


Abstract
The goal of a spine surgery is to achieve adequate neural tissue decompression, maintenance of spinal stability, and successful stabilization of an unstable spine. To achieve these surgical goals, damage to normal tissues, including the spinal column and surrounding soft tissues, is inevitable after the beginning of a spine surgery. Extensive damage to normal spinal column and paraspinal collateral tissues during operation can lead to unsuccessful outcomes due to persistent axial pain and additional surgeries due to occurrence of spinal instability. Numerous efforts, such as the usage of microscopy, tubular retractor systems, percutaneous instruments, and trials of new operative approaches have been attempted to reduce normal tissue damage and improve surgical outcomes. Endoscopic spine surgery (ESS) was introduced about 3 decades ago as a minimally invasive spine surgery and has been widely spread with the development of endoscopic surgical instruments and adoption of new endoscopic surgical approaches during the past 2 decades. Theoretically, ESS may be the gold standard method of spine surgery because of its minimal tissue damage and good visualization of the surgical field. However, surgeons hesitate to initiate an ESS due to its steep learning curve and the lack of high-level evidence of surgical outcomes. In this article, the rationale and advantages of performing ESS are discussed by reviewing published articles.
INTRODUCTION
Healthy maintenance of normal spine alignment and neuromuscular structures around the spine is essential to live human life actively. Recently, the number of patients with spinal diseases has rapidly increased with extended life expectancy.1 Main symptoms of spinal disease such as axial back pain, radiating leg pain, and neurogenic claudication can be treated with conservative methods including rest, pain medications, physical therapy, and lumbar epidural blocks. For cases refractory to conservative treatment or with neurologic deficits, decompression of neural structures or stabilization of the spinal column should be considered. Decompressive laminectomy, discectomy, and fusion surgery can be performed with an open surgical field to treat spinal problems. However, they can lead to damage of paraspinal soft tissues or the spinal column with the facet joint that sometimes need additional spinal surgery.2,3
Minimal invasive spine surgery (MISS) has been conspicuously developed in the last 3 decades to reduce the damage to normal spinal structures during an operation and improve functional outcomes. MISS can be divided into 2 main streams: (1) spine surgery using a tubular retractor system and (2) an ESS. MISS using a tubular retractor can reduce damage to paraspinal muscle and ligaments compared to a traditional open surgery. However, its narrow surgical field may be associated with technical difficulty and risk of neural tissue damage.4,5 Moreover, paraspinal soft tissue injury cannot also avoid to exposure of surgical field. Another mainstream of MISS is ESS. Initially, ESS was started slowly through a transforaminal route to remove posterolateral or central disc herniations.6 At that time, ESS had many limitations due to restricted surgical instruments, blurred visions from the existing camera system, high radiation exposure, and a steep learning curve. However, ESS has rapidly expanded from the lumbar spine to cervical and thoracic lesions with developments of better endoscopic equipment and the introduction of new endoscopic approaches, including an interlaminar approach and biportal endoscopic approach during the past 2 decades.7,8 In this article, the authors review published articles and discuss the rationale and advantages of ESS.
BRIEF HISTORY OF SPINE SURGERY: OPEN, MICROSCOPY, AND ENDOSCOPY
Lumbar disc herniations and spinal stenosis are common spinal degenerative disorders presenting motor and/or sensory deficits and neurogenic claudication in affected nerve roots. To find the current and future directions of spine surgery, it is very important to understand the history of spine surgery for lumbar degenerative disc herniations and spinal stenosis, which are the most common spine problems that require surgery. In the early decades of spine surgery, open surgery was mainly performed to decompress the thecal sac and nerve roots through total or subtotal laminectomy with extensive paraspinal muscle and ligament dissections.9 Successful removal of disc fragments or decompression through total laminectomy can improve radicular pain from nerve root decompression with wide vision space. However, it can lead to unexpected clinical results due to extensive damages to normal tissues including facet joint, paraspinal muscles, and ligaments.10 An interlaminar approach to remove disc herniation or canal decompression using microscopy was introduced in 1978 and published in The Spine Journal. This method had been considered the gold standard approach for lumbar disc herniations because it could minimize normal spinal bone and collateral damages compared to the previous open surgery through total or subtotal laminectomy.11 Successful adoption of microscopic lumbar spinal surgery makes it possible to perform complete nerve root decompression safely with reduced iatrogenic injury of the spinal column and paraspinal soft tissues. Favorable outcomes can also be achieved through a microscopic interlaminar approach for a long time. Despite these favorable outcomes, facet joint violation and injuries to iatrogenic paraspinal muscles and ligaments are still causes of persistent back pain and can accelerate the degenerative process of spine.12 The introduction of assessment tools for functional outcomes has accelerated the development of new surgical techniques and approaches to preserve normal spinal column and paraspinal tissues for improving functional outcomes.
During the development of an interlaminar approach using microscopy, percutaneous discectomy was initially performed under a fluoroscopic view. However, this technique was not widespread at that time. Kambin established the “Kambin triangle” as a safe working zone to the lumbar disc area between the superior articular process and the exiting nerve root.13 Percutaneous surgery through the Kambin triangle could theoretically result in successful discectomy without collateral damages, and it was expected to reduce postoperative back pain and promote early recovery.14,15 After introduction of the Kambin triangle, percutaneous discectomy using spinal endoscopy was initiated by several pioneers with favorable outcomes. However, endoscopic discectomy was not a popular procedure for the first 2 decades after its introduction due to poor endoscopic image, limitations of endoscopic surgical instruments, limited indications, and a steep learning curve.
With the development of endoscopic instruments such as drills, punches, hooks, and camera systems, endoscopic lumbar discectomy has become a hot issue of spine surgery in the past 2 decades. In particular, the development of endoscopic tools can make it possible to achieve decompression of the central spinal canal, the intervertebral foraminal space, and the extraforaminal area via various surgical approaches, including transforaminal, interlaminar ipsilateral, interlaminar contralateral, and translaminar routes. Recently, biportal endoscopic spine surgery has been widely spread in Asia, especially in Korea.8 Although biportal endoscopic spine surgery is not a full-endoscopic spine surgery, relatively early adaptation of this technique in beginners for ESS might be an advantage to overcome the steep learning curve of ESS. The most important concept of a lumbar spine surgery is focusing on reducing damages to normal spinal structures and surrounding paraspinal soft tissues to enhance functional outcomes and achieve early return to normal activity. To achieve these goals, ESS has expanded from lumbar disease and simple decompression to cervical and thoracic spinal disease and eventually fusion surgery.
CURRENT STATUS, INDICATIONS, PUBLISHED OUTCOMES, AND COMPLICATIONS
To understand the rationale for ESS, it is essential to investigate the current status, indications, outcomes, and complications of ESS by reviewing published articles.
Current Status and Indications
A total of 4828 articles were found through a PubMed search using the term “endoscopic spine surgery” in May 2021. Most articles at the end of the 20th century were about transforaminal endoscopic lumbar discectomy (TELD) and accounted for about 10% of articles for ESS. Approximately 90% of ESS articles were published after the 21st century. The area of ESS in published articles has been expanded from TELD to interlaminar endoscopic lumbar discectomy, spinal canal decompression, including unilateral laminotomy bilateral decompression (ULBD), posterior cervical endoscopic foraminotomy, thoracic decompression or discectomy, and lumbar spinal fusion surgery.16,17 Spinal cord level decompression is also performed in current clinical fields with relatively favorable outcomes reported by a regional congress of spine surgery or published articles.18,19
Biportal endoscopic spine surgery was first introduced in 1996 by Antoni using arthroscopy.20 At that time, biportal approach was not popular in spine surgery. However, biportal ESS has been the hot issue in MISS during the past few years, especially in Asia. Biportal ESS is expanding from an interlaminar lumbar approach to a paraspinal approach, a posterior cervical approach, and a lumbar interbody fusion surgery with favorable outcomes in short-term follow-up studies.8,21,22 If the surgeon has sufficient experience of open microscopic spine surgery, biportal ESS can be easily adapted due to similar surgical anatomy, instruments handling, and clean magnified endoscopic view using large-diameter endoscopic camera and continuous fluent irrigation compared to a full-endoscopic spine surgery. For these reasons, biportal ESS may reduce surgery-related complications for beginners of ESS, and it may become a valuable approach with favorable outcomes and relatively lesser collateral damages. As mentioned above, concerns for ESS are increasing, and indications for ESS are also expanding to almost all spine diseases (Table and Figure).
Current published indications and methods of endoscopic spine surgery.
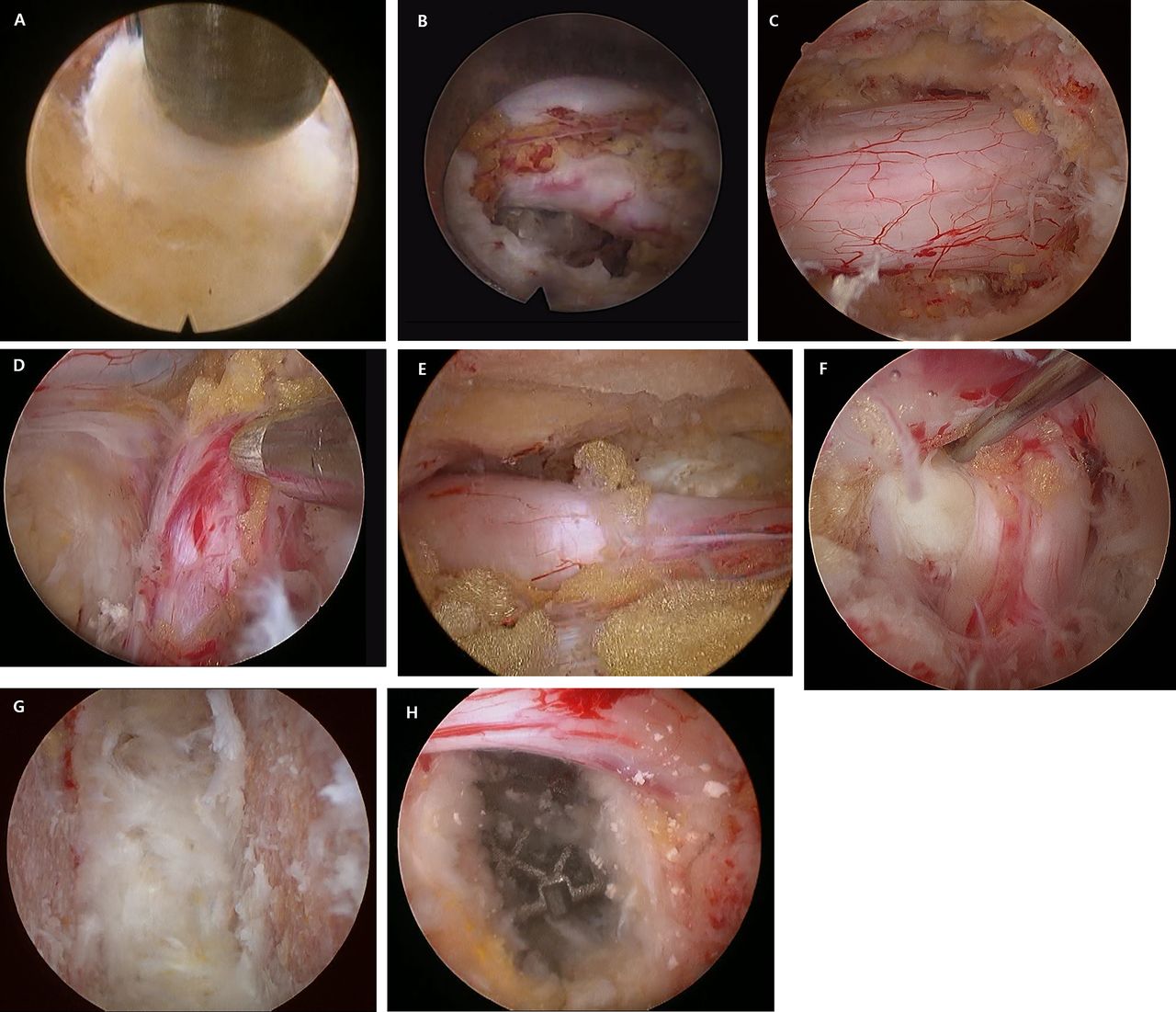
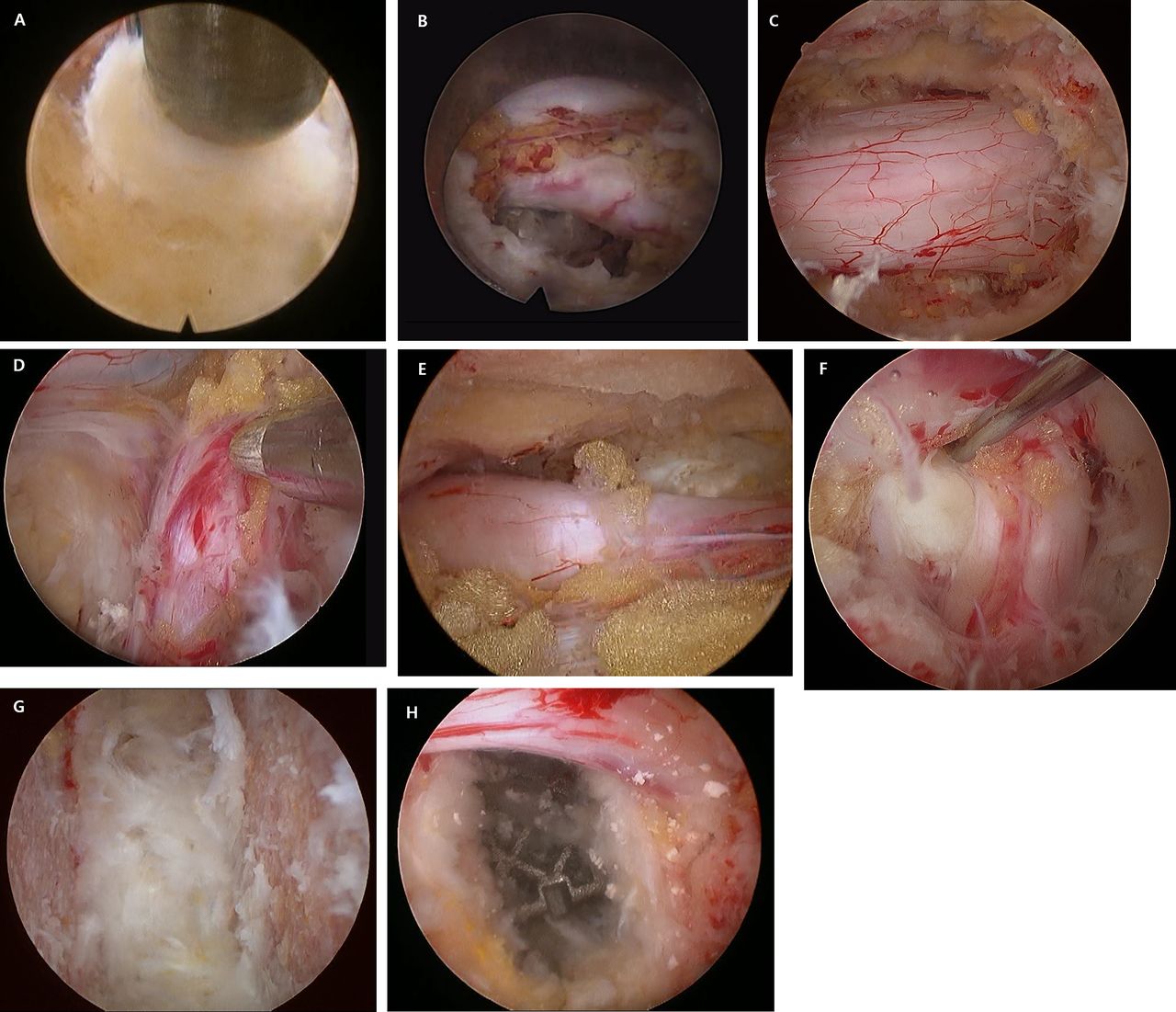
Various techniques of endoscopic spine surgery. (A) Transforaminal endoscopic lumbar discectomy. (B) Interlaminar lumbar endoscopic discectomy. (C) Interlaminar central lumbar decompression. (D) Paraspinal foraminal lumbar decompression. (E) Interlaminar contralateral lateral recess decompression. (F) Posterior cervical foraminotomy and discectomy. (G, H) Endoscopic lumbar interbody fusion (fusion bed preparation and cage insertion).
Published Outcomes
Many articles have reported ESS outcomes. First, some articles have compared outcomes between percutaneous endoscopic discectomy and microdiscectomy. Through a meta-analysis, Qin et al reported that there is no statistically significant difference in Visual Analog Scale score or Oswestry Disability Index (ODI) score between the percutaneous endoscopic discectomy and open microscopic discectomy.23 Surgery-related complications, operation time, and recurrence rate were also similar. However, hospital stay and return to work were shorter in the percutaneous endoscopic discectomy group. Another meta-analysis study had a similar complication rate, recurrence, and functional outcomes between endoscopic discectomy and open microscopic discectomy. However, shorter operation time and hospital stay were achieved in the group receiving an endoscopic discectomy.24 Percutaneous lumbar discectomy showed better midterm and long-term outcomes in visual analog scale for back pain and ODI scores compared to micro-endoscopic lumbar discectomy, though there were no significant differences in complication rate, recurrence, or reoperation between the 2 techniques.25 These results may indicate that percutaneous endoscopic lumbar discectomy may lead to early recovery and early ambulation with reduced iatrogenic injury to normal anatomical structures and preservation of back muscle function compared to a conventional open microscopic lumbar discectomy. However, a recent systemic review and meta-analysis concluded that TELD shows similar results in leg pain and functional status at intermediate and long-term follow-up compared to an open microscopic discectomy.26 Consequently, many studies, including the meta-analysis,26 reported an early recovery and return to work after a percutaneous lumbar discectomy. However, robust studies for functional outcomes with long-term follow-up and cost-effectiveness are lacking.
Endoscopic interlaminar approach was developed by Ruetten and colleagues, and this approach was adopted particularly in L5-S1 disc herniations.27 Before the introduction of the interlaminar approach, ESS had been mainly performed for lumbar disc herniation. However, the interlaminar approach with the development of endoscopic drills and punches makes it possible to perform a decompression surgery to treat lumbar central and lateral recess stenosis. A randomized controlled study between endoscopic interlaminar decompression and conventional open microscopic decompression for central and lateral recess lumbar spinal stenosis showed similar clinical results for both groups. However, surgery-related complications and revision rate were lower in the group receiving an endoscopic ULBD.28 Biportal ESS was developed from an interlaminar approach. It is applied mainly for discectomy and canal decompression. Theoretically, a biportal ESS may be more invasive compared to a uniportal ESS. However, it also has advantages of a minimally invasive surgery compared to an open microscopic surgery. Biportal endoscopic interlaminar approach has similar surgical anatomy to a microscopic open surgery. Instruments used for a biportal ESS are also familiar to spine surgeons. Therefore, its learning curve may be low compared to a full-endoscopic spine surgery. Favorable outcomes such as low estimated blood loss, less postoperative backache, and shorter hospital stay have been reported. The degree of spinal canal decompression can be sufficiently achieved through a biportal endoscopic decompression with favorable clinical outcomes.21 A meta-analysis of 5 comparative studies and 4 randomized controlled studies with a total of 994 patients was performed to compare interlaminar endoscopic ULBD and microscopic decompression for lumbar spinal stenosis.29 The study concluded that endoscopic interlaminar ULBD for lumbar stenosis had statistically significant lower backache or leg pain and lower risk of complications compared to microscopic decompression. However, operation time and ODI scores did not show statistically significant differences between the endoscopic ULBD and microscopic decompression. Although the evidence of endoscopic interlaminar ULBD for lumbar spinal stenosis was not very high, ESS showed favorable outcomes with a minimally invasive concept. In the future, cost-effectiveness, the degree of postoperative satisfaction, and quality of life should be analyzed with sufficient data to clarify the surgical effectiveness of endoscopic interlaminar ULBD.
Lumbar fusion surgery should become a definitive surgery in index level. Extensive damage to collateral tissues is inevitable in a conventional fusion surgery. Various techniques of lumbar fusion have been developed to reduce damage to normal spinal tissues and paraspinal soft tissues with successful decompression and firm fusion. As a minimally invasive technique, endoscopic lumbar interbody fusion (ELIF) has been initiated with results published. An ELIF through the Kambin triangle could be performed under local anesthesia as the most minimal invasive fusion technique. However, its initial results showed relatively high rates (20%–30%) of complications such as transient exiting nerve injury, subsidence, and nonunion.30,31 Due to the limitation of a trans-Kambin approach for interbody fusion, a posterolateral approach such as a minimally invasive transforaminal lumbar interbody fusion has been used for an endoscopic lumbar fusion. This approach can provide sufficient direct decompression of spinal canal and good visualization of fusion bed to prepare endplates.22 Denudation of fusion bed under clear endoscopic view, developments of 3D-printing cage, and fusion materials such as bone morphogenetic proteins and demineralized bone matrix might play an important role in an endoscopic fusion surgery for successful long-term outcomes with solid fusion. Based on the evidence provided, a systemic review and meta-analysis showed that there is no significant difference in clinical outcomes or safety between ELIF and minimal invasive transforaminal lumbar interbody fusion in the treatment of lumbar degenerative diseases.32 Although an endoscopic lumbar fusion needs a relatively long operation time, it has advantages of less tissue trauma and rapid recovery after operation. However, long-term outcomes of fusion rate and quality of life should be investigated and randomized controlled trials for high-quality evidence should be performed.
Despite the many trials that have been performed on surgeries for cervical and thoracic spinal lesions, there are few high-quality articles with a large number of subjects and long-term follow-up data. Ruetten et al reported that full-endoscopic posterior cervical endoscopic foraminotomy had a 96% success rate outcomes in a randomized controlled trial.33 Minimal invasive cervical posterior foraminotomy can reduce intraoperative blood loss, operation time, and immediate postoperative pain compared to an open procedure. Posterior cervical endoscopic foraminotomy with or without discectomy showed favorable clinical outcomes as a lesser invasive technique than an open microscopic posterior foraminotomy.34 The decompression of the spinal cord level is more challenging. Serious complications may develop after the surgery. However, some pioneers have initiated spinal cord level decompression for cervical spondylotic myelopathy or thoracic stenosis with favorable outcomes.17,18,35 The level of evidence in spinal cord level decompression using ESS is very weak, and some catastrophic complications such as quadriplegia and paraplegia can develop after surgery. Therefore, careful trials and step-by-step processing are mandatory to establish ESS for spinal cord level decompression with considerations for possible catastrophic complications.
When considering the effectiveness of ESS through published articles, lumbar ESS, including decompression and fusion, has demonstrated quicker recovery when compared to a traditional open microscopic surgery. The level of evidence is gradually becoming higher with some randomized controlled studies and meta-analyses. Results of ESS for cervical or thoracic lesions showed favorable outcomes with advantages of a minimally invasive technique. However, ongoing studies with high-level evidence are required.
Intraoperative Complications
Hematoma
Continuous saline irrigation offers clean surgical field and hydrostatic pressure on epidural venous flexus and exposed cancellous bone, and it enhances bleeding control during surgical procedures. However, bleeding may occur after cessation of continuous saline irrigation and hydrostatic pressure effect on working space. The insertion of a drainage catheter on the epidural space without root irritation to prevent epidural hematoma is recommended.
Increased Intracranial Pressure
Too much hydrostatic pressures by improper outflow could lead to elevation of intracranial pressure, which leads to headache and, in some cases, life-threatening seizures after the surgery. If dural tear occurs during decompressive procedure, the surgical procedure must be completed as quickly as possible.
Incidental Durotomy or Neural Tissue Injury
Currently, endoscopic images are 2-dimensional, which increases the risk of durotomy or neural tissue injury during endoscopic drilling or other decompressive procedures. It is recommended that bone work using the endoscopic drill should be completed before complete removal of ligamentum flavum to reduce the risk of durotomy or neural tissue injury. Further bone work using small osteotomes or angled Kerrison punch is less risky after complete removal of ligamentum flavum. If durotomy is developed during surgery, most of the cases with small durotomy can be treated using collagen fibrin patches without conversion of open surgery. However, cases with large dural defect (more than 1 cm) should be considered for open direct suture of the defect site.
ADVANTAGES OF ENDOSCOPIC SPINE SURGERY
Reducing Collateral Damage and Preservation of Facet Joint
Dissection and retraction of paraspinal soft tissues, including muscles and ligamentous structures, are inevitable for an open microscopic decompression surgery, including fusion. Depth of lesion and retraction time of paraspinal soft tissue are significantly correlated with serum creatinine kinase (CK) level.36 It means that the degree of CK elevation after spine surgery can indirectly indicate the degree of iatrogenic back muscle injury during an operation. Choi et al reported that the group receiving an open microdiscectomy shows higher elevation of serum CK level than the group receiving an endoscopic discectomy.37 Postoperative back pain during hospital admission and the duration of hospital stay are also significantly higher in the microdiscectomy group than in the endoscopic group. These results suggest that reducing iatrogenic injury to paraspinal tissues through an endoscopic approach may be helpful to obtain early activity and return to work.
Facet joint violation during spine surgery is also inevitable to obtain an optimal decompression of neural structures. If optimal decompression is not performed, surgical outcome will be poor due to incomplete canal decompression, the development of dynamic stenosis, or early restenosis. Microscopy offers a straightforward view of the target area for decompression. Therefore, about 30% of ipsilateral facet joint resection is required to reach successful decompression of the central canal and lateral recess.38 However, it has already been reported that slippage increment of segmental level can develop after a microscopic decompression.39 Full-endoscopic equipment has about 15° of angle, making it possible to undercut the facet joint during a decompressive surgery. This angle view has the advantage of preserving the facet joint compared to a microscopic surgery. A biportal ESS, which is becoming popular, can use 0° and 30° of endoscopy. It may be helpful to preserve the facet joint during surgery with view magnification. ESS may reduce iatrogenic injury of paraspinal soft tissue and the facet joint, and it is clearly helpful in improving functional outcomes and reducing hospital stay for patients with spinal diseases.
Recently, angled endoscopy and flexible drill have been used in an ESS, leading to successful decompression of foraminal lesions. In the microscopic era, a fusion surgery was mainly considered for cases with severe foraminal stenosis or combined foraminal disc herniations. However, ESS with instrumental development can solve lumbar foraminal lesions with only a decompression surgery without a fusion surgery. Kim et al reported successful decompression of L5-S1 foraminal and extraforaminal stenosis through a uniportal endoscopic contralateral approach.40 If ESS is not developed, these coexisting foraminal and extraforaminal lesions might have to be treated with a fusion surgery.
View Magnification and Clean Endoscopic View Through Continuous Irrigation
The development of spinal endoscopy has led to high magnification of the operation field, thus reducing the possibility of neural tissue injury and dura injury. Moreover, complete removal of pathologic lesions is also possible with the development of endoscopy and instruments, eventually leading to favorable clinical outcomes. Rough dissection between neural tissue and pathologic lesions may be associated with dura injury or neural tissue damages under an open microscopic view. However, spinal endoscopy can take more magnified images compared to a microscopy. It is very helpful for distinguishing normal area and pathologic area. Moreover, continuous irrigation provides a clean operative field through wash out of bone dust or other removed tissues, and hydrostatic pressure on exposed cancellous bone or venous plexus provides a clean operative field by reducing epidural bleeding.21
Low Risk of Infection
Discitis, spondylitis, and epidural abscess can be serious complications after a spinal surgery. Decreasing postoperative spinal infection may be an essential factor to reduce postoperative pain, hospital stay, and medical cost associated with each surgical method. The rate of postoperative infection after spinal surgery has been reported to be 4.4% in the modern antibiotic prophylactic era.41 However, postoperative infection after ESS has been rarely reported in the literature. The small skin incision in ESS may prohibit contact of airborne particles with the surgical wound. Continuous irrigation might also play an important role in decreasing the prevalence of postoperative spinal infection.
Fusion Bed Preparation
Fusion surgery should become the definitive treatment option in pathologic level. Adequate decompression and successful fusion are essential to reach favorable outcomes. Many spinal surgeons may consider that an endoscopic spinal fusion is unsuitable for achieving successful outcomes due to incomplete decompression, neural structure damages associated with a narrow surgical field, fusion failure, and so on. However, ELIF has been initiated by some pioneers with favorable outcomes as a technique of MISS.22,30,31 The removal of cartilage endplates and preservation of bony endplate are very important to reach successful solid fusion without subsidence. Heo et al reported that endplate preparation could be performed under direct clean endoscopic view to both endplates, and the use of angled spinal endoscopy can make it possible to have successful full preparation of the contralateral endplate.22 The development of fusion materials, well-designed 3D-printing cage, and expandable interbody cages will play an important role in successful endoscopic fusion surgery as a minimally invasive fusion technique.
Cost-Effectiveness
Cost-effectiveness is very important when determining the optimal surgical method. An ESS is a sufficient and safe surgical tool with higher patient satisfaction rate, lower intraoperative blood loss, and shorter hospital stay compared to a conventional open surgery. Medical costs may also be low for the endoscopic group with an early recovery from postoperative pain. Although a shorter hospital stay and earlier recovery might mean early return to workthe long-term outcome of an ESS might not be different from that of an open conventional surgery. Unfortunately, there are few articles that compare cost-effectiveness between conventional surgery and endoscopic surgery. Recently, Choi et al showed that the incremental cost-effective ration is higher in microdiscectomy than in endoscopic discectomy 1 year after surgery.42 More independent high-quality randomized controlled trials using sufficiently large sample sizes with cost-effectiveness analyses are needed.
Low Risk of Surgery-Related Morbidity
The percentage of the population aged 65 years or older is increasing in many countries. Older patients also have multiple medical morbidities, including diabetes mellitus, hypertension, hyperlipidemia, stroke, and cancer. The increment of an aging person with medical comorbidity might be associated with the development of serious medical complications after spine surgery. The development of serious medical complications is mainly related to long operation time and more intraoperative blood loss, especially in an aging person. This fact demands the application of lesser invasive surgical technique to spine diseases with less anesthetic requirements, low intraoperative blood loss, low risk of collateral damages, and shorter hospital stay. An ESS can be performed with epidural or local anesthesia and a relatively short operation time. It will be the most valuable benefit to reduce the development of medical comorbidity after surgery. Reducing paraspinal muscle damage and decreasing intraoperative blood loss are well-known benefits described in published literature.29,37
SUMMARY—RATIONALE OF ENDOSCOPIC SPINE SURGERY
Background
The use of microscopy for spine surgery could decrease damage of neural structures through magnification of pathologic lesions. However, early postoperative pain and persistent back pain due to collateral damages during open microscopic surgery have been continuously a hot-button issue to spine surgeons and patients. Collateral damage during open spine surgery may be a cause of postspinal surgery syndrome due to muscle atrophy and increment of segmental instability.
Technological Advancement
Spinal endoscopy was first used about 3 or 4 decades ago. Its limitations include poor images. In addition, its approach methods and restricted endoscopy instruments could disturb the expansion of ESS with a steep learning curve for spine surgeons. However, technological advancement of ESS is creating new surgical approaches and favorable clinical outcomes with decreased damages to the facet joint and paraspinal collateral tissues. View magnification, continuous irrigation system, water-based surgery, and use of endoscopy with angled lens may reduce neural structure damage, facet joint resection, and infection risk.
Early Recovery and Economic Benefits
Benefits of ESS in terms of preservation of normal spinal structures have been published in several articles. Although differences in long-term clinical outcomes between ESS and conventional microscopic surgery have not been clarified yet, the degree of normal structures damage is clearly associated with early postoperative pain. Axial spinal pain of paraspinal muscle-related pain can increase hospital stay. ESS can reduce immediate postoperative pain and inpatient stay, and ambulatory spine surgery is even possible without general anesthesia. Eventually, short hospital stays and ambulatory spine surgery can reduce the overall medical cost, thus decreasing the burden of health care in aging societies. Patients also receive economic benefits associated with reduced hospital cost and early return to work.
Surgical Variability
ESS was initially performed through the Kambin’s triangle. However, various approaches, including interlaminar approach, paraspinal approach, and contralateral approach have been used to treat a variety of lumbar spinal disorders with the development of endoscopic technology. ESS is expanding to cervical and thoracic spinal disorders with equivalent clinical outcomes and benefits of MISS, indicating that ESS can be a universal technique for treating various spinal diseases.
Patients’ Demands and Comorbidity
Patients with spinal disorders always want the least invasive technique to treat their problems. Aged patients with spinal problems often have multiple medical comorbidities. Short operation time, less blood loss, low-level anesthetic requirement, and decreased postoperative pain should be mandatory to reduce postoperative complications.
Currently, ESS might be considered the most suitable surgical technique to solve previously mentioned issues. Previously mentioned advantages of spinal endoscopy are very compelling to achieve goals of spinal surgery. In the future, studies about ESS with high-level evidence should be performed and published to support the superiority of ESS over conventional surgery as the gold standard minimally invasive technique for the treatment of spinal disorders.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}