


Abstract
Background Preoperative neutrophil-lymphocyte ratio (NLR) has been described in various fields to predict pain outcomes, but its prognostic utility for pain/functional outcomes after spine surgery is unclear.
Objective To determine the relationship between preoperative NLR and pain/functional outcomes at 12 months after lumbar fusion.
Methods We performed a single-center retrospective study of 53 patients who underwent lumbar fusion and collected demographic data including age, sex, body mass index, smoking status, spinal levels operated, and preoperative NLR. Visual analog scale (VAS) for back and leg pain and Oswestry Disability Index (ODI) at baseline and 12 months after lumbar fusion were also collected. The outcome measures were the occurrence of a clinically important improvement in VAS and ODI scores at 12 months. Binary logistic regression was used to estimate the associations of demographic factors and NLR with improvement in VAS and ODI scores. A P value of <0.05 was considered statistically significant.
Results There were no statistically significant associations between preoperative NLR and improvement in VAS or ODI scores. A unit increase in baseline VAS back pain score was associated with a 56% increase in the odds of improvement in back pain (OR: 1.56, 95% CI: 1.04–2.35, P = 0.03). Compared to male patients, female patients had 12 times greater odds of an improvement in leg pain (OR: 12.0, 95% CI: 1.3–110, P = 0.03).
Conclusion Preoperative NLR does not predict patient-reported pain/functional outcomes at 12 months after lumbar fusion. Large-scale prospective multicenter studies are warranted to confirm our findings.
Introduction
Back pain and leg pain caused by lumbar spine conditions are the leading causes of disability and low quality of life worldwide.1 Lumbar fusion, a commonly performed procedure for various degenerative pathologies, has been shown to significantly improve pain and functional outcomes in some patients.2,3 However, the procedure is associated with perioperative complications (incidence: 1.4%–57%) that are associated with increased morbidity and mortality.2,4–6 Hence, only patients who would benefit from lumbar fusion should be selected for the procedure.
Pain occurs secondary to inflammation and the inflammatory response.7 Neutrophil-lymphocyte ratio (NLR), a marker of subclinical inflammation, is believed to be a useful predictor of postoperative pain caused by inflammation secondary to surgical trauma. It is believed that a greater preoperative level of inflammation would correlate to postoperative pain and hence functional outcomes. NLR has been utilized as a prognostic marker of pain outcomes in arthroscopy, orthognathic surgery, and general surgery.8–10 However, the relationship between NLR and pain or functional outcomes following lumbar spine surgery is unclear. Our study aims to investigate whether NLR measured preoperatively is associated with improvement in pain and functional status reported by patients at 12 months after lumbar fusion.
Methods
Study Design
We carried out a retrospective observational study to investigate the relationship between improvement in pain/functional status and preoperative NLR in patients who underwent lumbar fusion. We included consecutive adult patients who underwent 1- or 2-level posterior or posterolateral lumbar fusion performed by the same surgeon in a UK regional neurosurgery center between October 2012 and September 2019. The exclusion criteria were previous lumbar spine surgery, a missing record of preoperative full blood count, a missing record of baseline visual analog scale (VAS) and Oswestry Disability Index (ODI) scores, and a missing record of VAS and ODI scores at 12 months. The pain management protocol at our neurosurgery unit was utilized consistently for all patients. Each patient received intraoperative local anesthetic wound infiltration, postoperative morphine patient-controlled analgesia for 1–2 days, and avoidance of nonsteroidal anti-inflammatory drugs in the postoperative period.
For each patient, the preoperative NLR was obtained from the neutrophil count and lymphocyte count recorded in their preoperative full blood count (NLR = neutrophil count divided by lymphocyte count). The demographic/surgical factors assessed included age, sex, smoking status (smoker or nonsmoker), body mass index (BMI), Charlson comorbidity index, and the number of spinal levels operated. VAS for back pain and leg pain, and ODI at baseline and 12 months postoperatively were collected. From the literature, the follow-up period of 12 months is sufficient to adequately assess the therapeutic effect of surgery, as spine surgery patients reach a recovery plateau at 3 and 12 months for pain and functional outcomes respectively.11
The threshold for a clinically important outcome in VAS and ODI scores was determined from the literature. The cut-offs for a clinically important improvement at 12 months are ≥33% for VAS back pain, ≥40% for VAS leg pain, and ≥30% for ODI.12 The outcome measures were (a) ≥33% improvement in back pain (yes or no); (b) ≥40% improvement in leg pain (yes or no); and (c) ≥30% improvement in functional status (ODI) (yes or no).
Statistical Analysis
Statistical analysis was performed using the IBM SPSS Statistics 26 (Windows) software. Pairwise deletion was utilized to deal with missing data. Descriptive statistics were presented as median and interquartile range (IQR) for continuous variables and absolute count for categorical variables. Binary logistic regression was used to evaluate the association between improvement in pain/functional status at follow-up and the independent variables including demographic/surgical factors and preoperative NLR. Spearman rank test was used to evaluate the association between preoperative NLR and baseline VAS and ODI scores. A P value of <0.05 was considered statistically significant at 95% CI.
Results
Case Series Characteristics
Seventy-eight patients met the inclusion criteria, but one patient was excluded due to having previous lumbar spine surgery. Six patients lacked a record of preoperative full blood count. The baseline VAS and ODI scores were missing for 9 patients, while a further 9 patients did not have a record of VAS or ODI scores at 12 months after lumbar fusion. Thus, 53 patients were included in our final analysis.
There were 31 (58%) female and 22 (42%) male patients. The median age of the patients was 52 (IQR = 19) years, and the median BMI was 29.7 (IQR = 6.1) kg/m2. The median Charlson Comorbidity Index was 1 (IQR = 2). The median preoperative VAS back pain score and VAS leg pain score were 8 (IQR = 2) and 8 (IQR = 3), respectively. The median preoperative ODI score was 56 (IQR = 26). Spondylolisthesis (46 cases) was the most common indication for surgery. The baseline demographic/surgical data are summarized in Table 1. The collected raw data of demographics, operative factors, preoperative NLR, VAS, and ODI scores are presented in Supplemental Material 1.
Baseline demographic/surgical data.
Supplemental Material 1.
At 12 months after lumbar fusion, 39 out of 50 (78%) patients showed ≥33% improvement in back pain, 42 out of 49 patients (86%) showed ≥40% improvement in leg pain, while 38 out of 53 patients (72%) showed ≥30% improvement in their functional status.
Association Between Demographic/Surgical Factors, Preoperative NLR, and Pain/Functional Outcomes
Association Between Preoperative NLR and Baseline VAS and ODI Scores
There were no statistically significant associations between preoperative NLR and VAS back pain (r = 0.01, P = 0.93), VAS leg pain (r = 0.11, P = 0.45), and ODI score (r = −0.15, P = 0.27) at baseline.
≥33% Improvement in Back Pain
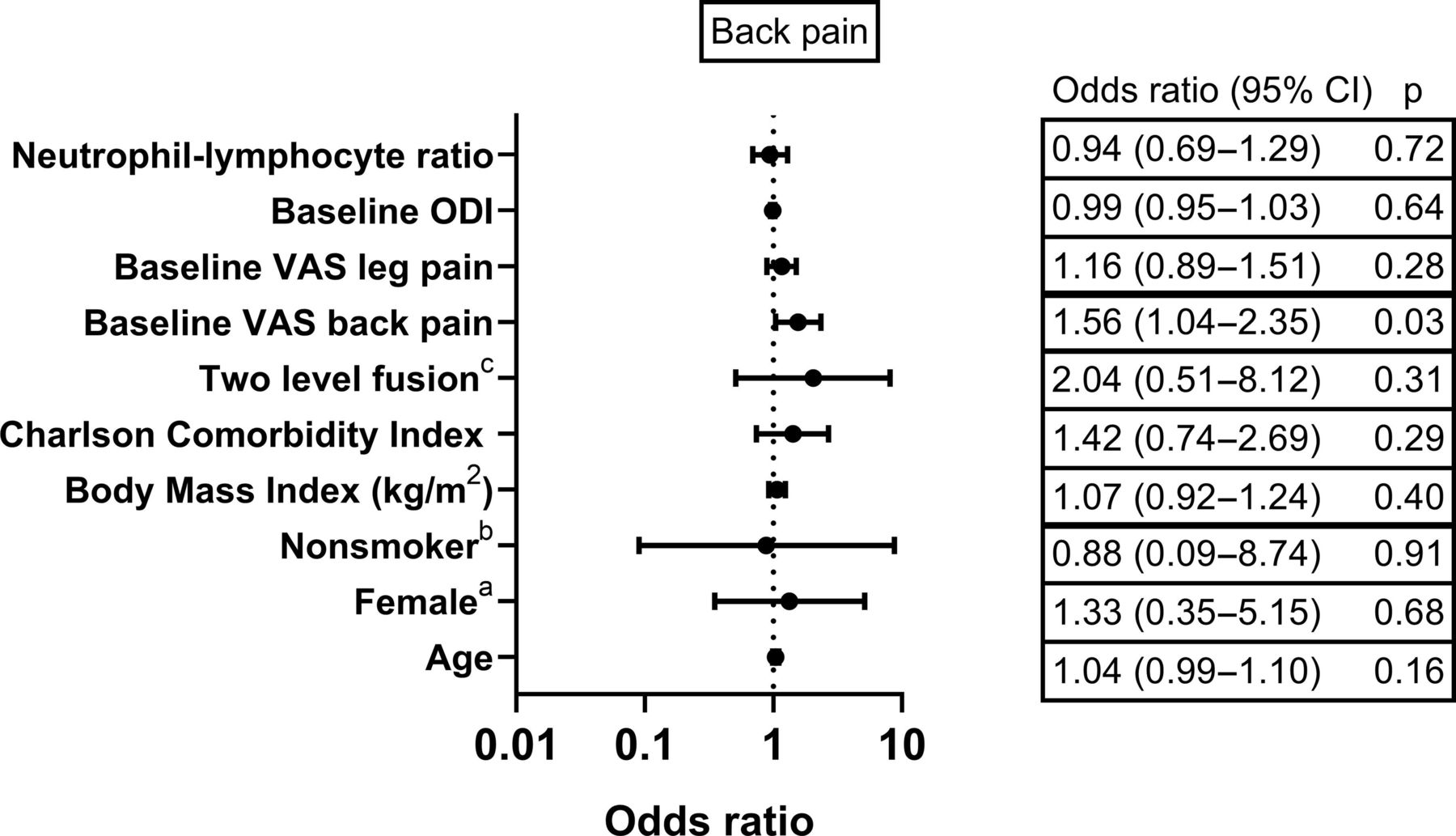
A unit increase in baseline VAS back pain score was associated with a 56% increase in the odds of ≥33% improvement in back pain at 12 months (OR: 1.56, 95% CI: 1.04–2.35, P = 0.03). There were no other statistically significant associations between the demographic/surgical factors, preoperative NLR, and improvement in back pain severity at 12 months (Figure 1).
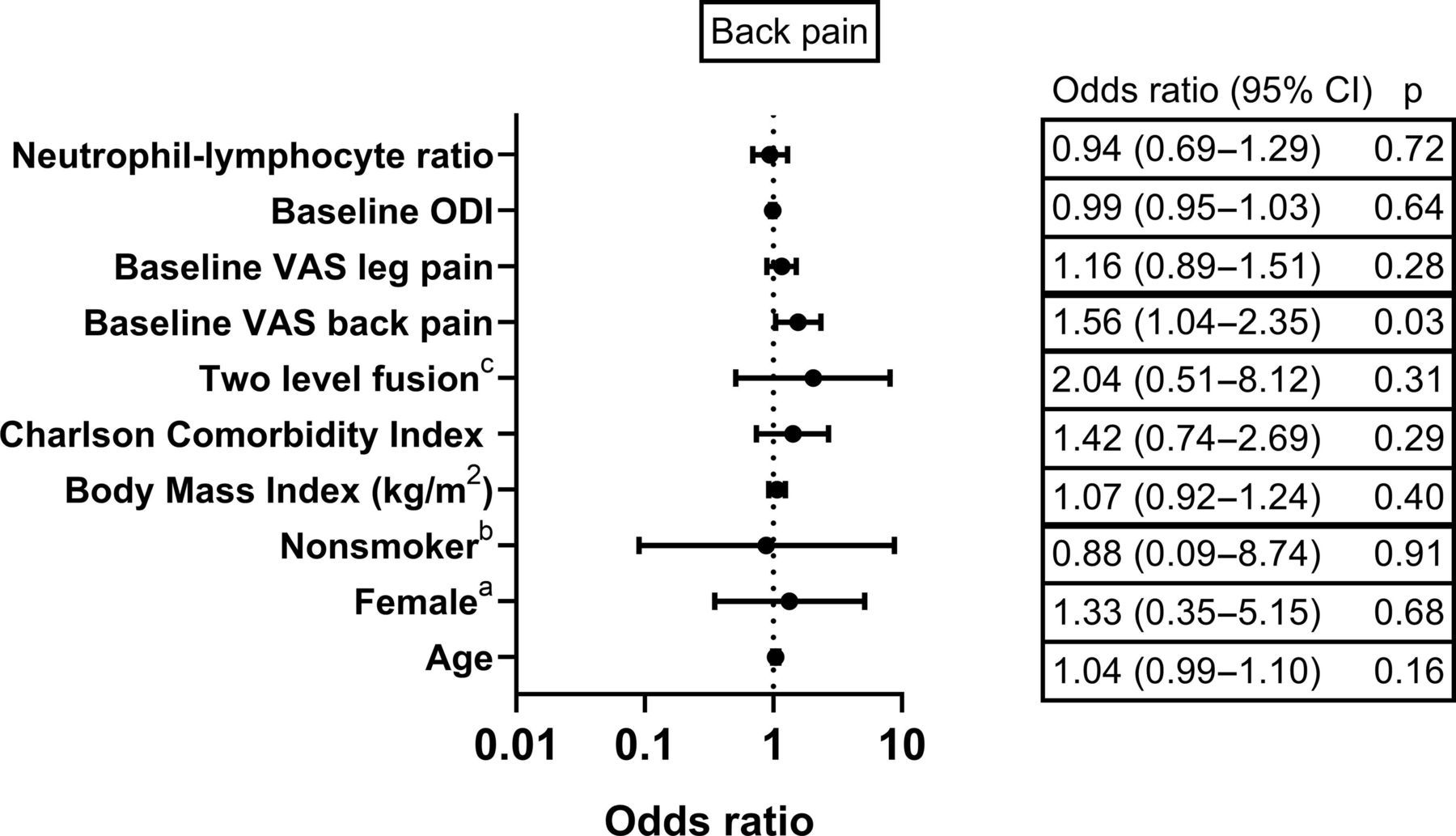
OR with 95% CI for ≥33% improvement in back pain according to demographic/surgical factors and preoperative neutrophil-lymphocyte ratio (NLR). aCompared to men, bcompared to smokers, and ccompared to single-level fusion. ODI, Oswestry Disability Index; VAS, visual analog scale.
≥40% Improvement in Leg Pain
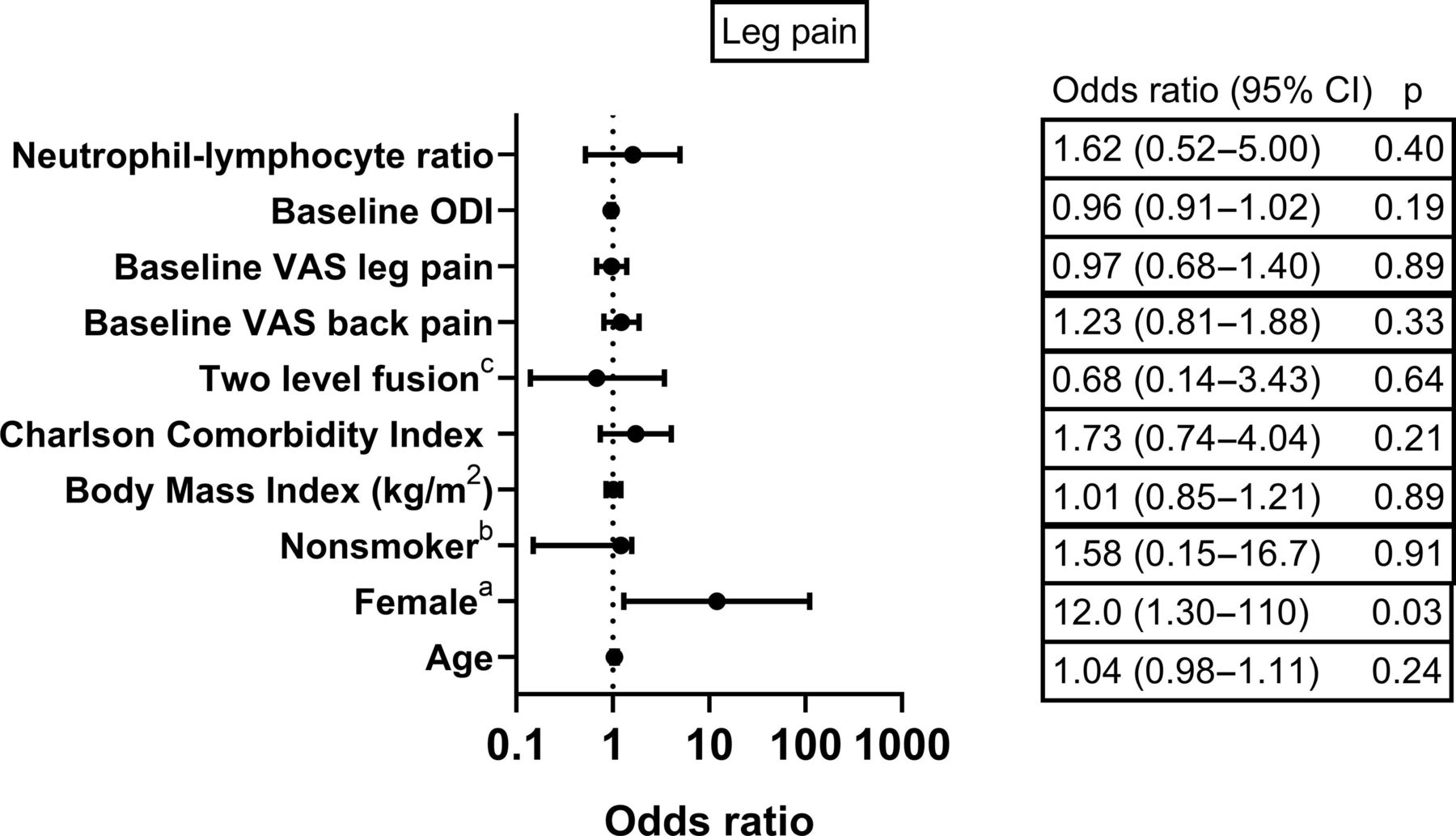
Compared to male patients, female patients have 12 times greater odds of ≥40% improvement in leg pain at 12 months (OR: 12.0, 95% CI: 1.3–110, P = 0.03). There were no other statistically significant associations between the demographic/surgical factors, preoperative NLR, and improvement in leg pain severity at 12 months (Figure 2).
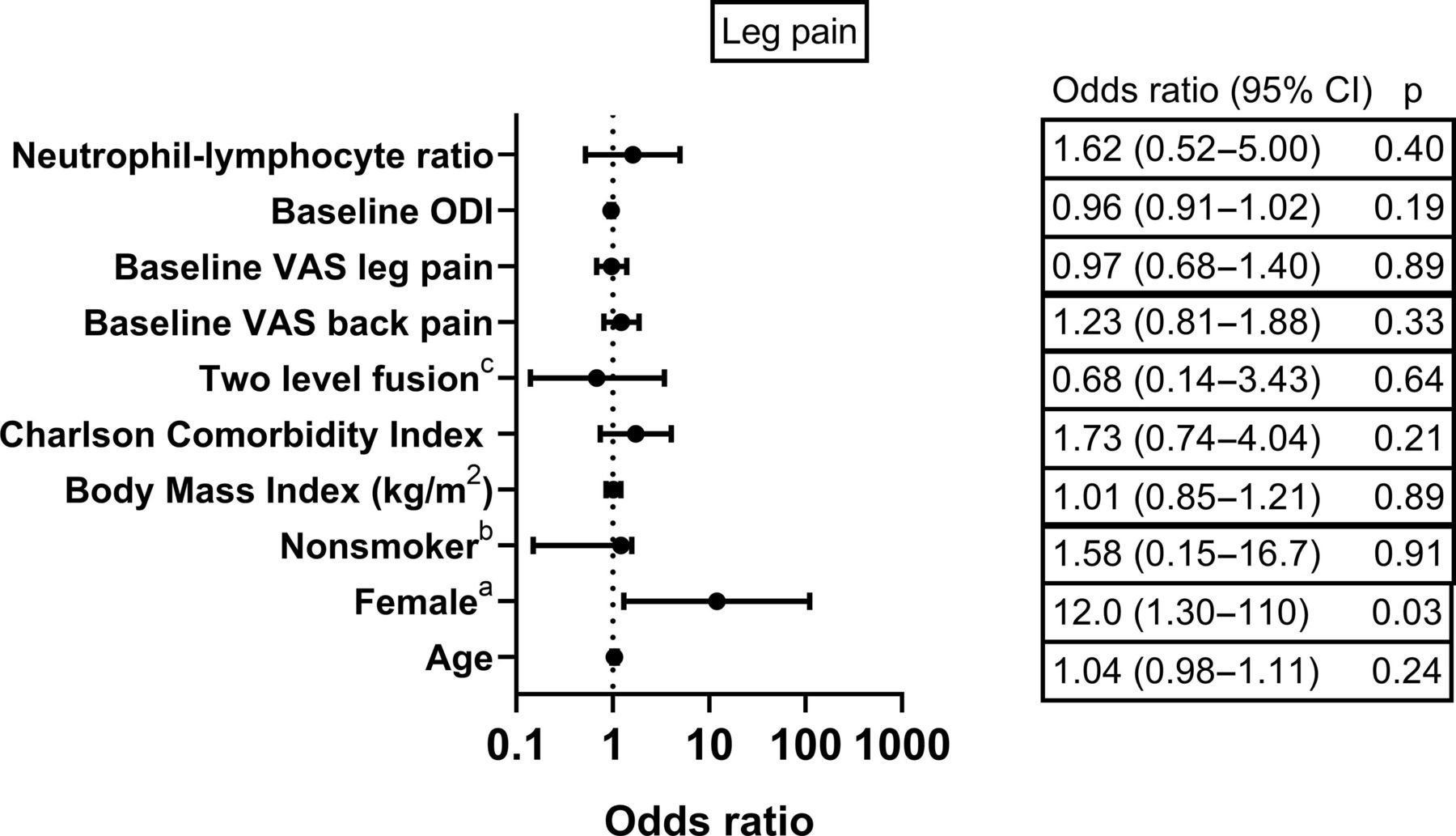
OR with 95% CI for ≥40% improvement in leg pain according to demographic/surgical factors and preoperative neutrophil-lymphocyte ratio (NLR). aCompared to men, bcompared to smokers, and ccompared to single-level fusion. ODI, Oswestry Disability Index; VAS, visual analog scale.
≥30% Improvement in ODI
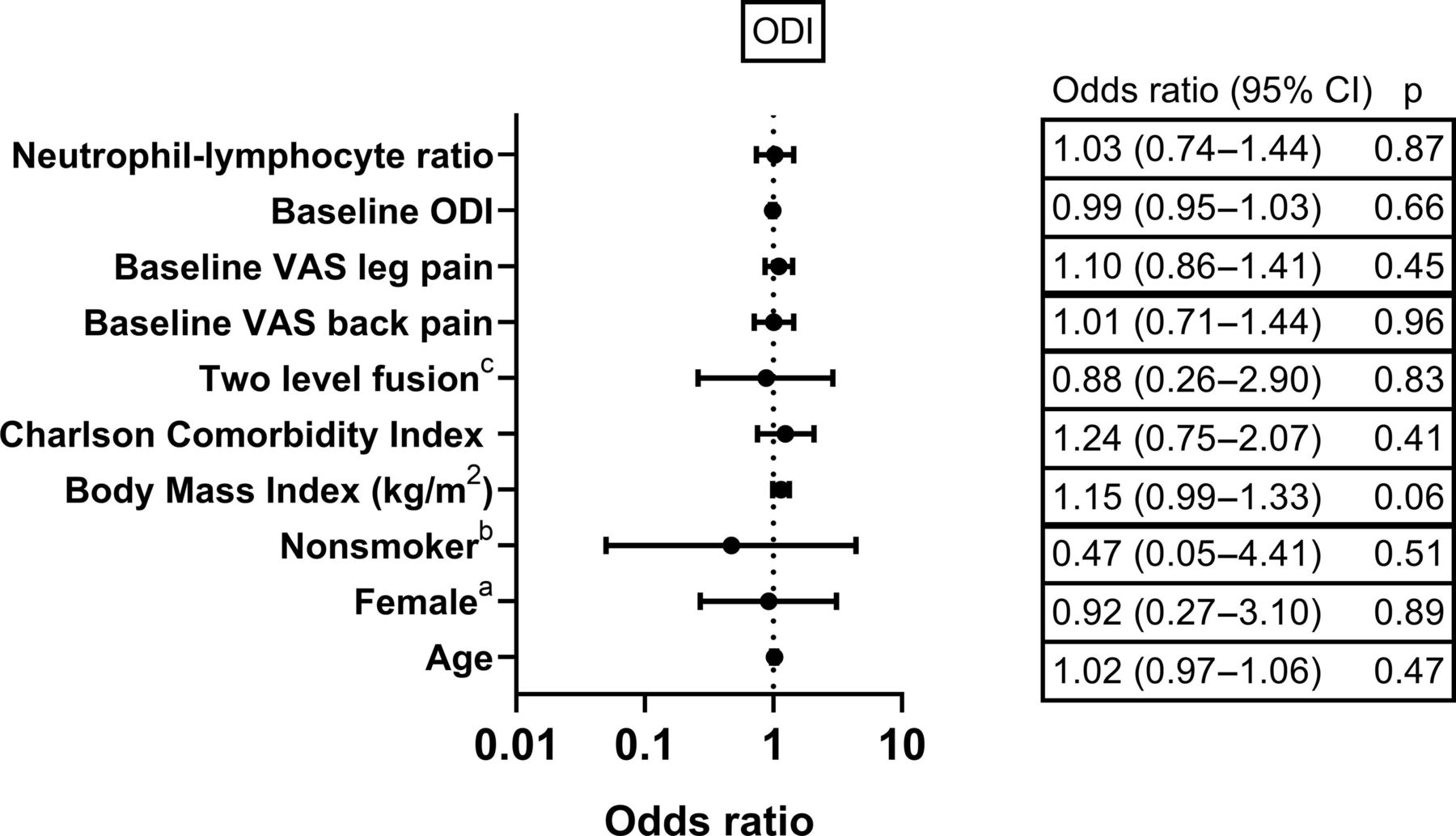
There were no statistically significant associations between the demographic/surgical factors, preoperative NLR and improvement in ODI at 12 months (Figure 3).
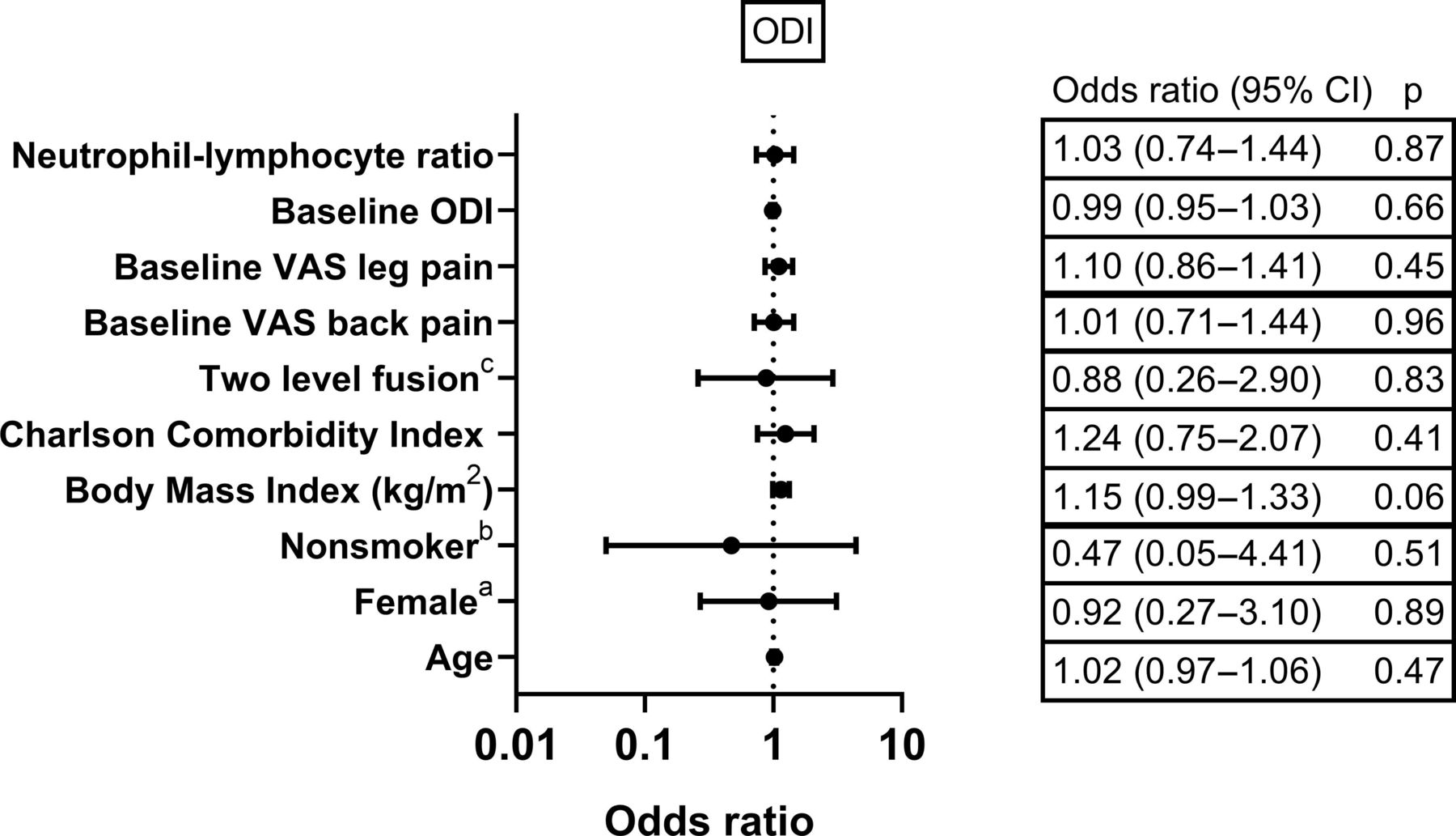
OR with 95% CI for ≥30% improvement in ODI according to demographic/surgical factors and preoperative neutrophil-lymphocyte ratio (NLR). aCompared to men, bcompared to smokers, and ccompared to single-level fusion. ODI, Oswestry Disability Index; VAS, visual analog scale.
The relationship between demographic/surgical factors, preoperative NLR, and improvement in VAS and ODI scores at 12 months is summarized in Table 2.
OR for improvement in VAS back pain, leg pain, and ODI scores ( ≥33% for VAS back pain, ≥40% for VAS leg pain, and ≥30% for ODI) at 12 months after lumbar fusion.
Discussion
This study found no evidence of a significant association between preoperative NLR and a clinically important improvement in patient-reported pain and functional outcomes at 12 months after lumbar fusion. Furthermore, we found that female patients and patients with higher preoperative VAS back pain scores have greater odds of improvement in pain outcomes postoperatively.
Immune cells contribute significantly to both inflammatory and neuropathic pain by releasing cytokines that act on nociceptors to sensitize pain pathways.13 However, measuring cytokine levels preoperatively to predict pain outcomes is expensive, time-consuming, and impractical. Cytokine production may directly influence NLR14 which is an inexpensive and objective indicator of systemic inflammation. Given the relationship between cytokine production and pain, it appears logical that preoperative NLR can predict pain outcomes postoperatively.
To our knowledge, only one other study has investigated the relationship between preoperative NLR and pain in spine surgery with none investigating the association between NLR and functional outcomes. Bozkurt et al conducted a retrospective study of 20 patients who underwent an operation for lumbar disc herniation. Although we found no statistically significant associations between preoperative NLR and preoperative pain/functional status, Bozkurt et al found a moderately positive association between preoperative NLR and baseline VAS score. Furthermore, Bozkurt et al reported a moderate positive correlation between preoperative NLR and postoperative VAS scores.15 The disparity between our findings and those of Bozkurt et al may be due to differences in our assessment of the outcome measures. Bozkurt et al used the VAS score at 6 months after surgery as their outcome measure and did not define a threshold improvement in VAS score that signifies that the patient benefited from the surgery. Conversely, we measured the percentage change in VAS and ODI scores at follow-up compared to baseline, defined improvement in pain/functional outcomes as ≥33% for VAS back pain, ≥40% for VAS leg pain, and ≥30% for ODI,12 and used the cut-offs to dichotomize the patients into “improved” and “did not improve” for each outcome measure. Measuring the percentage change in VAS or ODI scores and evaluating the proportion of patients that meet a clinically meaningful improvement threshold is the recommended method of analysis in clinical trials because it accounts for the influence of the baseline score on the postoperative score.16,17
In a retrospective study of 63 patients who underwent arthroscopic rotator cuff repair, Öner et al reported that compared to patients with preoperative NLR <2, patients with NLR ≥2 had greater pain severity and analgesic intake in the first week after surgery.8 Another retrospective study of 140 patients that underwent orthognathic surgery by Turgut et al reported that compared to patients with NLR <2, patients with NLR ≥2 had a significantly greater analgesic consumption in the early postoperative period. The authors interpreted this as a correlation of high NLR with increased postoperative pain.9 Daoudia et al conducted a cohort study of 60 patients who underwent laparoscopic cholecystectomy, investigating a relationship between preoperative NLR and postoperative pain measured by the total analgesic requirements during the first 48 hours postoperatively. In contrast to the Öner et al and Turgut et al studies, Daoudia et al found that a lower NLR was associated with higher analgesic requirements postoperatively.10 The discrepancy between these studies and ours could be due to the longer follow-up period of 12 months in our study compared to the early postoperative period in these studies. In addition, total analgesic consumption may not be a suitable surrogate measure for pain intensity.
The lack of evidence of a significant association between NLR and pain or functional outcomes reported in our study and the lack of consensus on this topic across various studies suggest that it is unlikely that NLR alone explains patient-reported pain/functional outcomes following treatment. Pain is subjective, and the perception of pain is influenced by biophysical, psychological, and sociodemographic factors. The multifactorial nature of pain is supported by the findings of Soriano et al who conducted a prospective observational study of 203 patients that underwent lumbar fusion to evaluate the predictors of improvement in pain and functional outcomes after 1 year.18 They reported that patients with higher educational levels and optimistic preoperative expectations at baseline had a greater improvement in pain/functional outcomes at follow-up. Like our study, Soriano et al reported that patients with more severe back pain at baseline had a greater improvement in back pain at follow-up.18
We also demonstrated that female patients have greater odds of improvement in leg pain at 12 months after lumbar fusion. This finding is corroborated by the results of a systematic scoping review of outcomes in the surgical management of lumbar degenerative disease which reported that female patients show an equal or greater improvement in pain outcomes compared to male patients.19
Although our study is the largest study investigating the relationship between preoperative NLR and patient-reported pain/functional outcomes in spine surgery, the sample size is relatively small, and this may have led to false-negative results. Although our hypotheses and analysis were preplanned, we have conducted multiple comparisons that increase the risk of type one error; hence, our statistically significant findings should be considered with caution. Due to a lack of data, we were unable to investigate the association between pain/functional outcomes and sociodemographic/psychological factors. Twenty-four out of 78 (31%) patients were excluded from our study due to missing data, and this may be a source of bias as it may have led to an overestimation or underestimation of the associations between the outcome measures and the independent variables that were considered.20 However, some spine surgery studies reporting a missing data rate of 22%–40% have demonstrated that missing data do not hamper the interpretation of findings in spine surgery patients.21–23 Lastly, our data were obtained from operations performed by the same surgeon at a single center; hence, the results may not be generalizable. Future studies should have a large prospective multicenter design and should incorporate sociodemographic/psychological factors in their analysis.
Conclusion
Our study found no evidence of an association between preoperative NLR and patient-reported pain/functional outcomes at 12 months after lumbar fusion. This suggests that contrary to previous studies, preoperative NLR alone is not a suitable independent predictor of pain/functional outcomes after lumbar fusion. Although there is a biophysical component to pain and disability, pain and disability are also influenced by sociodemographic and psychological factors that should be considered by the spine surgeon when selecting patients for lumbar fusion.
Footnotes
↵† Temidayo Osunronbi and Hiba Lusta are joint first authors.
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This retrospective study was registered and approved by the Clinical Audit Department at University Hospitals Plymouth NHS Trust (Study registration number: CA_2020-21-130. Approved on 12 October 2020). All applicable international, national, and institutional guidelines for the care and use of the patient’s anonymized clinical data were followed.
Data Availability The collected raw data of demographics, operative factors, preoperative NLR, and VAS pain scores are presented in Supplemental Material 1.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.