


Abstract
Background Intraoperative hypotension (IOH) has been found to be associated with organ damage, including cardiac injury and acute kidney injury (AKI). However, to our knowledge, this relationship has not been studied in a neurosurgery-specific patient population. In this report, we review our institutional experience to understand the magnitude of association between IOH in spinal fusion operations and incidence of postoperative AKI.
Methods This retrospective cohort study included 910 patients who underwent posterior spinal fusion procedures performed in the prone position. Intraoperative variables collected and analyzed include minute-by-minute mean arterial pressure (MAP) from an arterial catheter, intermittent blood pressure cuff readings, volume of administered intravenous fluids, urine output, and all relevant vitals and administered medications. The electronic medical record was queried for additional patient data. IOH was defined as MAP <65 mm Hg for greater than 10 minutes. The primary endpoints of the study were presence and staging of AKI ( [Kidney Disease: Improving Global Outcomes] consensus classification), postoperative ileus, and postoperative troponin leak.
Results Using a partial correlation analysis, no association was found between IOH metrics (IOH occurrence, IOH duration >10 minutes, and total IOH time) and any outcome metrics, including AKI, except for vasopressor usage and estimated blood loss. Patient age at surgery was not associated with any outcome variables. The lack of association between IOH and AKI contrasts with existing literature; this could be due to underlying differences in our patient population or could highlight a more complex relationship between IOH and AKI than previously understood.
Conclusion Occurrence and duration of IOH were not associated with AKI, postoperative ileus, troponin leak, length of stay, or any other major outcome variables in spinal fusion patients.
Clinical Relevance These findings depart from previous literature showing a correlation between IOH and AKI and provide level 3 evidence clinically relevant to spinal surgery. Further research is needed to better understand the exact nature of this relationship.
Level of Evidence 3.
Introduction
Intraoperative hypotension (IOH) is a frequent side effect of general and spinal anesthesia1,2 and is reported to be associated with adverse perioperative events and poor surgical outcomes. Ischemia-reperfusion injury as a result of prolonged decrease in mean arterial pressure (MAP) is thought to contribute to complications such as myocardial injury,3 acute kidney injury (AKI),4 and stroke,5 especially in the setting of major noncardiac surgery. Development of AKI in particular may adversely affect other major organs such as the brain, heart, and lungs, and it puts a patient at greater risk for other serious conditions such as chronic kidney disease, stroke, and heart disease.6 Given these potential risks, it is crucial that IOH be accurately diagnosed and managed by the surgical and anesthesia teams.
Still, the specific relationship between IOH and organ damage remains unclear, particularly with respect to the development of AKI. Debate exists regarding the threshold MAP values that lead to AKI, whether these thresholds are absolute or relative to preoperative MAP,7 and whether other factors such as systolic blood pressure variability modulate AKI risk.8 This imprecise characterization is partially due to the lack of consensus on definition of IOH; 1 survey of 130 research articles found 140 different definitions of hypotension utilized, with varied usage even among the same authors of subsequent publications.9
Furthermore, while IOH has been extensively investigated in vascular, general, plastic, and gynecological surgery, the field of neurosurgery remains largely unexplored in this regard. Given the prolonged operative times and significant risk for blood loss in neurosurgical procedures, the contribution of intraoperative hemodynamic instability in serious postoperative complications such as AKI ought to be well understood. In this report, we review our institutional experience to understand the magnitude of association between IOH in spinal fusion operations and incidence of postoperative AKI.
Methods
Study Design
A retrospective cohort study of 910 patients was designed to assess the relationship between IOH during spine fusion operations and the development of AKI. Only patients who underwent fusion surgeries were included; anterior cervical discectomy and fusion procedures were excluded due to short operative time.
Intraoperative variables collected and analyzed include minute-by-minute MAP measurements from an arterial catheter, intermittent blood pressure cuff readings, volume of administered intravenous fluids, urine output, and all relevant vitals and administered medications. Other variables collected included preoperative serum creatinine and preoperative estimated glomerular filtration rate (eGFR) to assess baseline kidney function. The electronic medical record was queried for additional patient data. The primary endpoints of the study were presence and staging of AKI, postoperative ileus, and postoperative troponin leak.
Relevant Definitions
Given the lack of a standardized definition of IOH, great attention was given to defining the MAP threshold used to determine occurrence of IOH. Despite this lack of consensus, recent literature review has shown that MAP <65 mm Hg is frequently considered the most appropriate threshold value for defining IOH.10 Here, we defined IOH as patients with MAP <65 mm Hg for 10 cumulative minutes throughout the procedure.
AKI was defined using the KDIGO (Kidney Disease: Improving Global Outcomes) consensus classification11 that applies serum creatinine criteria as follows:
Stage 1 AKI: serum creatinine 1.5 to 1.9 times baseline or increase by ≥0.3 mg/dL
Stage 2 AKI: serum creatinine 2.0 to 2.9 times baseline
Stage 3 AKI: serum creatinine ≥3 times baseline or increase by ≥4.0 mg/dL or need for renal replacement therapy
Partial Correlation Analysis
A partial correlation analysis was performed to measure the association of multiple covariates (eg, baseline demographics, intraoperative MAP, etc) with postoperative outcomes. All statistical analyses were performed using MATLAB R2017b (MathWorks, Natick, MA).
Covariates included in this analysis are control covariates (sex, preoperative eGFR, angiotensin-converting enzyme inhibitor usage, diuretic usage, and history of relevant comorbidities) and independent variables (IOH occurrence, IOH duration >10 minutes, total IOH time, age, and preoperative creatinine). Outcome variables explored included postoperative ileus, postoperative troponin leak, AKI, length of hospital stay, estimated blood loss (EBL), need for intraoperative transfusions or medications, and occurrence of relevant postoperative complications).
Pairwise comparisons of each independent variable with the outcome variables were performed using nonparametric analysis for categorical comparisons and parametric analysis for continuous variables to generate Spearman and Pearson correlation coefficients, respectively. Corresponding P values were calculated, representing the test against the null hypothesis that there was no correlation between the independent and dependent variables. P values were compared against a threshold corrected for multiple comparisons (55 comparisons in total) using the Bonferroni correction to arrive at  .12
.12
Differences in baseline demographic characteristics were controlled for using the set of control covariates. Additionally, independent variables apart from the variable of interest in the comparison were controlled to isolate the contribution of each specific variable. The only exception to this was any pairwise comparisons involving any 1 of the 3 IOH-related metrics (IOH, IOH >10 minutes, and total IOH time) did not use the other 2 as internal controls.
Odds Ratio
Additionally, odds ratios were calculated to aid in visualization. Logistic regression was first performed between independent variables and all categorical dependent variables to generate regression coefficients. Odds ratios for each independent variable were then calculated by taking the natural exponentiation of the regression coefficient corresponding to each variable. Confidence intervals were calculated with respect to Bonferroni-corrected α values.
Results
Demographic Data
The mean age at surgery of our patient sample was 61.6 years. Most patients (92.1%) experienced at least transient IOH, defined as MAP <65 mm Hg, with 68.2% of all patients experiencing IOH for 10 minutes or longer. Full demographics and outcomes data for the patient cohort can be found in Table 1.
Summary of patient cohort.
Partial Correlation Analysis
There was no association found between any of the IOH-derived metrics (IOH occurrence, IOH duration >10 minutes, and total IOH time) and any of the outcome metrics, including AKI, except for vasopressor usage and EBL. Patient age at surgery was not associated with any outcome variables. Preoperative creatinine was associated with the ratio of the postoperative creatinine to the preoperative creatinine as well as the length of stay (LOS) in days. All other pairwise comparisons between independent and dependent variables were not significant (Table 2).
Partial correlation coefficients and P values between variables of interest and outcomes.
Odds Ratio
Nonadjusted odds ratios (Figure 1) and adjusted odds ratios (Figure 2) were calculated. With and without controlling for covariates, occurrence of IOH, IOH duration >10 minutes, and total IOH duration were not associated with significantly increased odds of any outcome variables, including AKI, except for use of vasopressors (Tables 3 and 4).
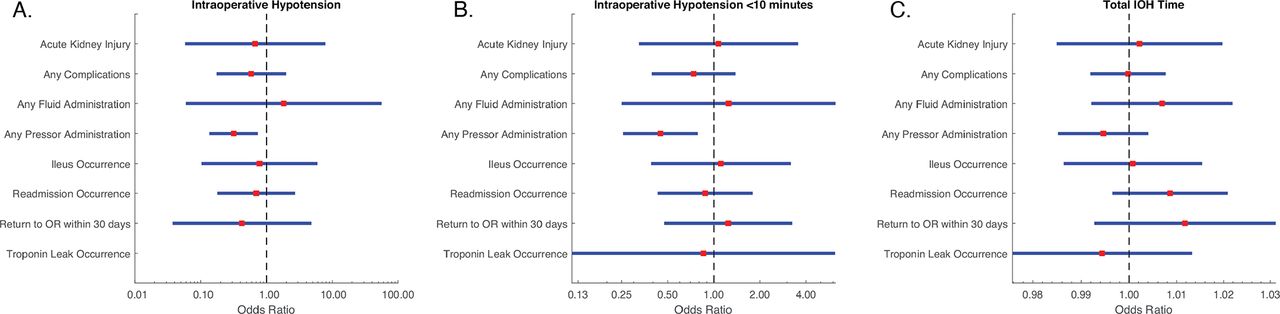
Forest plot of unadjusted odds ratios between postoperative outcomes and (A) occurrence of intraoperative hypotension, (B) intraoperative hypotension lasting for 10 min or longer, and (C) duration of intraoperative hypotension.

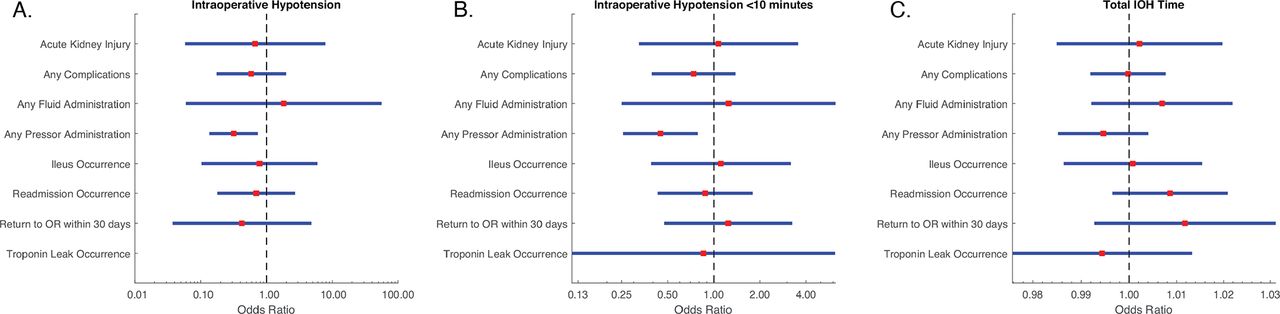
Forest plot of adjusted odds ratios between postoperative outcomes and (A) occurrence of intraoperative hypotension, (B) intraoperative hypotension lasting for 10 min or longer, and (C) duration of intraoperative hypotension.
Nonadjusted odds ratios for association of intraoperative hypotension and outcomes.
Adjusted odds ratios for association of intraoperative hypotension and outcomes.
Discussion
This study sought to determine whether IOH during spinal fusion surgery is independently associated with adverse outcomes such as AKI, myocardial injury (as measured by troponin leak), and postoperative ileus. IOH was characterized as 10 or more cumulative minutes with an MAP of less than 65 mm Hg. AKI was characterized by the ratio of preoperative to postoperative serum creatinine and was staged based on the KDIGO criteria. Using these definitions, we failed to find any independent association between IOH during spinal fusions and AKI, troponin leak, or postoperative ileus. To our knowledge, this is the first study investigating the relationship between IOH and organ injury in spine surgery.
Current literature strongly indicates that IOH is correlated with AKI, though these observational studies have not been able to establish a causative relationship. The hypothesized etiology for AKI after occurrence of IOH stems from previous human13 and animal14,15 studies, which suggest that the lower limit of renal blood flow autoregulation is at an MAP of 50–75 mm Hg, after which blood flow becomes pressure-dependent. In the event of IOH, where MAP reaches the lower threshold of the autoregulation curve, ischemic injury can damage the kidney resulting in AKI. While these thresholds are individual rather than empiric, preventing the definitive conclusion that IOH leads to AKI,4 numerous previous studies have suggested this relationship. For example, Salmasi et al7 found that hypotensive events less than 65 mm Hg were associated with higher odds of both AKI and myocardial injury. This association appears to be time sensitive as well; a systematic review of 42 studies regarding IOH and organ injury found that the risk of organ injury seemed to start at blood pressures less than 80 mm Hg if durations were longer than 10 minutes.16
In contrast to this body of literature, our data do not reveal an independent association between IOH and AKI. Furthermore, the lack of association between IOH and AKI was independent on the duration of IOH that the patient experienced. Several factors could contribute to our findings being inconsistent with previous studies, including the nature of spine procedures and characteristics inherent to the neurosurgical patient population.
One possible reason for the lack of association between IOH and organ injury is the general health of this patient cohort. Mathis et al reviewed more than 130,000 cases of major noncardiac surgeries, using factors such as surgery type, eGFR, and American Society of Anesthesiology (ASA) physical status classification to stratify patients into risk quartiles. Interestingly, they found that low-risk patients could tolerate MAP values as low as 50 mm Hg with no association to AKI.17 While ASA class was not explicitly measured in our patient cohort, studies have shown that the proportion of lumbar fusion patients with ASA class I or II can range as high as 94.8% to 99.6%, leaving very few patients in the higher-risk ASA classes.18,19 It is plausible that our patient cohort comprised a greater proportion of low ASA class patients, and thus, were less sensitive to AKI after experiencing IOH as compared with surgical patient populations with higher average ASA classes.
Different surgical protocols may also affect the relationship between IOH and AKI. It has been previously suggested that the association between IOH and AKI may not be due to a direct effect from IOH itself but rather how IOH is managed in the operating room.4 For instance, administration of high volumes of normal saline (NS; 0.9% sodium chloride) has been shown to cause increased rates of renal dysfunction in patients when compared with the use of balanced crystalloids.20 It is possible that NS administration acts as a confounding variable between IOH and AKI, creating different relationships in surgeries that require varying levels of fluid replacement. However, the effect of NS administration on renal function has been primarily studied in patients who are critically ill or in septic shock.21 Further research is required to understand the effect of unbalanced fluids in the setting of elective surgery and whether such a confounder could have a contributory role in the discrepancy between our findings and current literature.
While we offer possible explanations for our data, it is important to note that more investigation is necessary to fully determine the extent to which IOH and AKI are related. While our analysis indicates that AKI may not be as pertinent as an issue in spinal fusion patients who experienced IOH as previously believed, standard surgical protocols should be followed to avoid and treat IOH; more research must be done to completely understand this phenomenon.
Our study did find correlations between IOH and various secondary outcomes measured. For example, IOH was significantly associated with the use of vasopressors; this finding serves to validate our study, as hypotension is an indication for intraoperative vasopressor administration. Additionally, EBL was associated with total IOH duration but not the binary variable of IOH occurrence. Again, this is not surprising because a longer duration of IOH, rather than a transient IOH period, may indicate a higher quantity of blood lost. Last, preoperative serum creatinine correlated to LOS, possibly indicating that preoperative creatinine is a marker of overall patient health; sicker patients may require a longer recovery after surgery, an interpretation that has been proposed in previous literature.22,23
Our study had several strengths. Our use of an arterial line to measure MAP provided us with a more accurate and physiological evaluation of blood pressure than using an external cuff to measure systolic blood pressure.24 Additionally, our choice to use a partial correlation analysis allowed for the evaluation of the relationship between IOH and our primary outcomes while controlling for other variables, such as age, sex, preoperative use of angiotensin-converting enzyme inhibitors, etc.
This study also had limitations. First, IOH was defined using a threshold of MAP <65 mm Hg; thus quantifying the degree of hypotension (eg, if MAP drops to 55 mm Hg) was not possible. Future studies should attempt to investigate the relationship between AKI and IOH with hypotension as a continuous variable, as previous literature has identified a graded relationship between the extent of IOH in a patient and the risk of organ injury.16 We also viewed the time that a patient was hypotensive as a cumulative measure (ie, a patient hypotensive for 1 minute at 10 separate timepoints is equivalent to a patient who was continuously hypotensive for 10 minutes). This could have diluted the relationship between IOH and organ injury as hypotension for just a short amount of time with recovery periods in between allow for organ reperfusion and potentially minimize acute damage. Last, our findings may also caution against future study designs that group multiple types of major surgeries into the same analysis, as factors unique to different types of surgery and patient populations may impact the measured association between IOH and AKI.
Conclusion
Occurrence and duration of IOH were not associated with AKI, postoperative ileus, troponin leak, LOS, or any other major outcome variables in spinal fusion patients. This is the first such investigation in a neurosurgical patient population, and our findings depart from previous literature showing a correlation between IOH and AKI. Further research is needed to better understand the exact nature of this relationship.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Mitchell Weinstein discloses research support from Edwards Lifesciences for perioperative perfusion monitoring. The remaining authors have no disclosures.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.