


ABSTRACT
Background: Minimally invasive (MIS) techniques have gained considerable attention for the management of degenerative spinal pathologies. However, few studies have compared the outcomes between MIS and open thoracolumbar corpectomies. The purpose of this study was to compare perioperative variables between MIS and open thoracolumbar corpectomy.
Methods: Retrospective review of 33 patients who underwent either an MIS or open thoracolumbar corpectomy by a single surgeon between 2005 and 2012 was performed. Patients were separated into anterior-posterior MIS (MIS AP), anterior-posterior open (AP), and posterior open (P) cohorts. Postoperative narcotic use was converted to oral morphine equivalents (OMEs). Demographics, comorbidity, perioperative variables, complications, and computed tomographic analyses were assessed. Fisher exact test was performed for categorical variables and Student t test for continuous variables. A P value of ≤ .05 denoted statistical significance.
Results: Thirty-three patients underwent an MIS AP, AP, or P thoracolumbar corpectomy (39.4% vs 15.2% vs 45.5%, respectively). MIS AP patients were younger with a lower comorbidity burden than either open cohorts. In addition, MIS AP patients demonstrated a decreased procedural time, lower blood loss, and shorter hospitalization than either open cohorts. MIS AP patients required less units of transfusion than P and AP patients while demonstrating lower postoperative narcotics consumption and reoperations rates than open AP patients. Surgical site infection rates, body mass index, intraoperative fluid requirements, and complication rates were similar between cohorts. All patients demonstrated successful arthrodesis at 1 year based upon computed tomography.
Conclusions: MIS AP thoracolumbar corpectomy patients incurred decreased procedural times, shorter hospitalization, and lower blood loss compared with open patients. MIS AP patients demonstrated decreased postoperative narcotics consumption and reoperation rates compared with traditional AP patients. All patients demonstrated successful arthrodesis.
Clinical Relevance: The MIS approach to thoracolumbar corpectomies appears to be a safe and efficacious alternative when compared with traditional methods.
INTRODUCTION
Pathologies involving the structural integrity of the vertebral bodies can pose a technical challenge for spine surgeons. Traditionally, thoracolumbar corpectomies have been used for a wide range of spinal pathologies including metastatic disease, burst fractures, and osteomyelitis. These procedures facilitate a thorough neural decompression while offering a biomechanically sound stabilization. However, traditional open thoracolumbar techniques have been associated with complication rates as high as 79%.1–5 Posterior-based (extra-cavitary) approaches are associated with incomplete visualization of the anterior structures, which can lead to unsatisfactory decompression and instrumentation.6,7
Minimally invasive (MIS) techniques for spine surgery has demonstrated decreased blood loss, reduced postoperative pain, shorter hospitalization, and lower infection rates in the setting of degenerative spinal conditions.8–10 However, evidence for the use of MIS corpectomies via a limited anterior-posterior (AP) approach has been limited to small series with heterogeneous populations. As such, the purpose of this study is to compare the perioperative outcomes, complications, and fusion rates between MIS and traditional open thoracolumbar corpectomies for conditions including tumor, infection, and trauma.
METHODS AND MATERIALS
Patient Population
Internal institutional review board approval was obtained to retrospectively review a prospectively maintained registry for all patients who underwent a single-level thoracolumbar corpectomy by a single surgeon between 2005 and 2012. All patients presented with nonmechanical pain, dynamic instability, or neurologic compression (ie, radiculopathy, myelopathy, or myeloradiculopathy). Patients with hemicorporectomies, cervical pathologies, sacral pathologies, revision surgeries, and less than 2-year follow-up were excluded. Patients were stratified by surgical approach into MIS AP, open AP, and open posterior (P) cohorts.
Perioperative Characteristics
Preoperative patient demographics, comorbidity burden, body mass index (BMI), vertebral level, and diagnosis were compared. Patient comorbidity burden was assessed via a modified Charlson Comorbidity Index (CCI).11 These modifications included (1) a history of myocardial infarction was omitted, and (2) liver disease was given an adjusted weight of 2 points rather than 1 point for mild disease and 3 points for moderate to severe liver disease. Previous studies have demonstrated that slight modifications to the CCI have minimal impact on the overall score.11,12 Intraoperative characteristics such as procedural time, estimated blood loss (EBL), fluid administration, and transfusion rates were recorded. Postoperative hospitalization outcomes such as length of stay, narcotic consumption, and short-term complications were compared. Fusion and reoperation rates were recorded at latest follow-up.
Postoperative opioid consumption data were collected and narcotics were converted to oral morphine equivalents (OMEs) using a standardized calculation in order to account for differences in dosage, potency, and route of administration. The study on opioid equianalgesic calculations by Gordon et al13 was referenced to determine narcotic to oral morphine conversion ratios.
Surgical Technique
Open AP
A standard thoracotomy was used with the approach being performed by a board-certified thoracic surgeon using single lung ventilation via a double lumen endotracheal tube. An oblique incision was centered over the pathologic level with the overlying rib (if applicable) being disarticulated and morcellized for bone graft. If necessary, additional bone graft was harvested from the iliac crest. The parietal pleura (at the upper thoracolumbar interface) was opened and split near the costovertebral joint. The lung was retracted anteriorly. A bronchial blocker was used, and the lung was only deflated as needed during the exposure. Resection of the costovertebral joint and rib head allowed anterolateral visualization of the vertebral body. Chest tube placement was required upon closure of the thoracotomy. For retroperitoneal exposures, a direct lateral thoracoabdominal approach was used via formal cutting of the external and internal oblique musculature. The posterior approach consisted of a standard midline exposure with open placement of the pedicle screws and standard decortication of the posterior transverse processes.
Open Posterior
A standard midline approach was used with a complete laminectomy and facetectomy being performed. The thoracic level exiting nerve root was resected, and a standard extra-cavitary approach was done resecting the vertebral body and the superior and inferior disc space. An expanding articulating cage was then placed via the extra-cavitary defect with posterior pedicle screws being placed 2 levels above and below the corpectomy site. Iliac crest bone graft was used for the majority of cases.
MIS Anterior-Posterior (MIS AP)
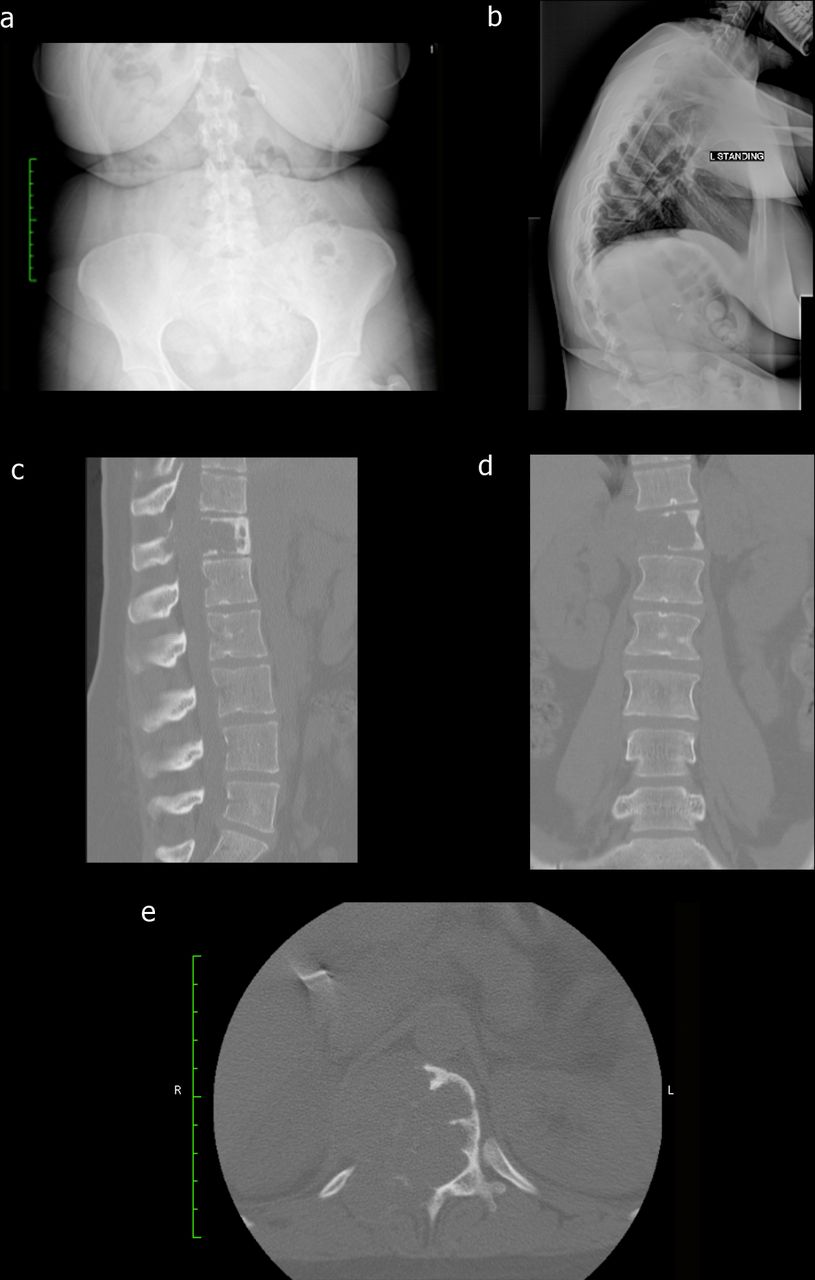
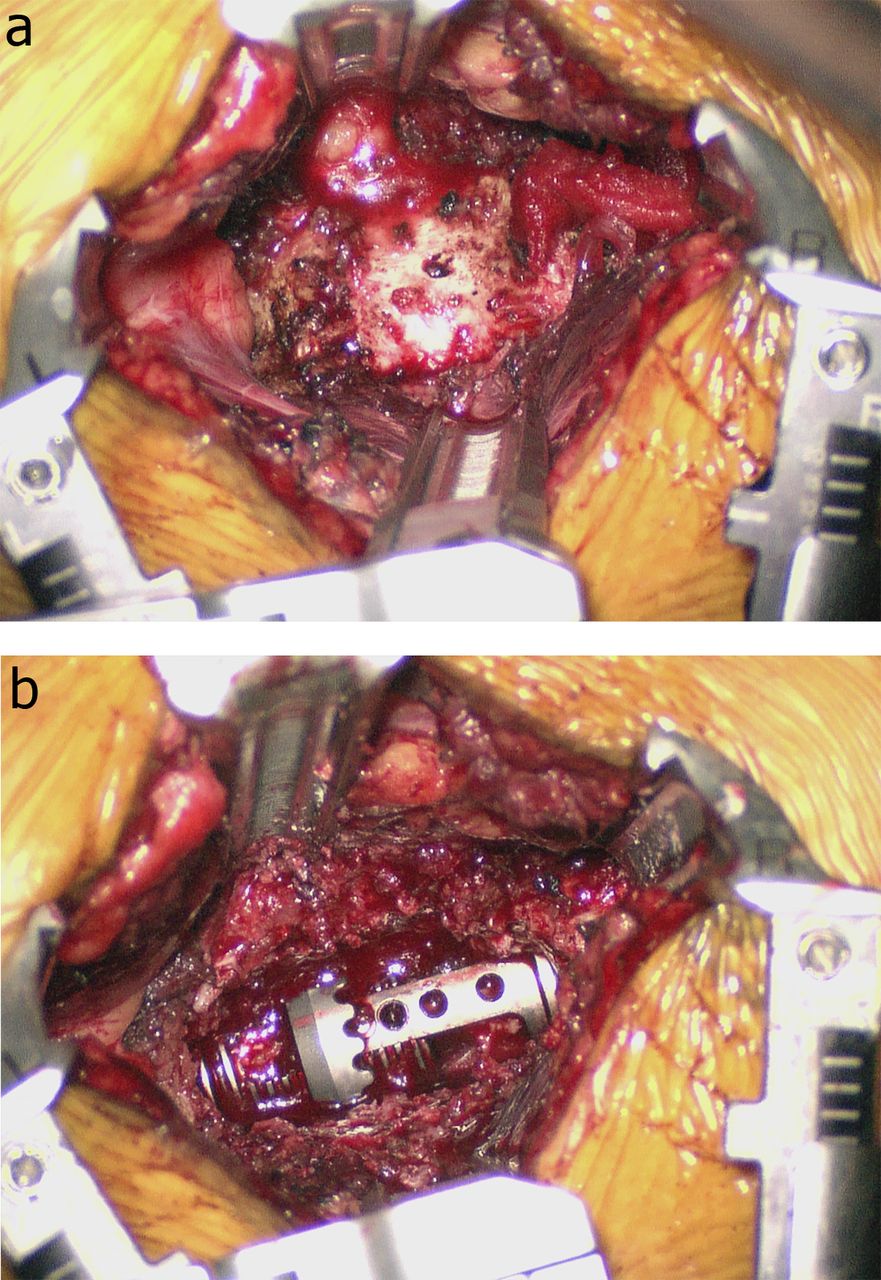
Appropriate preoperative imaging was analyzed (Figure 1a–1e). The patient was placed in the lateral decubitus position. Following appropriate intraoperative imaging, an oblique incision (2.5 cm in length) was made over the level of pathology. At the lower thoracic or upper lumbar level, the incision was made over the rib. After subperiosteal dissection, a segment of the rib was removed (2 cm) from the underlying pleura and neurovascular bundle and morcellized for bone graft. When necessary, bone graft was harvested from the facet joint. For retropleural access (T10-11), the parietal pleura was bluntly swept anteriorly. A bronchial blocker was used, and the lung was only deflated as needed during the exposure and subsequently reinflated once the tubular retractors were placed. For access to T12-L1, an extrapleural subdiaphragmatic approach was undertaken. Anterior exposure of L2-L5 was done through a retroperitoneal, trans-psoas approach. Fixed expandable retractors were placed after dilation (Figure 2a–2b). Real-time neuromonitoring was used throughout the case (lumbar) with specific stimulated monitoring during the approach, retractor adjustments, and instrumentation. Posterior instrumentation was placed percutaneously after repositioning the patient into the prone position on a Jackson table (Figure 3a–3b).

(a) Forty-two-year-old female presents with worsening back pain and thoracic discomfort for the past 3 months. Preoperative anterior-posterior (AP) radiograph demonstrating thoracic deformity secondary to giant cell tumor with complete osteolysis of the pedicle. (b) Preoperative lateral radiograph demonstrating kyphosis secondary to vertebral body destruction secondary to the giant cell tumor. (c) Preoperative sagittal computed tomography (CT) scan demonstrating T12 vertebral body osteolysis secondary to giant cell tumor infiltration. (d) Preoperative coronal CT scan demonstrating thoracic spinal deformity secondary to pathologic burst fracture of the T12 vertebral body. (e) Preoperative axial CT scan demonstrating burst fracture of T12 vertebral body secondary to giant cell tumor infiltration with extension into the spinal canal.
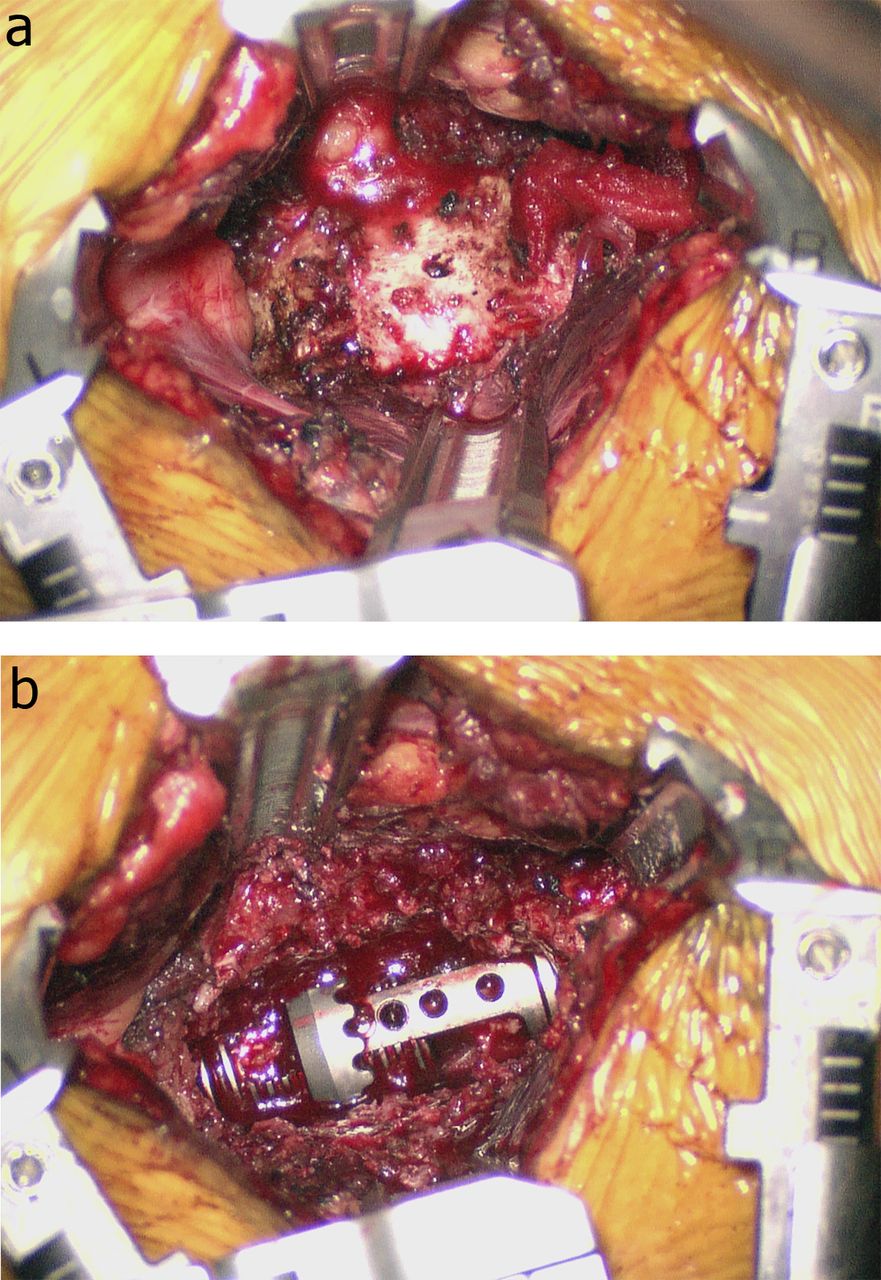
(a) Intraoperative image demonstrating retractors in place with adequate visualization of the T12 vertebral body via minimally invasive (MIS) retropleural subdiaphragmatic approach. (b) Intraoperative image demonstrating completed corpectomy with expandable titanium cage in place.

(a) Postoperative anterior-posterior (AP) radiograph demonstrating placement of the expandable titanium cage and instrumentation. (b) Postoperative lateral radiograph demonstrating placement of the expandable titanium cage and instrumentation and restoration of normal thoracic kyphosis. (c) Two-year postoperative sagittal computed tomography (CT) scan demonstrating arthrodesis and resolution of deformity without cage migration. (d) Two-year postoperative coronal CT scan demonstrating proper placement of expandable titanium cage with arthrodesis across the graft. (e) Two-year postoperative axial CT scan demonstrating expandable titanium cage with instrumentation and no recurrence of the giant cell tumor. (f) Two-year postoperative sagittal magnetic resonance imaging (MRI) demonstrating placement of expandable titanium cage and decompression of spinal cord without recurrence of the giant cell tumor. (g) Two-year postoperative axial MRI demonstrating placement of expandable titanium cage without recurrence of the giant cell tumor.
Statistical Methods
Statistical analysis was performed using an independent sample t test for continuous variables and Fisher exact test for categorical data. An α level of <.05 denoted statistical significance. Analyses were performed with SPSS version 20.0 (Prentice Hall, Chicago, Illinois).
RESULTS
Patient characteristics are described in Table 1. A total of 33 patients were included in the analysis. Of these, 5 (15.2%) open AP, 13 (39.4%) MIS AP, and 15 (45.5%) open P patients were identified. The level of corpectomy ranged from T4 to L5. The MIS AP cohort was younger than the open P group (45.1 vs 59.3, P < .05) and demonstrated a lower comorbidity burden compared with both open cohorts (CCI 4.15 vs 7.8 and 9.2, P < .05). Gender, BMI, and metastatic profile were similar between cohorts. In addition, the posterior open (P) cohort was more likely to undergo a corpectomy procedure for tumors when compared with the MIS AP patients. However, no differences were demonstrated in the rate of metastatic disease between the P, MIS AP, and open AP cohorts.
Patient characteristics.
The MIS AP cohort had a decreased operative time (3.9 vs 6.1 vs 6.0 hours, P < .05), length of hospitalization (5.5 vs 9 vs 11 days, P < .05), and reduced blood loss (400 vs 2,260 vs 2,275 cc, P < .05) compared with the open AP and open P cohorts, respectively (Table 2). No differences were demonstrated in the rates of intraoperative complications, in-hospital complications, or surgical site infections between all cohorts. However, the narcotic use (OME 540 ± 259 vs 1,095 ± 745, P < .05) and the reoperation rate was significantly lower in the MIS AP patients when compared with the open AP cohort. All patients demonstrated radiographic evidence of arthrodesis at the 1-year follow-up based upon computed tomographic imaging (Figure 3c–3g).
Perioperative and postoperative characteristics.
The MIS AP patients demonstrated lower transfusion rates than the open P cohort (15.4% vs 80.0%, P < .05) and the open AP patients (15.4% vs 80.0%, P < .05; Table 3). In those patients who received intraoperative transfusions, the MIS AP patients received significantly less units of packed red blood cells (0.5 ± 1.1 vs 2.6 ± 2.8 units, P < .05) and fresh frozen plasma (0 vs 0.6 ± 0.8, P < .05). However, no differences were demonstrated in the amount of postoperative packed red blood cells transfused between the cohorts.
Transfusion and intraoperative intravenous fluid administration characteristics.
DISCUSSION
The current study attempted to compare outcomes between traditional means of thoracolumbar corpectomy and less invasive techniques. Despite the small and heterogeneous population, it appears MIS AP corpectomies can be as safe and effective in providing adequate decompression and stabilization for a variety of pathologies without the morbidity associated with traditional open techniques. The results demonstrated in the current study have been consistent with other studies regarding MIS corpectomies.14–16 Uribe et al16 analyzed outcomes following a mini-open lateral approach for the management of thoracic spine tumors. Their rates of postoperative complications for MIS, traditional AP, and traditional P approaches were 4.8%, 6.9%, and 11.1%, respectively.16 Additionally, the authors found that the less invasive approach offered similar access compared with the open anterior approach without the need for single-lung ventilation or extensive rib resection.16 Kossman et al14 analyzed the effectiveness of a novel retractor system in 65 patients undergoing MIS corpectomies. The authors demonstrated that the retractor system allowed for improved surgical access when compared with traditional open approaches with no reported cases of postoperative paraplegia, vessel laceration, or infections.14
In the current study, the MIS AP patients demonstrated decreased operative time, blood loss, and transfusion rates as compared with both open P and AP cohorts. These benefits have been part of the hallmark benefits of MIS techniques. Similarly, Lu et al5 demonstrated decreased blood loss and length of hospitalization with similar operative times and complication rates between patients who underwent mini-open and traditional posterior corpectomies. Despite the similar pathologies involved, differences in patient demographics and surgeon experience may confound these findings. Specifically, the open AP and P techniques were performed earlier in the senior surgeon's career, whereas MIS corpectomies were performed later with increasing experience with the MIS technique. As such, the learning curve may have beneficially influenced his results in subsequent MIS cases.
MIS AP patients demonstrated a lower reoperation rate than the open AP cohort. The latter cohort required 2 reoperations for spinal fluid collection and impingement from a malpositioned pedicle screw. However, the low sample size in the cohorts should warrant caution in deriving clinical significance from these findings. Other studies have reported a low overall reoperation rate using a variety of techniques. Snell et al17 analyzed outcomes of 15 patients following a posterior-based thoracolumbar corpectomy over a mean length of 10.6 months. Revision surgery was required in 1 (7%) patient due to hardware failure.17 Lee et al18 reported 4 reoperations due to anterior cage migrations following 19 L5 corpectomies via the open retroperitoneal approach.
In our analysis, MIS AP corpectomy patients consumed less narcotics compared with the open AP cohort. These findings are consistent with the growing body of evidence demonstrating decreased postoperative morbidity and subsequently less narcotic requirements in patients undergoing MIS spine surgery.21–23 Proper postoperative pain management has been associated with expeditious recovery and prevention of chronic pain.19,20 Schwender et al23 assessed narcotic use in 49 patients who underwent an MIS transforaminal lumbar interbody fusion (TLIF). The authors demonstrated that these patients achieved narcotic independence by 2 to 4 weeks following surgery.23 In addition, Adogwa et al21 demonstrated that MIS TLIF patients ceased narcotic use 2 weeks earlier than the open TLIF cohort. The present study is the largest of its kind to compare narcotic consumption between patients undergoing corpectomies via the 3 techniques.
Arthrodesis rates between the cohorts were similar. Each patient underwent a computed tomography scan as part of the senior surgeon's postoperative protocol. All patients demonstrated complete bridging of bone as confirmed by computed tomography scan at 1 year. Snell et al17 demonstrated no pseudarthrosis at a mean of 10.6 months following open posterior-based thoracolumbar corpectomy in 15 patients. In contrast, Hofstetter et al24 demonstrated an arthrodesis rate of only 68% in 67 patients with either traumatic or osteomyelitic fractures. Again, the small cohort restricts any conclusions that could be made regarding fusion rates between techniques.
The MIS AP approach does have drawbacks. The technique is associated with a significant learning curve. The difficulty is compounded by a long working distance and narrow surgical working space through a tubular retractor.16 Additionally, the technique requires extensive familiarity with the anatomy as standard anatomical landmarks may not be visible for reference.16 Finally, the MIS AP corpectomy relies heavily on intraoperative fluoroscopic imaging, which may increase the radiation exposure to the patient and surgical team.
There were several limitations to this study. First, the sample size of each cohort was relatively small and the study was nonrandomized. This would imply selection bias. However, there were no differences in the diagnoses or levels undergoing corpectomy between cohorts. In addition, the study was underpowered to address certain clinical outcomes such as complication rates or health-related quality of life. However, the present study remains one of the larger comparisons of MIS and traditional corpectomies. Second, these procedures were performed by a single spine surgeon. As such, these findings may not be generalizable to all spine procedures in all regions of the United States. Third, the differences in perioperative outcomes may be associated with the younger age and lower comorbidity burden in the MIS AP cohort. Finally, patients underwent a corpectomy for mainly metastatic disease, trauma, and infection. Unquestionably, larger studies are warranted; however, these pathologies are heterogeneous in nature and far from ubiquitous.
The findings of the present study suggest that MIS AP thoracolumbar corpectomies are a viable alternative to traditional approaches. Benefits include decreased procedural times, hospitalization, narcotic use, and blood loss without increasing complications or compromising fusion rates. Further studies should focus on detailed and long-term health-related quality of life outcomes for patients undergoing MIS techniques for traditionally morbid pathologies.
Footnotes
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.