


Abstract
Background There remains a paucity of literature on the impact of overlap on neurosurgical patient outcomes. The purpose of the present study was to correlate increasing duration of surgical overlap with short-term patient outcomes following lumbar fusion.
Methods The present study retrospectively analyzed 1302 adult patients undergoing overlapping, single-level, posterior-only lumbar fusion within a single, multicenter, academic health system. Recorded outcomes included 30-day emergency department visits, readmission, reoperation, mortality, overall morbidity, and overall morbidity/surgical complications. The amount of overlap was calculated as a percentage of total overlap time. Comparison was made between patients with the most (top 10%) and least (bottom 40%) amount of overlap. Patients were then exact matched on key demographic factors but not by the attending surgeons. Subsequently, patients were exact matched by both demographic data and the attending surgeons. Univariate analysis was first carried out prior to matching and then on both the demographic-matched and surgeon-matched cohorts. Significance for all analyses was set at a P value of <0.05.
Results Within the whole population, increasing duration of overlap was not correlated with any short-term outcome (P = 0.41–0.91). After exact matching, patients with the most and least durations of overlap did not have significant differences with respect to any short-term outcomes (P = 0.34–1.00).
Conclusion Increased amount of overlap is not associated with adverse short-term outcomes for single-level, posterior-only lumbar fusions.
Clinical Relevance The present results suggest that increasing the duration of overlap during lumbar fusion surgery does not lead to inferior outcomes.
Level of Evidence 3.
Introduction
Surgeons often perform cases that can overlap in operating time, a practice known as overlapping surgery. Overlapping surgery came into public attention following a 2015 Boston Globe investigation, leading to increased scrutiny and demands for research evaluating the safety of overlapping surgery.1 In response, the American College of Surgeons updated their guidelines regarding overlapping surgery.2 They stated that concurrent surgery—in which a surgeon simultaneously performs the critical elements of multiple cases—is always inappropriate. In contrast, overlapping surgery—in which a surgeon alternates operating rooms after completing the critical elements of a case, allowing another practitioner to complete the noncritical elements of the case—is acceptable.
Given the recent public concern about patient safety, additional research is warranted to examine the impact of overlap on surgical outcomes.3 Previous literature across multiple surgical services has not demonstrated an increase in morbidity, mortality, or complication rate, despite occasionally finding an increased duration of surgery.4–7 There are similar results for overlap within neurosurgery, with previous studies reporting noninferior outcomes following all neurosurgical procedures,8,9 elective neurosurgical procedures,10 pituitary adenoma resection,11 microvascular decompression,12 and spine surgery.13 Although these reports suggest that surgical overlap is safe, few studies have evaluated whether an increasing amount of overlap during surgery confers additional risk to patients. Previous studies in orthopedic surgery found no association with complication rate and increasing duration of overlap,5,14 but there are a paucity of studies that have evaluated the impact of varying degrees of neurosurgical overlap on short-term outcomes.
Here, we assess increasing duration of surgical overlap on 30-day outcomes in the setting of posterior-only, single-level lumbar fusion. Lumbar fusion is a common neurosurgical procedure that can have complication rates near 13% to 16% in the short-term postoperative period, making it particularly relevant to determine the risk factors for adverse outcomes.15,16 This study utilized coarsened exact matching (CEM) to compare outcomes among patients matched on an increasing number of variables, including demographics and attending surgeon.
Methods
Sample Selection
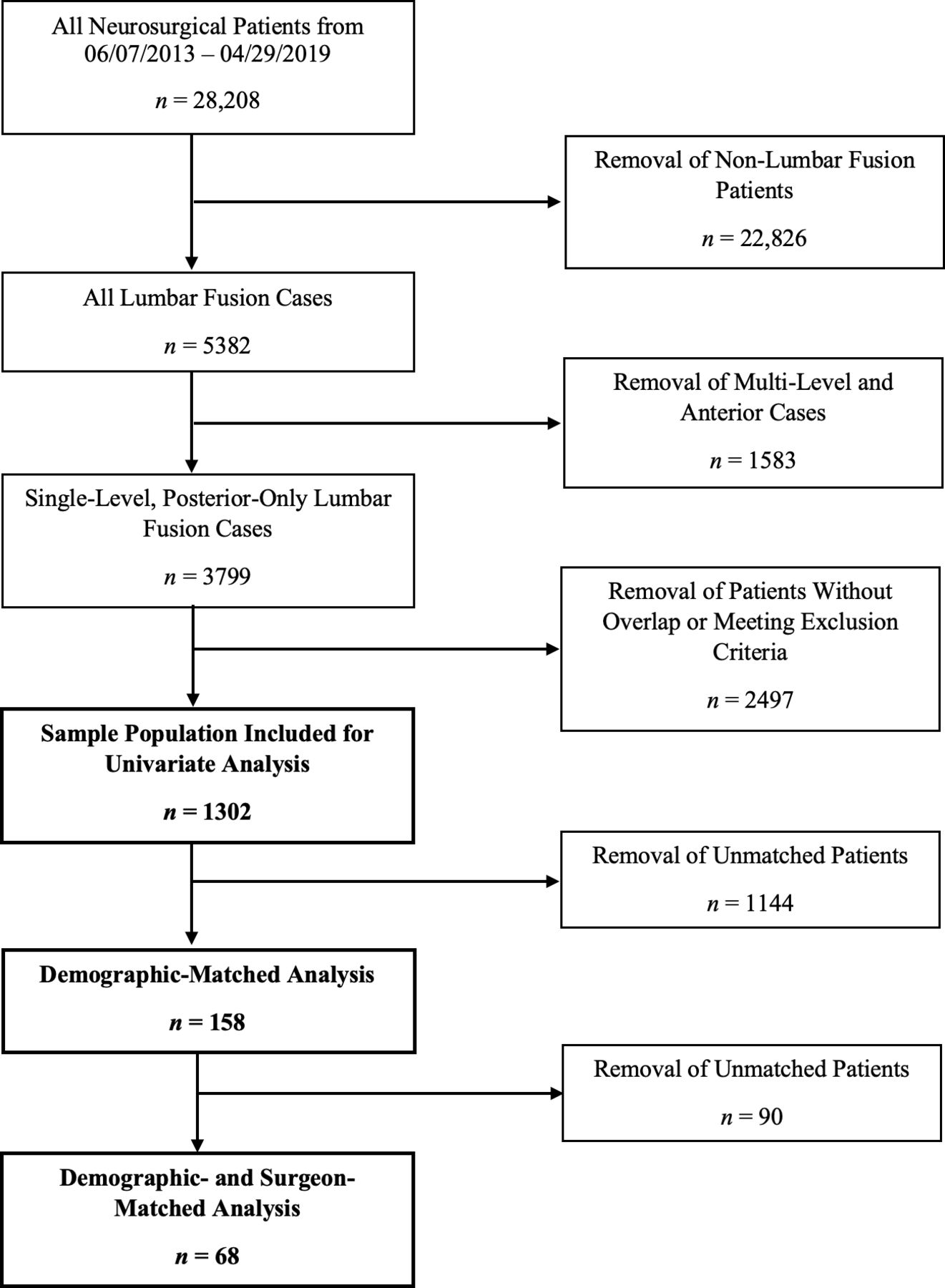
This Institutional Review Board–approved study was considered to pose a minimal risk to patients and was granted a waiver of informed consent. A total of 3799 consecutive patients undergoing single-level, posterior-only lumbar fusion at a single, multihospital, academic health system over a 6-year period (from 07 June 2013 to 29 April 2019) were enrolled retrospectively (Figure 1). Exclusion criteria included patients with missing health information, significantly elevated body mass index (BMI), nonelective/nonroutine operations, nongeneral anesthesia, and unclean wound closure. Key patient characteristic data were acquired via EpiLog—a nonproprietary data acquisition system created by the senior author (N.R.M.) and built within the existing electronic health record for quality improvement initiatives.17
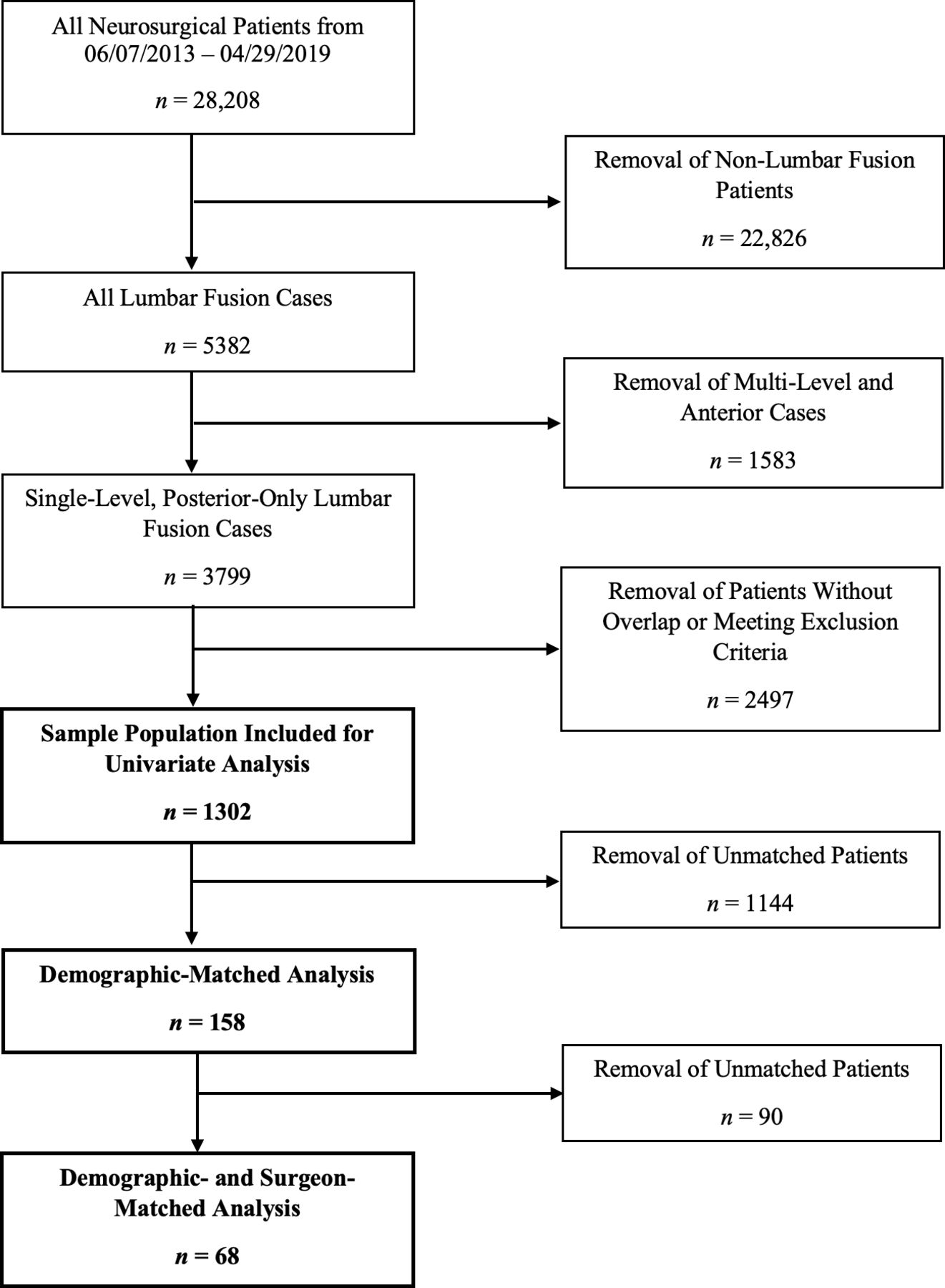
Flowchart of lumbar fusion cases included within the present study.
The whole population for analysis included only patients with overlap during operative time (n = 1302). The amount of surgical overlap for each patient was defined as a percentage of total operative duration. Univariate logistic regression was employed to correlate increasing amount of overlap with short-term patient outcomes, including readmission, reoperation, emergency department visits, mortality, morbidity, and surgical complications. Furthermore, exact-matched patients with the least amount (bottom 40%) and most amount (top 10%) of overlap time were compared.
Data Collection and Matching Process
CEM was performed to account for potentially confounding variables when comparing patients with the least and most amounts of overlap. CEM employs 1:1 matching via the original covariates.18 This contrasts propensity score matching, which converts the covariates into a composite value for matching, otherwise ignoring the original values. Under the present CEM protocol, an exact match was defined as a match on every prespecified covariate.
Patients with the least and most amounts of overlap were exact matched on 27 unique patient characteristics including gender, race, insurance status, median household income, level of education, tobacco use history, BMI, Charlson Comorbidity Index (CCI) score and its underlying components, American Society of Anesthesiologists (ASA) grade, and surgical history. Binary matching was employed for race (white or nonwhite) and median household income (above or below the median value for the dataset). Ternary matching was performed for BMI, CCI, and ASA grade, with patients binned into either a low-, medium-, or high-value cohort. Exact matching was performed for the remaining matching covariates. Unmatched patients were removed from the matched analysis. After matching on demographic data, matches were limited to those with the same operating surgeon.
Statistical Methods
Demographic, clinical, and outcome data were extracted from the electronic health record via EpiLog and placed into defined spreadsheets. Univariate logistic regression was performed using SAS version 9.4 (SAS Institute Inc., Cary, North Carolina) to analyze the duration of overlap as a continuous variable (ie, 1% increase in amount of overlap). For CEM, binning of the matching variables and removal of missing values were performed using SAS version 9.4, whereas matching was completed with the MatchIt programming package in R Statistics (R Core Team, Vienna, Austria, 2017). McNemar test was used to compare means of outcomes between all exact-matched groups. Statistical significance was defined as a P value <0.05 for all analyses.
Results
Patient Characteristics: Before Exact Matching
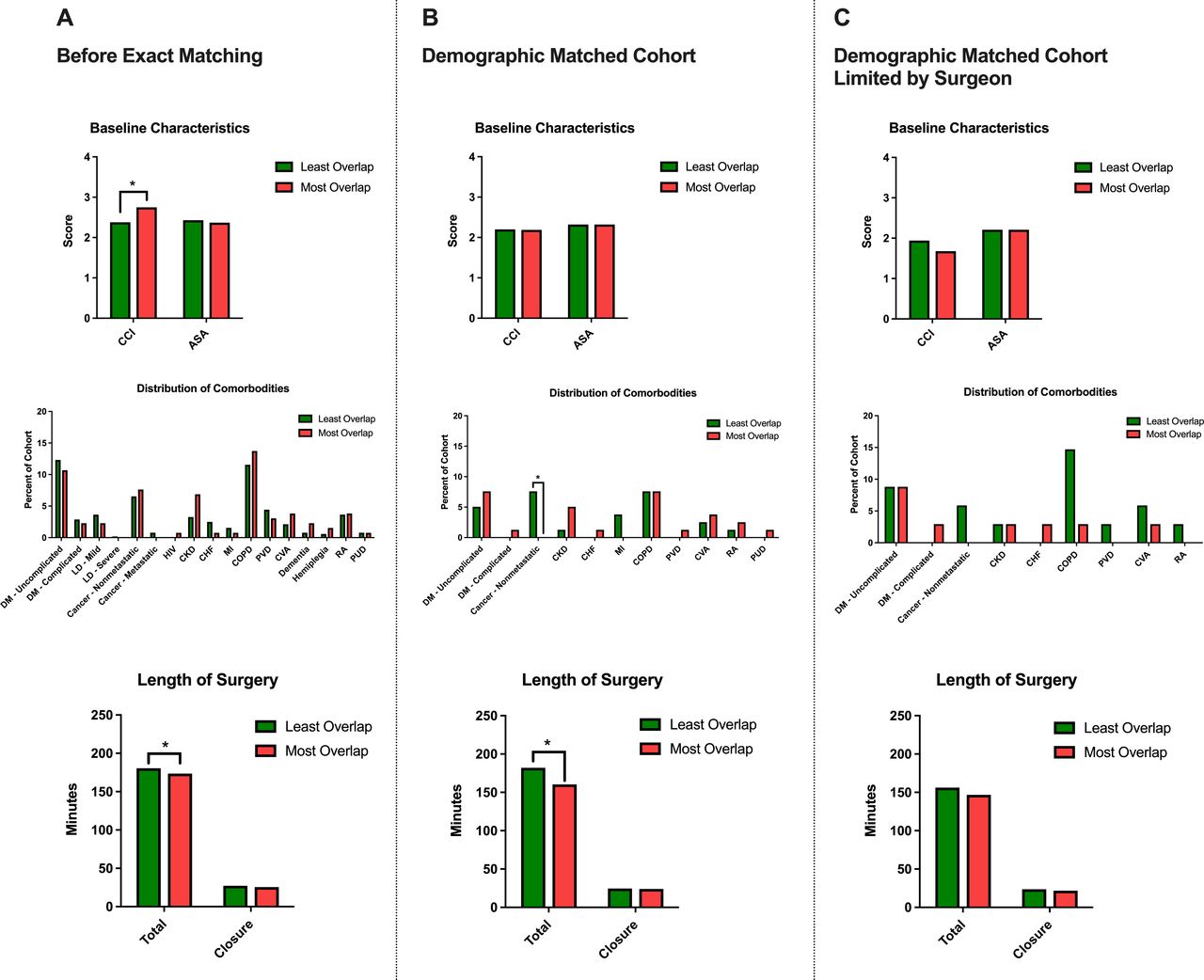
Prior to exact matching, patients with the most surgical overlap demonstrated greater CCI baseline score (P = 0.031), but a comparable distribution of comorbidities, and a similar ASA grade (Figure 2A). No significant difference in surgical history was observed. Patients with the most amount of overlap also had significantly shorter total length of surgery (P = 0.017), but a comparable length of multilayered wound closure. Patients with the most amount of overlap also had significantly shorter length of stay (P = 0.006) and duration of follow-up (P = 0.018), but no difference in the number of non-neurosurgical interventions within 30 days of the index operation (Table 1). Patients with increasing overlap had significantly lower operating room costs (P < 0.001) and differed by the insurance provider (P = 0.017).

Comparison of baseline health characteristics, distribution of comorbidities, and operative time among patients with the most and least amount of surgical overlap. *Significance at P value <0.05. ASA, American Society of Anesthesiologists grade; CCI, Charlson Comorbidity Index score; CHF, congestive heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; DM, diabetes mellitus; HIV, human immunodeficiency virus; LD, liver disease; MI, myocardial infarction; PUD, peptic ulcer disease; PVD, peripheral vascular disease; RA, rheumatoid arthritis.
Characteristics of patients whose surgeries had the least amount of overlap (bottom 40% of patients with overlapping surgeries) and the most amount of overlap (top 10% of patients with overlapping surgeries).
Patient Characteristics: Demographic-Matched Cohort
Patients were exact matched on demographic variables but not limited to the same operating surgeon (n = 158). Matched cohorts demonstrated similar CCI score and ASA grade and a similar distribution of comorbidities, but patients with the most surgical overlap had significantly lower rates of nonmetastatic cancer (P = 0.028) (Figure 2B). No significant difference in surgical history was observed. Patients with the most amount of overlap had a shorter total length of surgery (P = 0.018), but not the length of multilayered wound closure. No difference was observed in duration of follow-up, but patients with the most overlap were observed to have significantly shorter lengths of stay (P = 0.001) (Table 2). There was no difference in the insurance provider, but patients with more overlap had a lower operating room cost (P < 0.001).
Characteristics of the subset of patients with the least amount of overlap (bottom 40% of patients with overlap) and the most amount of overlap (top 10% of patients with overlap), subsequently matched on demographic variables but not the operating surgeon.
Patient Characteristics: Demographic-Matched Cohort Limited by Surgeon
After exact matching on demographics, matches were limited to those with the same operating surgeon (n = 68). No significant differences were observed in CCI score, distribution of comorbidities, ASA grade, and surgical history. Furthermore, there was no difference in length of surgery or length of multilayered wound closure (Figure 2C). Finally, no significant differences were observed in the duration of follow-up, length of stay, insurance type, or cost of surgery (Table 3).
Characteristics of the subset of patients with the least amount of overlap (bottom 40% of patients with overlap) and the most amount of overlap (top 10% of patients with overlap), subsequently matched on both demographic variables and limited to the same operating surgeon.
Patient Outcomes: Whole Population
Within the whole population, increasing duration of overlap was not correlated with any morbidity or mortality outcome, including 30-day readmission, reoperation, emergency department visits, or mortality (P = 0.41–0.91). When evaluating overall morbidity or overall morbidity including surgical complications, there was also no significant correlation (P = 0.70–0.78) (Table 4).
Short-term outcome data analyzing the impact of increasing duration of overlap as a continuous variable. Exact-matched patients with the most amount of overlap (top 10%) and least amount of overlap (bottom 40%) were also compared.
Outcomes in Demographic-Matched Cohort
After exact matching patients with the most overlap to those with the least overlap after on demographics, but not by the surgeon, there was no difference in any 30-day adverse outcome, overall morbidity, or overall morbidity/surgical complications (P = 0.38–1.00). There was no 30-day mortality recorded in this exact-matched cohort (Figure 3, Table 4).
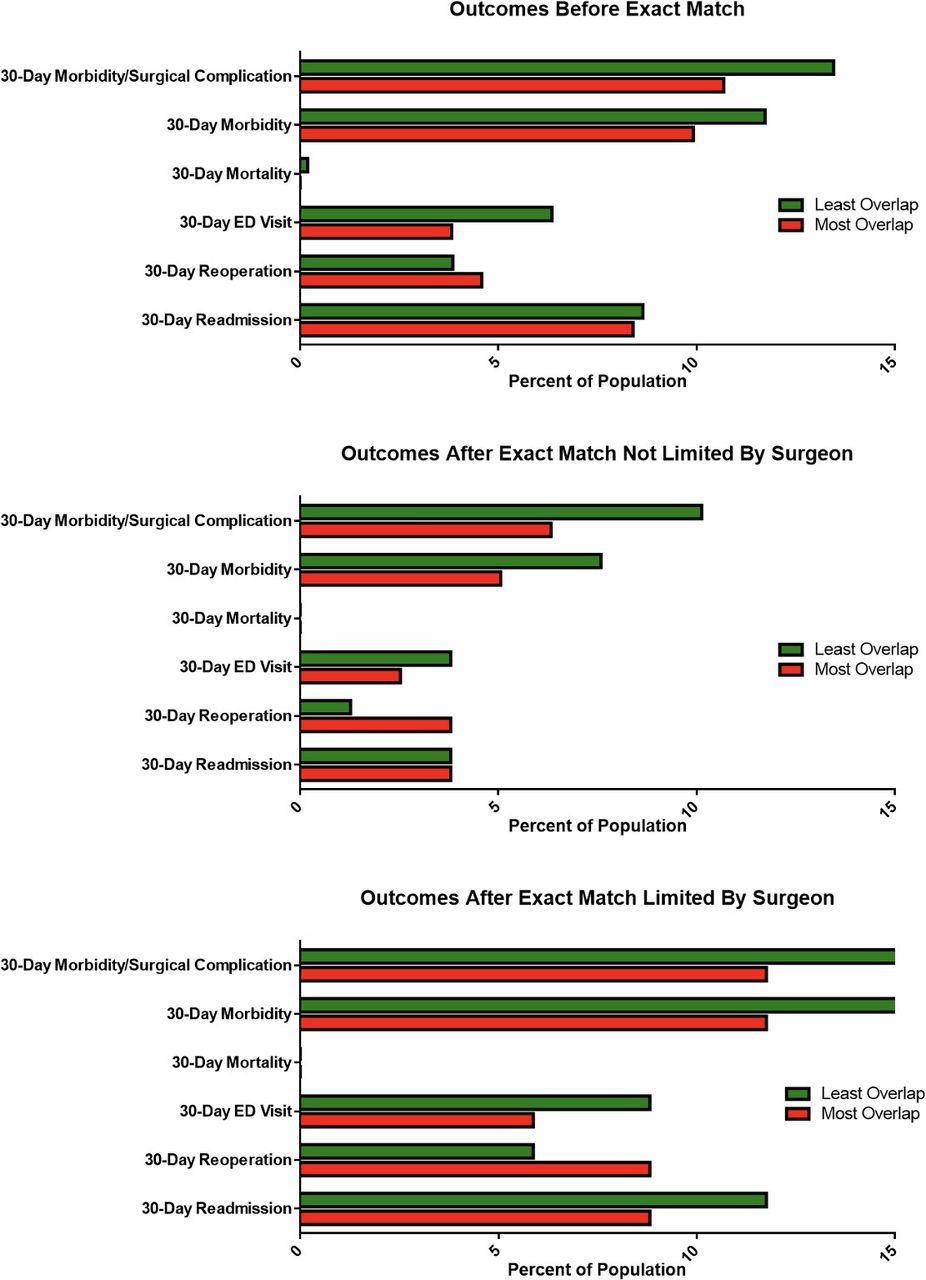
Distribution of short-term outcomes following single-level, posterior lumbar fusion. No differences were observed in any morbidity or mortality outcomes between exact matched cohorts. ED, emergency department.
Outcomes in Demographic-Matched Cohort Limited by Surgeon
After exact matching cohorts on both demographics and limiting to the same operating surgeon, there was no significant difference in any 30-day adverse outcome, overall morbidity, or overall morbidity/surgical complications (P = 0.34–0.69). No 30-day mortality events were recorded in this exact-matched cohort (Figure 3, Table 4).
Discussion
Increasing duration of overlap, in the setting studied, does not lead to adverse short-term outcomes following single-level, posterior-only lumbar fusion. Duration of overlap was not correlated with any short-term patient outcome in the whole population. When comparing demographic exact-matched cohorts with the least and most amounts of overlap, there were no significant differences in any short-term morbidity outcome. Comparison of exact-matched cohorts yielded the same results, when matching was further limited by the surgeon performing the operation.
There is a paucity of research on the impact of increasing overlap duration on neurosurgical outcomes. Previous studies in orthopedic surgery have not demonstrated any association between duration of overlap and adverse 30- or 90-day patient outcomes.5,14 Our results supplement these findings by demonstrating that an increasing amount of overlap time during lumbar fusion does not lead to an increased risk of 30-day complications when controlling for patient demographic variables and surgeon variability. Future studies should examine increasing overlap time, longer-term outcomes, and outcomes following other procedures to thoroughly assess the safety of increasing overlap time in neurosurgery.
Previous studies have found that individuals selected for overlapping surgery are typically healthier at baseline and have lower CCI score, fewer comorbidities, and lower ASA grade.10,19 However, this study found that patients with the most overlap had similar CCI score, similar distribution of comorbidities, a higher ASA grade as compared with patients with the least overlap. This difference suggests that, although surgeons typically select healthier patients as candidates for overlapping surgery, it is not always the case.
Previous studies within neurosurgery found that patients with overlap typically had a longer length of surgery as compared with patients without overlap, but no additional risk of adverse outcomes.8–13 Here, among the whole population and the cohort exact matched on key patient characteristics, patients with the most amount of overlap were observed to have shorter total length of surgery; these results disappeared after controlling for the attending surgeon, potentially suggesting that the supervising surgeon drives operative time, rather than the amount of overlap time for any given patient. This contrasts prior work by George et al,14 which found that patients with a greater surgical overlap had a longer length of surgery during total joint arthroplasty. This difference in results may be due to variability in risk and complexity between the procedures studied, which further highlight the importance of evaluating the impact of overlap duration in a procedure-specific manner.
Limitations
This study was retrospective and is therefore susceptible to sampling biases. Furthermore, all patient health care encounters were recorded within the university-wide electronic health record; therefore, patient encounters that occurred at outside health system may not have been captured, leading to potential under-reporting of morbidity outcomes. This limitation was mitigated by an extensive mean duration of follow-up (38.2 and 43.6 months, for patients with the most and least overlap, respectively). During each follow-up visit, all external health care encounters were asked and recorded. Furthermore, any potential under-reporting of adverse events would be expected to equally affect patients with the most and least amounts of overlap, preserving the internal validity of this study.
While certain demographic and clinical variables were excluded from our CEM protocol, the matching variables used herein were carefully selected from the surgical literature. Race,20–24 smoking status,25 BMI,26,27 CCI,28–30 duration of surgery,31,32 and ASA score33 have all been demonstrated to independently impact postoperative morbidity. By controlling these variables via CEM, we expect to ensure the overall validity of the study findings.
The present analysis used a decile-based matching protocol, which has previously been employed by the present authors.34–37 This approach allowed analysis of the extremes of overlap duration, while ensuring an adequate population sample assessment via exact matching. CEM resulted in 158 patients included in the matched analysis, with a match rate 60.3% among the most overlap cohort. Relative to other matching protocols, CEM includes fewer patients for analysis, but offers more precise control of confounding variables, resulting in enhanced focus on the impact of surgical overlap in 1-level spinal fusion surgery.38
This study examined only single-level, posterior lumbar fusions, enhancing the internal validity of the results at the expense of generalizability. That said, among lumbar fusions, single-level instrumented fusions are the most frequently performed procedure. Furthermore, the differing number of levels of disease presents in different manners, which has implications for results and complications and thus was thought to be too heterogeneous for the intense focus on overlap undertaken herein.39 Additional studies are needed to corroborate these findings across other spinal procedures.
Conclusion
In the presence of overlapping surgery, increasing duration of overlap during lumbar fusion does not lead to adverse short-term patient outcomes. When comparing exact-matched patients with the least and most amounts of overlap time, no significant differences were found in any specific morbidity outcome or overall morbidity. Further studies should evaluate longer-term patient outcomes among patients with increased amounts of overlap during lumbar fusion and other neurosurgical procedures.
Acknowledgments
The EpiLog Project.
Footnotes
Funding N.R.M. received support from the Kevin and Bernadette McKenna Family Research Fund.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Committee Approval This study was approved by the IRB at the University of Pennsylvania. IRB number for this study is: 831423. A waiver of informed consent was granted by the University of Pennsylvania IRB as this study was considered to be minimal risk to patients. All ethical guidelines and rules were followed to protect patient privacy
Contributorship Statement Conception and design: N.R.M. and A.S.F. Acquisition of data: N.R.M. and A.S.F. Analysis and interpretation of data: A.S.F., K.S., S.D.M., and N.R.M. Drafting the article: A.S.F., D.K.E.D.D., G.G., A.J.B., and N.R.M. Critically revising the article: A.S.F., D.K.E.D.D., G.G., A.J.B., K.S., S.D.M., and N.R.M. Approved the final version of the manuscript on behalf of all authors: A.S.F., D.K.E.D.D., G.G., A.J.B., K.S., S.D.M., and N.R.M. Administrative/technical/material support: D.K.E.D.D., G.G., A.J.B., N.R.M. Study supervision: N.R.M.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.