


Abstract
Background This study aimed to clarify the quantitative threshold of intraoperative radiological parameters for suspecting posterior malposition of the oblique lumbar interbody fusion (OLIF) cage triggering contralateral radiculopathy.
Methods We measured the sagittal center and axial rotation angle (ARA) of the cage using postoperative computed tomography (CT) in 130 patients (215 cages) who underwent OLIF. The location of the cage tip was determined from axial magnetic resonance imaging in selected cases based on CT simulations to assess whether the cage was in contact with the contralateral exiting nerve or whether the surgical instruments could contact the nerve during intradiscal maneuvers.
Results The sagittal center of the cages was on average 41.5% from the anterior edge of the endplate (shown as AC/AP value: anterior end plate edge-cage center/anterior-posterior endplate edge ×100%), and posterior cage positioning ≥50% occurred in 14% of the cages. The ARA was −2.9°, and posterior oblique rotation of the cages ≥10° (ARA ≤ −10°) was observed in 13%. CT simulation showed that the cage tip could directly contact the contralateral nerve when the cage was placed deep in the posterior portion ≥50% of the AC/AP values with concomitant posterior axial rotation ≥10° (ARA ≤ −10°), or deep in an extremely rare portion ≥60% of the AC/AP values with posterior axial rotation ≥0° (ARA ≤ 0°). Six percent of the cages (13/215) were placed in these posterior oblique areas (potential contact area: PCA). Three cages in the PCA were in direct contact with the contralateral nerves, and 9 were placed deep just anterior to the nerves. Symptomatic contralateral radiculopathy occurred in 2 cages (2/13/215, 15.3%/0.9%).
Conclusions Two intraoperative radiological parameters (AC/AP and ARA) measurable during OLIF procedures may become practical indicators for suspecting cage malposition in PCA and may be available when determining whether to consider cage revision intraoperatively to a more ventral disc space or anteriorly from the opposite endplate edge.
Level of Evidence 4.
- oblique lumbar interbody fusion
- OLIF
- contralateral radiculopathy
- surgical complication
- cage malposition
- MPR-CT
- MRI
- radiological parameter
Introduction
In oblique lumbar interbody fusion (OLIF), a large footprint cage that reaches the opposite ring apophysis and orthogonal maneuvering through the ante-psoas approach are key concepts in achieving high fusion rates, sufficient deformity correction, and indirect decompression.1–5
Under fluoroscopic control with anteroposterior (AP) and lateral (right-left: RL) views, surgeons should be aware of the positions of the 4 radiographic markers attached to the polyetheretherketone (PEEK) cage to control the axial rotation angle (ARA) and the sagittal/coronal position of the cage to place the OLIF cage along the parallel axis of the disc space at the junction of the anterior one-third and posterior two-thirds in the sagittal plane.6
Posterior oblique and deep cage insertion beyond the opposite edge of the endplate may injure the contralateral exiting nerve directly6–11 or indirectly through extraforaminal disc extrusion12 or vertebral osteophyte/endplate fracture.6,8,12,13 In addition, intradiscal maneuvers such as aggressive breaking of the contralateral annulus with Cobb’s elevator and deep trial cage insertion may injure the nerve.
Contralateral radiculopathy is a rare but potentially serious complication of lateral lumbar interbody fusion14–21 and has been reported to occur in 0.4% to 9.3%6–13,22 of lateral lumbar interbody fusion cases. A recent article described 2 cases of contralateral radiculopathy due to extraforaminal disc herniation attributed to posterior oblique malposition of the OLIF cage.23 The sagittal and axial position of the inserted OLIF cage may be a critical issue for contralateral nerve root injury. However, few studies have addressed the effect of OLIF cage position on contralateral radiculopathy, and we could not find any reports discussing such an effect using quantitative 2-dimensional computed tomography (CT) analysis. To date, the threshold of cage malposition that causes contralateral nerve injury is unknown.
The purpose of the present study was to quantitatively evaluate the position of the OLIF cage in the sagittal, coronal, and axial planes using CT and to clarify the quantitative threshold of posterior oblique cage malposition that causes contralateral radiculopathy. Finally, we aimed to define a useful combination of intraoperative radiological parameters, measurable on fluoroscopic images, that would contribute to early reconfirmation of cage malposition and depth during OLIF procedures to avoid symptomatic radiculopathy.
Materials and Methods
Patients
We performed a single-center, retrospective review of patients with the following criteria: (1) age ≥18 years, (2) undergoing OLIF with posterior instrumented fixation using pedicle screw-rod systems, (3) treatment for degenerative lumbar disorders, (4) consecutive cases between June 2019 and October 2021, and (5) follow-up for more than 3 months after surgery. Patients with previous disc space surgery including discectomy and percutaneous procedures were excluded from this study. All patients underwent postoperative CT (HITACHI Supria 16 raw helical, Japan) and magnetic resonance imaging (MRI, GE Signa 1.5T, USA) within 2 weeks of surgery at the authors’ institution with informed consent, in addition to preoperative imaging studies to perform quantitative morphometric analysis of OLIF cage placement. Clinical signs of new-onset contralateral radiculopathy following OLIF procedures, such as radicular pain, numbness, and muscle weakness, were recorded between postoperative day 1 and 3 months. Institutional review board approval was obtained (HSC202303).
Surgical Technique
All patients underwent OLIF via the left-side retroperitoneal ante-psoas approach (5- to 6-cm skin incision) according to the standard protocol14,24 using a lordotic PEEK cage (6° lordotic, CLYDESDALE PTC, Medtronic, Memphis, TN, USA) without real-time electromyographic neuromonitoring. We used standard surgical instruments such as Cobb’s elevator, shaver, and curette equipped in the OLIF25 (Medtronic, Memphis, TN, USA) to release the contralateral annulus fibrosus from the vertebral endplates, taking care not to protrude these instruments too far beyond the endplate edge under fluoroscopic control. We used only a 6° lordotic cage because it fits well in the small Japanese disc space and has a shorter AP diameter (18 mm) than a 12° lordotic cage (22 mm). The cage size and height were 45 to 55 mm and 8 to 14 mm, respectively. The cages were filled with artificial bone materials (β-TCP: AFFINOS: Kuraray, Tokyo, Japan, or DBM: Grafton: Medtronic, Minneapolis, MN, USA) mixed with bone marrow blood collected from the iliac bone. The number of disc levels operated on ranged from 1 to 3 levels. In addition, all patients underwent posterior instrumented fixation with pedicle screw-rod systems via an open or percutaneous approach that included all fusion segments in OLIF. Decompression for concomitant lumbar canal stenosis (LCS) was performed either indirectly through OLIF or directly through laminotomy, depending on the status and severity of the stenosis. In cases of severe central canal stenosis causing cauda equina syndrome with neurogenic bladder dysfunction or muscle weakness (manual muscle testing: <3/5), we performed direct decompression. Foraminal stenosis was treated with indirect OLIF decompression.
Radiological Analysis
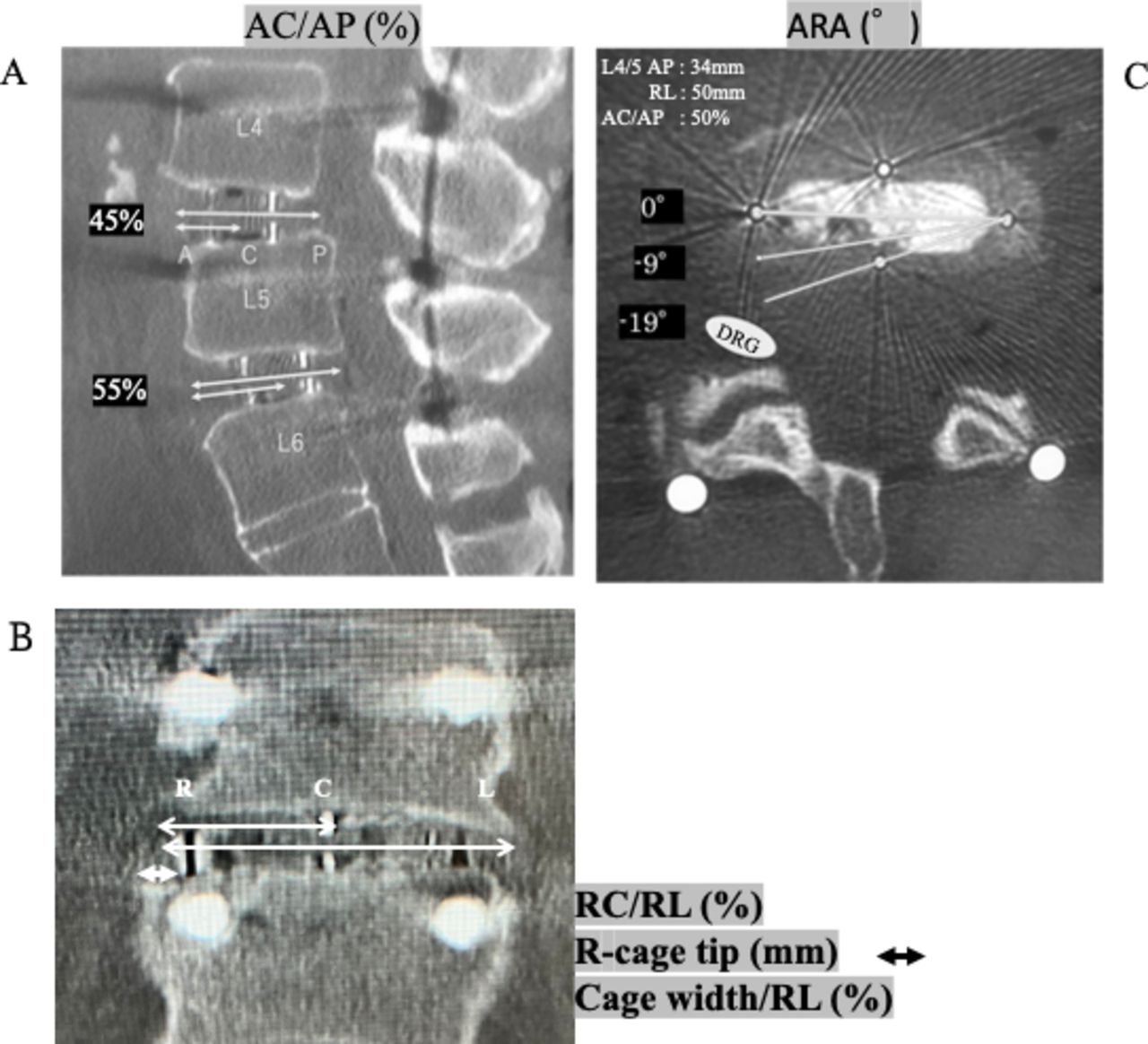
We measured the sagittal center position and rotation angle in the axial plane of the OLIF cages using postoperative CT images of 215 intervertebral discs in 130 patients. The sagittal center of the inserted OLIF cage was calculated as the AC/AP value × 100% on the sagittal CT images (Figure 1a). The coronal center of the OLIF cage ( right endplate edge-cage center/right-left endplate edge [RC/RL] value: × 100%) and the distance between the cage tip and the right endplate edge (R-cage tip mm: expressed as anterior [−] or posterior [+] to the edge) on the coronal CT images were measured in selected cases based on the CT simulations (Figure 1b). The cage rotation angle in the axial plane (ARA) was expressed as anterior [+] or posterior [−] rotation from the transverse axis of the disc on the axial CT images (Figure 1c).

(A) The sagittal center of the cage (AC/AP value, %). (B) The coronal center of the cage (RC/RL value, %) and the distance between the cage tip and the right endplate edge (R-cage tip, mm). (C) The ARA (a posterior rotation from the transverse axis of the disc was expressed as "-") are measured on the MPR-CT images. The oblique lumbar interbody fusion cage (50 × 18 mm) is inserted orthogonally to the transverse axis (ARA: 0°) at 50% from the AC/AP at L4/5 (AP: 35 mm, RL: 50 mm). Three white lines indicate 0°, 9°, and 19° of posterior rotation (ARA: 0°, −9°, and −19°). A white oval indicates the right L5 exiting nerve root. Abbreviations: AC/AP, anterior endplate edge-cage center/anterior-posterior endplate edge; AP, anteroposterior; ARA, axial rotation angle;MPR-CT, multi-planar reconstruction computed tomography; RC/RL, right endplate edge-cage center/right-left endplate edge; RL, lateral (right-left).
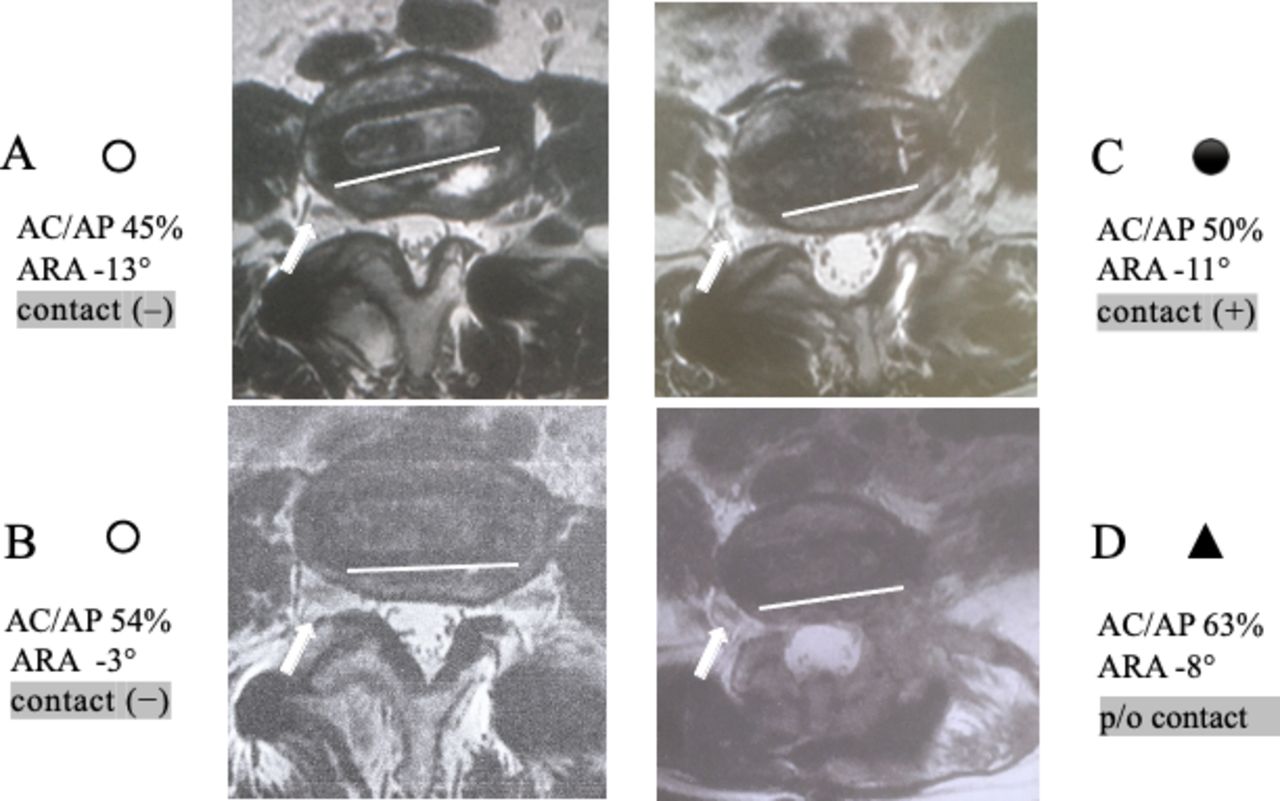
The position of the front (right) tip of the cage and the direction of cage insertion were determined from the axial MRI (T2W/SE, Figure 2) in selected cases based on the CT simulations to determine” whether there was direct contact of the contralateral exiting nerve root by the cage tip in the extraforaminal space (contact [+]: “●”) or not (contact [−]: “○”). Even if there is no direct contact between the cage tip and the opposite nerve root, there is a possibility of damage to the opposite nerve root by surgical instruments during intradiscal maneuvers (ie, during curettage of disc cartilage or insertion of Cobb’s elevator and trial cage) if the cage tip is directed toward the opposite posterolateral corner in the disc space and is inserted deeply just in front of the nerve (possibility of [p/o] contact: “▲”). In addition to the position of the cage tip, the direction of the cage toward the contralateral nerve root, which was expressed by a white dotted line marked on the posterior edge of the cage (Figure 2), became a determining factor in certifying the “p/o contact.”

The position of the front (right) tip of the cage and the direction of the posterior edge of the inserted cage were determined on axial magnetic resonance imaging. (A and B) Cases without direct contact between the cage and the opposite exiting nerve (contact [−]: “○”). (C) A case with direct contact between the cage and the opposite nerve (contact [+]: “●”). (D) A case with the possibility of injury to the opposite nerve during intradiscal maneuvers despite no direct contact between the cage and the nerve (the oblique lumbar interbody fusion cage was inserted deeply just in front of the nerve and directed toward the nerve, possibility of contact: “▲”).
To provide baseline data for simulating the possibility of contact between the OLIF cage and the contralateral exiting nerve at the extraforaminal space on the axial CT image of an average-sized vertebra, we evaluated the morphometry of the lumbar vertebral endplates, including the anteroposterior (AP) and lateral (RL) diameters and the ratio of AP diameter to RL diameter (AP/RL) from the L2/3 to L4/5 intervertebral disc levels using the sagittal and coronal CT images. We examined the respective means and differences between disc levels, sexes, and individuals.
Statistical Analysis
The Kruskal-Wallis nonparametric test was used to analyze AC/AP values and ARAs between disc levels (L2/3, L3/4, and L4/5/6). Data from the L4/5 and L5/6 disc levels were analyzed as 1 group due to the small number of patients at the L5/6 level (n = 2). Scheffe’s post hoc analysis was performed using the Kruskal-Wallis test. Pearson’s χ2 test was used to analyze the incidence of cages with ≥50% AC/AP values, cages with ≤−10° in ARA, and cages within a demarcated area among the 3 intervertebral disc levels. Pearson’s simple correlation coefficient between the AC/AP value and ARA was analyzed at each disc level from L2/3 to L4/5/6. A one-way analysis of variance test was used for the analysis of vertebral AP diameter, RL diameter, and the ratio of AP diameter to RL diameter between disc levels, and a t test was used for the analysis between men and women. Statistical significance was defined as a P value < 0.05.
Results
This study included 130 consecutive patients, including 54 men and 76 women, aged 44 to 90 years (mean: 72 years), who underwent OLIF for degenerative lumbar disorders such as degenerative lumbar scoliosis (n = 46), degenerative spondylolisthesis (n = 42), LCS (n = 40, including previous surgery), and LCS with old vertebral fracture (LCS + VFx, n = 2). The OLIF cages were placed in 215 intervertebral disc spaces at L2/3 (n = 35), L3/4 (n = 72), L45 (n = 106), and L5/6 (n = 2). In 2 cases with transitional anatomy (Castellvi type IIIb and type IV), we placed OLIF cages at the L5/6 level through the ante-psoas approach lateral to the aorta or common iliac vessels after preoperative evaluation of the vascular anatomy in the transitional zone based on MRI and 3D-CT angiography. The mean number of OLIF discs was 1.7 (1–3 levels, Table 1). A 6° lordotic PEEK cage was inserted in each case, and the width of the cage was determined to reach the opposite ring apophysis but not to exceed the opposite lateral edge of the respective endplate. The average cage size and height were 49.7 (45–55) mm and 10.3 (8–14) mm, respectively (Table 1). Cages were filled with beta-tricalcium phosphate (17 cages/10 cases), or decalcified bone matrix (198 cages/120 cases).
Demographic data of patients (N = 130).
The sagittal center positions of the OLIF cages at L2/3, L3/4, and L4/5/6 were 41.1%, 42.2%, and 41.2% from the AC/AP values, respectively. There was no statistically significant difference in AC/AP values between the disc levels. Posterior installation of the cages ≥50% of the AC/AP values at L2/3, L3/4, and L4/5/6 was observed in 14.3%, 16.7%, and 10.2% of cages at each level, respectively (Table 2; Figure 3).
Demographic data of radiological analysis.

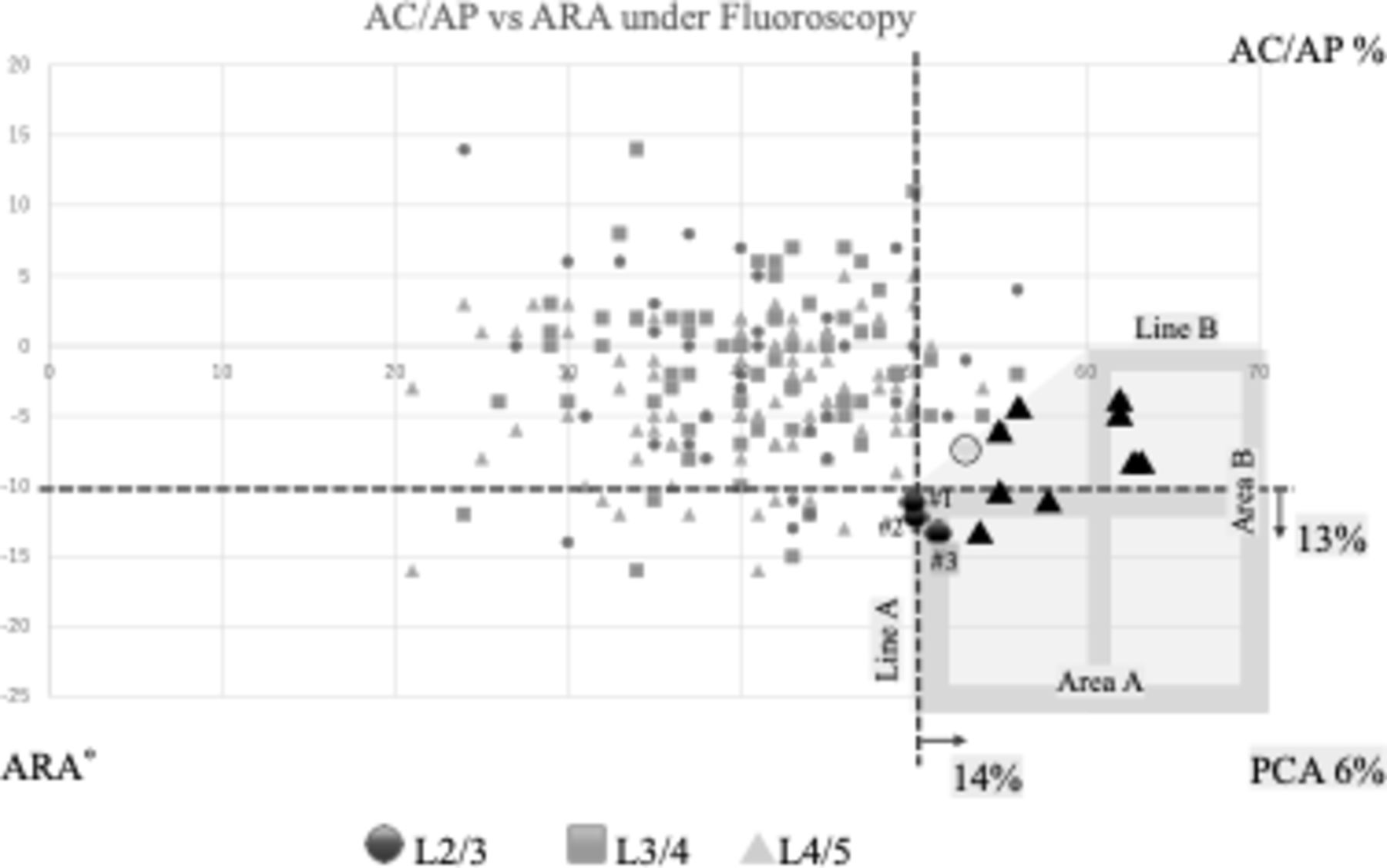
The sagittal center position (AC/AP value, the x-axis) and the axial rotation angle (ARA, the y-axis) of the oblique lumbar interbody fusion cages at L2/3 (n = 35), L3/4 (n = 72), and L4/5 (n = 108, including two L5/6 transitional vertebrae) were plotted on the scatter plot. The right-lower area delineated by lines A and B and a connected line between lines A and B shows a “PCA” (consisting of area A, area B, and a transition area is colored gray). Six percent of the total cages (13/215 cages) were inserted into this area. Abbreviations: AC/AP, anterior endplate edge-cage center/anterior-posterior endplate edge; ARA, axial rotation angle; PCA, potential contact area.
The ARA of OLIF cages at L2/3, L3/4, and L4/5/6 were –1.7°, –1.9°, and –4°, respectively, with the ARA of L4/5/6 being less than that of L2/3 and L3/4 with a significant difference (L2/3, L3/4 vs L4/5/6, P < 0.05 by Kruskal-Wallis test). Posterior-oblique rotation of the cages ≥10° (ARA ≤ –10°) in the horizontal plane was observed in 11.4%, 11.1%, and 13.9% of the cages at L2/3, L3/4, and L4/5/6, respectively (Table 2, Figure 3). There were no significant differences in the incidence of ≥50% AC/AP values and the incidence of ≤–10° in ARA between disc levels (Table 2). There was no significant correlation between the sagittal center position (AC/AP value) and ARA of the OLIF cage at each level.
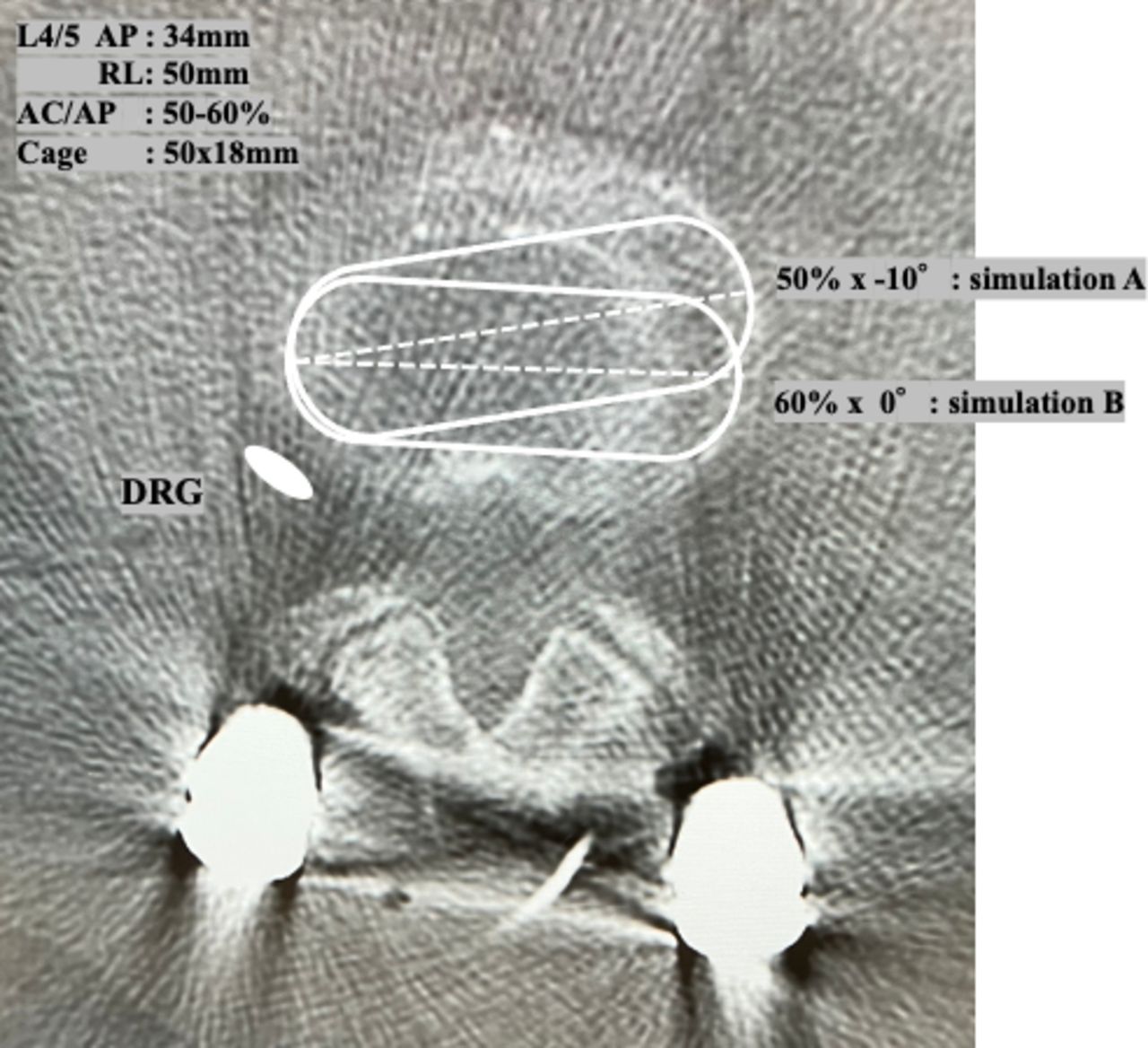
CT simulations on the axial vertebral endplate image with average-sized AP and RL diameters (AP: 34 mm, RL: 50 mm at L4/5, Figure 4 and Table 3) showed that the front (right) tip of the OLIF cage (cage width: 50 mm, cage depth: 18 mm) and surgical instruments may contact the contralateral exiting nerve root in the extraforaminal space when the cage/surgical instruments are inserted deep beyond the right edge of the endplate into the posterolateral part of the disc space ≥50% of the AC/AP values with concomitant posterior axial rotation ≥10° (ARA ≤ –10°). This area was delineated as the right lower area by line A and a rough dotted line on the –10° line of the scatter plot (area A: Figures 3 and 5). In addition, even an orthogonally placed OLIF cage (ARA = 0°) may contact the opposite nerve root if the cage was placed in an extremely rare portion of the disc space ≥60% of the AC/AP values (area B: a lower area delineated by line B, Figures 3 and 5).

The possibility of contact between the front (right) tip of the oblique lumbar interbody fusion (OLIF) cage and the opposite exiting nerve root was simulated on the axial computed tomography image of the average-sized endplate at L4/5 (AP: 34 mm, RL: 50 mm). Simulation A: Cage insertion in the middle part of the disc space (50% of the AC/AP value) with 10° posterior rotation (axial rotation angle [ARA]: –10°); Simulation B: Cage insertion in the extremely rare part of the disc space (60% of the AC/AP value) without axial rotation (ARA: 0°). In both simulations, the OLIF cage could contact and injure the opposite exiting nerve if inserted deeply. Abbreviations: AC/AP, anterior endplate edge-cage center/anterior-posterior endplate edge; AP, anteroposterior; DRG, dorsal root ganglion; RL, lateral (right-left).
Morphometry of vertebral endplate by sex.

Postoperative axial magnetic resonance imaging of 13 cages in PCA showed direct contact between the front (right) tip of the inserted cage and the opposite exiting nerve in 3 cages (#1–#3, contact [+]: “●”) and the possibility of contact during intradiscal maneuvers in 9 cages (possibility of contact: “▲”). One cage plotted on the border of the PCA showed no possibility of contact (contact [–]: “○”). Abbreviations: AC/AP, anterior endplate edge-cage center/anterior-posterior endplate edge; ARA, axial rotation angle; PCA, potential contact area.
Six percent of the total cages (13/215 cages; L2/3: 1/35 = 2.9%, L3/4: 6/72 = 8.3%, L4/5L5/6: 6/108 = 5.6%) were placed within area A, area B, and a transition area between areas A and B (Table 2, Figures 3 and 5).
The mean coronal center position of these 13 cages was 48.4% (42.2–52.4) from the right endplate edge-cage center/right-left endplate edge (RC/RL value), the mean distance between the cage tip and the right edge of the endplate (R-cage tip) was –0.5 (–5 to +7) mm, and the mean endplate coverage rate by the cage in the coronal plane was 93.8% (78.8–100; CW/RL value, Table 2).
Three cages in area A, area B, and a transition area had substantial contact with the opposite nerves on axial MRI images (#1–#3, Figures 5 and 6) and were at potential risk for contralateral radiculopathy (3/13 cages, contact [+]: “●”; Table 2). Although 9 cages in these areas did not contact the opposite nerves on axial MRI, these cages had the potential for contact between surgical instruments and the opposite nerves during deep or forceful intradiscal maneuvers because the cage tips were placed deep just in front of the nerves (9/13 cages, p/o contact: “▲”; Figure 5 and Table 2). Only 1 cage in these areas at L2/3 had enough space and no chance of contact between the cage/surgical instruments and the opposite nerve (1/13 cages, contact [–]: “○” in Figure 5 and Table 2).

Postoperative axial magnetic resonance imaging of 3 cages recognized as the contact (+) group and 1 cage causing extruded disc herniation within the PCA on the scatter plot are shown (cases #1–3 and #LDH). Cases #1 and #2 had direct contact between the cages and the opposite exiting nerves but had no symptoms (contact [+]: “●”). Case #3 had direct contact with the opposite nerve and presented with new-onset right L4 radiculopathy after oblique lumbar interbody fusion (OLIF; contact [+]: “●”). Case #LDH had right L5 radiculopathy due to extruded disc herniation induced by OLIF procedures, although there was no direct contact between the cage and the nerve (possibility of contact: “▲”). Abbreviations: AC/AP, anterior endplate edge-cage center/anterior-posterior endplate edge; ARA, axial rotation angle; LDH, lumbar disc herniation; PCA, potential contact area; p/o, possibility of.
New-onset symptomatic contralateral radiculopathy associated with OLIF procedures occurred in 2 cages at L4/5 and L5/6 within 12 cages classified as “contact (+) or p/o contact” group (case #3: “●” and case #LDH: “▲”; Figures 5 and 6),24 and the actual incidence of symptomatic radiculopathy was very low (15.4%: 2/13 cages in a demarcated area, 1/3 cages with contact [+] and 1/9 cases with p/o contact, Table 2).
Case #LDH was included in the p/o contact group because the extruded disc herniation caused right L5 radiculopathy with severe leg and foot pain, numbness, and muscle weakness of tibialis anterior and extensor hallucis longus (manual muscle testing: 3-/5). Discectomy was performed 1 week after OLIF without cage position adjustment because the OLIF cage did not directly compress the nerve. In case #3, the OLIF cage directly compressed the right L4 root, but the compression was not severe, and pain relief (mild → none) and neurological recovery (manual muscle testing: tibialis anterior 4/5 → 5/5) occurred spontaneously within several weeks without surgical intervention. In both cases, the right L5 and L4 radiculopathies were not present prior to OLIF procedures, and there were no causes other than extruded disc herniation and cage malposition leading to new-onset contralateral radiculopathies.
Of several cages placed just outside a defined area (areas A, B, and a transition area), only 1 cage at L4/5 was judged to be in the p/o contact group, which had no clinical signs.
Discussion
Among the various advantages of minimally invasive OLIF,3,5 deformity correction and indirect decompression with a large footprint cage24–26 through a retroperitoneal ante-psoas approach are considered to be major technical advances2,3 and are suitable for adult spinal deformity in elderly populations4 and revision cases.27,28 The orthogonal maneuver in OLIF is an important concept to place a large footprint cage in the safe area of the disc space without contralateral nerve damage and is usually performed under fluoroscopic guidance.29,30
Previous reports have described that contralateral lower limb radiculopathy occurs in 0.4% to 9.3% of OLIFs,6,8–13,21,22 and among several pathologies of contralateral radiculopathy, cage malposition has been reported as the most common cause.
To date, several radiological evaluations of the OLIF cage position have been published in terms of surgical effects on segmental lordosis, disc height, and cage subsidence, and few studies have discussed the effect of the OLIF cage position on contralateral radiculopathy.
Only Nisarg et al6 provided some guidelines to avoid this complication, recommending anterior cage placement at the junction of the anterior one-third and posterior two-thirds of the disc space.
Quantitative analyses of “malposition” have not been performed in previous articles6–8 because significant morphometric variations of the lumbar vertebral endplates between different disc levels, sexes, and individuals, as well as various vertebral deformities, may affect the actual cage/surgical instrument contact with the opposite nerve and subsequent nerve damage, even when a cage of the same width is inserted.
The current study showed that 13 cages (13/215, 6%) placed in the posterior oblique area of the disc space (including area A: posterior placement ≥50% in AC/AP value with concomitant posterior rotation angles ≥10° [≤–10° in ARA] area B: posterior placement ≥60% in AC/AP value with posterior axial rotation ≥0° [ARA ≤ 0°], and a transition area between areas A and B) had the potential risk of contact and injury to the contralateral nerve if the cage/surgical instruments were inserted deeply and forcefully.
Of 13 cages, postoperative axial MRI showed direct contact of the cage tip with the opposite nerve in 3 cages (contact [+]) and 9 cages placed just anterior to the opposite nerve without contact (p/o contact). New contralateral radiculopathy occurred after OLIF in only 2 cages (contact [+] and p/o contact groups), and most cages placed in areas A, B, and a transition area (11/13 cages: 85%) did not contribute to symptomatic contralateral radiculopathy (Figure 6).
There may be several reasons why the sensitivity of the 2 radiological parameters (AC/AP value and ARA) as a threshold for cage malposition leading to clinical contralateral radiculopathy was relatively low. In addition to the variations in the coronal central position and width of the inserted cages, several factors such as adhesion around the exiting nerve, the transverse route of the nerve, osteophyte formation, and significant morphometric variations of the lumbar vertebral endplates may influence the symptomatic manifestation of contralateral radiculopathy even in a case with actual cage-nerve contact (Table 3). Even with substantial contact between the OLIF cage and the contralateral exiting nerve on axial MRI, the nerve may escape severe damage and clinical manifestation of radiculopathy, if the nerve has sufficient mobility around the adjacent tissue. In fact, in 2 out of the 3 cases in the contact (+) group, there was no symptomatic radiculopathy. On the other hand, if the nerve is adherent to the surrounding structures (ie, intervertebral disc, vertebral osteophyte, and psoas muscle), even mild nerve compression by the protruding OLIF cage could injure the nerve and cause clinical signs due to radiculopathy.
There was no new-onset contralateral radiculopathy in any of the remaining 8 cases in the p/o contact group, except for case #LDH, which had indirect contact with the contralateral nerve through an extruded disc herniation. Substantial direct/indirect contact between the exiting nerve and the OLIF cage appears to be essential for the development of symptomatic radiculopathy, although there is a small possibility of nerve injury during the forceful release of the opposite annular ring beyond the endplate edge at the posterolateral corner of the disc space.
We have termed area A, area B, and a transition area the “potential contact area (PCA)” in the disc space during OLIF procedures (Figures 5 and 6), where an installed OLIF cage and surgical instruments may have a potential risk of contacting the opposite nerve root and causing contralateral nerve damage.
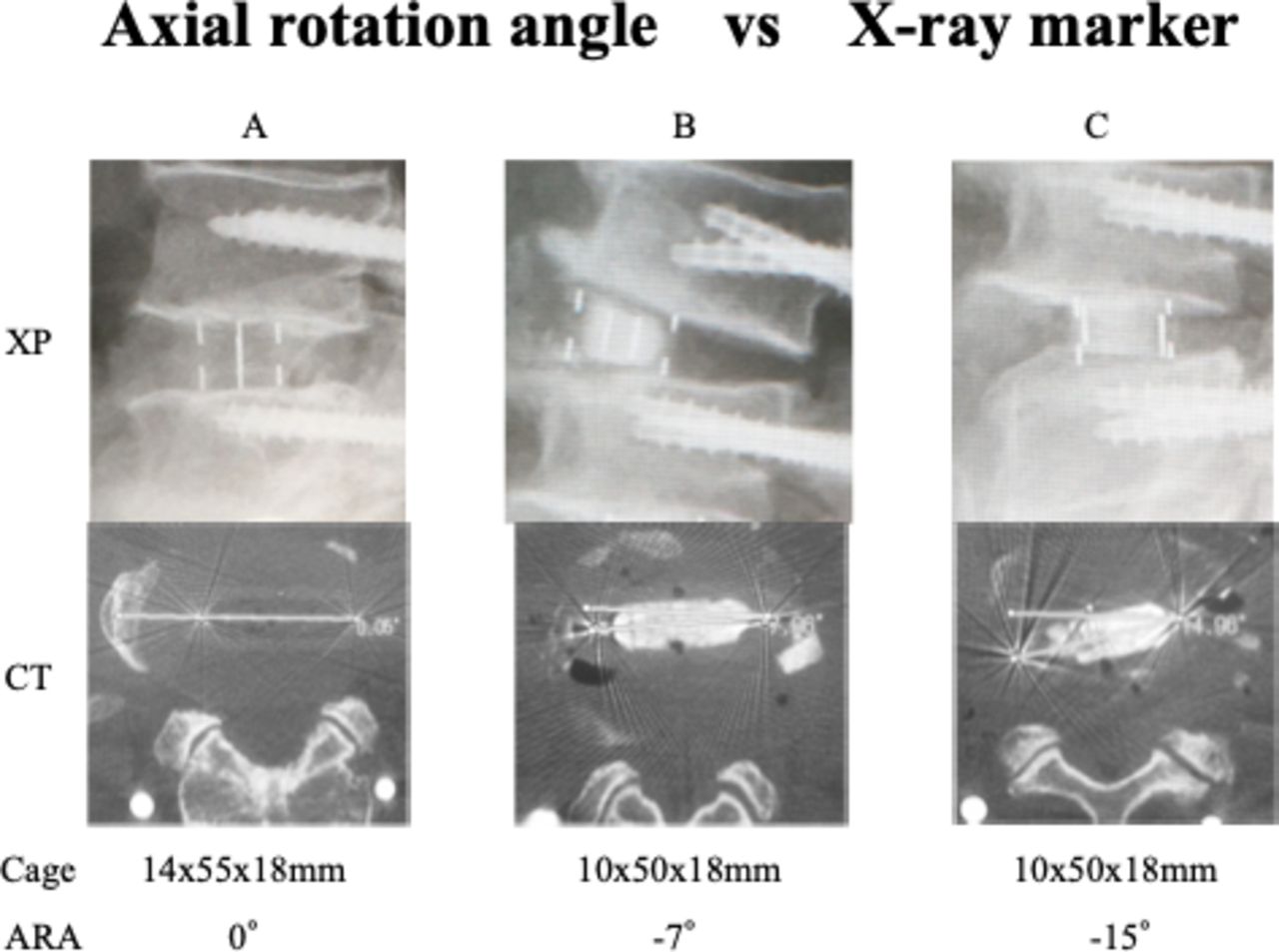
PCA is defined by a combination of 2 radiological parameters (AC/AP value and ARA) that indicate the sagittal center and axial rotation positions of the OLIF cage and are easily measured on the lateral fluoroscopic image during OLIF procedures. Four x-ray line markers are embedded in the PEEK cage and are considered practical indicators for predicting the ARA of the cage and its center position during cage insertion. Three x-ray line markers indicate orthogonal insertion to the transverse axis of the disc (ARA: 0°; Figure 7a), 4 x-ray line markers spaced every third of the AP diameter of the cage indicate approximately 7° to 9° of axial rotation depending on the cage width (an actual ARA: –7°; Figure 7b), and 2 x-ray line markers indicate approximately 15° to 19° of axial rotation (an actual ARA: –15°, Figure 7c).

The positions of 4 x-ray line markers embedded in the polyetheretherketone cage are useful indicators for predicting the ARA of the cage during cage insertion. (A) Three x-ray line markers indicate orthogonal insertion to the transverse axis of the disc (ARA: 0°). (B) Four x-ray line markers spaced every third of the AP diameter of the cage indicate 7° to 9° of axial rotation depending on the cage width (an actual ARA: –7°). (C) Two x-ray line markers indicate 15° to 19° of axial rotation (an actual ARA: –15°). Abbreviations: ARA, axial rotation angle; CT, computed tomography; PCA, potential contact area; XP, x-ray photography.
If posterior oblique cage insertion into the PCA is suspected based on these 2 radiological parameters during “orthogonal” procedures, revision of the cage to a more anterior disc space is recommended to avoid direct contact of the OLIF cage with the contralateral exiting nerve. Also, if posterior oblique insertion of the OLIF cage is unavoidable due to anatomical variations such as a rising psoas muscle or high iliac crest at the L4/5 and L5/6 transitional disc levels, the cage should be placed slightly anterior to the opposite endplate edge.
It is recommended to reconfirm the cage depth and measure the distance between the cage tip and the right endplate edge on the coronal fluoroscopic image to assess whether there is actual contact between the cage and the opposite nerve before considering revision, as these 2 radiological parameters do not provide any information on the coronal cage position. However, the shape of the vertebral endplate is generally oval, and surgeons should be aware that intraoperative fluoroscopic AP images may not provide the exact depth of the opposite cage tip if the cage is inserted obliquely.
The current study has several limitations, such as being a retrospective single-center study, limited data set available for analysis, data analysis based on inductive methods, and significant morphometric variations of the lumbar vertebral endplates, which may reduce the sensitivity of the present CT simulation model to clarify the threshold of radiological parameters to detect contralateral radiculopathy. In addition, different degrees of deformity with osteophyte formation may affect the actual contact rate and contralateral nerve injury.
Contralateral radiculopathy is a rare but potentially serious neurological complication of OLIF. This radiological definition of PCA may provide surgeons with new perspectives on OLIF cage placement and transform contralateral radiculopathy following OLIF from an unpredictable to a preventable complication.
Conclusion
We quantitatively analyzed the position of the OLIF cage in the sagittal and axial planes using 2 radiological parameters (AC/AP value and ARA) in addition to the coronal parameters and clarified the actual and potential risks of contralateral nerve root involvement related to the posterior oblique malposition of the cage. The tip of the cage and surgical instruments may directly contact and injure the contralateral nerve if the cage/surgical instruments are inserted deep in the posterior oblique area, defined as the PCA: the posterior portion ≥50% in AC/AP value concomitant posterior axial rotation ≥10° (ARA ≤ −10°), the posterior portion ≥60% in AC/AP value with concomitant posterior axial rotation ≥0° (ARA ≤ 0°), and a transition area. Although confirmation of the cage depth in the coronal plane is essential to estimate the actual contact of the cage with the contralateral exiting nerve, 2 intraoperative radiological parameters, AC/AP value and ARA, which are measurable from fluoroscopic images during the OLIF procedures, may become practical indicators to suspect cage malposition in PCA and available to the decision maker to consider cage revision to avoid opposite nerve injury.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethical Approval The institutional review board (Hachioji Spine Clinic review board) approved this retrospective study and granted a waiver of informed consent (approval code: HSC202303).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.