


Abstract
Background Nowadays, minimally invasive lateral lumbar interbody fusion (LLIF) is used to treat degenerative lumbar spine disease. Many studies have proven that LLIF results in less soft tissue destruction and rapid recovery compared with open posterior lumbar interbody fusion (PLIF). Our recent cost-utility study demonstrated that LLIF was not cost-effective according to the Thai willingness-to-pay threshold, primarily due to the utilization of an expensive bone substitute: bone morphogenetic protein 2. Therefore, this study was designed to use less expensive tricalcium phosphate combined with iliac bone graft (TCP + IBG) as a bone substitute and compare cost-utility analysis and clinical outcomes of PLIF in Thailand.
Methods All clinical and radiographic outcomes of patients who underwent single-level LLIF using TCP + IBG and PLIF were retrospectively collected. Preoperative and 2-year follow-up quality of life from EuroQol−5 Dimensions−5 Levels and health care cost were reviewed. A cost-utility analysis was conducted using a Markov model with a lifetime horizon and a societal perspective.
Results All enrolled patients were categorized into an LLIF group (n = 30) and a PLIF group (n = 50). All radiographic results (lumbar lordosis, foraminal height, and disc height) were improved at 2 years of follow-up in both groups (P < 0.001); however, the LLIF group had a dramatic significant improvement in all radiographic parameters compared with the PLIF group (P < 0.05). The fusion rate for LLIF (83.3%) and PLIF (84%) was similar and had no statistical significance. All health-related quality of life (Oswestry Disability Index, utility, and EuroQol Visual Analog Scale) significantly improved compared with preoperative scores (P < 0.001), but there were no significant differences between the LLIF and PLIF groups (P > 0.05). The total lifetime cost of LLIF was less than that of PLIF (15,355 vs 16,500 USD). Compared with PLIF, LLIF was cost-effective according to the Thai willingness-to-pay threshold, with a net monetary benefit of 539.76 USD.
Conclusion LLIF with TCP + IBG demonstrated excellent radiographic and comparable clinical health-related outcomes compared with PLIF. In economic evaluation, the total lifetime cost was lower in LLIF with TCP + IBG than in PLIF. Furthermore, LLIF with TCP + IBG was cost-effective compared with PLIF according to the context of Thailand.
Clinical Relevance LLIF with less expensive TCP + IBG as bone graft results in better clinical and radiographic outcomes, less lifetime cost, and cost-effectiveness compared with PLIF. This suggests that LLIF with TCP + IBG could be utilized in lower- and middle-income countries for treating patients with degenerative disc disease.
Level of Evidence 3.
- cost-utility analysis
- lateral lumbar interbody fusion (LLIF)
- posterior lumbar interbody fusion (PLIF)
- quality-adjusted life-year (QALY)
- tricalcium phosphate (TCP)
Introduction
Low back pain is considered the most common and most expensive cause of work-related disability in people older than 45 years.1 After treatment with instrumented fusion, long-term studies showed positive outcomes over conservative care.2 Lumbar spinal fusion became a common surgical procedure used to treat a variety of degenerative pathologies, including spondylolisthesis, degenerative disc disease, and lumbar spinal stenosis. With the aging of society in Thailand, the number of lumbar spinal fusions has increased, where total expenditures are growing relative to the economy. Improving the cost-effectiveness of surgical interventions will be a major focus for spine surgeons.
Minimally invasive extreme lateral lumbar interbody fusion (LLIF) for lumbar spondylosis enabled the surgical treatment of back pain and leg pain while minimizing tissue injury, accelerating overall recovery, and more cost-effectiveness. These findings were supported by the study by Delozio et al,3 who reported that the average length of stay of the LLIF group was 49% less than that of the open posterior lumbar interbody fusion (PLIF) group, and the average cost of surgical procedure and initial hospital stay in the LLIF group was 6% less than that of the open PLIF group with an average cost savings of 9.6% or 2563 USD/patient. Another study by Lucio et al4 compared LLIF and open PLIF in patients who undergo double-level lumbar interbody fusion and found a shorter average hospital stay in the LLIF group (1.2 vs 3.2 days), more frequent complications in the open PLIF group (14% vs 6%), and an average cost savings for LLIF over open PLIF of 2825.37 USD/patient.
Although this LLIF technique has been demonstrated to shorten the recovery time and cost-effectiveness in developed countries, it was also typically associated with higher instrument costs, especially in developing countries. Our previous study for cost-utility analysis in Thailand, at 1-year follow-up, found that LLIF was not cost-effective compared with open PLIF, in contrast to a previous study in a developed country.5 These may be explained by the higher cost of instrumentation and recombinant human bone morphogenetic protein-2 (rhBMP-2) used as a bone substitution in LLIF surgery. However, recently, our group demonstrated that less costly tricalcium phosphate combined with iliac bone graft (TCP + IBG) had comparable effectiveness in clinical outcomes compared with rhBMP-2 in LLIF surgery.6 To our knowledge, there were no studies on the cost-effectiveness of LLIF using TCP + IBG compared with open PLIF using local bone graft (LBG). Therefore, the aim of this study was to investigate the cost-effectiveness of LLIF using TCP + IBG as bone substitution compared with open PLIF using LBG in single-level spinal fusion surgery.
Materials and Methods
This retrospective cohort study was carried out by collecting data from electronic medical records and the Siriraj Spine Registry Database of Siriraj Hospital, Mahidol University, Bangkok, Thailand. This study was reviewed and approved by the Siriraj Institutional Review Board (COA no Si 679/2023). The requirement to obtain written informed consent was waived due to the retrospective and anonymous nature of the study.
Study Population
Patients who underwent lumbar spinal fusion surgery with the LLIF or open PLIF technique using 1 polyetheretherketone (PEEK) cage at a single level between 2014 and 2020 were identified. All LLIF procedures were performed by a senior surgeon (M.R. or W.S.), while PLIF procedures were performed by 1 of 3 senior surgeons (E.K., M.R., or W.S.). Pedicle screw fixation for posterior supplementation was used for LLIF and PLIF patients. Patients were enrolled if they were aged 18 years or older, diagnosed with lumbar spondylosis with back and leg pain, underwent single-level lumbar fusion surgery with the open PLIF or LLIF technique, and were followed for at least 2 years. Operative notes, anesthesia records, discharge summaries, clinical progression notes, radiographic outcomes, and cost details were collected and assessed. Patients were excluded if they had incomplete medical or surgical details or could not respond to questions effectively. Patients who had severe postoperative medical complications (eg, pneumonia, coronary artery disease, or stroke) were also excluded due to our economic model based on surgical-related complications.
The sample size calculation was based on data from the utility score reported by Gandhoke et al7 in single-level transforaminal lumbar interbody fusion (TLIF) and Boonsirikamchai et al6 of LLIF using TCP + IBG. The mean utilities of 45 patients who underwent single-level TLIF and 25 patients who underwent LLIF, measured by the EuroQoL Group 5-dimension questionnaire (EQ-5D), were 0.78 ± 0.20 and 0.86 ± 0.13, respectively. An online statistical sample size calculator program “Statulator” was used to compare 2 independent means with a power of 80% and a level of significance of 5% with equality.8 The study required a sample size of at least 25 for each group.
Surgical Techniques
Lateral Lumbar Interbody Fusion
The patient was placed in the lateral decubitus position and prepped and draped in a sterile technique. The standard LLIF procedure, previously described, was performed using the mini-open lateral approach. Then, discectomy with endplate preparation was performed after insertion of interbody cage (CoRoent XL; NuVasive, Inc, San Diego, CA, USA) filled with 2 to 4 cc of β-Tricalcium phosphate (AttraX; NuVasive, Inc., USA) combined with 1 to 2 cc of cancellous IBG that was harvested using the mini-open technique during the lateral decubitus position. After closing the wound in the lateral decubitus position, the patient was subsequently induced into the prone position for posterior instrumentation by percutaneous fixation of the pedicle screw.
Posterior Lumbar Interbody Fusion
The patient was operated in the prone position. After being prepped and draped in a routine sterile manner, a skin incision was made over the operating level. Pedicle screw insertion and laminectomy were done. Then, discectomy with endplate preparation for interbody fusion was performed using an interbody cage (CoRoent PEEK, NuVasive, Inc, San Diego, CA, USA, and CAPSTONE PEEK, Metronic Inc., Memphis, TN, USA) filled with LBG. After the vacuum drain was applied, the surgical wound was closed.
Study Procedure
The patients were divided into 2 groups: a “LLIF group” and a “PLIF group.” Data relating to the preoperative, perioperative, and 2-year postoperative periods were reviewed. The estimated blood loss, operative time, and length of hospital stay were used to evaluate perioperative outcomes. The quality of life of the patients and functional outcomes were evaluated using the EuroQol 5 Dimensions 5 Levels (EQ-5D-5L) questionnaire, the EuroQol Visual Analog Scale (EQ-VAS), and the Oswestry Disability Index (ODI) scores. EQ-5D-5L responses were converted to utility scores using previously published coefficient factors specific to the Thai population.9
Radiographic Measurements
Plain radiography and computed tomography (CT) of the lumbar spine were collected after a 2-year follow-up for evaluation by 2 spine surgeons (P.T. and W.S.) at our center. All radiographic evaluations were measured using an image viewer computer system (Sectra IDS7 version 15.1.28.6; Sectra AB, Linkoping, Sweden). The angle of lumbar lordosis was determined by the angle formed by the superior endplate line of the L1 vertebra and the superior endplate line of the S1 vertebra. The height of the intervertebral disc was measured as the distance between the inferior endplate and the superior endplate at the middle line of the vertebral body. The foraminal height was measured as the distance between the inferior pedicle wall above the index disc space and the superior pedicle wall from below. Successful bony fusion was defined as the presence of interbody bone bridging trabecular bone in the coronal and sagittal views of CT.10 The subsidence of the PEEK was determined by CT and was defined as adjacent endplates breaches >2 mm.11
Statistical Analysis
The demographic and clinical characteristics of the patients were analyzed and descriptively reported. Categorical data were compared using the χ 2 test and Fisher’s exact test, as appropriate. The distribution of continuous numeric data was verified using the Shapiro-Wilk test. Continuous data normally distributed between the 2 groups were compared using an independent t test. Preoperative and postoperative data within each group were compared using a dependent t test. The results are presented as mean ± SD and frequency (percentage). For data that were not normally distributed, nonparametric tests such as Mann-Whitney U tests or Wilcoxon signed-rank test were used for calculation. Median (interquartile range; IQR) was used for representing nonparametric outcome parameters. A 2-tailed probability (P) value of less than 0.05 was considered statistically significant. The various data analyses were carried out using SPSS Statistics for Windows, version 19.0 (IBM Corp, Armonk, NY, USA). Cost-utility analysis was performed using Microsoft Excel 2019 (Microsoft Corporation, Redmond, WA, USA).
Economic Evaluation
The cost-utility analysis compared the lifetime costs and health outcomes of the LLIF and PLIF groups. A decision tree and Markov model were adopted to simulate the natural history of the degenerative spinal disease in virtual patients. We analyzed the results of cost-utility using a societal perspective following the Thai Health Technology Assessment guidelines.12 The results are presented as incremental cost and quality-adjusted life-year (QALY) gained in 2022 USD. The interpretation of the cost utility of the 2 fusion techniques was based on a willingness-to-pay (WTP) threshold of 4706 USD/QALY gained. It was derived from the Thai WTP threshold reported by the Thai Health Economic Working Group (160,000 Thai baht/QALY gained), using the average exchange rate of 2022 of 1 USD = 34.90 Thai baht.13 An annual discount rate of 3% was used for future costs and health outcomes.
Economic Model
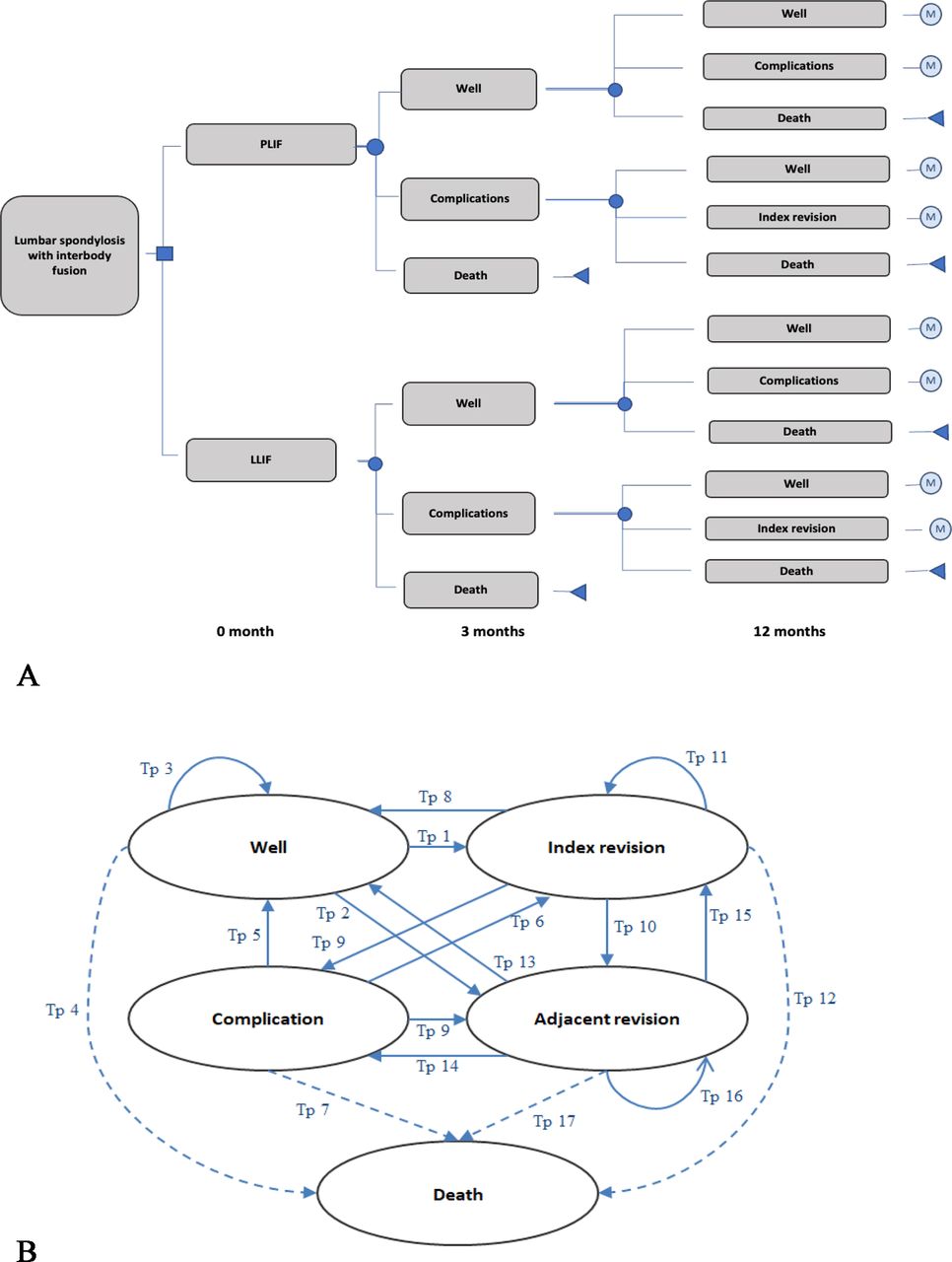
The development of our economic model commenced with the construction of a decision tree that divided patients into the LLIF and PLIF groups. The decision tree then subclassified the patients according to their short-term surgery outcomes (with and without complications). An index revision was allowed to be performed when necessary for some complications. The tree is illustrated in Figure 1a. Subsequently, patients were entered into a 5-health state Markov model to capture the lifetime costs and health outcomes of the interventions. The 5 health states were “well,” “complications,” “index revision,” “adjacent revision,” and “death” (Figure 1b). The flow of virtual patients is depicted with an arrow, with individual patients either maintaining the same health state or transitioning to another state, per the natural course of the disease.

Decision tree and Markov model. (A) A decision tree was constructed to divide patients into 4 groups: “well,” “complications,” “index revision,” and “death” based on the health status outcomes of each surgical treatment.. The filled circles indicate choice node, the squares indicate decision node, the triangles indicate endpoint node, the circled "M" indicates Markov model. (B) In the Markov model, patients could remain in the same disease state or move to another health state. Tp = transitional probability.
Input Parameters
Transitional probabilities were calculated based on data related to disease progression and surgical techniques (LLIF and PLIF) reported by Nemani et al,14 Nayar et al,15 Kobayashi et al,16 and Sears et al.17 Because there was limited evidence on clinical outcomes after revision, we had to calculate related transitional probabilities based on expert opinion. In addition, we assumed that there was no complication after the index revision and adjacent revision. The mortality rate of the virtual patients was based on the age-specific mortality rate from the World Health Organization Life Table.18 The utilities were calculated from primary data and the previous local study.5 Because our study adopted a societal perspective, the overall costs included direct medical costs (eg, room, medication, nursing service, imaging, surgical procedure, anesthesia, implants, and physical therapy) and nondirect medical costs (such as travel and meal expenses). We assumed that a loss or impaired ability to work or participate in leisure activities due to disease morbidity and treatment would be captured as disutility in the QALY analysis.19 Consequently, indirect costs were not included in the analysis. Direct treatment costs, outpatient and hospital visit rates, and utility data were obtained from the retrospective review of the data from the electronic database and the data registry. Direct nonmedical costs were obtained from a previous local study.20 All costs were converted to 2022 USD using the consumer price index.13,21 In the Siriraj Spine Registry Database, patient quality of life was prospectively collected at the preoperative and 2 years postoperative time points. The details of the input parameters used in the economic model are listed in Table 1.
Input parameters used in the health economic model.
Cost-Utility Analysis
The base case analysis compared the health-related outcomes and costs of LLIF vs PLIF. The results of the cost-utility analysis were presented as an incremental cost-effectiveness ratio and a net monetary benefit (NMB) that was calculated using the following equation:
NMB = (WTP threshold × total QALY gained) – incremental cost
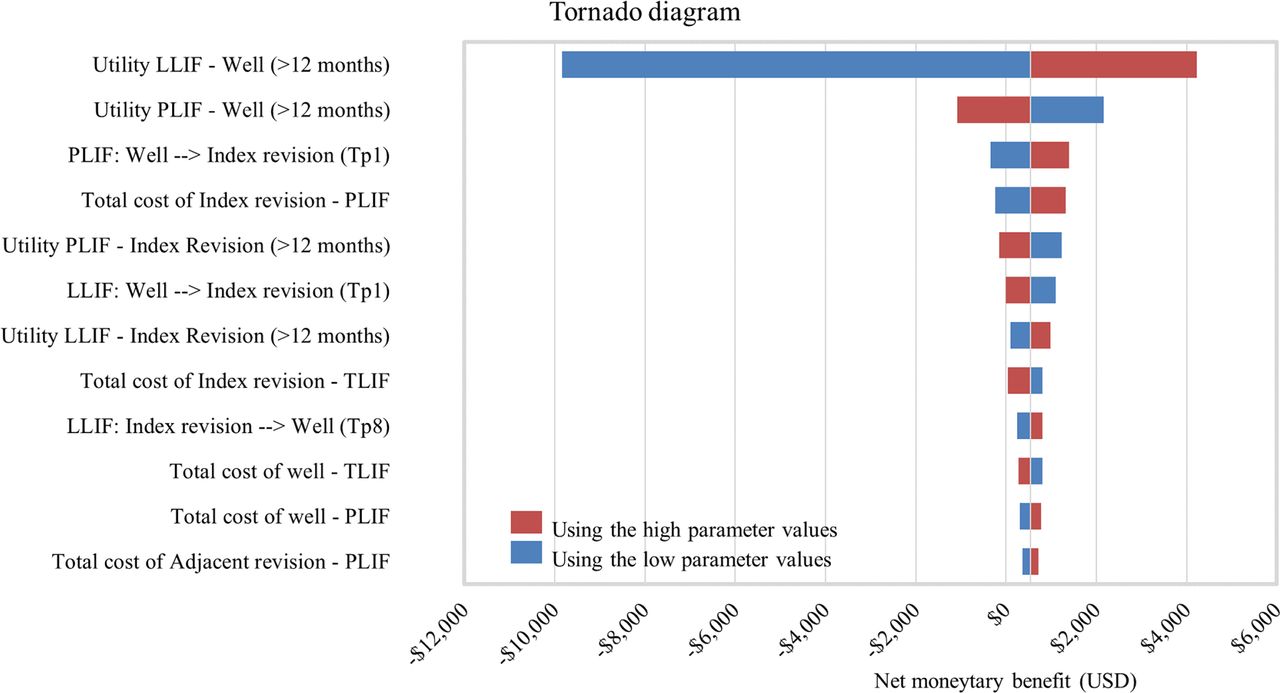
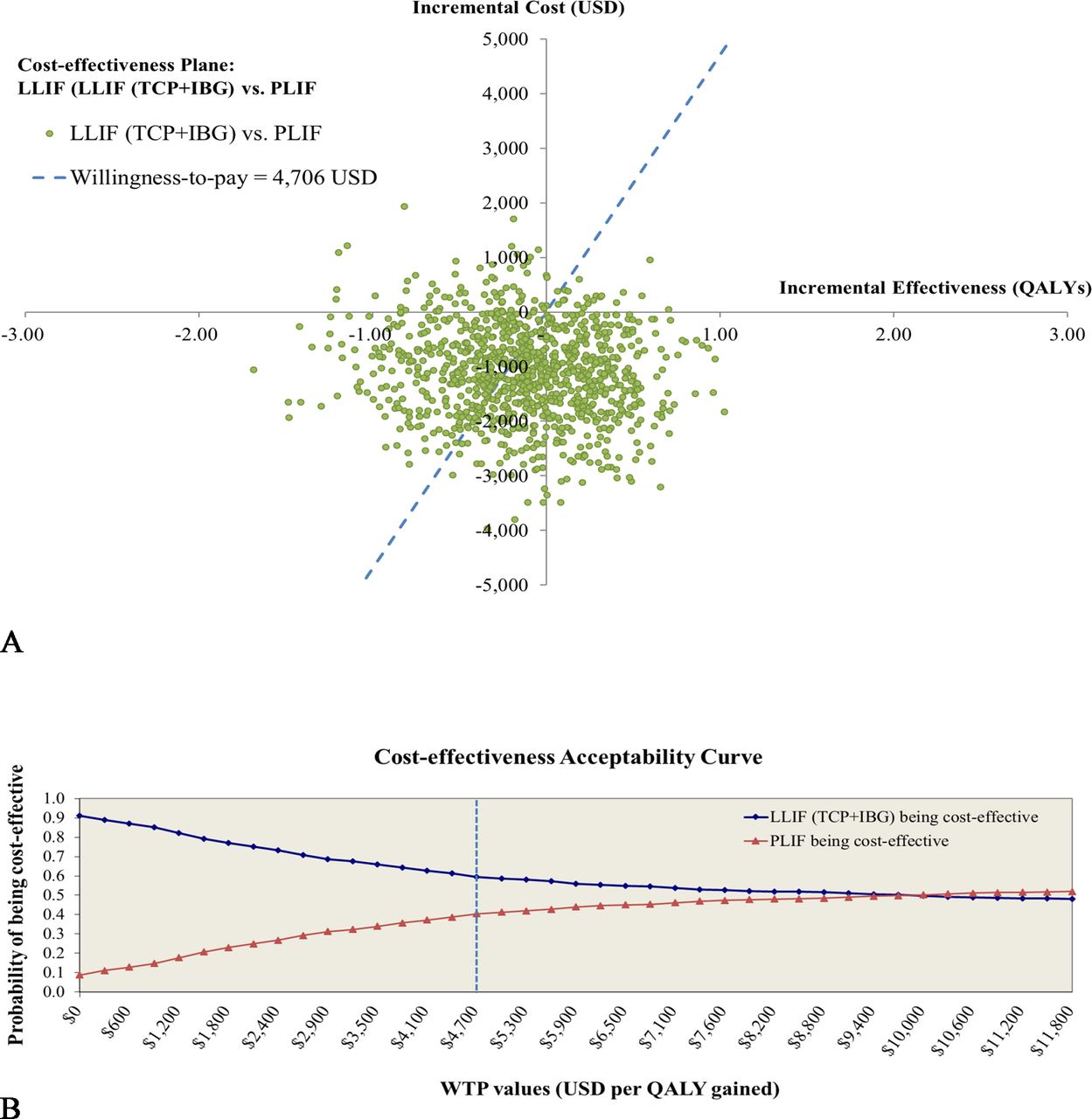
A 1-way sensitivity analysis was performed to find influence effects by altering the values of the input parameters within the 95% confidence interval ranges or ±10 % of the base-case values if a 95% confidence interval was not available. The results of the 1-way sensitivity analysis are presented as a tornado diagram (Figure 2). A probabilistic sensitivity analysis (PSA) was performed to examine the simultaneous effects of all parameter uncertainties. Transitional probabilities and utilities were assigned a beta distribution, while costs were assigned a gamma distribution.22 One thousand Monte Carlo simulations were run to obtain values for total lifetime costs, outcomes, and incremental cost-effectiveness ratios (ICERs). The PSA results are represented as a cost-effectiveness plane (Figure 3a) and a cost-effectiveness acceptability curve (Figure 3b).

Tornado diagram illustrates the results of a 1-way sensitivity analysis. Abbreviations: LLIF, lateral lumbar interbody fusion; PLIF, posterior lumbar interbody fusion; Tp1, transitional probability from well to index revision; Tp8, transitional probability from index revision to well.

Multivariate probabilistic sensitivity analysis. The results are based on 1000 Monte Carlo simulations and are shown as a cost-effectiveness plane (A) and a cost-effectiveness acceptability curve (B). Abbreviations: IBG, iliac bone graft; LLIF, lateral lumbar interbody fusion; PLIF, posterior lumbar interbody fusion; QALY, quality-adjusted life year; TCP, tricalcium phosphate; WTP, willingness to pay.
Results
In total, 80 consecutive patients were identified as having undergone a single-level lumbar spinal fusion with LLIF or PLIF in our department between 2014 and 2020 and were followed for 2 years. Of those, 30 patients underwent LLIF with combined TCP with IBG and 50 patients underwent PLIF with LBG. Demographic data for both groups are provided in Table 2. There were no statistically significant differences in gender (P = 0.633), age (P = 0.598), body mass index (P = 0.894), or underlying disease (P = 0.319). Most of the patients in both groups were women (70% in LLIF and 64% in PLIF), and hypertension was the common underlying disease. There were statistically significant differences in diagnosis and level of operated spine. Spinal stenosis was the most common diagnosis for the LLIF group (53%), while spondylolisthesis was the most common primary diagnosis for the PLIF group (64%). L4 to L5 was the most common spinal surgical level in both groups (LLIF: 77% and PLIF: 64%). Additionally, the L5-S1 spinal level was operated on only in the PLIF group.
Demographic data.
Perioperative Clinical Parameters
The LLIF group has a less median estimated blood loss compared with the PLIF group (200 [100, 250] mL of LLIF vs 350 [200, 500] mL of PLIF, P < 0.001). However, LLIF also had a longer operative time compared with the PLIF group (215 [170, 291] in LLIF vs 180 [150, 211] in PLIF, P = 0.007). There were no statistically significant differences in median hospital stay (LLIF: 6 [5, 9] days vs PLIF: 7 [6, 8] days, P = 0.437).
There were no serious complications with significant differences in both groups of patients during the operation and follow-up (P = 0.794). Common complications in the LLIF group were anemia and electrolyte imbalance, while dural tear was the common complication in the PLIF group, as shown in Table 3. For proximal limb neuropathy, only in the LLIF group (27%) was there total recovery after 3 months of follow-up. In our cohort, there was no serious complication that required index revision. The fusion rate did not show significant differences between these 2 groups at 2 years of postoperative follow-up (P = 0.937). The LLIF group demonstrated fusion in 25/30 (88.3%), and the PLIF group resulted in fusion in 42/50 (84%). However, there was a higher subsidence rate of PEEK in the LLIF group compared with the PLIF group with statistical significance (LLIF: 46.6% vs PLIF: 20%, P = 0.022).
Perioperative data, postoperative complications, fusion rate, and PEEK subsidence rate.
Radiographic Parameters
At the preoperative time, there were no statistically significant differences in any of the radiographic parameters (lumbar lordosis, foraminal height, or disc height) between the LLIF group and the PLIF group (P > 0.05). Two years after the operation, all parameters were improved with statistical significance (P < 0.001 and P = 0.015) in both groups of LLIF and PLIF. At 2-year follow-up, the LLIF group surprisingly had more improvement in all parameters (lumbar lordosis: P = 0.049, foraminal height: P < 0.001, and disc height: P = 0.001) compared with the PLIF group. The LLIF group had 42.97° ± 13.42° of lumbar lordosis, 19.30 ± 3.32 mm of foraminal height, and 11.33 ± 2.93 mm of disc height, while the PLIF group had 37.08° ± 12.38° of lumbar lordosis, 13.30 ± 2.56 mm of foraminal height, and 9.53 ± 1.83 mm of disc height. All preoperative and postoperative data for both groups are shown in Table 4.
Radiographic data of LLIF and PLIF preoperatively and at the 2-year follow-up.
Health-Related Quality of Life Results
The results of health-related quality of life at preoperative and 2 years postoperative follow-up timepoints are shown in Table 5. At the preoperative time, there was no statistically significant difference in utility, ODI, or EQ-VAS between the LLIF group and the PLIF group. All clinical quality of life related to health (utility, ODI, and EQ-VAS) significantly improved in both groups compared between preoperative and 2-year follow-up (P < 0.001 and P = 0.004). However, there were no differences at 2-y postoperative follow-up in utility (P = 0.501), ODI (P = 0.584), or EQ-VAS (P = 0.698) between the LLIF group and the PLIF group.
Utility, ODI, and EQ-VAS of LLIF and PLIF preoperatively and at the 2-year follow-up.
Cost-Utility Analysis Results
Base-Case Analysis
Life expectancy was estimated at 24.6 years. The total lifetime costs per patient for LLIF vs PLIF were 15,355 USD vs 16,500 USD, respectively. Total QALYs were 14.48 in the LLIF group and 14.61 in the PLIF group, respectively. The LLIF group had less total lifetime cost and total lifetime QALY than the PLIF group, and the differences were 1145 USD and 0.13 QALYs, respectively. The NMB for LLIF was 539.76 USD compared with PLIF. The interpretation of these results according to the Thai WTP threshold was that LLIF with TCP + IBG was cost-effective compared with PLIF with LBG. The results of the base case analysis are shown in Table 6.
Results of the base case analysis.
One-Way Sensitivity Analysis
The 3 most influential variables in our model were the utility of LLIF of the “well” health state >12 months after surgery, the utility of PLIF of the “well” health state >12 months after surgery, and the transition probability from the “well” to the “index revision” health state of PLIF (Figure 2).
Probabilistic Sensitivity Analysis
Based on the 1000 Monte Carlo simulations, the PSA results are presented in a cost-effectiveness plane (Figure 3a). The plots scatter both above and below the WTP threshold line, suggesting that the result of LLIF being cost-effective is likely to be uncertain and not robust. At the WTP threshold of 4706 USD per QALY gained, the probability of LLIF being cost-effective was 59.6%. PSA results are also illustrated as acceptability curves for cost-effectiveness (Figure 3b). The probability of LLIF being less cost-effective than PLIF switched at a WTP of 10,000 USD per QALY gained and above.
Discussion
Clinical Outcomes
Our study did not show differences in health-related quality of life results (utility, ODI, and EQ-VAS) at the 2-year postoperative follow-up between the LLIF group and the PLIF group. Both groups demonstrated a significant improvement in clinical health-related outcomes between the preoperative and postoperative phases. Furthermore, the differences between these 2 groups for fusion rate, length of stay, and serious complications were nonsignificant. However, differences in outcomes were observed between these groups in intraoperative blood loss, operative time, PEEK subsidence rate, proximal limb neuropathy, and radiographic data.
LLIF has gained popularity in spinal surgery due to the advantages of minimally invasive surgical techniques and biomechanics, which provide the most extensive endplate preparation and disc removal.23 Our results showed less intraoperative blood loss in the LLIF group compared with the PLIF group, similar to the standard benefits of minimally invasive surgery.24 Regarding the perioperative time, our group observed a more prolonged operative time in the LLIF group compared with PLIF. This differs from the report of Gandhoke et al,7 but intraoperative time can be challenging and time-consuming due to the 2-stage operative technique of LLIF, which involves fusion of the interbody in the lateral position first and insertion of the pedicular screw and rod system in the prone position sequentially.25
From our study, 2 postoperative parameters in the LLIF group had disadvantage outcomes compared with the PLIF group. First, we found proximal limb neuropathy only in the LLIF group (27%), although this symptom completely recovered after a 3-month follow-up, and there were no serious complications. This complication was found only in the LLIF group due to dissection of the psoas muscle. However, most proximal limb neuropathic cases resolve in 6 months, with 90% resolved within 1 year.26 Second, we found an incidence rate of PEEK subsidence higher than in the TLIF group (46.6% vs 20%). We hypothesized that the difference in the size of the interbody device and the endplate preparation technique can cause a different rate of PEEK subsidence. Satake et al27 reported that osteoporosis and a higher cage height affected endplate injury, causing PEEK subsidence in LLIF.
In the present study, there was a significant improvement in postoperative radiographic data, including lumbar lordosis, foraminal height, and disc height in the LLIF and PLIF groups. Furthermore, the LLIF group showed superior radiographic data compared with the PLIF group at the 2-year postoperative follow-up (P < 0.05). The LLIF technique was recognized to provide better anterior column support outcomes with larger interbody cages and a greater surface contact area of bone graft to vertebral endplates.27 Our study was consistent with the study by Marchi et al28 that LLIF significantly improved restoration of disc height, segmental lordosis, and total lumbar lordosis compared with PLIF. However, in our study, there was no correlation between the improvement in the lumbar lordosis profile and the quality of life related to health in a single level of spinal interbody fusion. However, we hypothesized that multiple levels of LLIF can improve sagittal alignment, affecting clinical outcomes in patients with degenerative spondylosis.
This study reported similar 2-year postoperative follow-up of all health-related clinical outcomes between these 2 groups. These findings were in contrast to our previous study at 1-year follow-up. At 2 years of follow-up, there were no significant differences in utility between the LLIF group and the PLIF group (0.86 ± 0.13 in the LLIF group vs 0.88 ± 0.09 in the PLIF group, P = 0.501), while at 1 year of follow-up, the PLIF group had significantly better utility than LLIF (0.89 ± 0.09 in the PLIF group vs 0.84 ± 0.15 in the LLIF group, P = 0.023). These findings may be explained by the greater effectiveness of indirect decompression, as described by Mahatthanatrakul et al.29 LLIF could also provide indirect decompression due to decreased thickness and remodeling of the ligamentum flavum after 20.2 ± 11.9 months of follow-up, resulting in improved cross-sectional area of the spinal canal.
Cost-Utility Analysis
Our economic analysis revealed that LLIF with the TCP + IBG group had less total lifetime costs of about 15,355 USD with total QALYs equal to 14.48, while the PLIF group had total lifetime costs of approximately 16,500 USD with total QALYs equal to 14.61. The LLIF group had a net monetary benefit of approximately 539.76 USD. These findings were interpreted as LLIF having a cost-effectiveness comparative to the PLIF group according to the Thai context.
Our finding on the cost-effectiveness of LLIF with TCP + IBG was compared with many studies that compared cost-utility between LLIF and PLIF. Our study demonstrated a lower total lifetime cost of LLIF, compared with PLIF, of about 1145 USD per patient. The study by Deluzio et al3 and Lucio et al4 revealed a cost savings of 2 levels of LLIF greater than PLIF at 2563 USD per patient and 2825 USD per patient in a time interval of 45 days consecutively. Furthermore, the study by Hartman et al30 found that a standalone LLIF also showed a cost savings of 7756 USD per patient more than PLIF with a 30-day follow-up.
In contrast to our study, Gandhoke et al7 showed the different outcomes in the 2-year time horizon of a single-level LLIF group vs TLIF group. They revealed similar mean cumulative QALY gained in the 2-year interval (0.67 for TLIF and 0.60 for LLIF; P = 0.33) and had to use an additional cost (ICER) of 35,347 USD to provide 1 additional QALY gain compared with TLIF. However, LLIF was concluded to be cost-effective due to the high value of the WTP threshold at 100,000 USD/QALY in their country. Additionally, in our study in Thailand on single-level spinal fusion with 1-year follow-up, the utility of LLIF was lower than that of PLIF (0.84 vs 0.89, respectively; P = 0.023). LLIF was not cost-effective compared with PLIF with an ICER of 19,359 USD per QALY gained, interpreted at the WTP threshold of 5003 USD/QALY. The Thai WTP threshold was much lower than that of the USA.5
The reasons for the difference in the economic model outcomes between our present study and previous studies are the following: First, in the current study, we focus only on a less expensive TCP + IBG rather than a more expensive rhBMP-2 as a bone substitution. The average price of an Infuse kit was 4632.2 USD (2.8 cc of rhBMP-2), while a β-TCP price was 179.2 USD (cost per 2–3 cc strips of TCP).6 Second, the rate of revision and adjacent revision surgery was higher in PLIF than in LLIF. Nemani et al14 reported a rate of postoperative revision surgery of 1.69% in LLIF mainly due to persistent clinical symptoms, while Kobayashi et al16 reported 2.03% in PLIF/TLIF due to surgical site infection and dural tear. The studies by Nayar et al15 and Sears et al17 showed that the incidence of the adjacent revision rate in LLIF was only 0.88% per year compared with 2.5% to 3.9% per year in open PLIF. Third, our study did not find significant differences in utility gained after 2 years of follow-up between LLIF and PLIF. However, we used the nonadjusted utility data (LLIF = 0.854 and PLIF = 0.882) in the economic model. These 3 important input parameters resulted in the higher total lifetime cost and QALY of PLIF, compared with that of LLIF, as well as the different economic outcomes compared with other previous studies.
Strengths and Limitations
Our study had many strengths. First, our study showed all data that affect the clinical and economic comparison between LLIF and PLIF procedures, which included clinical outcomes and radiographic data in 2 years of follow-up and a cost-utility analysis. To our knowledge, there is no previous study that has conducted all dimensional data analysis and compared duration of follow-up times in LLIF and PLIF before. Second, we used the cost-utility analysis from the societal perspective to project the clinical and economic outcomes within the lifetime time horizon. These methods reduce the uncertainty of short-term postoperative outcomes. Third, we used all costs from local sources, and a cost-utility analysis was conducted from a societal perspective. And fourth, experts in the clinical field were involved in the development and analysis of economic models. The main limitation of the present study is its single-center retrospective design and relatively small sample size. These limited the generalizability of the results acquired from this study. Furthermore, there were transitional probabilities that we could not find through the literature review process; therefore, these parameters were based on experts’ opinions. More studies with more valid methods and larger sample sizes are needed to confirm the precise knowledge.
Conclusions
LLIF with TCP + IBG demonstrated excellent radiographic and equally clinical health-related outcomes compared with PLIF with LBG. In economic evaluation modeling, the total lifetime cost was lower in LLIF with TCP + IBG than in PLIF with LBG. Furthermore, LLIF with TCP + IBG was cost-effective compared with PLIF according to the context of Thailand. Therefore, LLIF with TCP + IBG could be considered as the alternative treatment for degenerative spinal disease in a developing country.
Acknowledgments
All authors gratefully acknowledge Miss Supani Duangkaew of the Orthopedic Research Unit, Department of Orthopedic Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University for data analysis and coordination of the journal submission process.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval The protocol for this study was approved by the Institutional Review Board of the Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand (COA no Si 679/2023).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.