,56 The bandwidth in breach rates seen in Figure 3a can be reduced by greater specificity of screw selection by vertebral level. It should be noted that screw sizes available from the major manufacturers are limited, typically in 0.5 mm increments. Two studies in the current review specifically noted the inadequacy of current pedicle screw systems for instrumenting the midthoracic levels, with Liau et al34 commenting that current systems are not suitable for the majority of the Malay population, and Gstoettner et al36 concluding that one-third of midthoracic pedicles of scoliosis patients cannot be instrumented safely.
A final point of discussion we would like to propose is the clear difference in acceptable SD/PW in pediatric versus adult populations. Of the qualitative studies found, 3 made SD/PW recommendations relevant for pediatric populations and averaged 1.18.24,36,37 These high SD/PW values can be explained by the relative plasticity of the pedicle cortex in the pediatric spine, which has been suggested to be capable of expanding 25% upon screw insertion.24,37
CONCLUSIONS
A commonly accepted criteria for pedicle SD selection in adult thoracic fixation has yet to be proposed in the literature. Although 80% of the PW defines the SD as reported by several authors, this assertion is rarely reported for the midthoracic region of the spine. These vertebras are characterized by relatively narrower pedicles where high pedicle breaches are usually found. This could be associated with the unavailability of SD sizes. In addition, fixation strength has been shown to be associated with BMD and cortical bone purchase, but it is not directly related to the SD/PW ratio. Based on this review of the literature, we believe that proper selection of the SD for individual vertebral level directly affects the insertion technique and the potential breach.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.