


ABSTRACT
Background: Pseudarthrosis following spinal fusion is a complication that frequently requires revision surgery. Reported rates of pseudarthrosis after surgical site infection (SSI) range from 30% to 85%, but few studies have identified infection as an independent risk factor for its development. The purpose of this study was to determine the incidence of clinically symptomatic pseudarthrosis in patient who developed SSI following lumbar fusion and to identify factors associated with its development.
Methods: This was a retrospective review of a prospectively collected database. Patients who underwent spinal surgery and developed SSI between January 2005 and March 2015 with a minimum 2-year follow-up were included. Patient-specific and procedural characteristics were recorded. Presence of pseudarthrosis was determined clinically by the treating surgeon and was confirmed radiographically. All those in the Pseudarthrosis group required a revision procedure after the eradication of infection. Univariate and multivariate analyses were conducted as appropriate.
Results: A total of 416 patients were included. Of these, 21 (5.0%) developed symptomatic pseudarthrosis following SSI. In this cohort, multivariate regression showed that age, Charlson Comorbidity Index, male sex, and surgical approach were not significant predictors of pseudarthrosis formation. However, number of levels fused was found to be the leading predictor for pseudarthrosis development (odds ratio [OR], 1.356/level, P < .001), followed by body mass index (OR, 1.083/point, P < .009) in this cohort. The number of levels fused was found to be a significant predictor of hardware removal (OR, 1.190/level, P < .001). Of the 21 pseudarthrosis cases, 85.7% found staphylococcal species, of which 27.8% exhibited methicillin-resistant Staphylococcus aureus.
Conclusions: The number of spinal levels fused and body mass index are independent predictors of pseudarthrosis in patients who develop SSI after spinal fusion.
Level of Evidence: Level 4
Clinical Relevance: This is the first known study to specifically identify risk factors for the development of symptomatic pseudarthrosis.
INTRODUCTION
Spinal surgery is associated with many serious complications, including pseudarthrosis, neurological injury, paralysis, sepsis, and even death. One of the major problems after spinal surgery is development of surgical site infection (SSI). The literature reports1–7 the incidence of infection following spinal surgery to be between 0.5% and 7%. Significant scientific effort has been exerted to identify risk factors that may predispose patients to infection. Several patient-specific factors such as age, body mass index (BMI), subcutaneous fat thickness, and nutritional status have been implicated, in addition to extrinsic factors such as volume of allogenic transfusion and length of surgery.8–10 Interventions such as the intraoperative application of vancomycin powder to the surgical site and use of negative-pressure dressings have improved infection rates following spinal surgery.11–13 Despite these advancements, infections following spinal procedures continue to present a significant challenge to surgeons and serve as a cause of significant morbidity for patients. In addition to the morbidity, the financial implications of infection and revision surgery cannot be overstated.
The ultimate goal in management of postoperative spinal infections is to eradicate the pathogen without compromising patient function. Aggressive irrigation and debridement of the wound bed with supplemental antibiotic treatment is the standard of care for all deep and most superficial infections. In each case, the surgeon must decide whether to remove existing spinal instrumentation. Hardware retention is typically achievable in cases where the infection is identified early, appropriate antibiotics are started, and the wound is aggressively debrided. However, certain organisms, such as Staphylococcus aureus, coagulase-negative staphylococci, and Pseudomonas aeruginosa, possess the ability to create adherent biofilms on implanted instrumentation, typically necessitating hardware removal for successful treatment. Early hardware removal, aggressive debridement of bone graft, and the physiological implications of infection can all contribute to the development of pseudoarthrosis.14
Reported rates of pseudarthrosis after deep spinal wound infections range from 30% to 85% in the literature, but few studies have identified independent risk factors for the development of pseudarthrosis following infection.15 The purpose of this study was to determine the incidence of symptomatic pseudarthrosis in a cohort of patients who developed SSI after spinal fusion and to identify specific factors that may increase the risk of this complication. In addition, we evaluated whether removal of hardware in the setting of infection resulted in higher rates of pseudarthrosis. To our knowledge, this is the single largest study to date of pseudarthrosis in the setting of infection.
MATERIAL AND METHODS
Study Population
A prospectively collected database at a single institution was retrospectively reviewed to identify all patients who underwent spinal surgery and developed a SSI, as defined by National Healthcare Safety Network criteria, between January 2005 and March 2015.16 Patients who underwent spinal procedures (instrumented decompression and fusion) for trauma, degenerative pathologies, and deformity were included.
Patient Demographics
Clinical data regarding each patient were collected using operative records, billing code queries, patient charts, and clinic notes. Patient characteristics recorded included age, sex, BMI, tobacco use, and Charlson Comorbidity Index (CCI) score.
Surgical Data
Surgical data collected included number of levels fused, duration of surgery, approach, time until development of infection, number of irrigation and debridement procedures, organisms identified in intraoperative specimens, removal of hardware, presence or absence of radiographic and/or clinical/symptomatic pseudarthrosis, and use of vacuum-assisted closure. Pseudarthrosis was determined clinically by the treating surgeon and confirmed radiographically.
All patients included in the Pseudarthrosis group required an instrumented revision procedure following eradication of infection. All patients received prophylactic antibiotic treatment per the standard of care. Microbiologic cultures were collected from all patients who developed deep SSI.
Statistical Methods
Univariate analysis was conducted to compare patients who developed pseudarthrosis after infection with those who did not. Variables included in the analysis were type of surgery, number of spinal levels fused, number of washouts needed for infection control, whether removal of hardware was required, timing of hardware removal (if applicable), whether vacuum-assisted closing devices were used, and pathogens identified in culture.
Multivariate analysis was performed on R version 3.2.2 (Lucent Technologies, Murray Hill, New Jersey) using a Random Forest technique, including a χ2 test, to account for the large number of patient-related factors included in the data analysis and identify potential risk factors for pseudarthrosis. Multiple logistic regression analysis was also performed to determine risk factors for the development of pseudarthrosis, with pseudarthrosis as the categorical dependent variable and the following outcomes/factors as independent variables: age, BMI, sex, CCI number of spinal levels fused, removal of hardware, and surgical approach.
Data management and statistical analysis were performed using Excel 2010 and SPSS version 20 (IBM Corp, Armonk, New York). Results were considered statistically significant when P ≤ .05.
Results
Demographics and Clinical Data
A total of 416 patients were included, consisting of 238 men (57.2%) and 178 women (42.9%) who developed surgical site infection following spinal fusion. Mean age of included patients was 57.1 years (range, 17–87 years). Of 416 patients, 21 (5.0%) developed a clinically apparent pseudarthrosis (Pseudarthrosis group). More detailed information about patient-specific and procedural characteristics can be found in Table 1 and Table 2, respectively. Of the individuals with available BMI values, 112 (30%) patients were overweight, 82 (22%) were obese, and 98 (26.3%) were morbidly obese. There were 81 (21.7%) individuals with a BMI < 25, of whom only 5 (1.3%) were underweight.
Univariate analysis comparison of demographic information between patients who developed pseudarthrosis and those who did not.
Univariate analysis of procedural parameters comparing those who developed pseudarthrosis with those who did not.
The average CCI did not vary significantly between groups: For patients with pseudarthrosis after infection, mean CCI was 3.57 (range, 0–11), compared with 3.30 for patients without pseudarthrosis (Nonpseudarthrosis group; range, 0–17; P = .648). Among Pseudarthrosis patients, 15 cultures were monomicrobial, whereas 6 patients had polymicrobial culture results. More detailed characteristics of the patients who developed pseudarthrosis can be found in Table 3.
Patients with pseudarthrosis.
Aside from spinal fusions involving the lumbar segment (256 patients, 61.5%), all remaining curves were equally affected (cervical: 140 patients, 33.7%; thoracic: 146 patients, 35.1%; and sacral: 113 patients, 27.2%). Surgeries on multiple segments were slightly more frequent than unisegmental fusions (221 patients, 53.1% versus 195 patients, 46.1%, respectively). Almost half of the fusions involved 2 segments only (cervicothoracic: 66 patients, 15.9%; thoracolumbar: 40 patients, 9.6%; and lumbosacral: 98 patients, 23.6%; total = 204 individuals, 49%), whereas surgeries of ≥3 spinal curves were rare (17 patients in total, 4%; of whom only one individual underwent an entire cervico-thoraco-lumbo-sacral fusion).
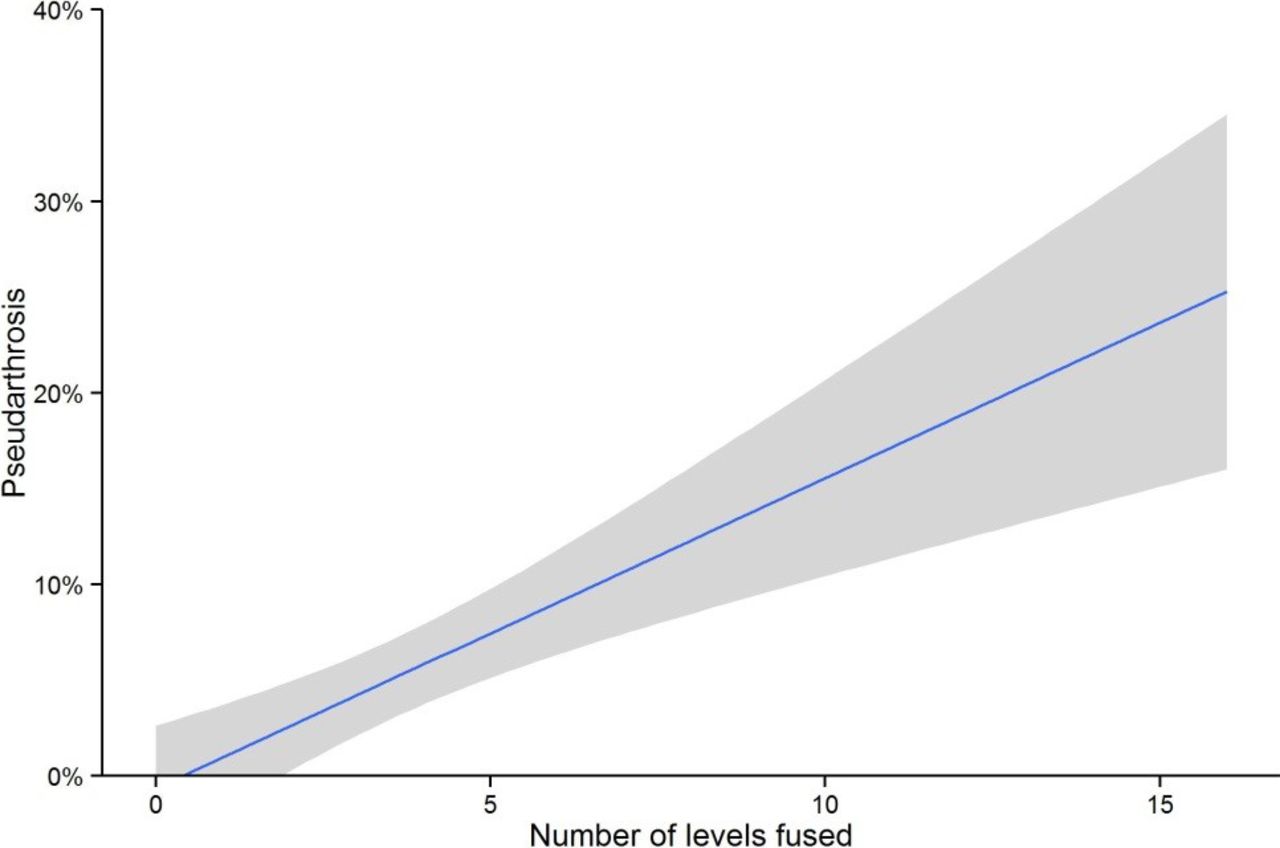
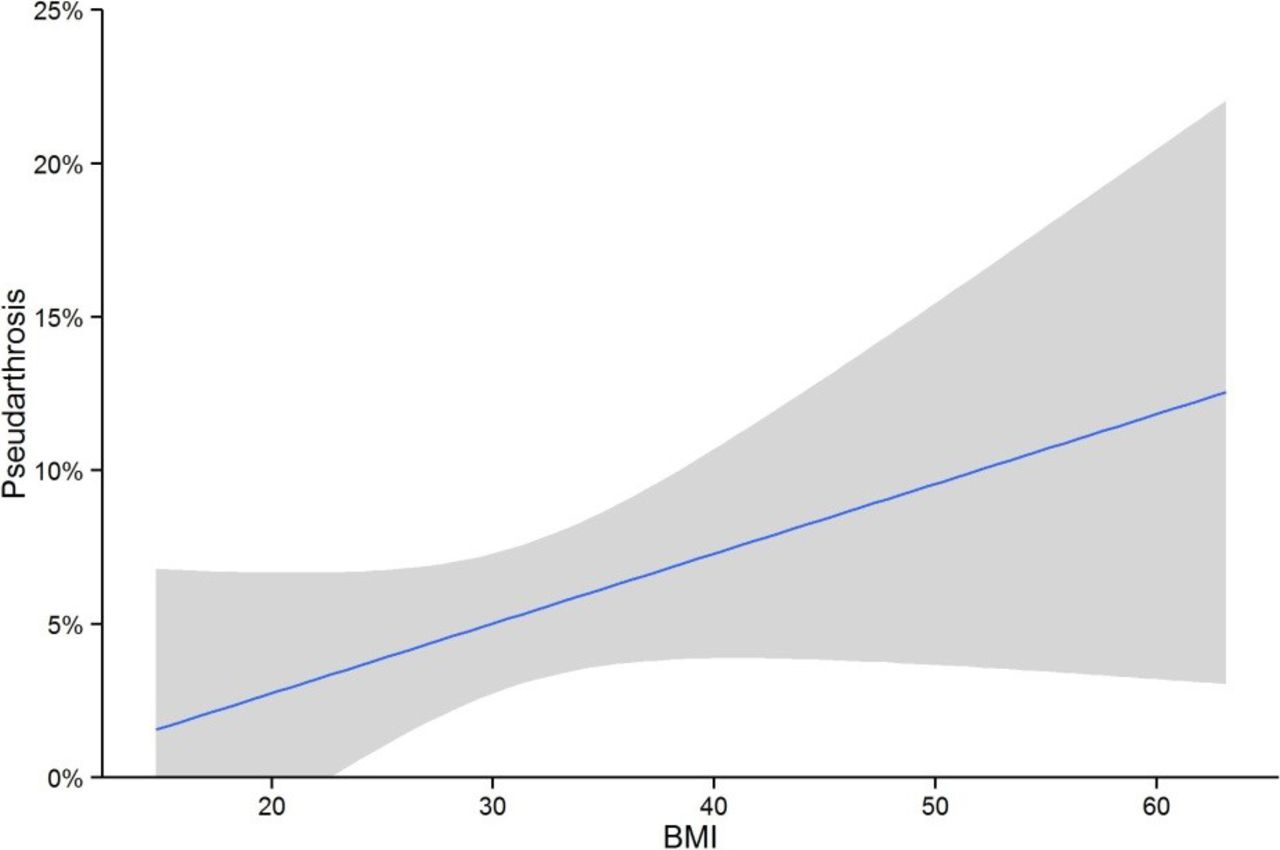
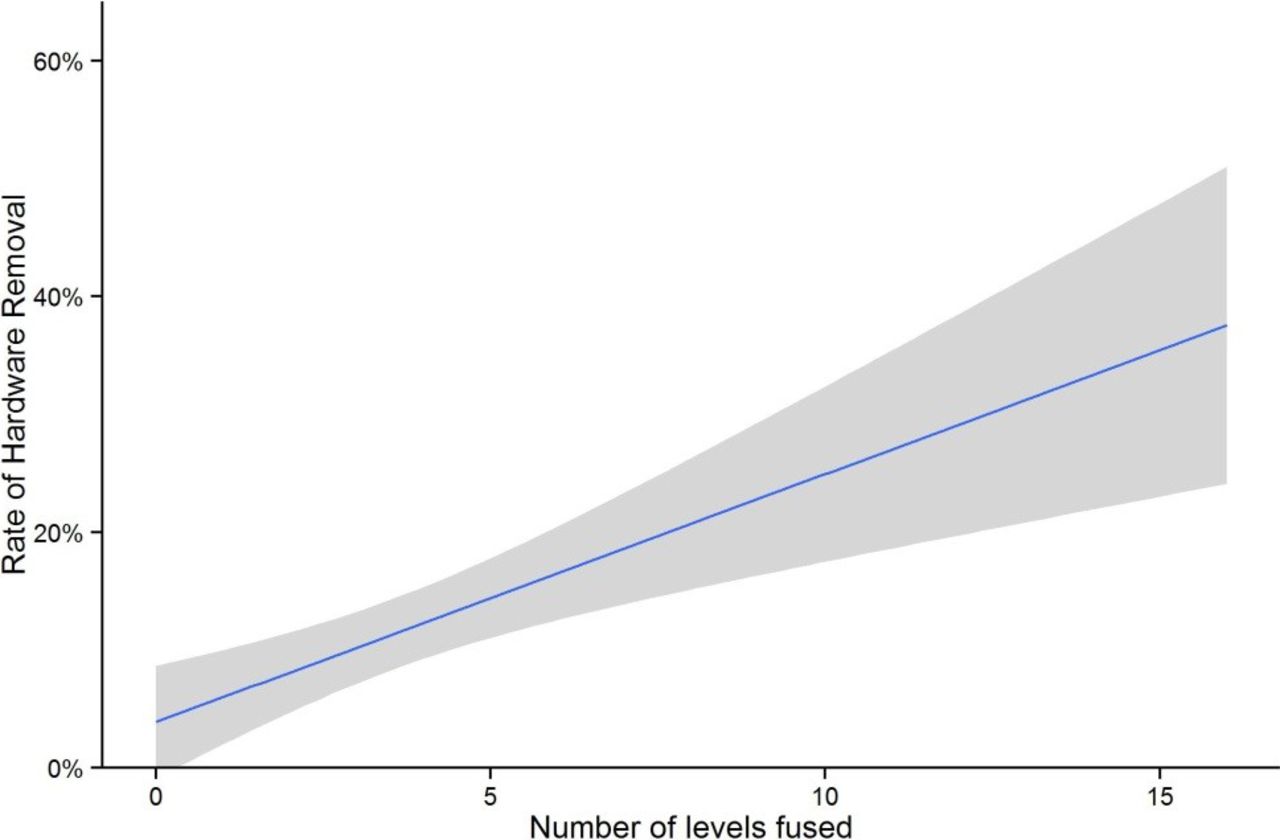
Multivariate regression identified the number of spinal levels fused (odds ratio [OR], 1.356/level, 95% CI, 1.15–1.54, P < .001) as the most significant predictor for the development of pseudarthrosis, followed by BMI (OR, 1.083/point, 95% CI, 1.02–1.15, P = .008; Figures 1 and 2). Age, CCI, sex, and surgical approach were not found to be significant predictors (P > .05). Timing of hardware removal was not significantly associated with development of pseudarthrosis (P = .967). The number of levels fused was found to be a statistically significant predictor of hardware removal (OR, 1.19/level, 95% CI, 1.08–1.30, P < .001; Figure 3).

Variable importance plot of the number of levels fused, showing a statistically significant association with the development of pseudarthrosis. The grey shadow spans the 95% confidence interval region.

Variable importance plot of body mass index (BMI), showing a statistically significant association with the development of pseudarthrosis. The gray shadow spans the 95% confidence interval region.

Number of levels fused associated with removal of hardware. The gray shadow spans the 95% confidence interval region.
Pathogen Culture
Among all 416 patients who developed SSI, cultures showed that 24 pathogens, including 23 bacterial pathogens and 1 fungus, were isolated. Eighteen patients (4.6%) either had no cultures taken or showed no growth once cultures resulted.
The prevalence of gram-positive rods in culture did not vary significantly between groups (80.9% Pseudarthrosis versus 86.3% Nonpseudarthrosis, P = .959); this was also the case for gram-positive cocci (14.3% among Pseudarthrosis versus 9.9% without, P = .435). Rate of identification in culture of gram-negative rods also did not differ significantly between the 2 groups (28.6% in those with pseudarthrosis versus 44.3% in those without, P = .324). Anaerobes were identified significantly more frequently in patients who developed pseudarthrosis than in those who did not (14.3% versus 6.3%, P = .01).
Among the 21 pseudarthrosis cases, staphylococcal species were the most common etiologic agents of infection among all gram-positive cocci (18/21 isolates; 85.7%), with 27.8% of these exhibiting methicillin resistance (5/18). Of the 395 isolates from patients without pseudarthrosis, staphylococcal species were also the most common isolate among gram-positive cocci and were present in 86.1% (324/395) of positive cultures (including 1 case with polymicrobial culture results). Of these isolates, 26.2% (85/324) were further demonstrated to be methicillin-resistant Staphylococcus aureus; the culture rates were comparable between patients with and without pseudarthrosis (P > .05). Overall, methicillin-sensitive S. aureus culture rates did not vary significantly between groups (42.9% among Pseudarthrosis versus 30.6% without, P > .05). Coagulase-negative staphylococci were the next most common agent identified in patients without pseudarthrosis, occurring in 30.6% of nonpseudarthrosis cultures (118/395). More detailed culture results can be found in Table 4.
Results of microbial cultures taken from all patients included in this study.
DISCUSSION
Despite the use of modern antibiotics, SSI remains a relatively common postoperative complication. Infections associated with spinal surgery have a large impact on a patient's postoperative course, often requiring additional open procedures; infection may also increase the risk of other complications, such as pseudarthrosis. As previously mentioned, the postoperative infection rate for spinal procedures has been reported in recent literature1–6 to range from 0.7% to 15.0%.
The present study sought to examine the rate of development of pseudarthrosis in patients with postoperative infection after spinal fusion surgery and to identify patient-specific and procedural characteristics that predicted pseudarthrosis development. To our knowledge, this study examined the largest such infection cohort. Comparison of our results with those of previous studies was difficult, given the dearth of literature describing spinal pseudarthrosis in the context of infection. Nonetheless, several illuminating contrasts were highlighted. In 1997, Weiss et al15 reported on the relationship between SSI and the development of pseudarthrosis in a relatively large series. Of 900 patients who underwent a posterolateral lumbar fusion, 29 (3.2%) developed SSI. Of these, 11 (38%) were subsequently diagnosed with pseudarthrosis. This was a far higher rate than observed in the present study, which may partly be explained by improvements in surgical techniques and implant technology with a resultant increase in successful fusions over the past 20 years.17–19 The fact that the pseudarthrosis patients in the present study were selected specifically because they were diagnosed first clinically and then confirmed radiographically may also have contributed to this discrepancy, because nearly 30% of pseudarthroses have been suggested to be asymptomatic.20 In addition, in the Weiss et al15 study model, female sex, fusion involving the sacrum, and the use of allografts were significant predictors of pseudarthrosis development. Whereas the present study did not identify female sex as a risk factor for development of pseudarthrosis, the percentage of men in the Nonpseudarthrosis group was nearly twice that of the Pseudarthrosis group. The potential for an association between female sex and pseudarthrosis development merits further study.
The results of the present study also contradicted those of Mok et al,21 who performed a small case-control study to determine the impact of SSI on clinical outcomes of posterior spinal fusion as measured by patients' Short Form-36 questionnaire scores. Of 16 patients with postoperative infections, 3 underwent reoperation for pseudarthrosis (19%). The rate of development of pseudarthrosis in the noninfected group did not differ significantly from that of the control group. In addition, none of the variables evaluated—including number of levels fused—were associated with a significant difference in outcomes between the infection group and the control group. However, the number of patients included in the study was very small. Thus, it was possible that associations were missed, which may have helped to explain the contradiction with the results of the present study, which identified BMI and number of spinal levels fused as possible predictors of pseudarthrosis development. Chen et al22 conducted a larger cohort study examining long-term treatment outcomes after postoperative wound infection in patients with posterior spinal instrumentation. They found that 10 of 51 patients required implant removal (19.6%), with an overall pseudarthrosis rate of 31.4%. The overall hardware removal rate was comparable with that of the present study (49/416, or 11.8%), but the pseudarthrosis rate was again much higher in the smaller cohort. This was likely attributed to similar factors described above in contrast with the Weiss et al15 cohort.
Etiologic agents of infection were, overall, comparable between patients with and without pseudarthrosis in this study; we identified staphylococcal species to be the most common infectious agents found in pseudarthroses, a finding consistent with multiple other studies.1,6,8,10 We were surprised that removal of hardware was not a significant predictor in the multivariate regression model despite showing significance in the univariate analysis. This was likely due to bicorrelation; removal of hardware showed a significant association with the number of levels fused (OR, 1.19/level). Thus, each additional level included in the fusion operation may increase the risk of complications, such as subsequent requirement of removal of hardware.
Limitations of the present study included inclusion all of surgical approaches in a single group, without the ability to separately analyze the impact of approach. Posterior approach has a reported association with lower rates of pseudarthrosis development, and an ideal regression model may have better accounted for this covariate.20 In addition, though the sample size was much larger than those of many previous studies, this study identified no impact of sex on pseudarthrosis development, though such an effect has been suggested before.15 Comparison of asymptomatic pseudarthrosis patients with both symptomatic pseudarthroses and patients without pseudarthrosis may prove useful in future studies for further evaluation of the effects of female sex. Future studies with additional radiographic analysis would also aid in examining the effects of spinal alignment on patient-reported outcome measures following revision for pseudarthrosis. Finally, none of the aforementioned studies evaluated risk factors for pseudarthrosis following infection in the specific regional context of the lumbar spine. In this study, 2 factors that were most highly associated with the development of pseudarthrosis following infection were the number of levels fused and BMI. The impact of BMI is well documented in the literature, with obesity established as a risk factor for pseudarthrosis.20,23,24 However, the interplay between patient-specific factors such as BMI, procedural characteristics such as number of levels fused or approach, and the presence of postoperative infection may vary by involved spinal region.25 The present study examined this interplay in the lumbar spine, and future region-specific research should be conducted to examine the specific risks at each level.
CONCLUSION
In a cohort of unprecedented power with specific focus on patients with clinically apparent pseudarthrosis, multivariate logistic regression analysis identified number of spinal levels fused in the index procedure and BMI as significant predictors of pseudarthrosis development following spinal surgical site infections. Further research is recommended to explore the impact of surgical site infection and inflammation on the subsequent development of pseudarthrosis as well as regional specificity of risk factors.
Acknowledgments
The authors would like to thank Susan Lammers for her contributions to this study. This study was approved by the Thomas Jefferson University Institutional Review Board.
Footnotes
Disclosures and COI: No authors had any conflicts of interest or disclosures that have directly or indirectly influenced this study. The following authors have no disclosures: D.A.H., N.V.S., I.D.K., B.G.D. The following authors are consultants for or have received institutional or research support from the following companies: B.I.W.: Altus, NEXXT Spine, Precision Spine, and Stryker; G.D.S.: Advance Medical, AOSpine, Medtronic, Medtronic Sofamor Danek; C.K.K.: Biomet, Medtronic, and Pfizer; M.F.K.: Duratap, Innovative Surgical Designs, and Stryker; P.W.M.: Globus Medical; C.B.P.: DePuy/Johnson & Johnson/Ethicon; A.S.H.: Amedica, Benvenue, Biomet, Lifespine, Nexgen, Paradigm Spine, PSD, Spinal Ventures, and Vertiflex; A.R.V.: Advanced Spinal Intellectual Properties, Aesculap, Atlas Spine, Avaz Surgical, Bonovo Orthopaedics, Computational Biodynamics, Cytonics, Dimension Orthotics, Electrocore, Elsevier, Flagship Surgical, FlowPharma, Gamma Spine, Gerson Lehrman Group, Globus Medical, Guidepoint Global, Health Point Capital, In Vivo, Innovative Surgical Design, Insight Therapeutics, Medacorp, Medtronic, Nuvasive, Paradigm Spine, Parvizi Surgical Innovations, Prime Surgeons, Progressive Spinal Technologies, Replication Medica, Small Bone Innovations, Spine Medica, SpineWave, Spinology, Springer, Stout Medical, Stryker, Taylor Francis/Hodder & Stoughton, Thieme, Vertiflex, and Vexim; K.E.R.: 4 Web Medical, Globus Medical, Medtronic, NEXXT Spine, Nuvasive, Orthofix Inc, Orthopedic Sciences Inc, Pacira Pharmaceuticals, Simplify Medical, Stryker, and Zimmer.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2019 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.