


ABSTRACT
Background: Abnormal anatomy is a contributory factor to wrong-level surgery. Variations in the number of vertebrae in populations from different races and geographical regions have been described. A ∼10% prevalence of variations in number of thoracic and lumbar vertebrae in adolescent idiopathic scoliosis (AIS) patients has been previously reported. The objectives of present study were (i) to find out the prevalence of variations in the number of thoracic and lumbar vertebrae and the presence of lumbosacral transitional vertebrae (LSTV) in Indian AIS patients and (ii) to correlate these variations with gender and type of curve.
Methods: Hospital records and imaging of 198 AIS patients were reviewed retrospectively. A standardized numbering strategy was used to identify the number of thoracic vertebrae, number of lumbar vertebrae, and presence of LSTV. Patients' gender and curve type were correlated with the presence of an abnormal number of thoracic or lumbar vertebrae. Radiology reports and operation notes were reviewed to find out instances when the radiologist or surgeon had identified an abnormal number of vertebrae.
Results: Forty patients (20.2%) with abnormally numbered thoracic or lumbar vertebrae were identified. Twenty patients (10.1%) had abnormally numbered thoracic vertebrae, and 33 patients (16.7%) had abnormally numbered lumbar vertebrae. The prevalence of LSTV was 18.2%. Presence of variations did not correlate with gender or curve type. Radiology reports identified 2/40 patients with variations, whereas operation notes showed 4/40 patients had been correctly identified to have abnormally numbered vertebrae.
Conclusions: There is high prevalence of variation in the number of thoracic or lumbar vertebrae in AIS patients, with most of those missed being identified by radiologists or surgeons. The patient's preoperative imaging must be scrutinized to identify these patients and take the variation into account to avoid wrong selection of fusion levels.
Level of Evidence: 3.
Clinical Relevance: Text. The study raises awareness about possibility of wrong selection in fusion levels due to anatomical variations in surgery for AIS.
INTRODUCTION
Wrong site surgery has been designated as 1 of 5 “never events” in surgery—catastrophic occurrences that are preventable and must never occur.1 The American Academy of Orthopaedic Surgeons has reported that, in an average career of 35 years, an orthopaedic surgeon has a 25% chance of performing surgery on the wrong site or on the wrong patient.2 In a questionnaire-based study of the members of the American Academy of Neurologic Surgeons, half of the respondents reported that they had performed a wrong-level spine surgery at least once in their career.3 Similar figures were reported in a survey of neurosurgeons who were members of the Canadian Neurosurgical Society or the Royal College of Physicians and Surgeons.4 With many of these cases getting caught up in litigation, it is obvious that the ramifications of wrong-level spine surgery are worrying for both the patient and the surgeon.5 Anatomical variations and abnormalities have been identified as an important cause of wrong-level spine surgery.5–7 Use of intraoperative fluoroscopy is the most common way of identifying the correct level, since depending on visible or palpable anatomical landmarks alone is not reliable.8 In such a scenario, if the patient has unusual anatomy with an abnormal number of vertebrae that is not recognized before the surgery, intraoperative counting using fluoroscopy is prone to error and may lead the surgeon to a wrong level.
Authors of studies dating back to the early part of the 20th century have reported on variations in number of vertebrae in populations from different races and different geographical regions.9–11 More recently, 2 studies have reported on variations in the number of thoracic and lumbar vertebrae in patients with adolescent idiopathic scoliosis (AIS).12,13 While most of the literature on wrong-level surgeries has been with special reference to lumbar or cervical discectomies, operating at the correct levels is important in scoliosis surgery as well, since the choice of fusion levels can have important repercussions in outcome. In keeping with a long history of immigrations and invasions, India has served as a major corridor for dispersal of modern humans.14 The genetic, ethnic, religious, linguistic, and cultural plurality of this country gives it a unique identity from a racial point of view.15 With no previous authors, to our knowledge, reporting on the numerical variation in the thoracic and lumbar vertebrae in AIS patients from this part of the world, we decided to undertake this study with the following objectives: (i) to find out the prevalence of variations in the number of thoracic and lumbar vertebrae as well as the presence of lumbosacral transitional vertebrae (LSTV) in Indian AIS patients, (ii) to correlate these variations with gender and type of curve, and (iii) to establish how many of these variations were identified by the operating surgeons or the radiologists who examined the patients' preoperative imaging.
MATERIALS AND METHODS
The procedures used in this study adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study. Patients signed informed consent regarding publishing their data and photographs. The study was performed after prior approval from the Institutional Ethics Committee. Hospital records and imaging of patients with AIS who were operated at a single institute between January 2008 and October 2019 were retrospectively reviewed. Patients with a diagnosis of AIS who were surgically treated and had complete preoperative and postoperative radiological records were included. Patients with other types of scoliosis or without complete radiological records were excluded. Clinical details were documented from hospital records.
All patients had preoperative whole spine standing posteroanterior and lateral radiographs, in addition to noncontrast computed tomography (NCCT) scans of the whole spine with three-dimensional (3D) reconstruction images as a part of our routine protocol. The radiological analysis was performed by 2 orthopaedic surgeons (NM, AG) and 2 orthopaedic residents (NR, AU). We documented the number of thoracic vertebrae, the number of lumbar vertebrae, and the presence or absence of LSTV in each case. This was primarily done using the 3D reconstruction images and the coronal sections of the whole spine NCCT and corroborating it with whole spine radiographs. For this study, we followed the steps of labeling or numbering vertebrae laid out in the Spinal Deformity Study Group's Radiographic Measurement Manual.16 The first cephalad vertebra with a rib attachment was identified as the first thoracic vertebra. In addition, all the subsequent vertebrae with rib attachments, irrespective of whether they were normal or hypoplastic, were designated as thoracic vertebrae. Where there was a doubt regarding whether the ribs were hypoplastic, morphological comparison was made with the lumbar transverse processes—if a morphologically similar transverse process was identified, the vertebra was identified as a lumbar vertebra. Care was taken to ensure that a cervical rib was not miscounted as a thoracic rib by confirming that the rib was attached to the manubrium. All mobile and fully segmented vertebrae caudal to the last identified thoracic vertebra were identified as lumbar vertebrae. An LSTV was defined as a lumbar vertebra in which one or both of the transverse processes attached to the sacrum, through incomplete or complete osseous fusion or through a diarthrodial joint. This was also counted as a lumbar vertebra.
We also reviewed both the operative notes and radiologist's reports of preoperative radiographs for each patient where a variation in the number of vertebrae was encountered. In the operative notes, the surgeons had noted the levels at which the screws were placed and fusion was done. These were counted again on the postoperative radiographs considering the numbering strategy used in this study to identify the instances when the surgeons had missed identifying the variations in the number of vertebrae. The radiologist's reports were also read and reviewed to check whether they had identified the abnormally numbered vertebrae.
Statistical analysis was done using Stata 16 (StataCorp LLC, College Station, TX). The variation in the number of thoracic or lumbar vertebrae was correlated with gender; the variation in the number of thoracic vertebrae was correlated with the presence of a main thoracic (MT) structural curve (Lenke types 1–4 and 6), and the variation in the number of lumbar vertebrae was correlated with the presence of a thoracolumbar/lumbar (TL/L) structural curve (Lenke types 3–6). With each of these parameters being categorical variables, the χ2 test or Fischer's exact test was used to look for statistically significant difference. A P value <.05 was taken to be statistically significant.
RESULTS
A total of 221 AIS patients were operated between January 2008 and October 2019; 23/221 AIS patients did not have adequate radiological records and were excluded. The remaining 198 patients met the inclusion criteria and constituted the study population. An overwhelming 79.3% (157/198) of these patients were females. The mean age of the study population was 15.42 (range: 10–20 years). Over half of the patients (54%) had a Lenke Type 1 curve. The gender distribution and distribution of curve types have been detailed in Table 1.
Distribution of patients according to gender and curve types.
Forty patients (20.2%) had a variation in the number of thoracic or lumbar vertebrae, with 13 patients having a variation in both. All 13 patients had 11 thoracic vertebrae and 6 lumbar vertebrae. There was no patient who had 13 thoracic vertebrae and 4 lumbar vertebrae. 20/198 patients (10.1%) had a variation in the number of thoracic vertebrae, all of whom had 11 thoracic vertebrae (Figures 1 and 2). A total of 33/198 (16.7%) had a variation in the number of lumbar vertebrae; 7/33 patients had 4 lumbar vertebrae (Figures 3 and 4), whereas 26/33 patients had 6 lumbar vertebrae (Figures 5 and 6). In none of the patients was a cervical rib noted. LSTV was present in 36/198 patients (18.2%) (Figure 7); 16 of these were present in patients with a variation in the number of lumbar vertebrae (Figure 8). These findings are summarized in Table 2. Correlations between gender and the presence of variations in the number of vertebrae (Fisher exact test; P = .99), between the presence of a MT structural curve with presence of variation in the number of thoracic vertebrae (Pearson's χ2 test; P = .16), or between the presence of a TL/L curve with presence of variation in the number of lumbar vertebrae (Pearson's χ2 test; P = .12) were not found to be statistically significant.

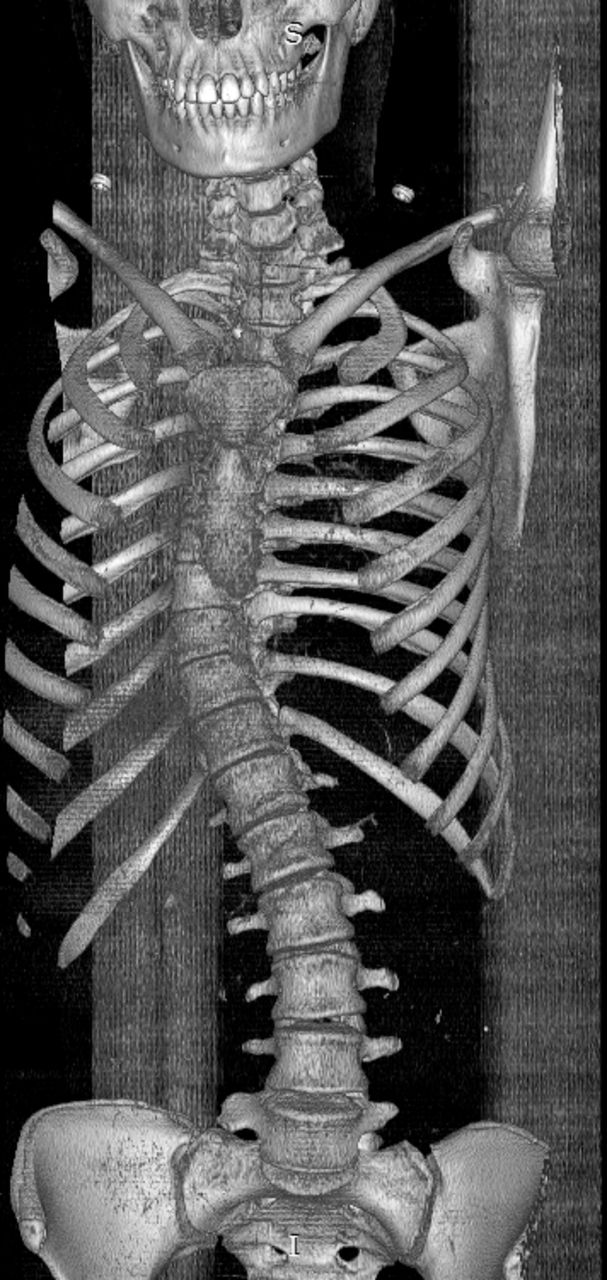
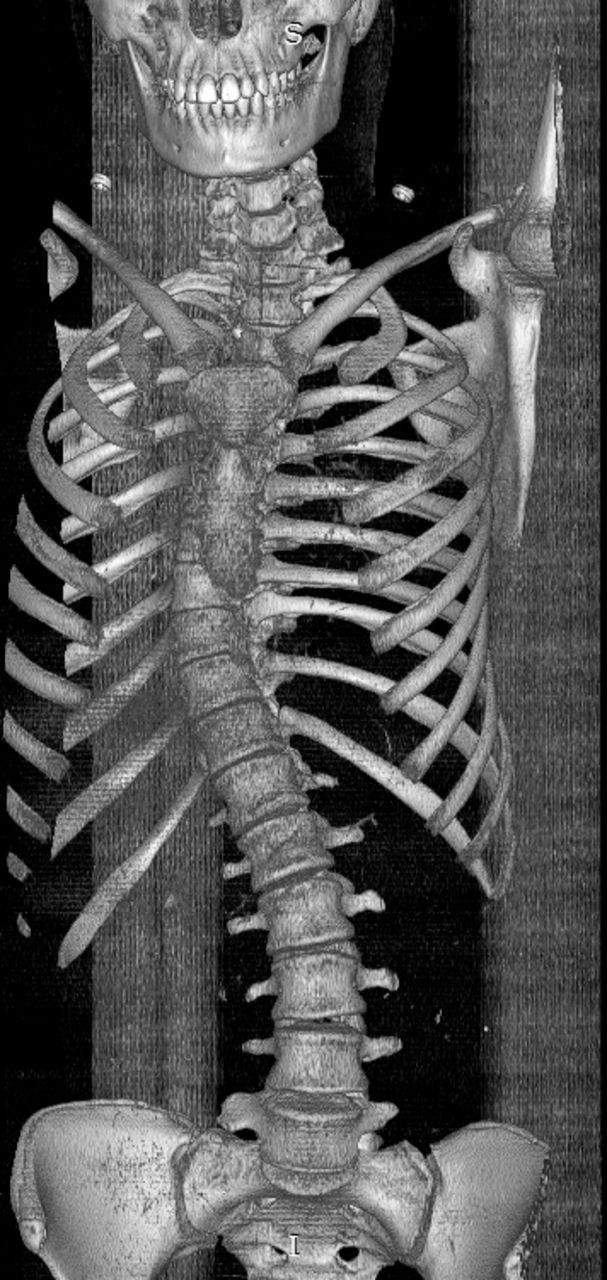
Three-dimensional reconstructed computed tomography imaging (A) of whole spine of 18-year-old female patient with 11 thoracic vertebrae.

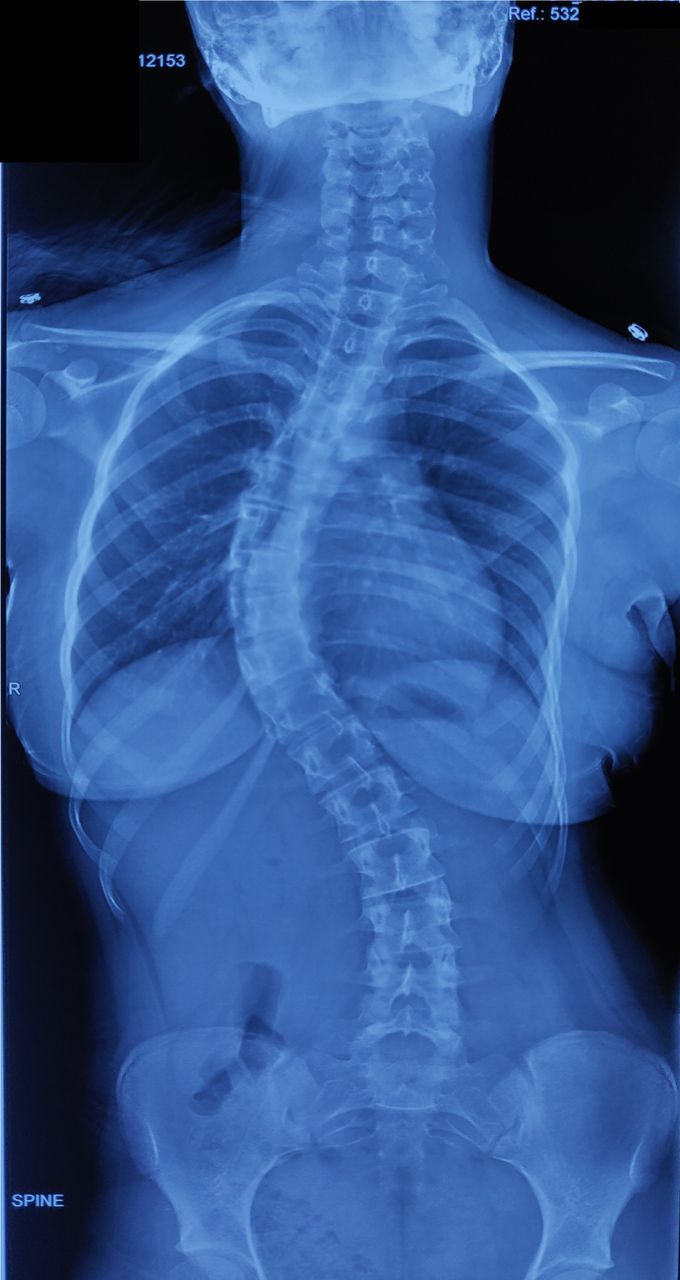
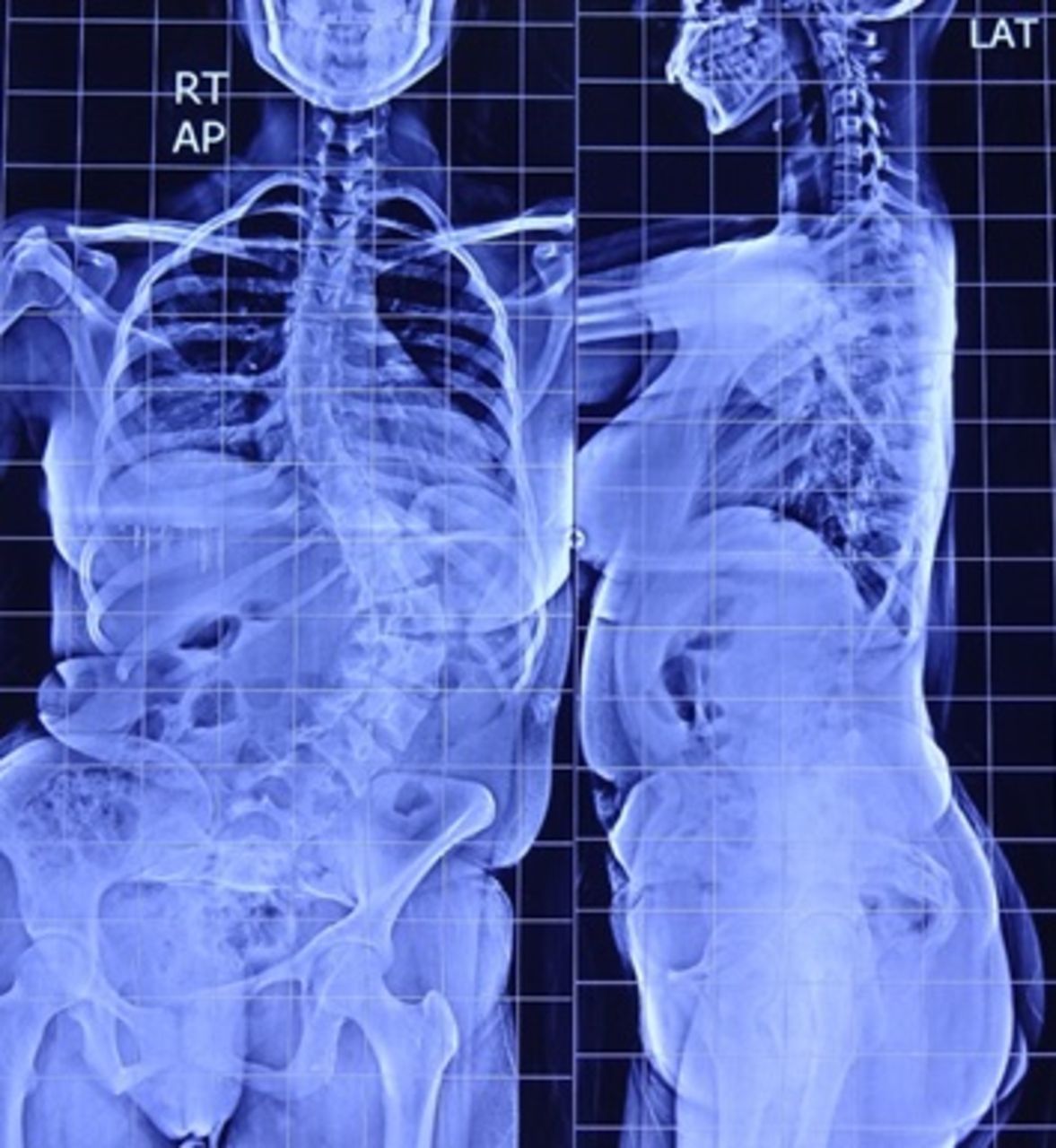
Posteroanterior and lateral whole spine x-ray of 18-year-old female patient with 11 thoracic vertebrae.

Three-dimensional reconstructed computed tomography imaging of 16-year-old female adolescent idiopathic scoliosis patient having 4 lumbar vertebrae.

Posteroanterior and lateral whole spine radiograph of 16-year-old female adolescent idiopathic scoliosis patient having 4 lumbar vertebrae. Note the presence of a hypoplastic rib at D12; this was counted as a thoracic vertebra.
Posteroanterior radiograph of a 13-year-old patient with 6 lumbar vertebrae.
Three-dimensional reconstructed computed tomography imaging of a patient with 6 lumbar vertebrae.

Three-dimensional reconstructed computed tomography imaging of a 13-year-old patient with a left-sided lumbosacral transitional vertebra.

Three-dimensional reconstructed computed tomography imaging of a patient with both left-sided lumbosacral transitional vertebra and 6 lumbar vertebrae.
Variations in the number of vertebrae and presence of lumbosacral transitional vertebrae in the study group of adolescent idiopathic scoliosis patients.
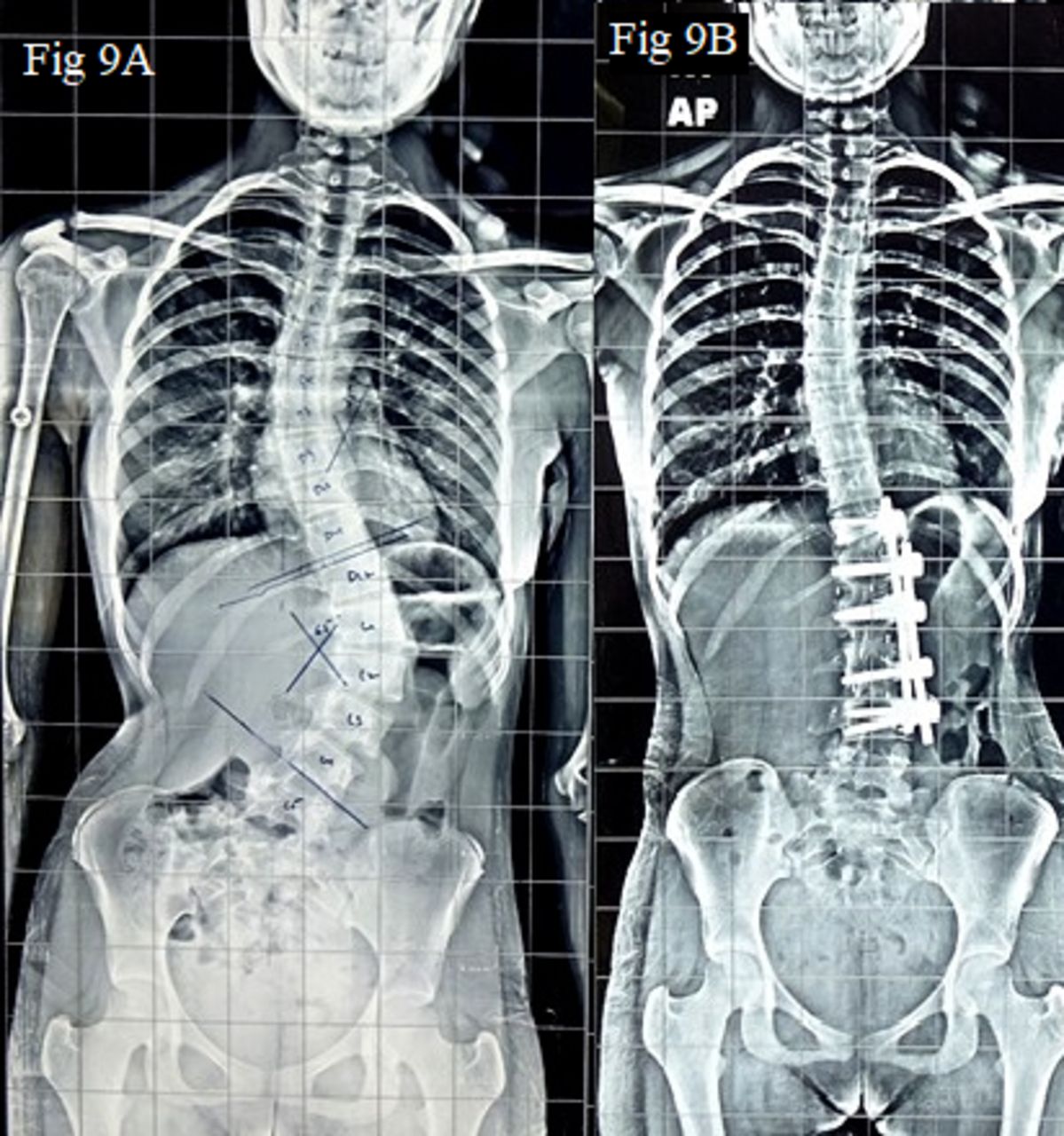
Only 2/40 patients (5%) with variations in the number of thoracic or lumbar vertebrae had a mention of such a variation in the radiology report of their preoperative radiograph. Moreover, when the labeling of the fusion levels in the surgeons' operative notes were analyzed, only 4/40 patients (10%) had the fusion levels labeled correctly if the variations were considered (Figures 9A and 9B).

(A) Preoperative posteroanterior radiograph of a 15-year-old female with a Lenke Type 5 curve with 4 lumbar vertebrae. However, in counting cephalad from L5, the surgeon has erroneously marked the D12 vertebra as L1 during preoperative planning. (B) Postoperative radiograph of the patient shown in (A). The fusion levels in the operation notes have been wrongly labeled as D12 to L4, when in fact, by conventional counting, the fusion levels would be D11 to L3.
DISCUSSION
Spine surgery, because of several inherent factors, portends an increased risk of operating at the wrong level than other types of surgeries.17 In fact, the North American Spine Society has also proposed guidelines in a bid to eliminate wrong-level surgery.18 Patients with variations in spinal anatomy are particularly likely to have their level of pathology miscalculated.4 The normal practice followed by most surgeons during intraoperative localization under fluoroscopy of a particular vertebral level during surgery is to count cephalad starting from the sacrum when the intended site of surgery is in the lumbar or lower thoracic region or to count caudad starting from the vertebra bearing the first rib (T1) when the intended site of surgery is in the upper thoracic region. Even with this practice, there are specific situations when intraoperative visualization of vertebral anatomy is difficult; poor bone mineral density, obesity, and scoliosis are examples.17
Variations in the number of vertebrae have been reported previously in South African Bantu tribes, American whites and Negros, and Australian aborigines.9,10,11,19 Such a variation in the number of vertebrae will make intraoperative localization of a particular vertebral level prone to error unless it is identified preoperatively and kept in mind during the counting process. Surgery for scoliosis usually involves long fusions of the thoracic and lumbar spine. The essence of deformity surgery lies in achieving an optimal curve correction with satisfactory coronal and sagittal balance without unnecessary sacrifice of motion segments, particularly in the lumbar spine. An inappropriate choice of fusion levels in scoliosis can lead to suboptimal curve correction, postoperative coronal or sagittal decompensation, distal adding-on of the curve, development of proximal junctional kyphosis, postoperative shoulder imbalance, and unnecessary loss of trunk mobility.20–24
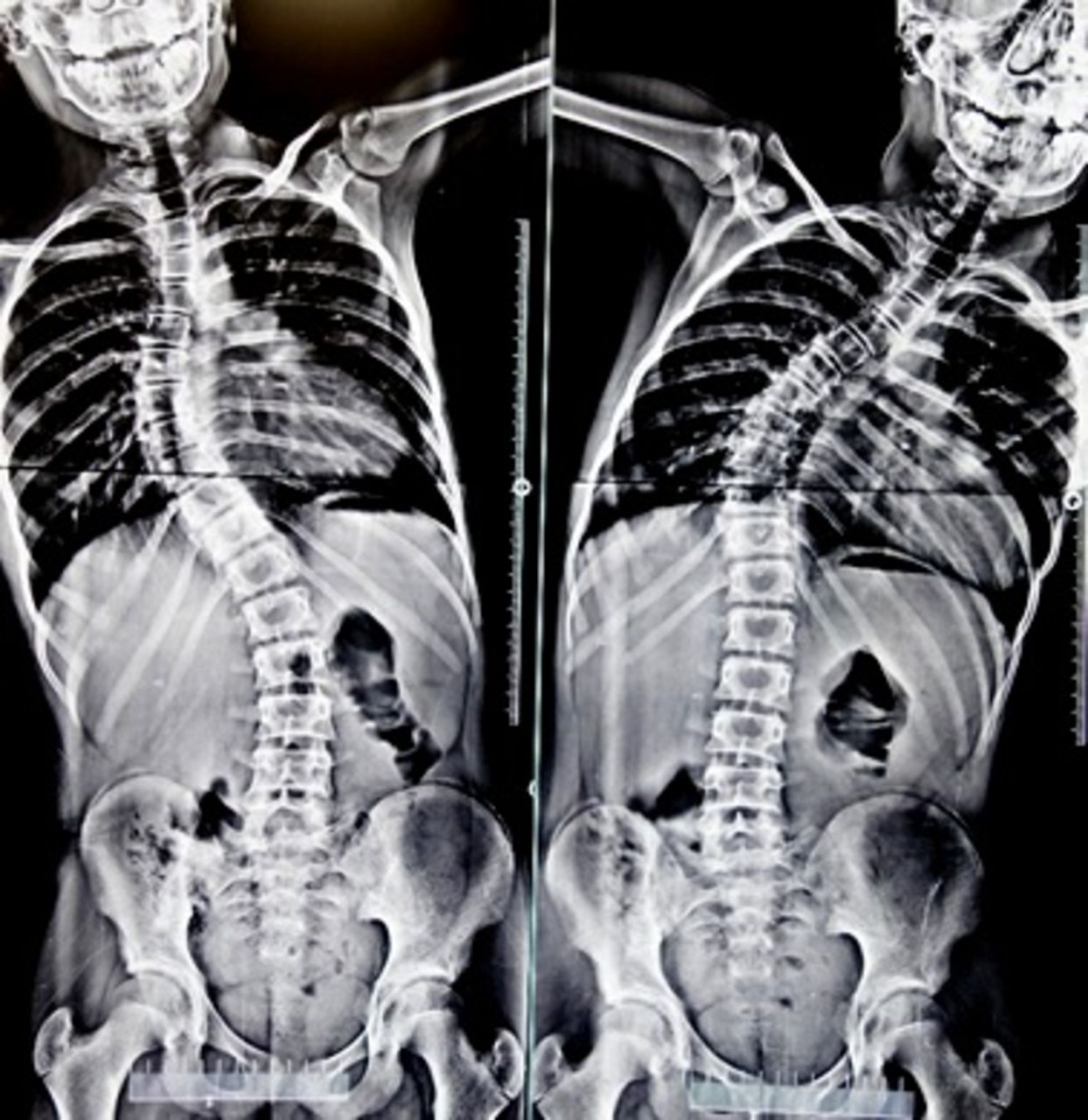
Two studies so far have described variations in thoracic and lumbar vertebrae in AIS patients. Ibrahim et al12 reported that 10.4% of the 364 AIS patients they studied had an abnormal number of thoracic or lumbar vertebrae as seen on full-length radiographs. Similar findings were echoed by a study from China, where the proportion of AIS patients with an abnormal number of vertebrae was 10.6%.13 Furthermore, this study also had a control group; however, no significant difference in the prevalence of variations in the number of vertebrae was noted between the AIS patients and the control group. Our study on 198 Indian AIS patients has some important methodological differences from the earlier 2 studies. Unlike the use of only the full-length whole spine radiographs by the earlier studies, we have used 3D reconstruction and coronal sections of NCCT scans of the whole spine to look for abnormal number of vertebrae or the presence of LSTV and corroborated this with full-length radiographs for each patient. In a developing country like ours where the imaging facilities are not necessarily of a high standard, the full-length whole spine radiographs are often not up to the mark. Scoliosis radiography mandates a careful attention to technique, and small differences in rotation, magnification, or patient position can significantly alter measurements.25 When the field of view is too large for a single projection, 2 or more digital radiographs are “stitched” together to form a full-length spine radiograph (Figure 10). In addition, various studies have declared that anteroposterior (AP) radiographs are inadequate to detect LSTV.26,27 We also correlated the abnormal number of vertebrae with gender, all variations in the number of thoracic vertebrae with the presence of a MT structural curve, and all variations in the number of lumbar vertebrae with the presence of a TL/L structural curve. However, no statistically significant difference was found in any of these correlations. Our study findings were compared with the findings of studies on variations in number of vertebrae in AIS patients published from United State of America (USA) and China (Table 3). We found a much higher prevalence of AIS patients with variations in the number of thoracic or lumbar vertebrae (20.2%). The prevalence of LSTV, which was 18.2% in our study population, was also higher than both these studies and the only other Indian study quoting the prevalence of LSTV in nonscoliotic patients.28 Startlingly, only a small fraction of patients with variations in the number of thoracic or lumbar vertebrae were identified by the radiologist reporting the preoperative radiographs (2/40; 5%) and by the surgeons, as gauged by their labeling of fusion levels in operative notes (4/40; 10%). Spencer et al29 made a similar observation in their study by noting that, in patients with abnormal vertebral counts, the surgeon's labeling of fusion levels differed from the actual conventional numbering in 41% of cases, whereas the radiologist's report did not report the abnormal vertebral counts in 51% of cases. One possible explanation for this is the greater insistence placed on meticulous documentation in the USA to avoid litigation and problems in disbursement of insurance claims because of discrepancy in the reported fusion levels in the radiology report and the surgeon's operative report; hence, the specialists are more likely to be oriented to this potential problem and exercise greater caution in ensuring that such variations in numbering of vertebrae do not go amiss. This contrasts with the situation in India, where the medicolegal consequences do not weigh as heavily on the minds of the specialists. Either they may not recognize this abnormality in number of vertebrae due to a general lack of awareness about its incidence in the AIS population, or they may not consider it important enough to be reported even after recognizing it. In any case, this study becomes more important in the Indian context to underscore the importance of preoperative recognition of the numerical variation in thoracic and lumbar vertebrae in AIS and making sure it is reported to avoid medicolegal consequences and potential risks of performing a wrong-level surgery.

Example of a “stitched” view of whole spine. A left-sided lumbosacral transitional vertebra can also be seen.
Comparison of the findings of our study with previously published literature.
We recognize certain limitations of our study. Firstly, the sample size is small, and all AIS patients were recruited from a single center. Secondly, we did not include a control group from the general population or from nonoperatively managed AIS patients to establish whether the reported prevalence of numerical variations in thoracic and lumbar vertebrae are specific to the operatively managed AIS patients. There was ethical concern in getting a CT scan or whole spine radiograph done for the control group; the patients in this study exclusively belonged to the pediatric age group, where these concerns are paramount. Thirdly, the retrospective nature of the study rules out the possibility of studying the association between anatomical variations and wrong-level surgery on treatment outcomes. Considering our findings that an overwhelming majority of Indian radiologists and surgeons seem to be unaware of the reasonable incidence at which abnormal numbers of vertebrae are found in the AIS population, there seems to be a pressing need to include this as a teaching point for radiologists and surgeons alike, with emphasis on recognizing and reporting these variations and enforcing strictly a uniform strategy such as that recommended by the Spine Deformity Study Group. Since ours was a retrospective study, we could not compare the results after such a teaching session was conducted for the specialists, but we do recognize the scope of a future prospective study on these lines to find out the difference it can make to our clinical practice.
CONCLUSIONS
We report that there is indeed a high prevalence of variations in the number of thoracic and lumbar vertebrae as well as the presence of LSTV in patients with AIS which do not bear a correlation with gender or the curve type. Most of these variations are missed by the radiologist or the surgeon involved. We recommend that carefully counting the number of thoracic and lumbar vertebrae on the patient's preoperative CT scan and radiographs can help identify these variations and avoid misjudging the intended fusion levels by making errors in their intraoperative localization.
Footnotes
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.