


Abstract
Background Posterior lumbar fusions are a common and successful procedure, yet surgical site infection (SSI) is still prevalent and causes significant morbidity. Obesity is a well-established risk factor for SSI. Still, the accuracy of the body mass index (BMI) caused some to suggest other metrics that are more representative of the thickness of the soft-tissue envelope in the surgical site.
Methods A retrospective review of all cases that developed SSI following posterior lumbar fusion over the past 5 years was done. An age and gender-matched control group was formed from the lumbar fusion cases that did not develop SSI. Demographic and clinical data were collected, and morphometric measurements of the soft-tissue envelope were performed at the level of L4 for all cases on standing x-ray imaging and magnetic resonance imaging (MRI).
Results A total of 366 patients underwent posterior lumbar fusion, 26 of whom developed SSI. BMI and skin to spinous process measurements on x-ray imaging—not MRI—were found to be significantly associated with SSI. Regression analysis further confirmed the strength of the association.
Conclusion While BMI and MRI measurements are useful, wound depth measurements on x-ray imaging can be predictive of SSI in lumbar fusion cases.
Clinical Relevace Wound depth measurements are predictive of lumbar wound infection. The information within this study can help surgeons better predict and manage infections of posterior lumbar wounds.
Level of Evidence 3.
Introduction
Surgical site infection (SSI) is a global issue, placing a significant burden on the health care systems of all countries.1 SSI following instrumented spine surgery is prevalent, with rates from 2% to over 20% in the current literature.2–5 It is the most common complication after elective spine surgery in most series and is responsible for a significant number of readmissions and reoperations.6–8 The morbidity and increased cost are substantial, up to 4 times the cost of an uninfected patient.9–11 Multiple risk factors have been associated with SSI following instrumented spine surgery. Smoking, diabetes mellitus (DM), increased blood loss, the number of levels fused, prolonged operative time, and obesity have all been implicated.12 Obesity is a global pandemic, rising in prevalence at an alarming rate.13 The association of obesity with worse outcomes in spine surgery has been reported on extensively.14–19 A significant portion of the morbidity comes from its proven status as a risk factor for SSI in spine surgery.14,15,17,20 Body mass index (BMI) alone is helpful, but studies have looked at the lumbar wound soft-tissue envelope thickness as a more accurate predictor of SSI.21–24 The correlation was found but was also disputed.25 All these studies have taken measurements from magnetic resonance imaging (MRI) or computed tomography in the standard, supine position. We have had concerns that these measurements are not very accurate, as it is well established that supine MRI can underestimate the findings as compared with standing MRI.26,27 Standing MRI scanners are not widely available, yet a standing radiograph is universally available and can provide the “skin to spinous process (SP)” measurement needed with accuracy and ease for all cases. In this study, we aim to take the erect lumbar radiograph measurements from cases of lumbar SSI and compare them to a control group. We hypothesize that standing lumbar radiographs are a more accurate measure of the subcutaneous layer thickness and a better predictor of postoperative lumbar SSI than MRI measurement.
Materials and Methods
All adult patients who underwent primary instrumented posterior lumbar spine fusion surgery in the past 5 years in our institution (from January 2015 to December 2020) were included in the primary review. The surgeries were done by 4 spine surgeons. An institutional SSI prevention protocol has been in place since 2012. It includes evidence-based antibiotic prophylaxis and wound care measures. These wound care measures included the release of retractors on an hourly basis, debridement of any necrotic tissue at the end of the procedure, soaking with a diluted (0.3%) povidone-iodine solution for 30 seconds, followed by irrigation with a standard 2 L of warmed normal saline. An amount of 1 g of vancomycin powder was added to the deep layer prior to closure. Wound closure was done using interrupted sutures for the deep facial layer and continuous sutures for the subcutaneous and skin layers.
Patients’ who developed SSI were defined as those who underwent either reoperation or readmission within 30 days of the initial surgery for infection and had positive tissue cultures proving the diagnosis. Datapoints to be collected included demographics, BMI, number of levels fused, estimated blood loss, length of anesthesia, glycemic control, use of drains, skin to SP on standing x-ray imaging, skin to SP on sagittal MRI, skin to SP on axial MRI, and skin to lamina on axial MRI. X-ray imaging was performed using a standard technique, with the elbows flexed and hands on the clavicles. All the measurements were taken at the level of L4 (Figure 1) using the standard imaging viewer software. An orthopedic spine surgeon (AA) took all the measurements and repeated them twice, 1 month apart. Intraobserver reliability using the kappa statistic was performed, and the data found to be very reliable. The means of measurements were used for the final analysis. Any patients who lacked any datapoints were excluded from the study cohort. Patients who underwent surgery for infection or neoplasia were also excluded. An age and sex-matched control group was chosen randomly from the cases that did not develop SSI. The research ethics board approval was obtained (21/5777/IRB [institutional review board]) prior to the collection of the data. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki declaration of 1975, as revised in 2000. The t test and the Mann-Whitney U test were used for continuous variables, whereas the χ 2 test was used for categorical variables. When a significant association was found, binary logistic regression was utilized to determine the strength of the correlation. A P value of less than 0.05 was used to assess significance. All analyses were performed using SPSS version 27 software (IBM Corp, Armonk, NY, USA).

Skin to spinous process measurements at L4 on x-ray imaging and magnetic resonance imaging.
Results
A total of 366 patients were included in the primary data collection, of whom 26 (7.1%) developed SSI as per the study definition. The cases were evenly distributed among the 4 surgeons. The demographic and clinical data are presented in Table 1, which shows the control group was well matched to the study group for age and sex. All the patients’ cultures were positive for Staphylococcus aureus except for 2 patients: one was positive for Pseudomonas aeruginosa, and the other was infected with methicillin-resistant S aureus.
Demographics and clinical data (N = 366).
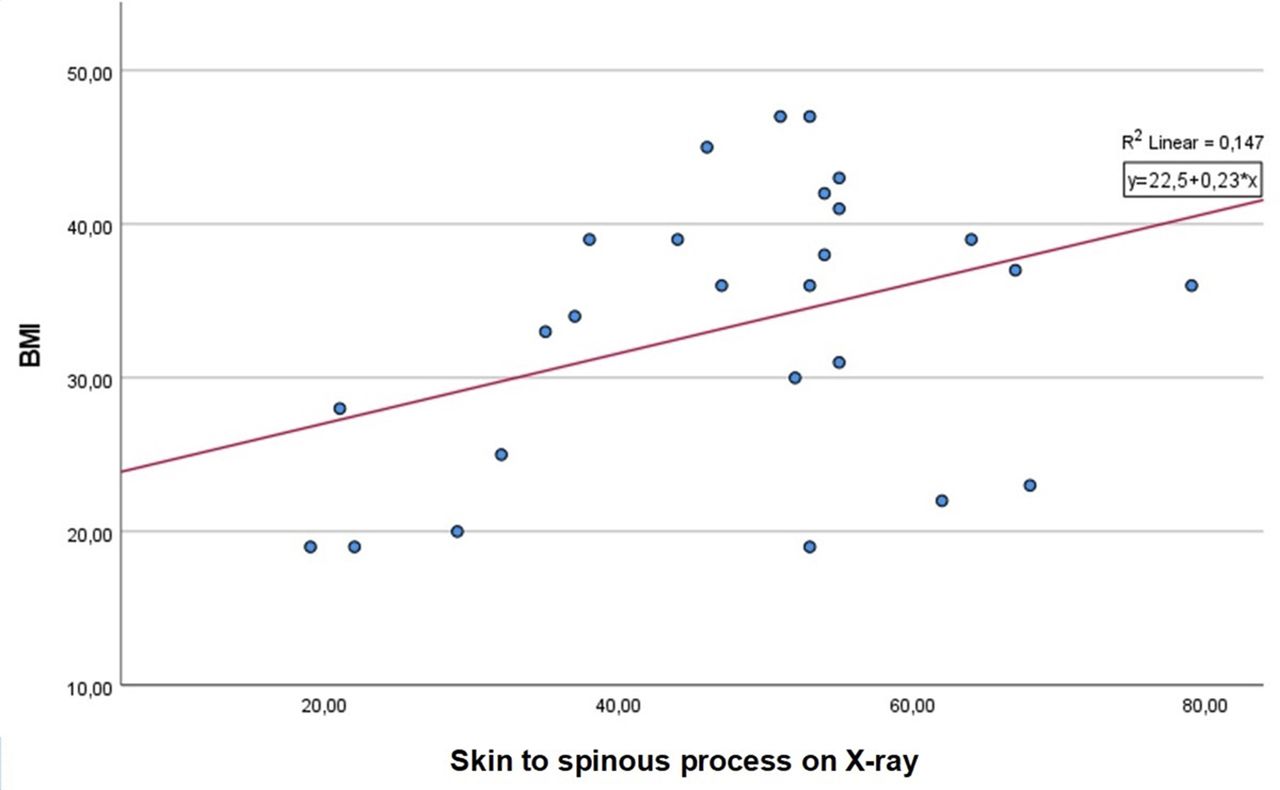
BMI was found to be significantly associated with SSI (P = 0.049). The average infected case was obese, while the average noninfected case was overweight (33 vs 29). A linear relation between BMI and skin to SP on x-ray imaging was found with an increase of 0.23 mm with each unit increase in BMI (Helsinki) (Figure 2).

Scatter plot showing linear relationship between BMI and “skin to spinous process” measurements. BMI, body mass index.
The skin to SP measurement was also found to be significantly associated with SSI (P = 0.017). A difference of 10 mm was found between the 2 groups, while MRI measurements showed only an 8.5 mm difference on the sagittal views, going down to 5 mm in the axial cuts. Multivariate regression is displayed in Table 2. The odds of SSI were higher with a higher BMI, thicker fat envelope on sagittal x-ray imaging and sagittal MRI. When the cases were divided into quartiles based on the skin to SP measurements, the patients with thickness above the 50% mark (44.5 mm) had a 6-fold increase in the odds of SSI (OR = 6.112, 95% CI = 1.479–25.259) compared with those less than 44.5 mm (P = 0.012).
Multiple regression analysis of risk factors for surgical site infection.
Discussion
The rates of postoperative infection following instrumented thoracolumbar spine surgery have been reported to be 4.4% to 13% in a recent systematic review.28 The rate in this series is within that range but higher than the average of other series.2,4,5 The factors identified in the literature as risk factors for SSI following spine surgery are many, so much so that a web-based calculator has been designed to predict the risk.29 DM has been identified by many as a risk factor.7,30 In our study, it did not correlate with the risk of SSI. The explanation might be that our perioperative protocols exclude patients with uncontrolled diabetes from having elective spine surgery. Others have reported that controlled DM should have no impact on the incidence of complications following spine surgery.31,32 Multiple operative factors have been implicated as risk factors for spinal SSI. Operative time, the number of levels fused, intraoperative blood loss, and the use of drains are commonly investigated.33–36 In this study, these factors were not associated with the development of SSI.
Obesity—commonly measured using BMI—is a well-established risk factor for spinal SSI.14,16,19,37,38 A recent meta-analysis found it to be responsible for worse clinical outcomes and higher complication rates—notably thromboembolic events and SSI.18 The correlation in this study is robust and confirms the findings of other studies. The concern that BMI might not be the best indicator of wound complications stems from being a general assessment that doesn’t consider fat distribution throughout the body. The subcutaneous layer is subjected to retraction during the procedure. Given its limited vascularity, this could result in tissue ischemia and fat necrosis.39–41 The thicker the subcutaneous layer is, the more dead space will result and infection could follow.42
The first study to report on linear wound measurements—specifically skin to lamina and fat layer thickness—was by Mehta et al.21 The series of 24 patients who developed SSI were compared to an unmatched control group. While BMI was not correlated with SSI, obesity (BMI >30 kg/m2) was significantly associated with SSI. As for the wound measurements, Mehta et al reported on the skin to lamina, fat, and muscle layer thickness. The fat layer thickness was significantly predictive of SSI (OR = 1.037, 95% CI = 1.007–1.068), and the muscle layer thickness was not. Lee et al published a similar case-control study, again noting that obesity is a significant risk factor. Still, it was the subcutaneous fat thickness that was strongly predictive of SSI with an OR of 1.06 (95% CI = 1.02–1.10) on regression analysis. Two more studies were published in the past year having similar objectives to Mehta et al and Lee et al and arriving at similar conclusions.22,24 In the aforementioned studies, measurements were taken from MRI or CT. Most took the measurements from the skin to the SP, while some added “skin to lamina.” The measurement from the skin to the SP was more correlated with SSI in these studies than the “fat layer thickness” that can only be evaluated on MRI.21,24,43 As such, it was used as the primary measurement in our study albeit from erect radiographs rather than MRI or CT. Our results confirm the findings of the previous studies.
Our study was limited by its retrospective design and its small sample size. Nevertheless, our results confirm the association of SSI with a higher BMI and a thicker soft-tissue envelope. Future larger, prospective studies that add more risk factors to the analysis are needed.
Conclusion
This study describes a simple and readily available measurement that can serve as a predictor of SSI following lumbar spine fusion surgery.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest or financial disclosures with respect to the research, authorship, and/or publication of this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.