


ABSTRACT
Background: Previous studies stratified postoperative infection risk by patient comorbidities. However, it is unclear whether the incidence varies by surgical approach in a specialized orthopaedic setting. This study aims to compare infection rates and microbiologic characteristics of postoperative spine infections requiring return to the operating room for debridement by hospital setting: a dedicated orthopaedic and spine hospital versus a general hospital serving multiple surgical specialties.
Methods: The study is a retrospective review of prospectively collected data. Procedures performed between March 2006 and August 2008 at the multispecialty university hospital were compared with cases at an orthopaedic specialty hospital from September 2008 through August 2016. The surgeons, residents, and patients were similar, but the operative venue changed in 2008.
Results: The overall general university hospital infection rate was 2.03%, higher than the overall infection rate at the dedicated orthopaedic and spine hospital of 1.31% (P < .0104). The general university infection rate was 2.27% in the final years of practice, compared with 0.91% at the dedicated orthopaedic and spine hospital (P < .0001) during a recent 2-year time frame. Demographic variables did not significantly differ between the 2 settings. The overall proportion of Gram-negative infection rates was not statistically different (21.7% vs 18.6%), despite an increased proportion of Gram-negative infections at the general university hospital following surgery from an anterior approach. Most of the organisms isolated in both facilities were Staphylococcus species. There was no difference in the seasonality of postoperative spine infections in either setting.
Conclusions: In transitioning from a multispecialty university hospital to a dedicated orthopaedic hospital, the incidence of postoperative spine infections was significantly reduced to 0.91%. Despite the change in venue, the proportion of Gram-negative infections (∼20%) following spine surgery did not significantly change. These results suggest improved infection rates during the course of the last 10 years with consistent proportions of Gram-negative infections.
Level of Evidence: 3.
- spine
- Gram-positive bacteria
- hospital setting
- specialty hospital
- seasonal variability
- demographic variables
- anterior approach
- posterior approach
- postoperative infection
- microbiology
INTRODUCTION
The incidence of spinal pathology that may necessitate surgical intervention likely will increase, given the 113% increase in lumbar fusions performed between 1996 and 2001.1 With an increase in surgical volume, there will likely be an increase in postoperative complications and infections. Currently, 0.7% to 4.2% of spine surgeries result in infection.2 Consequently, it will be critical to understand characteristics that contribute to postoperative infection development and prevention. Several methods exist to reduce the risk of postoperative infections, such as perioperative prophylactic antibiotics given prior to and during surgery. The most common prophylactic antibiotic regimen consists of cephalosporins.3,4 However, because of the increased incidence of methicillin-resistant Staphylococcus aureus (MRSA),5,6 the use of vancomycin has increased, especially at institutions with resistant bacterial strains. However, previous studies of intraoperative application of vancomycin powder have revealed mixed results. For example, an increased incidence of spinal infections and life-threatening side effects,7,8 as well as a decrease in infection rates following spine surgery from 10.9% to 2.5%,2,9 have been reported. Furthermore, it is unclear whether current antibiotic prophylactic regimens provide sufficient microbiologic coverage.10,11 Thus, there are conflicting views regarding the routine use of intraoperative vancomycin powder within the wound site and whether proposed alternative antibiotic regimes could benefit spine surgery patients; future studies will be beneficial to clarify guidelines.
Another method to reduce the risk of complications following surgery is the development of centers of excellence for hospital specialization. In particular, in the past 20 years the fields of cardiac and orthopaedic surgery have moved toward specialty-specific hospitals, which have shown decreased mortality and readmission rates compared with general hospitals, where multiple types of surgery are performed.12,13 The creation of specialized hospitals has also been found to result in improved postinjury recovery compared with a general setting.14 Taken together, these studies suggest that infection rates could be further decreased in a specialty hospital setting compared with a general hospital serving multiple specialties.
Despite prophylactic antibiotic regimens and attempts during surgery to decrease infection development, postoperative spine infections occur and increase morbidity and mortality in affected patients.15–17 Typically, postoperative spine infections are colonized with Gram-positive bacteria, mostly from the Staphylococcus species.17,18 There is also an increased infection risk following surgery from a posterior approach, compared with an anterior approach.19–21 However, it is currently unclear whether the microbiologic characteristics of postoperative spine infections differ between hospital settings and whether the incidence varies by surgical approach in a specialized orthopaedic setting.
Therefore, we sought to determine the incidence rates and microbiologic characteristics of postoperative spine infections requiring return to the operating room for debridement following spine surgeries at a general university hospital compared with a dedicated orthopaedic hospital.
METHODS
Institutional Review Board approval was obtained for this retrospective study examining prospectively collected infection surveillance data at a single academic institution. The surveillance program began in March 2006. A total of 12 845 consecutive cases performed at a single academic medical center from 2006 through 2016 were included. From March 2006 to September 2008, all cases were performed at the general university hospital, where multiple surgical specialties operated within the same facilities. However, in 2008, upon the opening of the dedicated orthopaedic specialty hospital, all spinal procedures were moved to this facility. The attendings, residents, and patient population remained the same, but the operative and postoperative locations changed. Infection was defined clinically as the need for intravenous antibiotics and/or repeat irrigation and debridement within 1 year of index procedure, in accordance with the Centers for Disease Control and Prevention guidelines for a surgical site infection22,23 and according to clinical judgment by the treatment team based on factors including, but not limited to, wound drainage and patient-reported fever or chills.
Demographic variables were collected, including age, body mass index, sex, diabetes status, steroid use, and smoking history. Operative variables were collected, including whether lumbar instrumentation was performed, whether procedures were a primary surgery or revision, whether procedures involved a complex deformity (defined as >6 levels), as well as procedure date, which was used to categorize the procedure season of winter, spring, summer, or fall. Infection variables were collected, such as the cultured bacteria, including organism species, as well as whether an anterior cervical infection specifically occurred.
Mann-Whitney U nonparametric test or χ2 analysis was performed using GraphPad Prism software (San Diego, CA). Significance was set at P < .05.
RESULTS
Infection Incidence Reduced at Dedicated Orthopaedic Hospital
The overall infection rate at the general university hospital was significantly higher, at 2.03%, compared with the 1.31% rate at the dedicated orthopaedic hospital (P < .0104; Table 1). Furthermore, when comparing the final 2 years of practice at the general university hospital to the most recent 2 years of practice at the dedicated orthopaedic hospital, there was a decreased infection rate from 2.27% at the general university hospital to 0.91% at the dedicated orthopaedic hospital (P < .0001; Table 1). The 2-year incidence rates were subcategorized by procedure type: spinal instrumentation, primary, or revision surgery. There was a decreased infection rate at the dedicated orthopaedic hospital for procedures that involved instrumentation (P = .0394), noninstrumentation (P = .0006), and primary surgeries (P = .0003). There was no difference in the infection rate of revision surgeries (P = .1067; Table 2). These results indicate that the change in setting and improvements during the last 10 years from a general university hospital to a dedicated orthopaedic hospital resulted in a reduction in postoperative spine infections.
Decreased overall and 2 year incidence rates at a dedicated orthopaedic hospital.a
Decreased 2-year incidence rate at a dedicated orthopaedic hospital for subcategorized procedure types.a
No Substantial Differences in Demographics Between Hospital Settings
Because particular demographic factors, such as obesity, smoking, and diabetes, have been associated with an increased risk of postsurgical spine infections,21,24–26 demographic variables that could account for the differences in infection rates observed were analyzed. At the general university hospital, the mean age of infected patients was 53.8 years, compared with 62.2 years at the dedicated orthopaedic hospital (P = .0020). This was surprising, given that older patients are at increased risk for developing postoperative complications and infections.26 Furthermore, in infected patients there were no differences in the body mass index (P = .3645), proportion of males and females (P = .7651), or proportion of diabetic patients (P = .8571) between the 2 locations. Additionally, <25% of infected patients were diabetic and >50% of patients were nonsmokers (Table 3). Two patients developed an anterior cervical infection at the dedicated orthopaedic hospital, representing 2.2% of all infected cases, compared with no anterior cervical infections at the general university hospital (P = .3111). Furthermore, there were no differences in the rates of lumbar instrumentation (P = .7664) or procedure complexity (P = .1642) at the general university compared with the dedicated orthopaedics hospital (Table 4). The most common prophylactic antibiotic administered in either setting was cephalosporins, with a 99% overall prophylactic antibiotics adherence rate.
Demographic variables at a general university versus a dedicated orthopaedic hospital.
Operative variables at general university versus dedicated orthopaedic hospital for combined postoperative spine infections, regardless of surgical approach.a
Subgroup analysis of infections in anterior procedures between the 2 facilities showed no difference in sex (P = .9999), proportion of diabetes (P = .6405), and smoking status (P = .1056) in the 2 hospital settings. Additionally, subgroup analysis of infections in posterior procedures showed no difference in sex (P = .9509), proportion of diabetes (P = .9426), and smoking status (P = .7446) in either setting (Table 5).
Demographic variables at general university versus dedicated orthopaedic hospital for anterior and posterior post-operative spine infections.a
No Differences in Microbiologic Characteristics
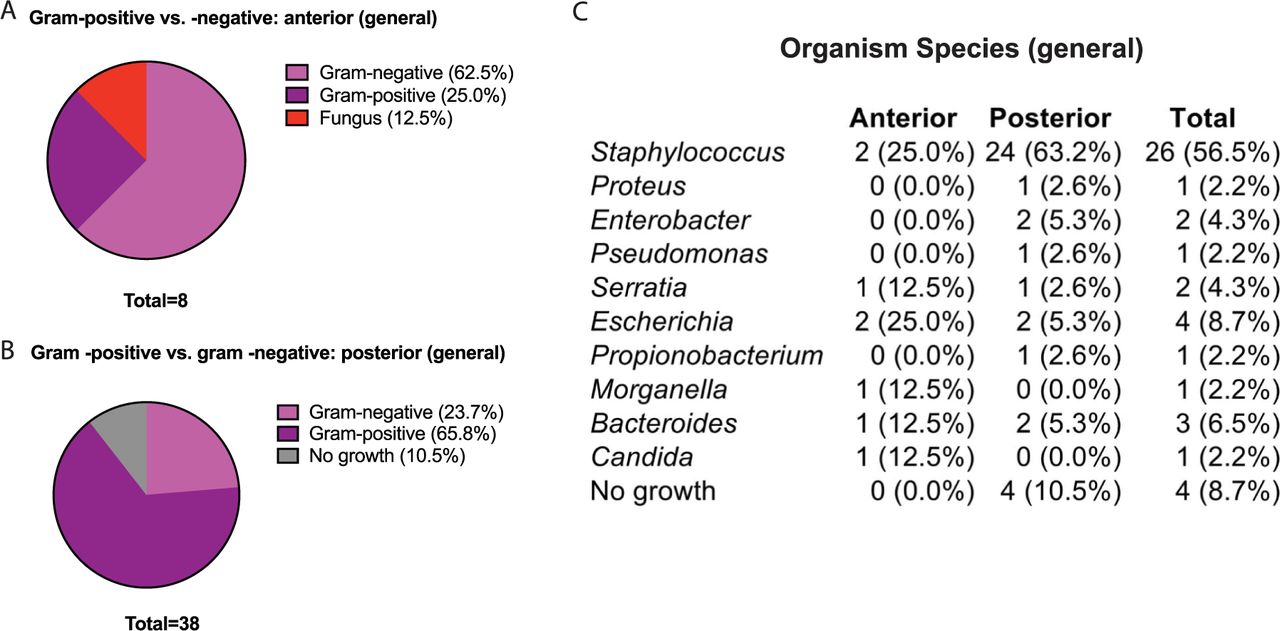
Because procedures from a posterior approach have been associated with greater likelihood of infection development19–21,27 and the prevalence of Gram-positive bacteria is high in postoperative orthopaedic infections,17,18 the microbiologic characteristics of spine infections at the general university hospital were compared to the dedicated orthopaedic hospital subgrouped by surgical approach. At the general university hospital, there was a nonsignificant trend toward more Gram-negative infections in patients who underwent spine surgery from an anterior approach (Figure 1A). In contrast, there was a nonsignificant trend toward Gram-positive infections in patients who underwent spine surgery via a posterior approach (Figure 1A). However, when the cultured organisms from both anterior and posterior approaches combined at the general hospital were examined, Staphylococcus species dominated as the causative organism (Figure 1C), consistent with previous studies.17,18,26
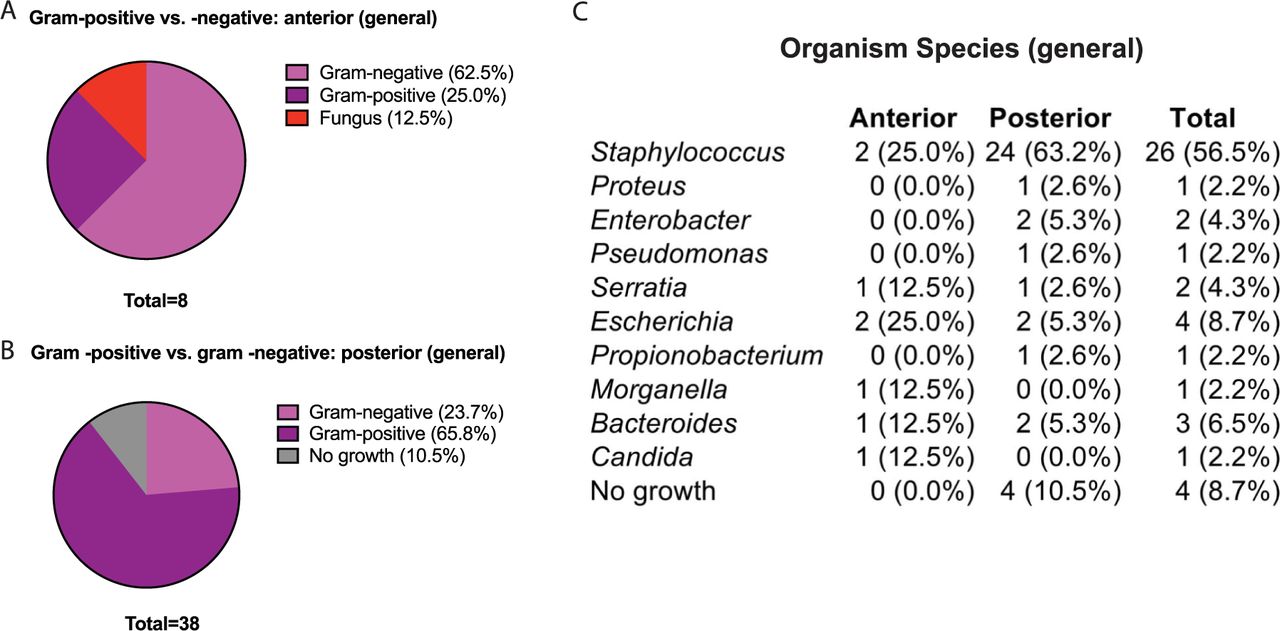
At the general university hospital, infections from an anterior approach were primarily from Gram-negative bacteria, whereas infections from a posterior approach were primarily from Gram-positive bacteria. (A) The percentage of Gram-negative and Gram-positive infections at the general university hospital following an anterior approach. (B) The percentage of Gram-negative and Gram-positive infections at the general university hospital following a posterior approach. (C) Organism species cultured from postoperative spine infections at the general university hospital following an anterior or posterior approach.
At the dedicated orthopaedic hospital, most postoperative spine infections were also due to Gram-positive bacteria, regardless of an anterior or posterior approach (Figure 2, A and B), with most infections due to Staphylococcus species (Figure 2C). Overall, there was no difference in the percentage of Gram-negative infections at the general university hospital compared with the dedicated orthopaedic hospital (21.7% vs 18.6%, respectively; P = .7430) nor in the diversity of cultured organisms (P = .3974). Taken together, these findings indicate that despite the trend toward gram-negative infections from an anterior approach at the general university hospital, most infections were due to Gram-positive bacteria, with approximately 20% of the infections from Gram-negative species in both settings.

At the dedicated orthopaedic hospital, infections from an anterior or posterior approach were primarily from Gram-positive bacteria. (A) The percentage of Gram-negative and Gram-positive infections at the dedicated orthopaedic hospital following an anterior approach. (B) The percentage of Gram-negative and Gram-positive infections at the dedicated orthopaedic hospital following a posterior approach. (C) Organism species cultured from postoperative spine infections at the dedicated orthopaedic hospital following an anterior or posterior approach.
Seasonal Variability of Infections Not Found Between 2 Operative Settings
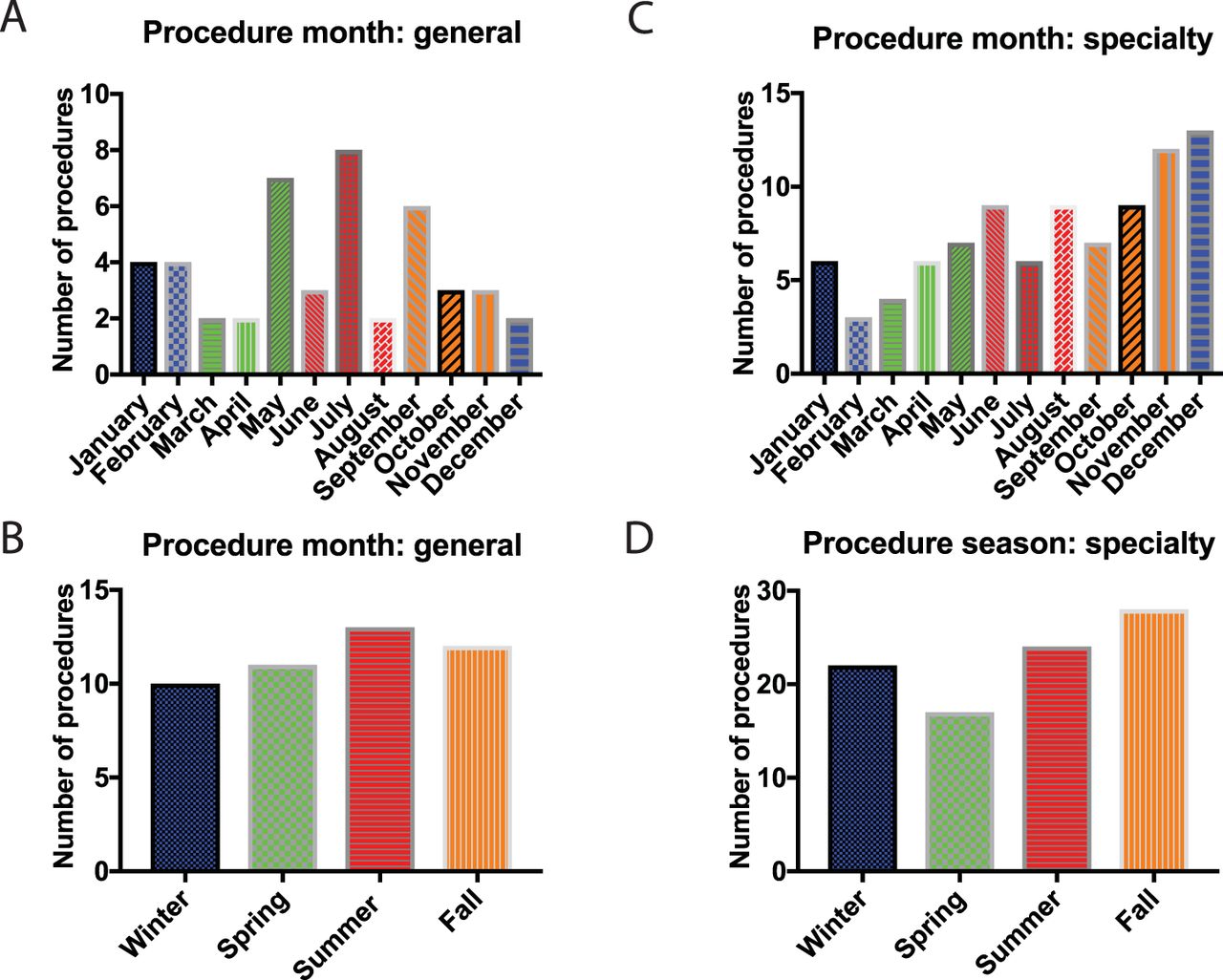
Because an increase in postsurgical spine infections has been reported in the summer,28,29 the procedure month and season of index cases, which later resulted in infection development, at the general university hospital versus the dedicated orthopaedic hospital were compared. There was no statistically significant difference in the procedure month (P = .2195) or season (P = .8598) between the general university hospital and dedicated orthopaedic hospitals (Figure 3).
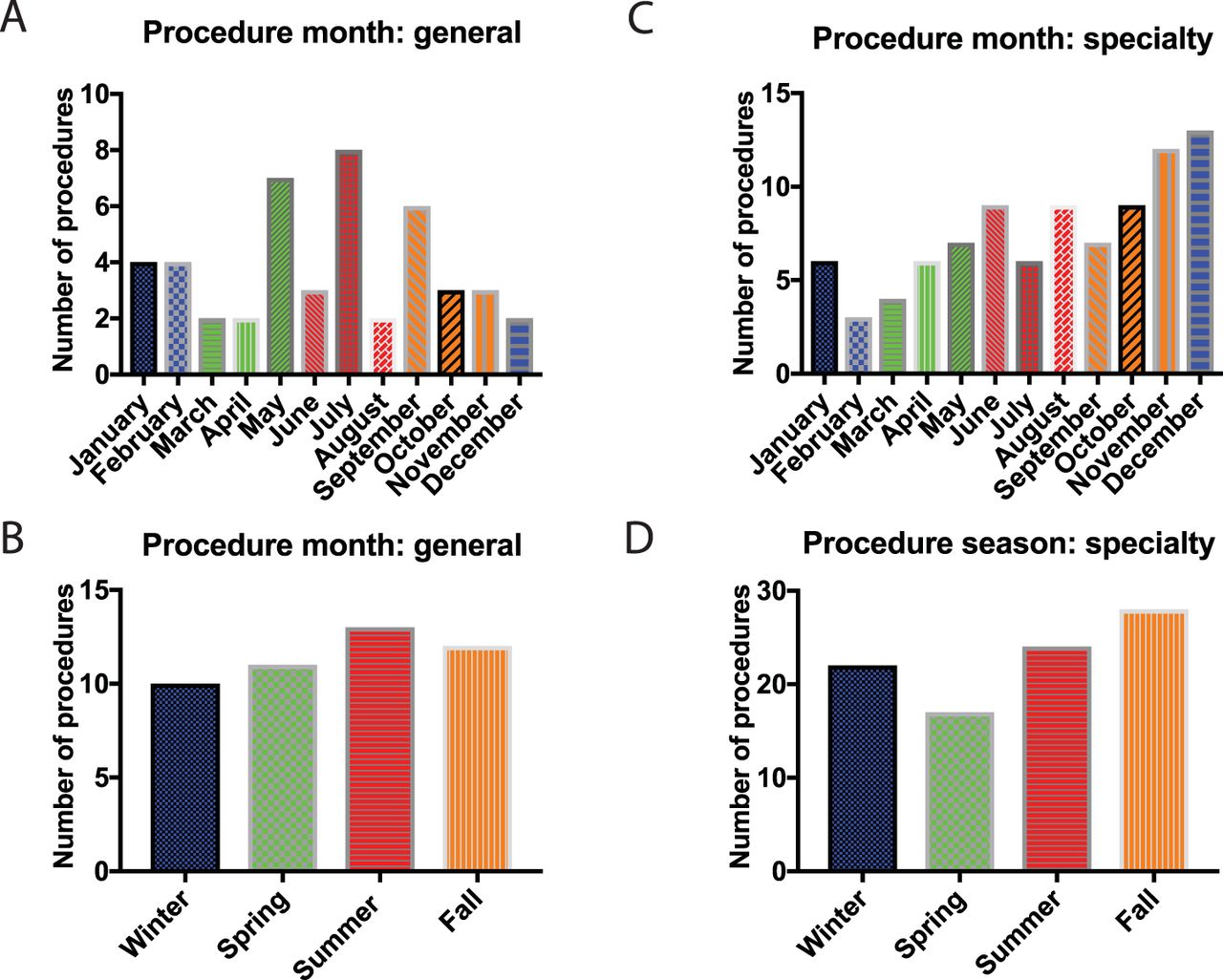
There were no observed differences in seasonality or procedure month between postoperative spine infections in the general university hospital and dedicated orthopaedic hospital. (A) Procedure month that a postoperative spine infection occurred at the general university hospital. (B) Procedure season that a postoperative spinal infection occurred at the general university hospital. (C) Procedure month that a postoperative spinal infection occurred at the dedicated orthopaedic hospital. (D) Procedure season that a postoperative spinal infection occurred at the dedicated orthopaedic hospital.
DISCUSSION
Orthopaedic care has started transitioning from general hospitals to specialized care at orthopaedic-specific hospitals, with the thought that specialty care could provide patients with decreased complication rates and better outcomes. Although the literature regarding specialty spine care is limited, the outcomes of hip and knee arthroplasty in specialty versus general hospitals have been more widely studied. For example, Cram et al30 found that patients who received hip and knee replacements at a specialty hospital had lower infection rates and a decreased risk of an adverse outcome compared with replacements at a general hospital. In a prospective study, Phillips et al31 observed a <1% infection rate in patients undergoing hip and knee replacements at a specialty hospital, indicating that specialty hospitals can lead to very low infection rates. In that cohort, Staphylococcus species were the most common causative organisms, in support of previous studies17,18,26 and our findings presented here. In this study, there was a significant decrease in the overall incidence of spine infections after the transition from the general university hospital to a dedicated orthopaedic and spine hospital, from 2.03% to 1.31% during the 10 years studied, with a greater decrease in infection rate during the most recent 2 years of practice in either setting (2.27% vs 0.91%). These results suggest that specialty orthopaedic care could decrease the rates of postoperative spine infections, but the reason behind this decrease is likely multifactorial.
In our study there was minimal difference in the demographic data between the groups. Despite the association of diabetes and smoking with later development of postoperative infections,21,24–26 <25% of infected patients were diabetic in both the populations. Furthermore, >50% of the infected patients were nonsmokers in both cohorts, again indicating that these patient variables may not be solely responsible for infections. Microbiologic characteristics examined in these 2 cohorts revealed that in both settings Gram-positive infections with Staphylococcus species were primarily responsible for infections, regardless of whether the operations were performed via an anterior or posterior approach, in support of previous studies.17,18,26 Interestingly, in infections following anterior spinal procedures at the general university hospital most were Gram-negative infections, whereas at the dedicated orthopaedic hospital, most infections were due to Gram-positive bacteria. However, the number of infections following anterior spinal surgeries was low (n = 8 patients) following an anterior approach at the general university hospital. Given this small number of infections, it would be an overinterpretation to conclude that the rate of Gram-negative infections was higher at the general university hospital, specifically when using an anterior approach, given the small sample size and the lack of literature supporting the association between Gram-negative colonization and anterior spinal surgeries.
The microbiologic profile of infections was especially interesting in our particular patient population, because we have previously observed that the rates of prosthetic joint infections were decreased at the dedicated orthopaedic hospital compared with the general university hospital.32 However, in our prosthetic joint infections data, the overall rate of infection was reduced (0.75% vs 1.43%), with a higher proportion of Gram-negative infections (25.3% vs 5.3%) at the dedicated orthopaedic hospital. Therefore, we hypothesized that the same trend may follow in the population of patients following spine surgery; however, there was no significant change in the microbiologic profile of spine infections between the two facilities.
Given that there were no differences in demographics, microbiologic characteristics, or seasonality between infections at the general university hospital and the dedicated orthopaedic hospital, our findings suggest that the specialty hospital venue and care pathways could contribute to the decrease in overall infection incidence. Indeed, previous studies have shown that hospitals are a source of bacterial exposure, even to multidrug-resistant organisms. For example, Lemmen et al33 sampled 20 locations within a German hospital, ranging from patients themselves to hospital gowns, door handles, and floors. Within the hospital environment, the detection rate for vancomycin-resistant Enterococci and MRSA was 24.7%.33 French et al34 compared the environments of non–MRSA-infected patients to those of MRSA-infected patients, finding that 74% of swabs from environments of MRSA patients yielded MRSA.34 In cultures of hospital dust, MRSA can still be isolated after more than a year.35 Environmental factors, such as the bacterial environment in hospitals and operating rooms, may predispose patients to later development of postoperative infections.33–37 Therefore, we hypothesize that the newer facility, with a decrease in the variety of operations performed, may contribute to an overall more sterile environment, leading to the decreased infection incidence observed, though this would be difficult to prove empirically. Dedicated orthopaedic hospitals can provide consistent personnel with greater attention to reducing operating room traffic, stricter adherence to Surgical Care Improvement Project guidelines, and sterile supply equipment and staff focused only on orthopaedic care. Further research examining the microbiological burden within each hospital and operative setting may further elucidate inherent bacterial colonization differences in the general university hospital versus the dedicated orthopaedic hospital, which is beyond the scope of this study.
Strengths and Weaknesses
One strength in this study is the large number of patients captured within a single university system, with the same attending surgeons and resident training program throughout data collection. The major change of the location of spine procedures during the 10-year period allowed us to examine how hospital setting affected the infection rate following spinal surgery, and limit variability in other factors. Despite this study design, one weakness was the overall small rate of infection. Although the number of infections may have been larger if a national data set was used, it can often be difficult to draw concrete conclusions given the variability in data input into these national databases. Furthermore, although we do not have data available for the relative surgical invasiveness scores between the practices, the overall surgical practices did not differ during this time period or between facilities. The surgeons, university training program, and Case Mix Index values were constant between facilities, limiting any change in relative surgical invasiveness scores between the facilities. Given that we compared data from postoperative infections at the general university hospital from 2006–2008 to data from the specialty hospital in 2008–2016 and showed an even more significant decrease in infection rate in the most recent 2 years at the specialty hospital, we may not be able to fully account for subtle changes that occurred in the intervening years to improve quality of care and reduce infection rates independent of moving facilities. Furthermore, because no orthopaedic procedures have been performed at the university hospital since the transition in 2008, it would be impossible for us to infer whether operations performed at the general university hospital more recently would have decreased infection rates because of improved quality of care or infection prevention protocols. Additionally, although intrawound vancomycin was starting to be used sporadically after the transition to a specialty hospital, to date we have not seen a significant change in infection rate directly due to intrawound vancomycin. This study was not focused on the intraoperative use of powdered vancomycin, and we are unable to conclude if its sporadic use affected the bacterial profile. Finally, although we are unable to quantify measures of stricter adherence to Surgical Care Improvement Project guidelines or reduction in operating room traffic at the specialty hospital, the dedicated orthopaedic-specific surgical teams and consistent attention to sterility are paramount for reducing infections in spine surgery.
Conclusions
In this study, we sought to determine whether the incidence of spine infection requiring return to the operating room differed following the transition from a general university hospital to a dedicated orthopaedic hospital. The overall infection rate (2.03% vs 1.31%) and most recent 2-year infection rate (2.27% vs 0.91%) were significantly reduced following the transition of care to the dedicated orthopaedic hospital. There were no differences in demographic, microbiologic, or seasonal factors between the locations of care. It is possible that this decrease in infection rate may reflect improved characteristics unique to dedicated orthopaedic and spine hospitals. These results highlight the important and growing role of dedicated orthopaedic hospitals in infection prevention and improved care following spine surgery.
Footnotes
Disclosures and COI: The authors have no competing financial interests.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.